
Abstract
OBJECTIVE:
To assess the effect of cardiovascular medications on the neurodevelopment of preterm infants, as measured by calculated cumulative time of vasoactive–inotropic score (VISct).
METHODS:
A retrospective study was conducted on preterm infants who developed significant hypotension defined as a mean BP more than 2SDs below the mean for GA and received treatment with duration > 6 hours for each hypotensive episode, we calculated the vasoactive inotropic score (VIS) and cumulative exposure to cardiovascular medications over time (VISct). The composite Bayley III was reported from the high-risk follow-up clinic for the surviving infants between 18 to 21 months corrected age.
RESULTS:
VISct was significantly higher in infants with abnormal neurodevelopment. Cognitive Bayley was the most affected component with median (IQR) VISct 882.5(249,2047) versus 309(143,471) (p-value 0.012), followed by language function with VISct 786(261,1563.5), versus 343(106.75,473.75) (p-value 0.016) when those with Bayley III <85 were compared with those with normal Bayley IIIs.
CONCLUSION:
High VISct scores may have negative effect on cognitive and language neurodevelopmental outcomes.
Keywords
Abbreviations
Blood Pressure
Compromised systemic circulation
Intraventricular hemorrhage
Mean arterial blood pressure
Necrotizing enterocolitis
Vasoactive inotropic score
Vasoactive inotropic score with cumulative time of exposure to cardiovascular medication
Introduction
Many preterm infants <29 weeks GA receive cardiovascular medications either soon after birth or during admission and have been reported as high as 98% [1–3]. There is no consensus guideline or algorithm even within most NICUs for treating hypotension [4]. In a prospective observational study that included 367 infants from 16 centers affiliated to the National Institute of Child Health, 15 different definitions were used among the 16 participating centers, and cardiovascular medication administration was not associated with improved short term outcomes for all definitions of low blood pressure (BP) investigated; treated infants had worse outcomes [4]. The available data suggest that cardiovascular medications might improve BP, but there are no data to support these medications improving end-organ blood flow [1, 5], a recent study showed increased mortality related to the unnessessary combination of cardiovascular medication and validated the VISscore as a predictor for CSC (Compromised systemic circulation) and mortalityin neonatal population [6]. No study has shown that the management strategies for treating low BP or specific medications, including volume expanders, vasopressors, or inotropes, have any positive effect on developmental outcomes [3]. The main aim of this study was to assess the association of cumulative exposure to cardiovascular medications using VISct scores and neurodevelopmental outcomes at 18 to 21 months of age in preterm infants <29 weeks GA.
Methods
All infants admitted to the 2 tertiary NICUs in Winnipeg, Canada, between 2011–2015 who received cardiovascular medications were identified using the pharmacy’s electronic records. Preterm infants <29 weeks were identified, and a retrospective chart review was undertaken. Significant hypotension was defined as a mean BP more than 2SDs below the mean for GA [1, 7], we used the lowest mean blood pressure as shown in (Table 3). Those with significant hypotension persisting for > 6 hours and received cardiovascular medications were included. All infants with congenital or chromosomal anomalies were excluded. We calculated the vasoactive inotropic scores (VIS) as follows [Dopamine (mcg/kg/min)+Dobutamine (mcg/kg/min)+Epinephrine (mcg/kg/min)×100 + Norepinephrine (mcg/kg/min)×100 + Vasopressin (IU/kg/min)×10000 + Milri-none (mcg/kg/min)×10 [6, 8–10]. Then we calculated the cumulative vasoactive inotropic time (VISct) by multiplying the (VIS) for each drug with the exposure time in hours. Demographic and clinical data were abstracted from the chart review. Those data included antenatal steroids, gestational age (GA), birth weight, sex, Apgar scores at 5 and 10 minutes, confirmed sepsis, and IVH. The study period was before the era of targeted neonatal echocardiography being a standard of care in our NICU for the assessment of infants with refractory hypotension; the cardiovascular medications were prescribed empirically, starting with dopamine with the addition of dobutamine or epinephrine as the second or third line, plus the administration of multiple empirical normal saline boluses. A comprehensive neurodevelopmental assessment was performed at 18–21 months postnatal age; The assessment included a standardized history, physical and neurologic examinations, and administration of the Bayley Scales of Infant and Toddler Development (Bayley)-third edition (Bayley-III) by trained assessors. Bayley-III cognitive, language and motor composite scores were obtained. The Bayley-III Adaptive Behavior questionnaire result was used in cases where the child could not be tested. A diagnosis of cerebral palsy was made using Gross Motor Function Classification System (GMFCS) of 2 or more degree of functional impairment [10]. 11. Hearing assessment results and the need for hearing aids or cochlear implants were obtained through history. Ophthalmology follow-up for retinopathy of prematurity and visual status was documented. If vision history was unknown, a small- scarred eye, sustained sensory nystagmus, or lack of response to a 1 cm object on white background from 30 cm was defined as visual impairment [11, 12]. Ethics approval was obtained from the University of Manitoba Research Ethics Board.
Statistical analysis
Data are presented as median with interquartile range for continuous variables and count with percentage for categorical variables. For continuous and categorical variables, comparisons between groups were analyzed by mood’s median test and Chi-square test; p < 0.05 was considered significant. Receiver operator curve was constructed to assess the predictive values of VISct. All analysis were performed using R statistical software version 4.1.2.
Results
A total of 102 preterm infants were enrolled, 35 infants died due to refractory hypotension before discharge, and 67 infants survived. 24 infants had no follow-up records, and neurodevelopmental follow-up was conducted on 43 preterm infants (64% follow-up rate) in our high-risk follow-up clinic. They were divided into 2 groups, group 1 with normal neurodevelopmental outcome and group 2 with abnormal neurodevelopmental outcome defined as composite Bayley <85 or 1 SD below the mean and/or hearing impairment and/or visual impairment and/or any cerebral palsy.
Median (IQR) gestation and birth weight of 26(25–28) weeks and 860(740–1105) gm respectively. Twenty-one had normal neurodevelopmental outcomes, and 22 had composite Bayley III <85. VISct was calculated for both groups and found to be significantly higher (P-value 0.015) in infants with abnormal neurodevelopmental outcomes as well as the cumulative time of low BP (P value 0.002) (Table 1). There was no significant difference between both groups in GA, BW, sex, antenatal steroids, Apgar scores at 5, 10 minutes, chorioamnionitis, confirmed infection, duration of mechanical ventilation, necrotizing enterocolitis (NEC), retinopathy of prematurity (ROP) and any IVH. Cognitive Bayley was the most affected component (Table 2) with median (IQR) VISct 882.5(249,2047) versus 309(143,471) (p-value 0.012), followed by language function with VISct 786(261,1563.5), versus 343(106.75,473.75) (p-value 0.016) when those with Bayley III <85 were compared with those with normal Bayley IIIs. Motor development, hearing loss and impaired vision were the least affected. A VISct cut off 400 had sensitivity and specificity of 72.7% and 57.1%, and positive and negative predictive values of 64% and 66.7%, respectively in predicting at least one poor neurodevelopmental aspect. Figure 1 shows the receiver operator curve. Based on the results of the ROC analysis, VISct has significant predictive power for composite neurodevelopment with a high accuracy (AUC = 0.73, 95% CI; 0.57–0.88).
Descriptive data of the studied groups presented as median (IQR) and percentages, p value is bold when significant
Descriptive data of the studied groups presented as median (IQR) and percentages, p value is bold when significant
GA, gestational age; BW, birth weight; VISct, vasoactive inotropic scores cumulative; NEC, necrotizing enterocolitis; ROP, retinopathy of prematurity; IVH, intraventricular hemorrhage.
Neurodevelopmental outcomes for both groups as composite Bayley III <85 [language, cognitive, motor] presented as comparison between median (IQR) of VISct
Blood pressure ranges for post-Menstrual age (in weeks)
Derived from Zubrow, A.B., Hulman, S., Kushner, H. & Falkner, B. (1995). Determinants of blood pressure in infants admitted to neonatal intensive care units: A prospective multicenter study. Journal of Perinatology, 15(6), 470-479.
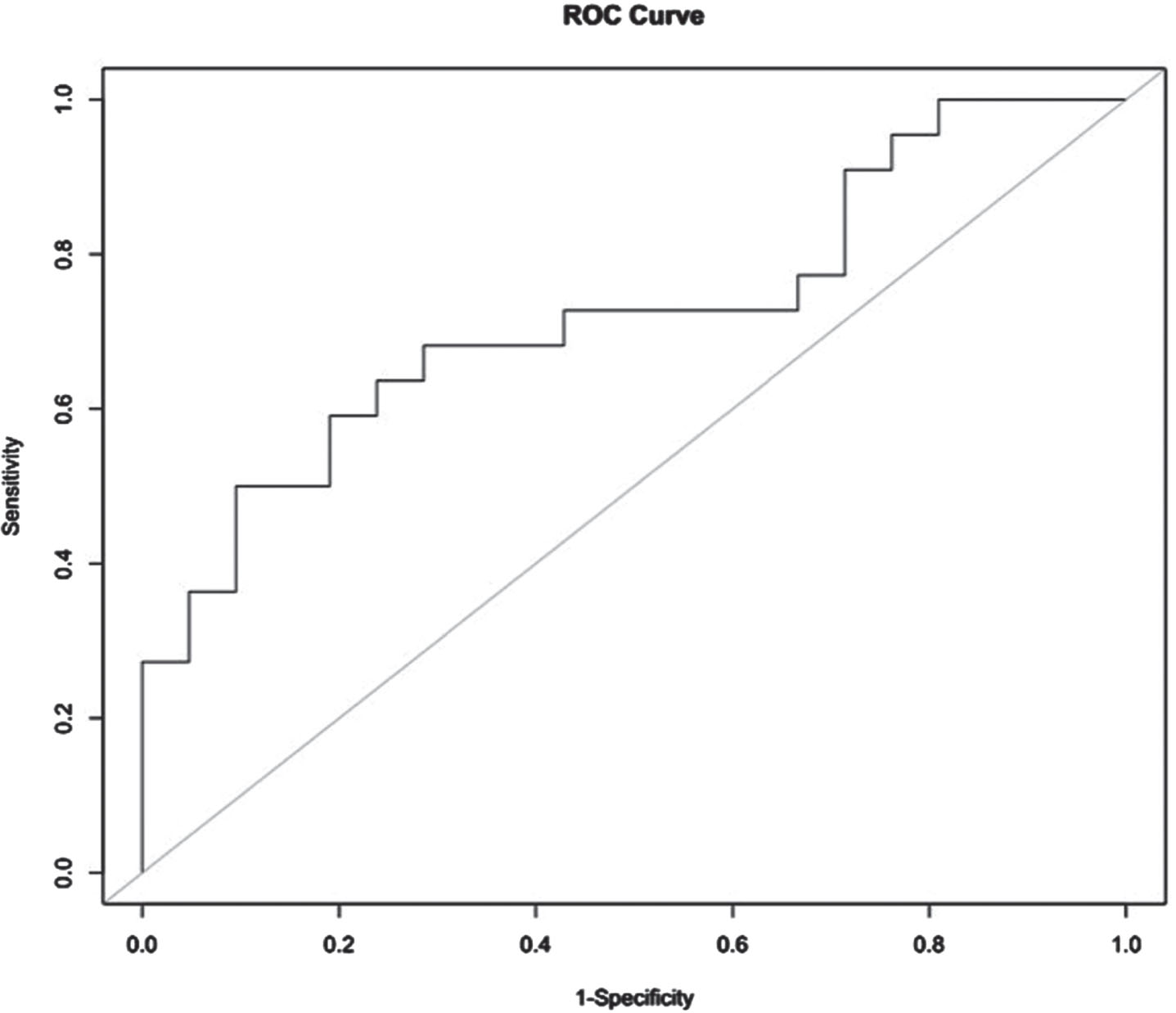
ROC curve of VISct and composite neurodevelopmental scores.
We have examined in this study the association of cumulative exposure to cardiovascular medications using the VISct scores and different neurodevelopmental parameters. The current research provides that neonatal hypotension could be associated with adverse short and long-term outcomes. The most common detrimental short-term clinical consequences are intraventricular hemorrhage (IVH) and periventricular leukomalacia necrotizing enterocolitis (NEC), and finally death [13–15]. No known cardiovascular medication has been proven in randomized control trials to improve short- or long-term outcomes other than improving blood pressure itself [1–3]. A report from the Canadian neonatal network (CNN), which took the lowest recorded blood pressure into account, showed that infants who had blood pressure below their gestational age, or had blood pressure below the 10th percentile, had a slightly increased chance of having a severe IVH. Still, this risk disappeared after correction for the use of cardiovascular medications, interestingly the infants from the same database who had treatment with cardiovascular medications despite a BP that was never low according to these two criteria, had a higher incidence of severe IVH than hypotensive infants who were not treated [3]. Another study conducted by CNN (Canadian Neonatal Network) on infants who received inotropes in the first week of life showed lower cognitive and motor scores associated with longer duration of inotropes [16]. The explanation could be that cardiovascular medications are more harmful than hypotension itself [1, 18] especialy if escaleted without looking into the physiological cause or modifying the medication based on an adequate hemodynamical assessment. To our knowledge, this is the first study to report the association between the cumulative exposure to cardiovascular medications using the VISct scores and neurodevelopmental scores, VIS score was validated recently this year as a mortality predictor in neonatal population [6], our data shows that the higher exposure was associated with significant impairment of cognitive and language development and less effect on the motor, impaired vision, and hearing loss, and cumulative exposure to low BP was associated with significant neurodevelopmental changes. This could be related to inappropriate random selection of cardiovascular support, which was inconsistent with the underlying pathophysiology [19–21],in addition to prolonged use of medications despite no clinical improvement rather than changing the treatment approach. This study has several limitations, including retrospective analysis, almost one-third of eligible infants missed follow-up, and a small number of the studied group.
Conclusion
VISct may be usefull in predicting the neurodevelpomental outcomes in Preterm Infants <29 weeks gestation.
Statements and declarations
Funding
None.
Conflicts of interest/Competing interest
None of the authors have any conflicts of interest or competing interest.
Ethics approval
Obtained from the University of Manitoba Research Ethics Board.