Thyroxin Threshold Linked to Impaired Outcome in Preterm Infants: A Retrospective
Cohort Study
Jean Michel Hascoet1, Stephanie
Coquelet1, Helene Deforge2
1Department of Neonatology, Regional Maternity, CHRU Nancy,
France
2EA3450- DevAH, University of Lorraine, France
Introduction: It remains controversial whether
transient hypothyroxinemia of prematurity influences short- and long-term outcomes. Thus, we
aimed to define a thyroxin threshold associated with neonatal clinical impairment and
outcome at 3 years of age.
Methods: We retrospectively analyzed medical
records of infants born at a gestational age (GA) of < 29 weeks. A thyroxin threshold
value was defined by ROC curve analysis in a cohort of infants born from 10/2008–12/2012,
and validated in a second cohort of infants born from 01/2014–12/2016 in our
institution.
Results: Our analysis included 460 patients
(mean GA, 26.7 ± 1.3 weeks; mean birth weight, 935 ± 206 g). Thyroxin (FT4) measurements
were available for 196/274 infants from the early time period, among whom 35 exhibited
neonatal clinical impairment. ROC curve analysis indicated an FT4 threshold of 10 pmol/L,
with a sensitivity of 85.7%, and a specificity of 49.1%. FT4 measurements were available for
176/186 infants from the second time period: neonatal clinical impairment occurred in 20/78
infants with FT4 = 10 pmol/L versus 3/98 with FT4 > 10 pmol/L (P <.001). Three-year
follow-up data were available for 147/196 eligible infants. Poor outcome occurred in 65%
(58/89) with FT4 = 10 pmol/L versus 34% (20/58) with FT4 > 10 pmol/L (OR, 3.555; 95% CI,
1.774–7.128; P <.001).
Conclusion: We defined and validated a FT4
threshold of 10 pmol/L as a significant risk factor for neonatal clinical impairment, and a
good predictor of poor outcome at 3 years of age.
Cardiovascular risk profile in former very preterm infants at a preschool age
Ursula Kiechl-Kohlendorfer1, Anna
Posod1, Irena Odri Komazec2, Daniela Baumgartner3
1Department of Pediatrics II (Neonatology), Medical
University of Innsbruck, Innsbruck, Austria
2Department of Pediatrics III (Pediatric Cardiology,
Pulmonology, Allergology and Cystic Fibrosis), Medical University of Innsbruck, Innsbruck,
Austria
3Department of Pediatrics, Clinical Division for Cardiology,
Medical University of Graz, Graz, Austria
Introduction: Cardiovascular disease is the
leading cause of death worldwide. Evidence points towards an unfavorable cardiovascular risk
profile of former preterm infants in adolescence and adulthood. Aim of the study was to
determine whether cardiovascular risk predictors are already present at a preschool age.
Methods: We investigated five- to
seven-year-old children born with a gestational age < 32 weeks (n=76) and a control group
of same-aged children born at term (n=79). Basic data were collected by means of follow-up
databases and standardized questionnaires. At study visit, anthropometric data, blood
pressure readings, blood samples after an overnight fast, aortic intima-media thickness and
aortic elastic properties were obtained.
Results: Compared with children born at term,
the preterm group showed significant differences in blood pressure readings, fasting glucose
levels, homeostasis model assessment index, cholesterol levels (p<0.05, each),
differences in amino acid profiles and lipid metabolism. The preterm group showed
significantly reduced distensibility and increased stiffness of the descending abdominal
aorta (p<0.05).
Conclusions: Clinical follow-up of preterm
infants including cardiovascular parameters might be useful for tailoring early prevention
programs and counteracting cardiovascular risk in adulthood.
Keywords: Cardiovascular risk, preschool age, very
preterm infants
Relevance of oral glucose tolerance test (OGTT) in pregnancy and other maternal and
fetal measures for discrimination between LGA infants and infants of diabetic
mothers
Roland Hentschel1, Martine
Thill1, Alexandra Krause2, Julia Trost1, Mirjam
Kunze3, Karl Otfried Schwab2
1Dept. of General Pediatrics and Adolescent Medicine,
Division of Neonatology/Intensive, Care Medicine Medical Center and Medical Faculty -
University of Freiburg, Germany
2Dept. of General Pediatrics and Adolescent Medicine,
Division of Endocrinology/Diabetes, Medical Center and Medical Faculty - University of
Freiburg, Germany
3Dept. of Obstetrics and Gynecology, Medical Center and
Medical Faculty - University of Freiburg, Germany
Introduction: Newborns may be
large-for-gestational-age infants (LGA) from constitutional (ethnic) phenotype (fetal
macrosomia (FM)), or as a consequences of inadequately controlled gestational diabetes
mellitus (GDM) or preexisting diabetes mellitus (DM). It might be prudent to identify
infants from a diabetic mother (IDM) as early as possible, because of their specific
perinatal problems or the heritability of the diabetic predisposition.
Methods: Observational study on pregnant women
with DM, GDM or suspected FM using fetal ultrasound, medical history, OGTT and further
variables. Collection of anthropometric and metabolic data (mothers/infants). Measurement of
fructosamine, IGF-1, insulin, leptin and retinol-binding-protein-4 from cord blood.
Statistics: Mann-Whitney U test, Fisher’s exact test, logistic regression.
Results: 63 mother-infant dyads with GDM/DM,
17 with FM, and 47 controls (C) were enrolled. There was a good compliance with guidelines
for diabetes screening in pregnancy in all 3 groups (only 9.5% of IDMs >P90). OGTT was
able to discriminate between GDM and FM, or GDM and C (p<0.001). Mean of weight, length
and abdominal circumference at birth was highest in FM, lower in GDM and lowest in C
(p<0.001). In multiple linear regression analysis leptin and IGF-1 were both associated
with birth weight (p<0.001), however, all 5 serum markers were unable to discriminate
between LGA and FM.
Conclusion: High compliance with medical
recommendations for GDM may lead to vanishing LGA phenotype of IDM, and biochemical
parameters may be normal. Cord blood leptin and IGF-1 may be suitable to distinguish between
IDMs and FM infants in a less well controlled cohort.
4 years period analysis of newborns with Oesophageal atresia in Latvia
Renate Zarina, Alexandra Yurash
Clinic of Neonatology, University Children’s Hospital, Riga, Latvia
Introduction: Oesophageal atresia (OA) is
complicated congenital anomaly what is associated with complex and long term treatment. Our
objective was to describe the incidence of OA, patient characteristics and short term
outcomes for patients treated in our Neonatal clinic in Latvia. METHODS: Retrospective
analysis of clinical charts and case records of all neonates with diagnosed OA in Latvia,
treated in University Children’s hospital during 2013-2017.
Results: We enrolled 24 neonates, 3 of them
from twin pregnancy (12,5%),14 boys (58,3%), 10 girls (41,6%), 41,6% premature. Mortality -
8.3% (associated with other congenital pathologies). 23 neonates had OA with distal
tracheoesophageal fistula (TEF), 1- without TEF. For 20 infants oesophagoplasty was done
with primary anastomosis and ligation of TEF,4 patients had “long-gap” with delaying primary
repair. Postsurgical mechanical ventilation (MV) – median time 5 days (2>51),boys needed
longer MV (p<0.05),all received parenteral nutrition(PN)– average 22,7 days. Early
complications included pneumothorax-10 patients, sepsis 10 cases, surgical wound infection
1. Recurrent TEF and anastomotic leaks in 7 patients (29,1%). Mean hospital stay was 42 days
(16 to 120), for OA with “long-gap” - 65.25 vs 37.45 days p=0.054. Preterm neonates had
longer MV (5,2 vs 16.2 days ), PN (6.75 vs 32.1 days) and also hospital stay duration (27.14
vs 63 days), p>0.05.
Conclusions: This study describes population
characteristics (incidence 1:4447), management and outcomes (the most common early
postoperative complications were right-sided pneumothorax and sepsis) of OA patients treated
in Latvia in 4 years period. Longer hospital stay correlated with prematurity and “long-gap”
OA.
Keywords: Oesophageal atresia, neonates, early
postoperative complications.
High dose caffeine in very preterm infants: A systematic review and
meta-analysis
Petter Brattström1, Chiara Russo2, David
Ley3, Matteo Bruschettini4
1Lund University, Lund, Sweden
2Genoa University, Genoa, Italy
3Department of Pediatrics, Lund University, Lund, Sweden
4Department of Pediatrics, Lund University, Lund, Sweden;
Cochrane Sweden
Introduction: Observational studies suggest
that maintaining high blood concentrations of caffeine in very preterm infants is associated
with improved respiratory outcomes.
Methods: A systematic review was conducted to
assess the efficacy and safety of high (loading dose >20 mg/Kg and maintenance >10
mg/Kg/day) versus low dose of caffeine. MEDLINE, EMBASE, Central, and conference proceedings
for randomized controlled trials (RCTs) and quasi-RCTs were searched. A fixed-effect model
was used. The quality of evidence was assessed using the Grading of Recommendations
Assessment, Development and Evaluation (GRADE).
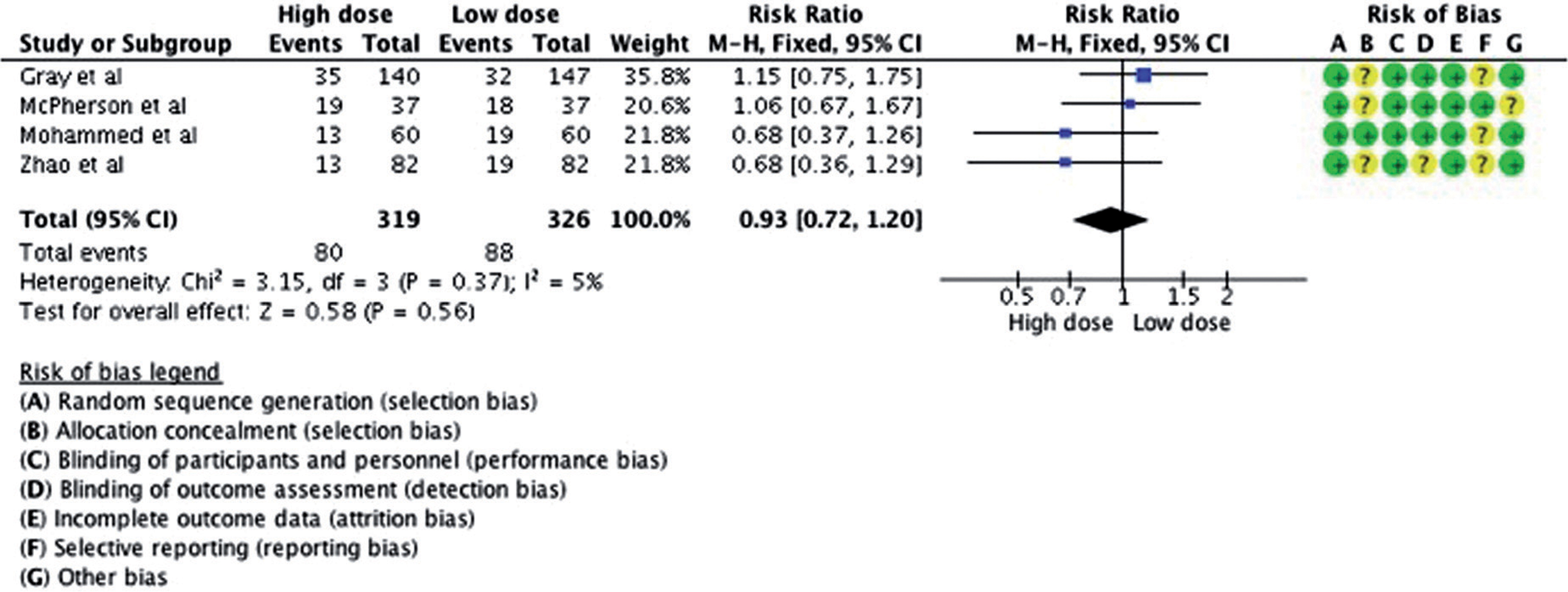
Results: Amongst the six included trials, the
loading and maintenance doses varied between 20-80 mg/kg/day and 3-20 mg/kg/day,
respectively. Overall, caffeine administration was started within 3-4 days of life and
lasted 25-30 days. The use of high dose had no impact on mortality (RR: 0.85; 95% CI:
0.53-1.38; studies = 4) or bronchopulmonary dysplasia (RR: 0.93; 95% CI: 0.72-1.20; studies
= 4). There were fewer cases of extubation failure and apneic spells in the high dose group.
The quality of the evidence was low due to imprecision of the estimates (GRADE). We
identified one ongoing trial which is conducted in China (estimated completion date October
2018).
Conclusion: High dose of caffeine might
improve short-term respiratory function without reducing bronchopulmonary dysplasia. However
the optimal information size has not been reached. Future trials should ameliorate
allocation concealment and outcome reporting.
High dose caffeine was not better than low dose for preventing bronchopulmonary
dysplasia (RR: 0.93; 95 % CI: 0.72;1.20)
Acknowledgements: We thank Matthias Bank
(Library and ICT-services - Lund, Sweden) for defining and running the search strategy;
Cochrane Austria for providing methodological training to Petter Brattström.
Keywords: methylxanthine, dose-response, cerebral
palsy, Cochrane, prevention, evidence-based medicine
Timing and Progression of Oxygen-Induced-Retinopathy by Recurrent Intermittent Hypoxia
and Desaturations in a Neonatal Rat Model
Kay D. Beharry, Gloria B. Valencia, J. V.
Aranda
Department of Pediatrics and Ophthalmology,State University of New York
Downstate Medical Center, New York, USA 11203
Introduction: The 3rd Global Epidemic of
Retinopathy of Prematurity (ROP) is underway and warrants pharmacologic and other
interventions to prevent it. The exact timing of retinal damage to guide strategic
interventions remains unknown. We tested the hypothesis that repeated exposures of immature
retina to Intermittent Hypoxia (IH) simulating neonatal apnea-desaturations produce early
retinal damage and define key time points for pharmacologic intervention.
Methods: Newborn rats were exposed to IH
within 2 hours of birth (P0) until P14, or allowed to recover in room air (RA) from P14 to
P21 (IHR). Retinal integrity (by retinal flatmounts stained with ADPase,
fluorescein-dextran, GFAP for astrocytic template, retinal thickness) and angiogenesis
biomarkers (VEGF, sVEGFR-1, IGF-1) were progressively assessed before (P0), during IH (P7,
P14) and post IH recovery in RA (P21), or IH recovery-reperfusion (IHR) and compared to
normoxic age-matched controls.
Results: Retinal damage occurred as early as
day 3 of neonatal IH, consistent with vascular abnormalities and marked early pathology of
astrocytic template which worsened during IHR. IH-group showed retinal endothelial cells
penetrating the inner limiting membrane to violate the vitreous fluid as early as P1 and
worsening at P3.
Conclusions: Pharmacologic and other
interventions to prevent ROP should be started shortly after birth in high risk preterm
neonates. Drug screening using a 3-D scaffold human retinal endothelial cell cultures may
help identify effective and safe drugs for targeted clinical drug development to prevent
ROP. Early intervention may prevent or decrease severity of ROP and avert a lifetime of
blindness or visual impairment.
Postnatal temporal changes in thickness of retinal and nerve fi ber & ganglion cell
layer in room air and Intermittent hypoxia
Keywords: Retinopathy of Prematurity, oxygen
induced retinopathy, intermittent hypoxia, neonatal apnea, timing of retinal damage
Study of neonatal platelet function with PFA-100 in neonates of pregnancies complicated
with intrauterine growth restriction, gestational diabetes and perinatal hypoxia
Nicoletta M Iacovidou1, Theodora
Boutsikou1, Elina Isaakidou1, Vasiliki Mougiou1, Maria
Kollia1, Maria Boutsikou1, Rozeta Sokou1, Serena
Valsami2, Marianna Politou2
1Neonatal Department, Aretaieio Hospital, National and
Kapodistrian University of Athens
2Hematology Laboratory-Blood Bank, Aretaieio Hospital,
National andKapodistrian University of Athens
Introduction: PFA-100(Platelet Function
Analysis) is an in-vitro test that assesses platelet-related hemostasis(aggregation and
agglutination) by measuring Closure Times (CTs), which are decreased in healthy term
neonates vs adults. We hypothesized that certain high-risk neonates, prone to hemostatic
disorders, may present with compromised platelet function. We aimed at performing PFA-100 in
offspring of pregnancies with IUGR(Intrauterine Growth restriction), Gestational Diabetes
Melitus(GDM) and Perinatal Hypoxia(PH) and correlate the results withperinatal
parameters.
Methods: The study comprised of 179 umbilical
cord(UC) blood samples:43 IUGR, 53 GDM and 43 PH vs 40 from uncomplicated pregnancies
serving as control. COLEPI and COLADP cartridges were used as platelet activators providing
2 CTs for each sample.
Results: No significant differences in COLEPI
values were observed between each of the 3 groups vs controls. COLADP was significantly
lower in the GDM and PH vs control(b=-3.045, CI95%-5.841-(-0.249), p=0.033 and b=-3.773,
CI95%-6.033-(-1.514), p=0.001 respectively). In the IUGR group COLADP was significantly
increased in female neonates and decreased in vaginally delivered neonates (b=0.53, CI95%
0.010- 0.097, p=0.018, and b=-0.58, CI95% - 0.106-(-0.011), p=0.016, respectively. The lack
of difference in COLEPI between each group vs control could possibly be attributed to
variable compensatory mechanisms apart from platelet function, like increased hematocrit.
Platelet hyperreactivity commonly presenting in diabetes and hypoxia, could possibly explain
lower COLADP in the respective groups.
Conclusion: In IUGRs, COLADP prolongation in
female fetuses could be attributed to the inhibitory effect of estrogens on PLT aggregation;
the COLADP decrease in vaginally delivered neonates reflects PLT activation due to
documented cytokine elevation present during vaginal delivery.
Keywords: neonates, IUGR, IDM, PH, PFA-100
Clinical factors influencing endogenous carbon monoxide production in newborns
Jana Lozar Krivec, Darja Paro Panjan
Division of Paediatrics, Department of Neonatology, University Medical
Centre Ljubljana, Slovenia
Introduction: COHb is an index of endogenous
CO formation during heme degradation catalyzed by hemo-oxygenase-1 (HO-1). We previously
reported that COHb measured with CO-oximetry could be used to confirm hemolysis in newborns
with AB0 incompatibility. The influence of other clinical factors, which are reported to
upregulate HO-1, on COHb in newborns, has not yet been fully investigated. We aimed to
evaluate the influence of sepsis, respiratory distress and postnatal age on COHb
values.
Methods: We retrospectively analyzed COHb
measurements determined with CO-oximetry in term, less than 14 days old newborns, classified
into 4 groups: sepsis (A), respiratory distress (B), hemolysis (C), healthy newborns
(D).
Results: Overall there were 737 COHb
measurements performed in newborns during two-year period. 137 fulfilled the inclusion
criteria. The mean COHb values were 1.41% (SD0.26), 1.32% (SD0.27), 2.5% (SD0.69) and 1.27%
(SD0.19) in groups A (n=8), B (n=37), C (n=16) and D (n=76) (p<0,0005). Post hoc analysis
showed that COHb in Group C was significantly higher than in other groups, the differences
in COHb between groups A, B and D were not statistically important. There was a negative
correlation between postnatal age and COHb in healthy newborns. The cutoff level 1.7% had
93% (95%CI, 89-97%) sensitivity and 94% (95%CI, 90-98%) specificity for diagnosis of
hemolysis.
Conclusion: COHb in newborns with sepsis and
respiratory distress was higher than in healthy newborns, the differences were small and
statistically insignificant. COHb in newborns with hemolysis was significantly higher. The
COHb values are higher during first days of life.
Using measurements of ventilation/perfusion ratio to estimate the alveolar surface area
in prematurely born infants
Theodore Dassios
Neonatal Intensive Care Centre, King’s College Hospital NHS Foundation
Trust, London, UK
Introduction: Conventionally, the alveolar
surface area (Sa) has been measured by using post-mortem morphometry. Such studies have
highlighted that Sa in prematurely-born infants is markedly smaller when compared to
term-born infants as a result of postnatal impairment or arrest of alveolar development. We
herein explore how, non-invasive measurements of the ventilation/perfusion ratio (Va/Q) can
be used to estimate Sa in prematurely-born surviving, convalescent infants. We also compare
Sa in prematurely-born infants measured at term-corrected age, to term-born infants using
previously published datasets of Va/Q.
Methods: Fick’s first law of diffusion is
employed for the conversion of Va/Q measurements to Sa values after correcting for
differences in pulmonary perfusion (Q), thickness of the respiratory membrane (d) and
alveolar-arterial gradient (AaG).
Results: Using the dodecahedral structure to
estimate the alveolar shape we develop a mathematical formula to correct for differences in
the thickness of the respiratory membrane between term and prematurely-born infants studied
at term. We correct for differences in pulmonary perfusion and alveolar-arterial gradient
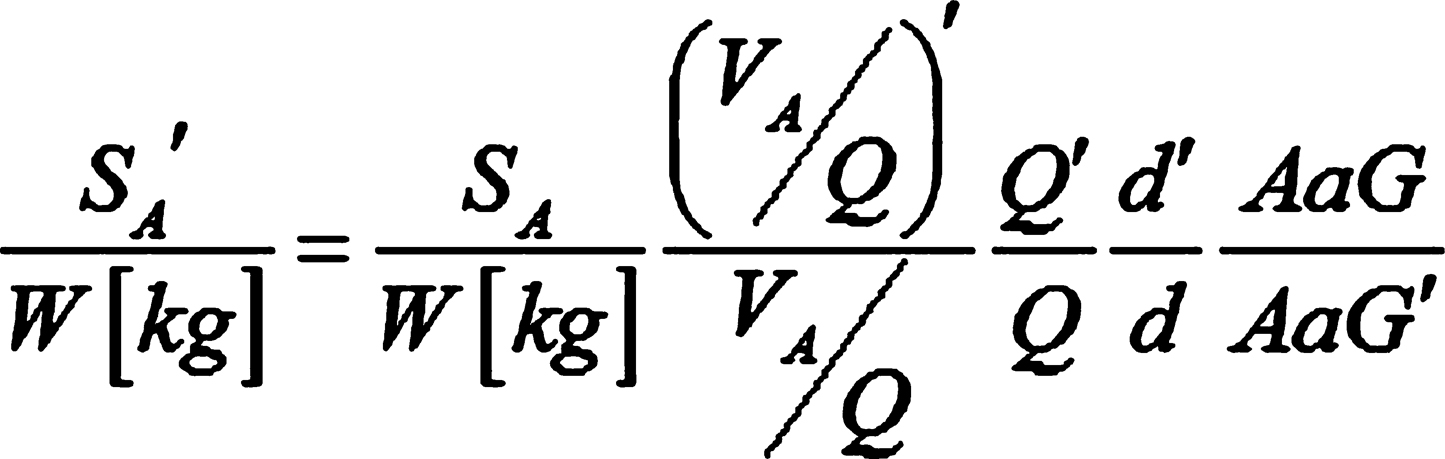
using previously published datasets. We present a generic equation to estimate the Sa in
prematurely born infants studied at term (figure 1). Using previously published datasets we
report that Sa is fivefold smaller in prematurely-born compared to term-born infants.
Conclusions: We conclude that non-invasive
measurements of Va/Q can be used for the functional estimation of Sa which could, in turn,
be used as a future outcome measure in respiratory studies of prematurely-born infants.
Keywords: alveolar surface area, premature infants,
alveolar development
The equation used to estimate the Sa. Primed variables are used for prematurely born
infants studied at term and unprimed symbols for term infants.
Combined use of probiotic Lactobacillus rhamnosis GG and vitamin D in very low birth
weight infants
Department of Neonatology, University Hospital of Obstetrics and
Gynecology,Maichin dom’’, Faculty of Medicine, Medical University of Sofia, Bulgaria
Introduction: Probiotic supplementation can
improve intestinal function in premature newborns and can be potentially beneficial to their
health.
Objectives: To monitor the
clinical,microbiological safety and tolerance of the probiotic Lactobacillus
rhamnosisGG+D3 in VLBWinfants and evaluate their vitamin D status.
Materials: A prospective study was carried out
from July 2017 to February 2018 at Neonatology Clinic,University O&G hospital“Maichin
dom”.The study included 25 newborns with average gestation age 30g.w. and average birth
weight 1170 gr.Levels of 25OH-D have been measured at 10thday and 8thweeks,biochemical
markers of bone metabolism (calcium, phosphorus, alkaline phosphatase,parathormone) and
microbiological specimens (nasal, pharyngeal, and anal)at ten-day intervals.According to the
blood levels vitaminDstatuswas defined as:normal>50nmol/l,insufficiency30-50nmol/l,and
deficiency<30nmol/l.The intake of probiotic started of mean 13thday in a dose of 7
drops,containing L.rhamnosusGG1.4x109CFU/d+400IU/D3.The newborns received an
additional dose D3500IU to a total dose of 900IU/d.
Results: At 10th day 72%VLBW infants have
normal 25OH-D levels 85,7 ± 2,5nmol/l, 16% with insufficiency35±19,3nmol/l, and 12% with
deficiency21,5±7,4nmol/l.At 8thweek, normal values of 25OH-D were maintained at 84% of
infants 85,1±35.5nmol/l.Vitamin D insufficiency was found in 16% of patients
43,2±4,4nmol/l.The biochemical bone markers were within normal limits.Average duration of
probiotic Waia-Lactobacillus rhamnosis GG+vitamin D is 36 days.The infants showed good
tolerance of enteral feeding and ascending weight curve.Asymptomatic carrier of pathogenic
intestinal flora(Klebsiella pneumonie ESBL+,Enterobacter aerugenosaESBL+,E.coliESBL+)was
observed after the 20thday in 48% of patients.There is lower colonization with Candida in
20%of infants at the end of the period.NEC and late neonatal sepsis have not been
established.
Conclusions: The administration of a probiotic
containing Lactobacillus rhamnosisGG+ vitamin D in VLBWinfants is microbiologically safe and
clinically well tolerated.
Do we give sufficient amounts of vitamin D to preterm infants?
Sophie Greim, Helmut Küster
Neonatology, University Medical Center Göttingen, Germany
Introduction: Vitamin D is given to every
newborn and it may have multiple benefits well beyond neonatal age. Recommended doses vary
and are independent of patient’s current weight. Vitamin D3 levels can be measured but this
is not standard of care and normal levels have not been agreed on.
Methods: Prospectively we measured every two
weeks vitamin D3 levels in all preterm infants with alkaline phosphatase >500 U/L and
adapted vitamin D supplementation to achieve a vitamin D3 level of 60 to 100 μg/L.
Results: Between January 2013 and December
2015, 194 patients had at least one vitamin D3 level measured. After exclusion of 16
patients with incomplete datasets, 178 datasets were used for analysis: mean gestational age
29±3 weeks, birth weight 1191±517 g, 55 % male, 19 % small for gestational age; 3 % had
necrotizing enterocolitis, 6 % nephrocalcinosis, only one infant died having trisomy 18. Up
to 2500 IE vitamin D were needed to achieve the desired vitamin D3 levels (mean 56 μg/L). A
level >60 μg/L was never achieved in 57 %, 21 % had at least one value >100 μg/L.
Logistic regression analysis revealed oral vitamin D supplementation to be the most
important early factor of influence for Vitamin D serum level (ROC 0.75).
Conclusion: Appropriate vitamin D3 levels are
not achieved in almost 2/3 of a population individually supplemented with up to 2500 IE
vitamin D. Higher than currently recommended doses of vitamin D seem to be needed,
especially for very preterm infants.
Keywords: Vitamin D, alkaline phosphatase, preterm
infants; nutrition, NICU
Tools and toys to study neonatal clinical pharmacology
Karel Allegaert
Department of Development and Regeneration, KU Leuven and Division of
Neonatology, Erasmus MC-Sophia Children’s hospitals, Rotterdam
Introduction: Neonates are not just small
children. Consequently, targets or biomarkers should be explored on their relevance in
neonates.
Methods: recently conducted studies on
vancomycin protein binding (AUCtotal target 400, converted to trough level of 10-15 mg/l)
and on the systemic and cerebral hemodynamics of propofol for endotracheal intubation will
illustrate the need to fully consider the neonatal physiology and setting when assessing the
targets or (side)- effects of drugs in neonates.
Results: Median total and unbound vancomycin
concentrations in 37 neonatal plasma samples were 14.25 (7.42-20.62) and 13.63 (7.17-22.47)
mg/L, respectively. Median unbound fraction was 0.90, higher compared to children (0.81) and
adults (0.62). This means that the adult AUCtotal of 400 reflects an AUCfree of 248. When
this target is converted to the newborn, the AUCtotal in neonates might be 275 (0.9 x 248)
instead of the 400 target generally aimed for. In a study on PK/PD of propofol in 22
neonates, intact cerebral autoregulation during permissive hypotension in the majority of
cases was observed, accompanied by decreased cerebral metabolism. However, some cases
displayed impaired autoregulation, despite the absence of systemic hypotension.
Conclusions: Integration of protein binding in
future pharmacokinetic/pharmacodynamics (PK/PD) analyses is needed to determine
population-specific vancomycin PD targets for neonates, while simultaneous collection of
data on systemic and cerebral hemodynamics confirm that systemic hemodynamics do not fully
reflect the cerebral hemodynamics. We hereby illustrated the need to fully consider the
neonatal PK/PD when assessing the targets or (side)- effects of drugs in neonates.
Keywords:Tools, toys, clinical pharmacology
Determination of fetal age and date of delivery
Dag Bratlid
Department of Health Administration and Health Economics, Institute of
Health and Society, Faculty of Medicine, University of Oslo, Norway
Introduction: Ultrasound (US) has gained a
dominating position for determination of fetal age and expected date of delivery (EDD).
Determination of fetal age by US has, however, significant flaws (1,2) as illustrated by the
following pregnancy history (3). Patient FAL had a regular menstrual history. From
biological parameters last menstrual period; positive ovulation test; date of conception;
and missed next period, EDDb was 14.2.2017. EDDus from biparietal diameter (BPD), crown-rump
length (CRL), and femur length (FL), varied from 28.2, 25.2 and 20.2, respectively. History
Despite significant discrepancies between EDDb and EDDus, as pointed out by the parents, EDD
was set at 28.2 based on BPD measurements according to advocated routines. At follow-ups on
20.1. and 3.2.2017, breech position was detected, and LAF was scheduled for turning of the
fetus on February 6. However, on February 4, membranes ruptured and delivery was imminent.
CT showed pelvis measurements too small for breech delivery, and c-section was performed.
The girl weighed 3160 gram, head circumference 36 cm and length 46 cm. Due to medical
complications after c-section, postnatal stay was 11 days
Discussion: Fetal US like BPD, CRL and FL
results in different EDDus and also have large variations from mean. These technologies are
therefore not better than a “correct” EDDb.
Conclusions: Negligence of EDDb can be harmful
for mother and infant. If EDDb had been considered, breech position could have been
corrected and c-section avoided with a better start for mother and infant.
Bratlid D Determination of birth term by early
ultrasonic examination--wrong, wrong and wrong again?. Tidsskr Nor Laegeforen.
1991:111:1379-81.
Bratlid D Estimating date of delivery
and gestational age - technology, biology or both? Tidsskr Nor Legeforen 2016;
136:1332.
Breast milk: to each his own. From nature the evidence of personalized
nutrition.
Serafina Perrone1, Mariangela
Longini1, Federica Lotti1, Fabrizio Proietti1, Francesco
Bazzini1, Maria Tassini2, Antonio Vivi2, Serena
Rossi1, Marco Calderisi3, Giuseppe Buonocore1
1Department of Molecular and Developmental Medicine,
University of Siena, Siena, Italy
2NMR Center, University of Siena, Siena, Italy
3Kode-solutions, Pisa, Italy
Introduction: Human milk is the best
nourishment for the healthy growth and development of infants. The composition of preterm
milk is pretty different from the full term milk. The aim of this study is to test the
hypothesis that milk metabolic profile from mothers delivering prematurely changes over time
never resembling milk from mothers delivering at term.
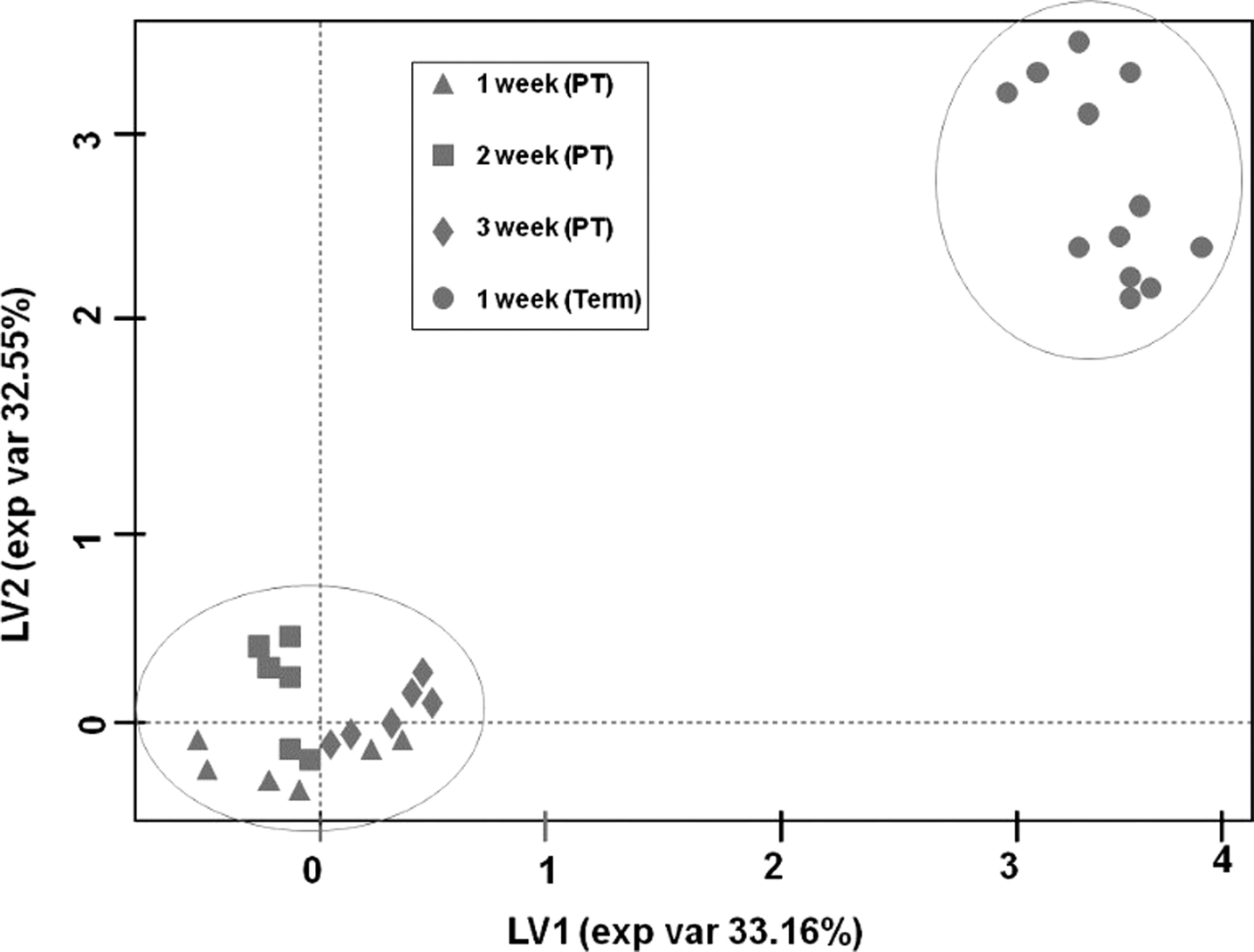
Methods-results:. 12 term milk samples,
collected once at 7 days after birth, were compared to 18 preterm milk samples, collected
weekly after delivery until the 4th week after birth. Metabolome pattern of all milk samples
was analyzed. Principal Component Analysis (PCA) showed two distinct metabolites groups, one
represented by the 18 preterm milk samples, and the other by the term milk samples (Fig 1).
Lactose and oligosaccharides levels were significantly more represented in preterm than in
milk term samples.
Conclusions: Preterm milk metabolome profile
changes during the first 4 weeks after birth, but does not resemble the term milk pattern.
The specific changes in preterm milk metabolic profile reflect the different nutritional
requirement of preterm infants. This knowledge is crucial to move from standardized
nutritional protocols to a tailored nutrition.
Keywords: Preterm milk
Increased plasma concentrations of NPBI in cord blood predict IVH in preterm
newborns.
Serafina Perrone, Antonino Santacroce, Maria
Luisa Tataranno, Simona Negro, Mariangela Longini, Fabrizio Proietti, Francesco Bazzini,
Anna Picardi, Giuseppe Buonocore
Department of Pediatrics, Obstetrics and Reproductive Medicine,
University of Siena, Italy.
Introduction: Intraventricular hemorrhage
(IVH) predispose to long-term neurologic disability in preterm infants. Oxidative stress
(OS) is a major risk factor in the pathogenesis of IVH. Non-protein bound iron (NPBI), a
reliable markers of OS, was reported to be related to poor neurodevelopmental outcome. We
test the hypothesis that NPBI concentrations in cord blood may predict IVH development in
preterm infants.
Methods: NPBI was measured in arterial cord
blood of 221 preterm newborns (GA = 32 weeks). According to the cerebral ultrasonography
findings during the first 48 hours of life, the population was divided in IVH group (n=80)
and non-IVH group (n=141). SPSS package was use for statistical analysis.
Results: IVH group had a lower GA (28.58±2.12
VS 29.6±2.02; p<0.001) and higher cord blood levels of NPBI (2.81±5.6 VS 1.23±2.37;
p=0.006) than the non-IVH group. A binomial logistic regression analysis showed the
significant relationship between NPBI and IVH (B=1.112, CI 95% 1.014-1.219; p=0.024). GA was
protective against IVH onset (B=0.802, CI 95% 0.699-0.921; p=0.002).
Conclusion: Cord blood NPBI concentrations are
increased in preterm newborns who develop IVH and may be useful for the identification of
the risk for IVH before the appearance of related biophysical signs. Data also suggest the
need of investigation about antioxidant strategies in perinatal period.
Keywords: plasma concentrations, NPBI, IVH
Early detection of developmental dysplasia of hip by ultrasound
Zita Gyurkovits1, G.
Sohár2, A. Baricsa2, G. Németh1, H. Orvos1, B.
Dubs1
1Department of Obstetrics and Gynaecology, University of
Szeged, Hungary
2Department of Orthopaedics, University of Szeged,
Hungary
Introduction: The aim of the study was to
assess the effectiveness of early universal ultrasound screening of developmental dysplasia
of the hip performed in the first days of life.
Methods: A prospective study of universal hip
screening and treatment of all mature neonates was conducted during a one-year period at the
Department of Obstetrics and Gynaecology, University of Szeged; 1636 newborns (3272 hips)
had clinical examinations and sonographic tests with the Graf-technique, within the first
three days of life. The incidence of DDH, risk factors, sensitivity and specificity of
clinical examinations of the universal screening model were evaluated.
Results: At the first US examination 55 of
1636 newborns (3.36%) had either unilateral or bilateral hip dysplasia; in terms of hips
2.14% were positive. All newborns had physical examination: 67 of 3272 hips (2.05%) were
Barlow or Ortolani positive, but among 67 hips, 14 (20.8%) were US positive, the remaining
(79.2%) were declared negative according to the standard method of US. Taking into
consideration the risk factors, female gender, breech presentation and positive family
history proved to be significant. Interestingly, of the 55 newborns with DDH, 28 (50.90%)
had neither positive physical signs nor any risk factors, except being a girl.
Conclusion: Universal US screening of the hip
in the first days of life reduced the need of operative procedures remarkably, compared to
the previously applied selective protocol. Physical examination proved to have low
sensitivity.
Keywords: Developmental dysplasia of the hip,
neonatal screening, ultrasonography
Antenatal factors and cognitive development at school age in very preterm children:
results from the Italian ACTION area-based cohort
Marina Cuttini, Lena Herich, Ileana Croci,
Action Study Group
Pediatric Hospital Bambino Gesù, Rome, Italy
Introduction: Survival of very preterm (VP)
infants has improved in the last decades but disability rates are still high, particularly
below 28 weeks of gestational age (GA).
Methods: We assessed health and cognitive
development at school-age (8-11 years) in a prospective area-based cohort of VP children (GA
<32 weeks) in three Italian regions (Lazio, Tuscany and Friuli Venezia-Giulia). Cognition
(Mental Processing Index, MPI) was measured using the Kaufmann-ABC, second edition. A total
of 804 children were recruited (response rate 70.4%). We used multilevel multivariable
Poisson regression to explore the relation between antenatal factors and below average MPI
(<85). Region was included in the model as random effect.
Results: Cognition was assessed in 730
children; 140 (20.4%) had MPI<85. Rates were higher (27%) for those born below 28 weeks
of gestational age (GA). Other variables significantly associated with below average MPI in
multivariable analysis were male gender, possibly homozygous multiple birth, intrauterine
growth retardation, presence of congenital anomalies, signs of prenatal infection, smoking
in pregnancy and younger (<24 years) maternal age. Higher maternal education appeared
protective.
Conclusions: Several biological, medical and
socio-demographic antenatal factors may influence long-term cognitive development in very
preterm infants. Further analyses will be necessary to assess the role of postnatal
variables in the causal chain leading to long-term cognitive outcome.
Keywords: Antenatal factors, cognitive
development
Effect of angiotensin converting enzyme gene polymorphism on respiratory muscle
function and exercise capacity in childhood: preliminary results
G. Dimitriou, A. Vervenioti, S. Fouzas
Neonatal Intensive Care Unit, Department of Paediatrics, University
Hospital of Patras, Greece
Background: It has been suggested that the
I-allele of Angiotensin Converting Enzyme (ACE) gene is associated with superior exercise
endurance in adults. We have previously shown that the I/I ACE genotype is also associated
with increased respiratory muscles (RM) effectiveness in neonates. In this study, the
relationship between ACE gene polymorphism, RM function, and exercise capacity in childhood
has been investigated.
Methods: Twenty one children born at a mean
gestational age (GA) of 35.6 weeks underwent RM function measurements and cardiopulmonary
exercise testing at the age of 6 to 7 years. The pressure-time index of RM (PTimus) was
calculated by the formula (Pimean/ Pimax) x (Ti/Ttot), where Pimean and Pimax are the mean
and maximal inspiratory pressure, respectively, and Ti/Ttot is the respiratory duty cycle.
Exercise capacity was assessed by means of maximum oxygen consumption (VO2max) using a
cycle-ergometer protocol. ACE genotyping was performed using DNA from peripheral blood. None
of the participants had a history of current asthma.
Results: Children with I/I genotype (N=3) had
lower PTimus and higher VO2max compared to those with I/D or D/D genotype (N=18) (PTImus
0.063 ±0.006 vs. 0.096 ±0.017, P=0.005; VO2max 51 ±6 ml/kg/min vs. 33.4 ±6 ml/kg/min,
P<0.001). In a stepwise multivariable regression model, the I/I genotype was the only
significant determinant of both PTImus (coefficient 0.557; P=0.004) and VO2max (coefficient
0.734; P<0.001), independently of the effect of GA, sex, BMI and lung function at school
age.
Conclusions: ACE gene polymorphism influences
the RM function and determines the exercise capacity in childhood.
Keywords: ACE, gene polymorphism
Use of specialist health services and costs during the first two years of life in
Estonian cohorts of very preterm infants
Liis Toome1, Anna Veera
Seppänen2, Raul Allan Kiivet3, Helle Visk3, Heili
Varendi4
1Clinic of Pediatrics, Tallinn Children’s Hospital, Tallinn,
Estonia; Department of Pediatrics, Institute of Clinical Medicine, University of Tartu,
Tartu, Estonia
2Obstetrical, Perinatal and Pediatric Epidemiology Research
Team (Epopé), INSERM U1153, Paris, France
3Department of Public Health, Institute of Family Medicine
and Public Health, University of Tartu, Tartu, Estonia
4Children’s Clinic of Tartu University Hospital, Tartu,
Estonia; Department of Pediatrics, Institute of Clinical Medicine, University of Tartu,
Tartu, Estonia
Introduction: Very preterm infants (VPI)
require more health services than term infants in their childhood because of the health and
neurodevelopmental risks associated with prematurity. No evidence-based guidelines exist on
use of the specialists to follow up VPI. However, these services might have an impact on the
health care quality and costs. The aim of the study was to describe medical specialist
service use by VPI in Estonia after the introduction of national follow-up guidelines and
the influence of systematic follow-up on the health care costs until two years of age.
Methods: Data on medical specialist use come
from the EPICE cohort of births before 32 gestational weeks in 11 European countries. In
Estonia, data for 138 VPI (98% of survivors at discharge) were collected through the parent
questionnaire at two years of corrected age. Health service costs during the first two years
of life were derived from the Estonian Health Insurance Fund for 2002–2003, 2007–2008 and
2011–2012.
Results: National follow-up guidelines for VPI
were introduced in 2008. Of VPI born in 2011–2012, all were followed up by a pediatrician,
99% by an ophthalmologist, 96% by a physiotherapist and 42% by a developmental psychologist.
The total health care costs did not increase over time from 2002–2003 to 2011–2012.
Furthermore, rehospitalisations during the first year of life decreased significantly
between cohorts (66%, 54%, 40%).
Conclusions: The Estonian experience shows
that the systematic follow-up of VPI might decrease the rehospitalisation and not
necessarily increase the costs.
Keywords: Very preterm infants, specialist health
services, follow-up, health service costs
Improvement of the 5-year outcome of live births with extremely low birth weight
(<1000 g) in Estonia
1Children’s Clinic of Tartu University Hospital, Tartu,
Estonia
2Clinic of Pediatrics, Tallinn Children’s Hospital, Tallinn,
Estonia
3Department of Pediatrics, Institute of Clinical Medicine,
University of Tartu, Tartu, Estonia
Introduction: Survival of very preterm infants
(22+0–31+6 gestational weeks, GW) has increased from 78% in 2002–03 to 92% in 2011–2012 in
Estonia that can bring along neurodevelopmental impairment (NDI) and health problems in
survivors due to extreme prematurity. We assessed the 5-year unfavourable outcome of the
national cohorts of children born alive with birth weight (BW) <1000 g and gestational
age 22+0–28+6 GW in Estonia between 2002–2012.
Methods: At 5 years, child development and
health of Estonian national cohorts born in 2002–2003, 2007 and 2011–12 (EPICE study) was
assessed using Kaufman ABC or WPPSI-IV; Movement ABC tests, or by interviewing the parents
(SHIPS study) with follow-up rate as 100%. The severe NDI (cerebral palsy without walking
with aids, deafness, blindness or mental development below -3 SD) and death were considered
as unfavourable outcome.
Results: Five-year survival of extremely low
birth weight infants born before <29GW has increased from 42.5% to 80 % in Estonia within
the 10-year study period. Unfavourable outcome of live births at 5 years has decreased from
62.5% to 20% (p < 0.05). Among survivors from the last period, EPICE study group, there
were no children with severe NDI but boys performed in all domains of assessed developmental
skills with significantly lower scores than girls.
Conclusion: The outcome of Estonian national
cohorts of live-born infants with BW <1000 g and <29GW, has improved within 2002–2012
with no severe NDI at 5 years of age in the last cohort.
Reference values of cranial volume – Chance to monitor postnatal head growth in preterm
infants
Marjin J. Vermeulen1, Dimitrios Konstantelos2,
Sascha Ifflaender2, Jorine A. Roelants1, Jürgen
Dinger2, Mario Rüdiger2, Wolfram
Burkhardt2
1Department of Neonatology and Pediatric Intensive Care
Medicine, Clinic for Pediatrics, Medizinische Fakultät der Technischen Universität
Dresden
2Erasmus MC, University Medical Center Rotterdam,
Netherlands
Introduction: Neurodevelopment of preterm
infants depends on postnatal brain growth, which is commonly estimated by head circumference
(HC). However, HC poorly correlates to cranial volume (CrV).1 3D-Scanners
represent a non-invasive and easy method to measure CrV. This study aimed to generate
percentiles and reference charts for cranial volumes for postnatal brain growth monitoring
in preterm infants.
Methods: CrV was measured using 3D-Laserscaner
(STARScanner, Orthomerica, Orlando, FL, USA)1 within the first 5 days of life in
all infants born in our institution, measured between 34-43 weeks post-conceptionally.
Newborns were excluded in case of intensive care treatment, congenital (skull) malformations
or cerebral injury. CrV-percentiles were calculated by gestational age (GA), by birth weight
(BW) and by HC for the total group and boys and girls separately.
Results: A total of 1893 newborns (49% female)
were studied. Median GA was 39.4 [IQR 38.3-40.4] weeks, BW 3310 [2898-3650] g, HC 35.0
[34.0-36.0] cm, length 51.0 [49.0-52.0] cm. Median CrV was 423 [383-457] cm3 and
was lower for girls than for boys (mean difference 26.4 cm3, p<0.001 adjusted
for gestational age). Median cranial volume increased from 307 [286-331] at 34 weeks to
433.5 [406-462] cm3 at 40 weeks, with growth decreasing from 18
cm3/week at 34 weeks to 13 cm3/week at 40 weeks.
Conclusion: This study presents the first
percentiles of normal CrV in newborns born between 34 to 42 weeks of gestation. The provided
cranial volume reference charts can be used to monitor head growth in late preterm
infants.
Early versus conservative treatment: Preliminary data of the national registry on
treatment option and its timing in patent ductus arteriosus
Ömer Erdeve1, Emel
Okulu1, Begum Atasay1, Saadet Arsan1, On Behalf Of
Interpda Study Group2
1Division of Neonatology, Department of Pediatrics, Ankara
University School of Medicine, Ankara, Turkey
2INTERPDA Trial Group, Turkey
Introduction: Regarding to the management of
patent ductus arteriosus (PDA) in preterm infants, no consensus on which PDA to treat, when
to treat, or how to treat has been reached. A prospective, multicenter (22 units) trial has
been conducted to compare the effects of conservative approach and early medical treatment
options on ductal closure, surgical ligation, prematurity related morbidities and mortality
in Turkey.
Methods: Infants with 24 0/7-28 6/7 gestation
weeks were enrolled and their PDA management data were recorded through an online registry
system.
Results: Among 497 enrolled infants (with mean
gestational age of 26.8±1.3 wk and mean birthweight of 926±232 g), 31% (n=155) had no PDA,
whereas 19% (n=94) had small PDA and 50% (n=248) had moderate-to-large PDA. 31% (n=107) of
infants with PDA were managed conservatively in contrast to 69% (n=235) who received
treatment at a mean age of 4.6±4.4 days. Prefered treatment options were ibuprofen
(oral;36%, iv; 35%) and paracetamol (iv;23%, oral;6%). 23% (n=25) of conservatively managed
infants required rescue treatment during the hospitalization. The rates of sepsis,
necrotizing enterocolitis, retinopathy of prematurity, bronchopulmonary dysplasia and the
length of hospitalization were similar between conservatively managed and treated infants
(p>0.05), and no difference with treatment drugs were observed. Infants who were
medically treated had higher surgical ligation (p=0.029) and home oxygen treatment (p=0.002)
rates, whereas conservatively managed infants had a higher mortality rate (p=0.000).
Conclusion: Early medical treatment of PDA
could not decrease the rate of surgical ligation but mortality was higher in conservatively
managed infants.
Early postnatal care and gender impacts infant vaccination status in rural
India
Sebastian Horn1, Mareike
Schön1, Cara Ebert2, Esther Heesemann2, Sebastian
Vollmer2
1Department of Pediatric Cardiology, Neonatology and
Intensive Care, University Hospital Medical Center, Georg-August-University Göttingen,
Göttingen, Germany
2Center for Modern Indian Studies, Georg-August-University
Göttingen, Göttingen, Germany
Introduction: Despite recent advances in
reducing newborn and infant mortality up to 40% of all newborn in low- and middle-income
countries are at risk of dying within the first month of life or encounter a faltered early
childhood development. Providing access to effective newborn care and early postnatal
measures is known to improve the odds for a healthy development.
Methods: Questionnaire-based surveys have been
conducted as well as sampling of anthropometric and early childhood development data of
about 2000 families in 2016 and 2017 in Madhepura district, state of Bihar, India. Data
sampling was performed with help of local enumerators using electronic data acquisition with
CSPro®. Data analysis was performed using R® and Stata® software packages.
Results: Across all holders of vaccination
cards completeness of vaccination status for newborn and infants at various time points was
assessed. An incomplete vaccination status can be seen as a proxy for an increased risk for
infection and poor development. Although vaccination within 24 hours seems equally performed
gender wise with an OR (odds ratio) of 1.023 (1=male, 0=female, n=931, p=0.883) at the age
of 31/2 months female infants tend to have a less complete vaccination status with an OR of
1.379 (n=931, p=0.019). Vaccination schemes are varying along national board recommendations
hence we assessed vaccination completeness according to the National Swedish Vaccination
Scheme.
Conclusion: Given the impact of a simple
public health measure like vaccination it seems imperative to be aware of gender driven
biases which will lead to defective health and development.
Keywords: early childhood development, vaccination,
postnatal care, infant health, gender
Hydrocortisone (hc): efficacy and outcome at 18-22 months in ventilated infants < 28
weeks ga.
K A Nguyen, J. Bartholomew, A.
Papageorgiou
Jewish General Hospital, McGill University, Department of Neonatology,
Montreal, Quebec, Canada.
Introduction: HC has shown promising results
in the prevention of BPD. However, the long term outcome is still under investigation.
Methods: We report response in 138 ventilated
infants <28 weeks GA treated in our NICU. We also report follow-up at 18-22 months of 45
infants who received HC to 93 infants who did not receive HC. The total amount of HC that
each infant received was 45 mg/Kg, with the exception of those who received a second course,
making a group average of 57.02 mg/Kg.
Results: FIO2 requirements and mean airway
pressure leading to extubation were dramatically improved, while BP and blood sugar remained
normal. The Bayley III scores at 18-22 months indicated no difference between the 45 infants
treated with HC and the 93 infants who were not treated with HC in cognition 94.9 vs 96.3,
language 87.3 vs 89.3, motor scores 93.3 vs 97.0, hearing 2,2 vs 0.00, cerebral palsy 4.4 vs
2.2, and ROP 0 vs 0.
Conclusion: Based on our protocol, treatment
with HC had no impact on neurodevelopmental outcome at 18-22 months on ventilated preterm
infants compared to those non treated, while a significant improvement was noted on their
respiratory parameters in the NICU. Our next evaluation will be done at 4½ years of age.
Keywords: hydrocortisone, BPD, Bayley III
scores
Comparison of three different non-invasive ventilation modes in preterm infants with
respiratory distress syndrome: prospective randomized study
Merih Cetinkaya1, Burcu
Cebeci2, Seda Yilmaz Semerci1, Dilek Kurnaz1, Özge
Saglam1
1Health Sciences University, Kanuni Sultan Suleyman Training
and Research Hospital, Department of Neonatology, Istanbul, Turkey
2Health Sciences University, Haseki Training and Research
Hospital, Department of Neonatology, Istanbul, Turkey
Introduction: Non-invasive respiratory support
has been increasingly used for early management of respiratory distress syndrome (RDS) as an
alternative for intubation and mechanical ventilation. The aim of this study was to compare
the effects of nasal intermittent positive pressure ventilation (NIPPV), nasal continuous
positive pressure (nCPAP) and high flow nasal canula (HFNC) for initial treatment of RDS in
preterm infants.
Methods: Preterm infants admitted to NICU with
RDS were randomized into: NIPPV vs. nCPAP vs. HFNC. The primary outcome was the need of
intubation within 72 hours of life. The secondary outcomes were duration of respiratory
support, duration of total oxygen, death, air leaks, and frequency of neonatal morbidities
including bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP),
intraventricular hemorrhage (IVH), patent ductus arteriosus (PDA), necrotizing enterocolitis
(NEC) and sepsis.
Results: A total of 60 infants were randomized
to NIPPV, nCPAP and HFNC. All groups were similar with respect to demographical features. No
significant differences were detected between 3 groups in terms of the need for intubation
within the first 72 hours of life, the incidences of BPD, ROP, IVH, NEC, sepsis, and air
leaks. The duration of respiratory support was significantly higher in HFNC group compared
with other groups (p=0.002).
Conclusion: Although NIPPV, NCPAP and HFNC
showed similar efficacy for prevention of intubation, HFNC group had higher duration of
ventilation peiod that may limit its usage. Therefore, we suggest that NIPPV and NCPAP may
be preferred as initial respiratory support modes in preterm infants to shorten the duration
of ventilation.
Reducing preventable harm: attitudes towards patient safety in an irish tertiary
neonatal unit
David Corcoran1, Liam
Dwyer2, Aishling Smith3, Colm Breathnach3
1Trinity College Dublin
2Royal College of Surgeons in Ireland
3Rotunda Hospital Dublin
Introduction & Aims: Crew Resource
management is widely used in aviation and is proven to be effective in reducing accidents.
There is little published research investigating interventions to improve safety culture in
neonatal units. This study aimed to explore the safety culture that exists within a level
III Irish neonatal unit in order to identify areas for potential improvement.
Methods: This was a quantitative,
cross-sectional study performed in the Rotunda Hospital, Dublin. A 30-item safety attitudes
questionnaire (SAQ) was utilizedto analyze staff perceptions in areas including job
satisfaction, working conditions and stress recognition. The scores were transformed into a
numerical 100-point scale (Positive score >75).
Results: The ‘Stress Recognition’ domain
received the highest score (75.3) followed by ‘Job Satisfaction’ domain with a mean score of
74.4. The lowest mean scale score in the neonatal unit was for ‘Perceptions of Management’,
with a mean score of 50.7.Collaboration and Communication scores were high across all
disciplines.
Conclusion: This SAQ has highlighted a number
of important areas for quality improvement and staff satisfaction in our neonatal unit.
Keywords: patient safety, attitudes, survey,
neonatal intensive care
Blood Glucose Fluctuations in Preterms After Reaching Full Enteral Nutrition
Division of Newborn Medicine, Gazi University, Ankara, Turkey
Introduction: Blood glucose homeostazis is
only reached after the first few days of life in the preterm newborn. It is usually assumed
that preterms have stable glucose levels within normal limits once they are on full enteral
feeds. The aim of this study is to investigate whether this is true by measuring blood
glucose at fasting and after feeding.
Methods: Preterms born = 32 weeks gestation
were included after reaching full enteral feeding volume of 180ml/kg with fortified breast
milk given at 3 hourly intervals. Blood glucose was measured with glucosticks before feeding
and 1 hour after feeding at 3 occasions each. Normal blood sugar levels were accepted as
between 70-120 mg/dl and low and high levels were defined based on these values.
Results: Eighteen preterms were included with
median BW: 1192 g (630-1930 g) and gestational age 31 weeks (26-32 weeks). Full enteral
nutrition was reached at median 12 days and 32 weeks gestation. Total of 62 fasting and 62
postprandial glucose measurements were made. During fasting, hypoglycemia was observed in 13
% and hyperglycemia was observed in 3 % of measurements. Postprandially hypoglycemia was
observed in 8 % and hyperglycemia was observed in 22.5 % of measurements.
Discussion: This is a pilot study
investigating the glucose homeostazis in preterms who are on full enteral feeds. Even in
this small group hypo and hyperglycemia has been observed frequently both during fasting and
postprandial periods. More studies performed with larger groups are needed.
Neonatal consequences of non-diabetic hyperglycemia during pregnancy
A. Kazancioglu1, E.
Koc1, P. Calis2, M. Bayram2, I. M.
Hirfanoglu1, E. Onal1, C. Turkyilmaz1, E.
Ergenekon1
1Gazi University, Division of Neonatology, Ankara,Turkey.
2Gazi University, Department of Obstetric and Gynecology,
Ankara,Turkey.
Introduction: It is controversial whether
maternal hyperglycemia less severe than that in diabetes mellitus is associated with
increased risks of adverse pregnancy outcomes. The aim of the study is to assess adverse
outcomes of infants of mothers whose glucose intolerance are less severe than overt diabetes
mellitus.
Methods: A total of 205 pregnant women
underwent 75 gr oral glucose tolerance testing between 24-28. gestational weeks were
enrolled. Infants of mothers with fasting glucose levels below 92 mg/dl, 1-h glucose levels
below 180 mg/dl and 2-h glucose levels below 153 mg/dl were evaluated prospectively. Primary
outcomes were birth weight above the 90th percentile for gestational age (LGA), primary
cesarean delivery, hypoglycemia. Secondary outcomes were delivery before 37 weeks of
gestation, birth injury and hyperbilirubinemia,
Results: The mean fasting, 1-hour, and 2-hour
plasma glucose levels were 76 ± 7.2 mg/dl, 116±27.3 mg/dl, and 99±21.3 mg/dl respectively.
LGA and primary ceserean delivery rates are significantly associated only with 1-h blood
glucose values (p:0.002, p:0.019). Blood glucose levels of the mothers were not associated
with hypoglycemia and hyperbilirubinemia (p> 0.05).
Conclusion: Our results indicate a significant
association of maternal glucose levels below those diagnostic of diabetes with increased
birth weight and cesarean delivery.
Keywords: hyperglycemia, pregnancy, newborn
Urinary Iodine Concentrations and Serum TSH, FT4 Levels in Neonates and Their Mothers
in a Mild-Deficiency Area
Gozde Apaydin1, Mehmet
Vural2, Olcay Evliyaoglu3, Fatih Aydin4,
Canan Kucukgergin4, Tugberk Bakar5, Yildiz Perk2
1Istanbul University, Cerrahpasa Medical Faculty, Department
of Pediatrics, Istanbul
2Istanbul University, Cerrahpasa Medical Faculty, Department
of Pediatrics, Division of Neonatology, Istanbul
3Istanbul University, Cerrahpasa Medical Faculty, Department
of Pediatrics, Division of Pediatric Endocrinology, Istanbul
4Istanbul University, Istanbul Medical Faculty, Department of
Biochemistry, Istanbul
5Istanbul University, Cerrahpasa Medical Faculty, Department
of Public Health, Istanbul
Background: Iodine is an essential element in
thyroid hormone synthesis and normal development of neurological system. Urinary iodine
concentration, serum TSH and FT4 levels can be appropirate indicators of body iodine status.
Aim of the study: The aim of this study was to determine the urinary iodine concentrations,
serum TSH and FT4 levels in neonates and their mothers to assess the nutritional iodine:
status.
Method: A cross-sectional voluntary screening
study was performed in Neonatology Unit in Cerrahpasa University Hospital. We collected
serum samples and spot urine samples from 102 neonates and their mothers. Urinary iodine
concentration (UIC) was calculated based on Sandell-Kolthoff reaction. Median urinary iodine
level <100 μg/L was considered as iodine deficiency.
Results: The median urinary iodine
concentrations in neonates and their mothers were 102,61 μg/L and 84,07 μg/L respectively.
41% of neonates and 49% of mothers had insufficient (<100 μg/L) urinary iodine
concentration (UIC). The median levels of serum TSH and FT4 for neonates and their mothers
were 12,31 mIU/L, 2,41 pg/dl; 2,26 mIU/L, 1,08 pg/dl respectively. 28% of neonates and 2% of
mothers had increased serum TSH levels.
Conclusion: Iodine deficiency with low urinary
iodine concentrations and high serum TSH levels was recognized among neonates and their
mothers in Cerrahpasa, Istanbul in spite of the programme of salt iodization. This study
suggests that national measures are required to correct iodine sufficiency with regular
iodine supplementation during the pregnancy in this region.