
Abstract
BACKGROUND:
To investigate if maternal body mass index, diabetes and hypertension are associated with orofacial clefts.
METHODS:
Case-control study. Information from 53,188 live births with and without orofacial cleft registered at USA Vital Statistics Natality Birth Data between 2017 and 2021. Case group consisted of all affected live births diagnosed with orofacial clefts (13,297 cases). Comparison group consisted of 39,891 live births without clefts or any other congenital malformation. Information about orofacial cleft cases were compared with the comparison group. The unadjusted and adjusted Odds Ratios were estimated to evaluate the strength of association between mother’s pre-pregnancy body mass index, maternal diabetes and hypertension and orofacial cleft occurrence, assuming a p value < 0.05 and 95% confidence intervals (95% C.I.) for statistically significant differences.
RESULTS:
Mother’s pre-pregnancy body mass index, maternal diabetes and maternal hypertension are conditions associated with an increased risk of orofacial cleft development in the child (OR = 1.08, p = 0.004, 95% C.I. = 1.024–1.149; OR = 1.32, 95%, p = 0.000, 95% C.I. = 1.202–1.444; and OR = 1.35, p = 0.000, 95% C.I. = 1.239–1.484; respectively). Maternal ethnicity, sex of infant, and cigarette smoking pregnancy remained as covariates after adjustments in all logistic regression models.
CONCLUSION:
Due to the increased prevalence of obesity, diabetes, and hypertension, and also to their association with congenital malformations, such as clefts, it is recommended that mothers planning to become pregnant to follow healthy habits, maintain healthy weight, and be screened for possible diabetes or hypertension prior to conception and early in pregnancy.
Introduction
Orofacial clefts (OC) are the most common congenital craniofacial anomalies with a prevalence rate of approximately 1 in 700 live births worldwide [1]. Clefts are generally classified as cleft lip with or without palate (CL+P) and cleft palate only (CP) [2]. OC have a complex etiology in which genetic and environmental factors act together, or in isolation in some instances, causing alterations in the fetus embryologic process [3].
More than one gene are related to this malformation, and since each of these individual genes has a small contribution, it is difficult to detect them, because affected individuals can express their conditions due to a variety of different mechanisms that may involve different pathways. The environment can modify these genes and predisposition to the occurrence of clefts is difficult to study [3, 4]. Defining the role of potential environmental factors could reduce the prevalence of this congenital malformation [5].
Several environmental factors have been suggested to be associated with OC, such as smoking tobacco, drinking alcohol, or occupational exposures [6]. Also, studies demonstrated that the risk for birth defects increases with increasing of maternal body mass index (BMI), diabetes and hypertension [7–9]. An intrauterine hyperglycemic environment may cause oxidative stress and increase the risk of congenital anomalies in developing fetuses [10]. The pregestational diabetes [11] and gestational diagnosis of diabetes mellitus indicate possible factors that lead to the OC [12]. Hypertension showed to increase risk of major non-chromosomal congenital malformations in all mothers with this condition [13]. Both maternal obesity [14], and underweight [15] have been found to be associated with clefts. Maternal weight gain seems to increase the risk for diabetes and hypertension [7], and these conditions could act synergistically in the pathogenesis of craniofacial abnormalities [16].
Obesity, diabetes, and hypertension are significant public health problems [17], and their rising rates in the population may result in an increased burden of birth defects, such as clefts [7]. However, issues regarding the relationship between these diseases and OC are still insufficiently studied [7]. Authors highlight the importance of understand the aspects related to OC etiology in order to prevent them when possible [6]. Therefore, the objective of this study was to investigate if maternal body mass index, diabetes and hypertension are associated with OC.
Methods
This is a case-control study conducted with data from 53,188 live births collected from the USA Vital Statistics Natality Birth Data for the last five years available (2017 to 2021). Natality data show demographic and health data for births occurring in the United States for each year. These data are provided to the National Center for Health Statistics (NCHS) through the National Vital Statistics System (NVSS) and are based on the Standard Certificate of Live Birth, which was fully implemented in all States of the United States (USA) and District of Columbia in 2016 [18]. The vital statistics data are interpreted according to various qualifying factors and methods of classification in order to verify their value for utilization in most general purposes [18], making these data the most comprehensive and reliable USA national source of birth information [19].
This study used public-use natality data from an open access information system, in which the data are presented without identifying the subjects. Investigators here had no contact with human subjects. Also, this study was reported according to the recommended STROBE (STrengthening the Reporting of Observational studies in Epidemiology) statement [20].
The cases consisted of all affected live births diagnosed with OC registered in the NVSS (13,297 cases in total, being 9,596 with CL+P, and 3,701 with CP) from 2017 to 2021. OC identified at birth were reported on the revised 2003 birth certificate, having a checkbox (“yes”, “no”, “unknown or not stated”) for each type (CL+P and CP). It was only considered as cases those with a confirmed register (Yes) of presence of CL+P and/or CP, with or without any other congenital malformation (syndromic and non-syndromic OC, respectively). Infants whose birth certificate did not indicate the presence of OC (“unknown or not stated”) were excluded for the study. Cases were combined in a 1 : 3 ratio with a comparison group of 39,891 live births without history of clefts or any other congenital malformation that were born during the same period. The selection of the control group was done randomly after remove from the population all births considered as cases, births without register for OC, and births that have a positive or unknown diagnosis for any of other 11 congenital malformations (cyanotic congenital heart disease, hypospadias, Down syndrome, gastroschisis, suspected chromosomal disorder, meningomyelocele/spina bifida, congenital diaphragmatic hernia, limb reduction defect, anencephaly, and omphalocele) without OC combined. For Down syndrome and suspected chromosomal disorder, it was also excluded those with “pending” confirmation (Fig. 1).
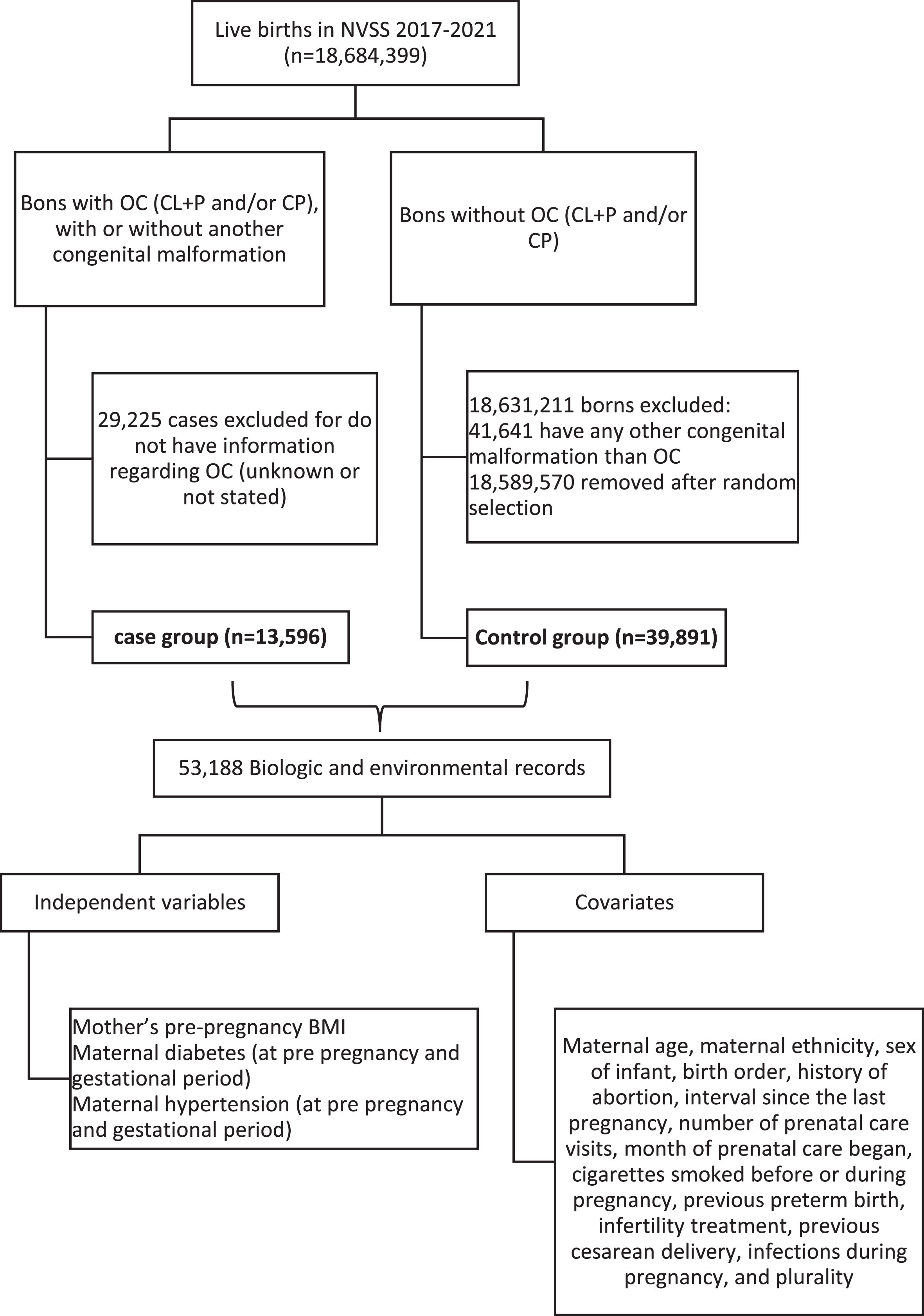
Overall study design.
Mother’s pre-pregnancy Body Mass Index (BMI) indicated mother’s body fat based on her height and pre-pregnancy weight [18]. It was calculated as: [mother’s pre-pregnancy weight (lb)/[mother’s height (in)]2] x 703. The categories for BMI classification adopted in the vital record were established by the National Health, Lung and Blood Institute [21] as underweight (BMI < 18.5), normal weight (BMI 18.5–24.9), overweight (BMI 25–29.9), class I obese (BMI 30–34.9), class II obese (BMI 35–39.9), and class III obese (BMI > 40).
Information about the presence or absence of maternal diabetes and maternal hypertension are available in the USA Vital Statistics Natality Birth Data for both pre pregnancy and gestational period, identified as “yes” and “no”. These data are collected directly from the Facility Worksheet for a Live Birth Certificate, which is typically completed by a medical professional based on mother’s prenatal care records. The dataset does not inform if these diseases were controlled or uncontrolled [18].
Maternal diabetes mellitus was defined as having type 1 or type 2 diabetes diagnosed prior to the pregnancy, as pre gestational diabetes, or during the pregnancy, as gestational diabetes [10].
Maternal hypertension was considered as the elevation of blood pressure above normal for age, gender, and physiological condition diagnosed prior to the onset of the pregnancy (pre gestational hypertension) or during this pregnancy (gestational hypertension). This elevation of blood pressure should be ≥140 mmHg (systolic blood pressure) ≥90 mmHg (diastolic blood pressure) on two separate occasions at least four hours apart after 20 weeks of pregnancy when previous blood pressure was normal [22]. This study also analyzed maternal diabetes and maternal hypertension without distinguishing between gestational and prepregnancy period in order to minimize chances of bias due to misclassification.
Information regarding maternal age, maternal ethnicity, sex of infant, birth order, history of abortion, interval since the last pregnancy, number of prenatal care visits, month of prenatal care began, cigarettes smoked before or during pregnancy, previous preterm birth, infertility treatment, previous cesarean delivery, infections during pregnancy, and plurality were collected and used as covariates.
All variables were analyzed previously according to the criteria of incompleteness proposed by Romero and Cunha [23, 24] as excellent (< 5%), good (5% to 9.9%), regular (10% to 19.9%), poor (20% to 49.9%), and very poor (≥50%). Differences between cases and controls were evaluated using chi-square. In addition, analyses were done by cleft type (cleft palate only and cleft lip with/without cleft palate) to explore the possibility of different etiological mechanisms that may affect differently the two cleft types [25]. Unadjusted Odds Ratios (OR) were estimated to evaluate the strength of association between mother’s pre-pregnancy BMI, maternal diabetes and hypertension, and types of OC occurrence. Because overweight and obesity are risk factors for both gestational diabetes and hypertensive conditions [19], stratified analyses were done according to the mother’s pre-pregnancy BMI status (normal x underweight/obese/overweight). Potential associations between the covariates and clefts were also determined. Then, logistic regression models were used to assess the adjusted OR, adjusting by those covariates that have been shown statistically significant differences associated with clefts. All these analyzes were done using STATA Software, assuming a p-value < 0.05 and 95% confidence intervals (95% C.I.) not involving 1.0 as statically significant.
From 53,188 live births collected from the USA Vital Statistics Natality Birth Data for the last five years available (2017 to 2021), 13,297 had OC, 31,074 (58.42%) mothers had altered BMI (underweight, overweight or obesity), 690 (1.30%) had pre gestational diabetes, 4,014 (7.55%) mothers had gestational diabetes, 1,302 (2.45%) mothers had pre-hypertension, and 4,318 (8.12%) mothers had gestational hypertension. All variables included in this study had an excellent to good degree of incompleteness, with missing data ranging between 0% to 3.03%, with the exception of “interval since the last pregnancy” that had a poor degree of completeness, missing 43% of data. Comparing the groups, only maternal age did not show to have a statistically significant difference (p = 0.959) between cases and controls.
Stratified analyses showed that the risk for OC in the child was lower among mothers with diabetes or hypertension who had normal BMI (OR = 1.31 and OR = 1.35 respectively), comparing with those underweight, obese or overweight (OR = 1.35 and OR = 1.37, respectively). However, none of these analyses were statistically significant (p = 0.653, 95% C.I = 1.138–1.508 and p = 0.891, 95% C.I. = 1.191–1.540 respectively). The unadjusted and adjusted OR regarding the strength of associations between mother’s pre-pregnancy BMI, maternal diabetes and hypertension and OC occurrence can be found in Table 1. Maternal ethnicity, sex of infant, cigarettes smoked before or during pregnancy, remained as covariates after adjustments in all logistic regression models.
Unadjusted and adjusted odds ratios (OR) between independent variables and orofacial clefts
Unadjusted and adjusted odds ratios (OR) between independent variables and orofacial clefts
Bold indicates statistically significant p-values under the threshold 0.05.
The findings of this study demonstrated that mother’s pre-pregnancy BMI, maternal diabetes and maternal hypertension are conditions associated with an increased risk of OC development in the child. These results reinforce the need to follow up pregnant women in order to control the identified risk factors.
Mother’s pre-pregnancy BMI was associated with OC, confirming findings that underweight or overweight/obese women are at higher risk to have a child with clefts, compared to women of recommended weight [7, 26]. The underlying mechanisms for the increased risk of OC in both underweight and obese mothers are unclear and could be very different [25]. However, several mechanisms have been hypothesized as potential explanations for this association, such as insulin resistance and hyperglycemia during embryogenesis (also common for diabetes) [16]. Maternal obesity [16, 27] and maternal underweight [25, 28] may also be associated with poor nutrient intake and low blood levels of nutrients critical for fetal development, resulting in poor reproductive outcomes. Some population studies using vital records of some United States regions have shown positive associations between maternal obesity and risk of orofacial clefts [9, 29]. A study using Western Australian Birth Defects Registry data found a twofold-increased odds of having an infant with OC among women with pre-pregnancy obesity [30]. Analyses of six large case-control studies of OC from Northern Europe and the USA also found an increased risk of clefts in obese mothers compared with normal-weight mothers and suggested that extremes of weight may have a specific effect on palatal development [25]. Given the increased risk for OC and other birth defects associated with maternal obesity [16], preconception counseling should emphasize the importance of maintaining normal weight [9, 29–31].
Pre-gestational and gestational diabetes are commonly linked to OC [32, 33]. In this study, the presence of maternal diabetes was associated with an increased risk for clefts, with a twofold increased odds for clefts among mothers who had pre pregnancy diabetes, confirming results found in other studies [10, 34]. Although the mechanisms underlying associations between diabetes mellitus and birth defects are not completely understood, it seems that hyperglycemia during embryogenesis could increase oxidative stress, epigenetic changes, hypoxia, and apoptosis, contributing to DNA damage and a higher risk for congenital malformations, such as clefts [12, 36].
Maternal hypertension is another pregnancy complication that can potentially increase the risk for clefts [7, 37]. Findings from the present study confirmed the association between pre or gestational maternal hypertension and OC in the offspring. Although the stratified analysis did not show statistically significant increases in the risk for obese hypertensive mothers, the literature revealed that the risk for OC seems to be elevated among mothers with hypertension who were also obese [7]. Due to the increased prevalence of obesity, diabetes, and hypertension, and also to their association with congenital malformations, such as OC, it is recommended that mothers planning to become pregnant to follow healthy habits, maintain healthy weight, and be screened for possible diabetes or hypertension prior to conception and early in pregnancy [7].
As strengths of this study, it has a full coverage of a nationwide population of mother-infant pairs, a large sample size, and low levels of missing data, which allow to better examine rare conditions, such as OC. Also, the analyzes done here took into account the adjustment for several covariates to confirm the findings. Here we opted to develop a case-control study because even though OC are among one of the most common congenital malformations of the craniofacial region [38, 39], they were also a rare event considering all population, which is one of the indications of using this kind of study design. Consequently, the association analyzes were done by OR, and the use of logistic regression becomes the better approach to obtain the adjusted OR when there is a dichotomous outcome [40]. Other studies were done using this kind of study design to assess the association between some risk factors and birth congenital anomalies [41, 42].
This study has some limitations inherent to the design of the case-control study, such as the convenience sample and the retrospective measurement of the predictive variables (susceptible to memory bias) [40]. Belong that, the principal limitation here would be the use of vital statistics data, which is susceptible to bias in the original records or in tabulation due to missing or misclassifications. However, this limitation does not decrease the value of USA Vital Statistics Natality Birth Data since they are analyzed by various qualifying factors in order to increase its reliability [18]. These data are the only USA database for births that is national in scope, and our analyzes revealed an excellent to good degree of information incompleteness, strengthening their use as a comprehensive and reliable USA national source of birth data. Another limitation would be the identification of OC cases solely from birth certificates registry due to chances of imprecision in cleft registration. However, OC are a type of congenital anomaly likely to be observable at birth, with relatively well-defined categories. Also, the registration of the presence or absence of OC in the birth certificate is done after medical evaluation. These factors minimize chances of OC misclassification (i.e., the infants who did not have diagnosis of OC at birth but were diagnosed later in life were treated as not having OC in this study) and increase the sensitivity. Furthermore, several studies have been performed using this approach to select cases and assess the association between some risk factors and birth congenital anomalies and in USA [9, 43–45] and in other countries [46–48].
Conclusion
The findings of this study demonstrated that mother’s pre-pregnancy BMI, maternal diabetes and maternal hypertension are conditions associated with an increased risk of OC development in the child. These results, along with the increased prevalence of obesity, diabetes, and hypertension, in the population, reinforce that mothers planning to become pregnant should follow healthy habits, maintain healthy weight, and be screened for possible diabetes or hypertension prior to conception and early in pregnancy.
Disclosure statements
No potential or actual interests are disclosed.