
Abstract
BACKGROUND:
The traditional Moroccan diet is typical of the Mediterranean diet (MD), but there have been few studies of the adherence of Moroccans adolescents to this diet and associated factors.
OBJECTIVE:
To evaluate MD adherence and its association with socioeconomic factors, nutritional status and dietary intake in a sample of secondary school pupils in the Rif region of Morocco.
METHODS:
In a cross-sectional study of a sample (n = 302) of Moroccan Riffian adolescents (13–18 years) from three secondary schools, we measured adherence to MD with the Mediterranean Diet Quality Index for children and teenagers questionnaire (KIDMED). A score below 8 was qualified as poor to average adherence to MD, while an optimal adherence was defined as a score of 8 or higher. Bivariate analyses and a logistic regression model were used to examine associations between adherence to MD and socioeconomic factors, nutritional status and dietary intake.
RESULTS:
Only 14.9% of adolescents had an optimal adherence to the MD (score≥8 points), 72.8% had average adherence (score 4–7) and 12.3% had poor adherence to the MD (score≤3). The factors associated with optimal adherence to MD were female sex (OR 2.28; 95% CI 1.07 –4.85; p = 0.031), high monthly family income > 8000 MAD (OR 7.10; 95% CI 1.52 –33.1; p = 0.013) and living in an apartment (OR 3.85; 95% CI 1.43 –10.3; p = 0.007). For others factors such as nutritional status and dietary intake, no associations were observed.
CONCLUSION:
We found a low level of adherence to the MD among adolescents in the Rif region, supporting the hypothesis that the dietary pattern of these Moroccan adolescents is in a transitional state characterised by a shift away from the traditional MD. The findings of this study suggest that interventions to optimize MD adherence should target boys, shared residences and lower income families.
Introduction
The traditional Moroccan food consumption model closely resembles the Mediterranean diet (MD) [1], considered to be one of the healthiest human dietary patterns, thanks to a combination of foods rich in anti-inflammatory and antioxidant compounds [2]. The MD not only fulfils all nutritional requirements [3], and helps to reach and maintain a healthy body weight [4], but is also associated with increased longevity [5], and a reduced risk of chronic disease, such as cardiovascular disease [6], type 2 diabetes [7], obesity [8], metabolic syndrome [9], certain cancers [4] and cognitive impairment [10]. Characterised by low consumption of red meat, processed meats and full-fat dairy products, the MD is nevertheless fat-rich due to the plentiful consumption of extra-virgin olive oil, with a high consumption of minimally-processed foods, cereals, legumes, locally grown vegetables, fruits and nuts. The moderate consumption of fish and shellfish, which varies depending on the proximity to the sea, is an important source of protein [11, 12]. Despite these advantages, the younger generations in most countries of the Mediterranean basin are not adopting or abandoning the diet [13]. Several studies have found high percentages of suboptimal adherence to the MD in teenagers: over 80% of school-age children and adolescents in Italy [14], with similar percentages in Spain, Turkey and Greece [15–17]. This phenomenon of dietary change has resulted in a nutritional transition, with a mounting prevalence of overweight, obesity and diet-related chronic diseases, which present new challenges for public health systems in Mediterranean countries [18]. Morocco is suffering from the consequences of this nutritional transition, which has progressed rapidly over recent decades [1], accompanied by profound changes resulting from growing urbanisation, economic development, globalisation and increased activity in the food processing industry [19]. Adolescents, more susceptible to the influences of advertising and the media on their behaviour and lifestyle, constitute a group of special interest. Furthermore, Moroccan adolescents have been found to show a lack of concern about the short-term negative health consequences of a poor diet [20–22].
In epidemiological surveys, different scoring methods have been devised and validated to assess the adherence of primarily adult populations to the MD: for example, the Mediterranean Adequacy Index (MAI) of Alberti-Fidanza et al. [23], the Mediterranean food pattern (MFP) of Martínez-González et al. [24], the Mediterranean diet scale (MD Scale) of Trichopoulou et al. [25] and the relative Mediterranean diet score (rMED) of Buckland et al. [26]. In previous Moroccan studies, researchers have applied two different scoring methods to assess the adherence of the adult population to the MD. El Rhazi et al. [27] and Mohtadi et al. [28] used a Simplified Mediterranean Dietary Score (SMD score). El Kinany et al. [29] developed a dietary score tailored specifically to southern Mediterranean populations, namely the Modified Mediterranean Dietary Score (MMD score). In southern Moroccan school-age children and adolescent populations, Anzid [30] and Azekour et al. [31] applied the Mediterranean Diet Quality Index (KIDMED). The KIDMED index was developed and validated by Serra-Majem and colleagues [32], and has been used since 2004 as a tool in nutrition research and assessment. The current study aimed to evaluate adherence to the MD in north Moroccan Riffian adolescents and its association with socioeconomic factors, nutritional status and dietary intakes.
Materials and methods
Participants and data collection
The cross-sectional study was designed to collect data on food consumption and adherence to the Mediterranean diet in a sample of adolescents aged from 13 to 18 years, living in the Rif region in north-eastern Morocco.
The methodology has been described in detail in a previous publication [33].
Study site
The study was conducted in the rural districts of Boudinar and Trougout and the town of Imzouren, situated 68 km, 25 km and 20 km respectively from Al Hoceima, the main Riffian city located on the Mediterranean coast of northern Morocco.
Sampling
The target population was defined as residents of the coastal Central and Eastern Rif regions. One of the 10 towns in the Central Rif region was randomly selected (Imzouren in Al Hoceima territory) and 2 of the 13 towns in the Eastern Rif region (Boudinar and Trougout in the Driouch territory). One of Imzouren’s three high schools was selected randomly. Selection was unnecessary in Boudinar and Trougout, which each have only one high school. A random stratified sampling technique was used to select a sample of the 2105 pupils enrolled in the 2012 school year. In each school, all pupils in a random selection of classrooms were informed about the study and invited to take part; participants were thus self-selected. Written consent was sought from all participants and their parents before the study. The research objective, the measurements and procedures were explained to participants, who could choose to quit the study on any grounds at any moment. Anonymity and confidentiality of participants was assured. The study conformed with the World Medical Association Helsinki ethical principles and obtained the ethical consent of the Ministry of Health and social protection (protocol 014446, August 17th, 2009).
Given the target study population of 2105 pupils, a 5% error margin, a 95% CI and an estimated response rate of 60%, 542 pupils had to be invited to participate to achieve the required sample size of 325. The actual number of invitations was 552. The final number of respondents with full data was 302. The drop-out rate was an acceptable 25.5% .
Participants had seven days to fill out the survey form; a researcher was available to help with any queries. Incomplete questionnaires (n = 141) are excluded from the current analyses, as are a further 109 questionnaires with inconsistent responses indicating a misunderstanding of the study procedure.
Data collection
Data were collected on socio-demographic variables (age, sex, residence area, monthly family income, family structure type, family size, housing category, parents’ education levels and occupations), the degree of adherence to the MD (KIDMED score), weight and height measurements and 3-day food consumption using a validated, locally-adapted and pretested questionnaire [34].
Evaluation of dietary intake
A food consumption diary over 3 nonconsecutive days was self-completed by participants, after receiving instruction from researchers on how to describe accurately the food items and quantities consumed, and the cooking methods. Quantities were recorded as common household measures (tablespoon, teaspoon, water, coffee or tea glass, etc.) and afterwards converted into quantitative measures using a digital electronic balance.
For each participant, mean daily micro- and macronutrient intakes and daily energy intake were estimated from the 3 days. The nutritional and energy composition of the food consumed individually was analysed using the DIAL ® program, adjusted for Moroccan dishes (couscous, tagines, etc.) [35–37]. Nutritional content details provided by the agro-processing industry were also included for locally processed products (beverages, yoghurt, sweets and fast foods). Data on nutrient intake did not include dietary supplements and medicines.
Assessment of the Mediterranean Dietary pattern
Adherence to the MD was assessed using the Mediterranean Diet Quality Index for children and adolescents (KIDMED index), a measurement tool developed and validated to estimate adherence to the Mediterranean dietary pattern specifically in children, adolescents, and young adults [32]. There are 16 questions about different dietary practices requiring a yes or no answer. Practices that do not conform to the MD are assigned a value of –1, and those that do conform are assigned + 1 (Table 1). The possible total KIDMED score ranges from 0 to 12, and can be categorised into three levels of adherence to the MD: poor ≤3, average 4–7, and optimal ≥8 [32]. For the present analysis, participants were grouped into two categories: a poor-to-average MD adherence category with KIDMED scores ≤7, and an optimal MD adherence category with scores ≥8.
The KIDMED index to assess adherence to the Mediterranean Diet in children and adolescents
The KIDMED index to assess adherence to the Mediterranean Diet in children and adolescents
Height was measured with a precision of 0.1 cm using a stadiometer, with subjects barefoot, heels touching the wall. Weight was measured with a precision of 0.1 kg using a Seca scale. Height and weight measurements were made in conformity with the International Biological Program guidelines [38]. Classification into underweight, normal weight, overweight and obese categories followed the World Health Organisation definitions [39]. Z-scores were calculated using the WHO Anthro-Plus 2007 software [40].
Statistical analysis
The SPSS statistical software for Windows version 19.0 was used for all statistical analyses [41]. Differences between categorical variables were tested by Chi-square test. Kolmogorov-Smirnov and Shapiro-Wilk tests were used to determine if a variable was normally distributed. Associations between normally-distributed variables were tested using Student’s t-test, and the Mann-Whitney U-test was used for continuous variables with non-normal distributions. A binary logistic regression was used to explore the significant factors associated with optimal adherence to MD. The odds ratios (OR) were estimated, with 95% confidence intervals (95% CI). A p value < 0.05 indicated statistical significance.
Results
Population characteristics
As shown in Table 2, the study sample comprised 302 adolescents aged 13 to 18 years old, 39.7% (n = 120) boys and 60.3% (n = 182) girls. The mean age was 14.9±1.4 years, boys being slightly but significantly older than girls. Over 80% of fathers were illiterate or had received primary education, and were employed as workers. Almost all of the mothers were housewives, and in the illiterate or primary education category. Only 6.3% of parents earned more than 8000 MAD (approx. 800 USD) per month, whereas 14.9% had a family income below 1000 MAD (100 USD) per month. More than 80% of participants lived in nuclear family households and resided in rural areas. Family size was predominantly small (2–4 members) to medium (5–7 members), only 15.6% living in families of 8 or more members. Most participants lived in traditional Moroccan houses. The study sample appears to be homogeneous in terms of illiteracy, poverty and rurality, and there are no significant difference between sexes.
Sociodemographic characteristics of the study participants, total and by sex
Sociodemographic characteristics of the study participants, total and by sex
SD: standard deviation; MAD: Moroccan Dirham (1 USD = approx.10 MAD); the sex differences were examined using the χ2 test for categorical variables and t-test for continuous variables, statistically significant differences: *p < 0.05, **p < 0.01).
The majority (79.5%) of participants were of normal weight, 7.3% were underweight and 13.2% were overweight or obese. The prevalence of overweight and obesity was significantly higher in girls (15.9%) than in boys (9.2%), but significantly more boys were underweight (13.3%) than girls (3.3%).
Figure 1 shows the level of adherence to the MD results by sex. The mean KIDMED score for the total study sample was 5.5 (±1.9), this value being statistically significantly higher among girls (5.7±1.9) than boys (5.2±1.7). Overall, only 14.9% of adolescents had optimal adherence to the MD, 72.8% had average adherence and 12.3% had poor adherence. Although the differences are not statistically significant, girls (18.7%) were twice as likely as boys (9.2%) to have optimal scores.
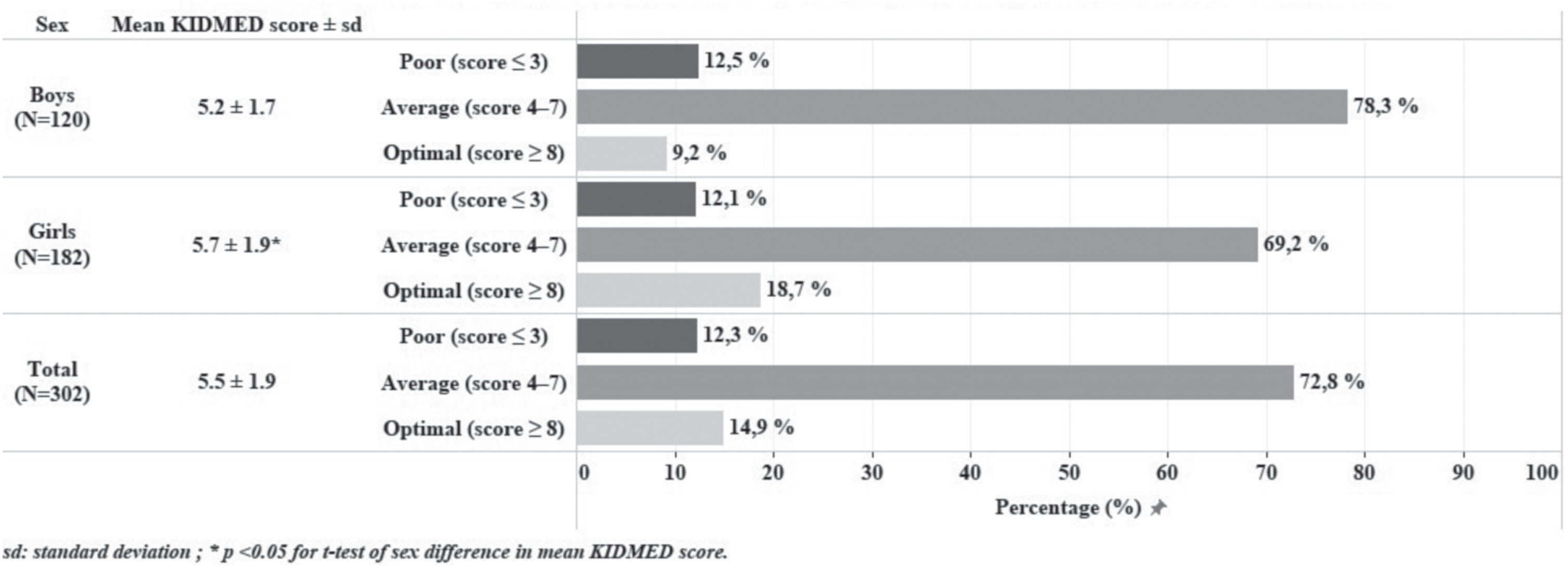
Adherence to Mediterranean Diet based on the KIDMED score for the total study population (N = 302) and by sex.
Among the sixteen items of the KIDMED index, only five elicited responses that differed significantly by sex (Fig. 2). The proportion of adolescents who indicated that they take a fruit or fruit juice every day, consume pasta or rice almost every day (5 or more per week), or skip breakfast, were significantly higher among girls than boys, whereas the proportion of girls who declared going more than once a week to a fast-food restaurant, or having commercially baked goods or pastries for breakfast was significantly lower than boys.
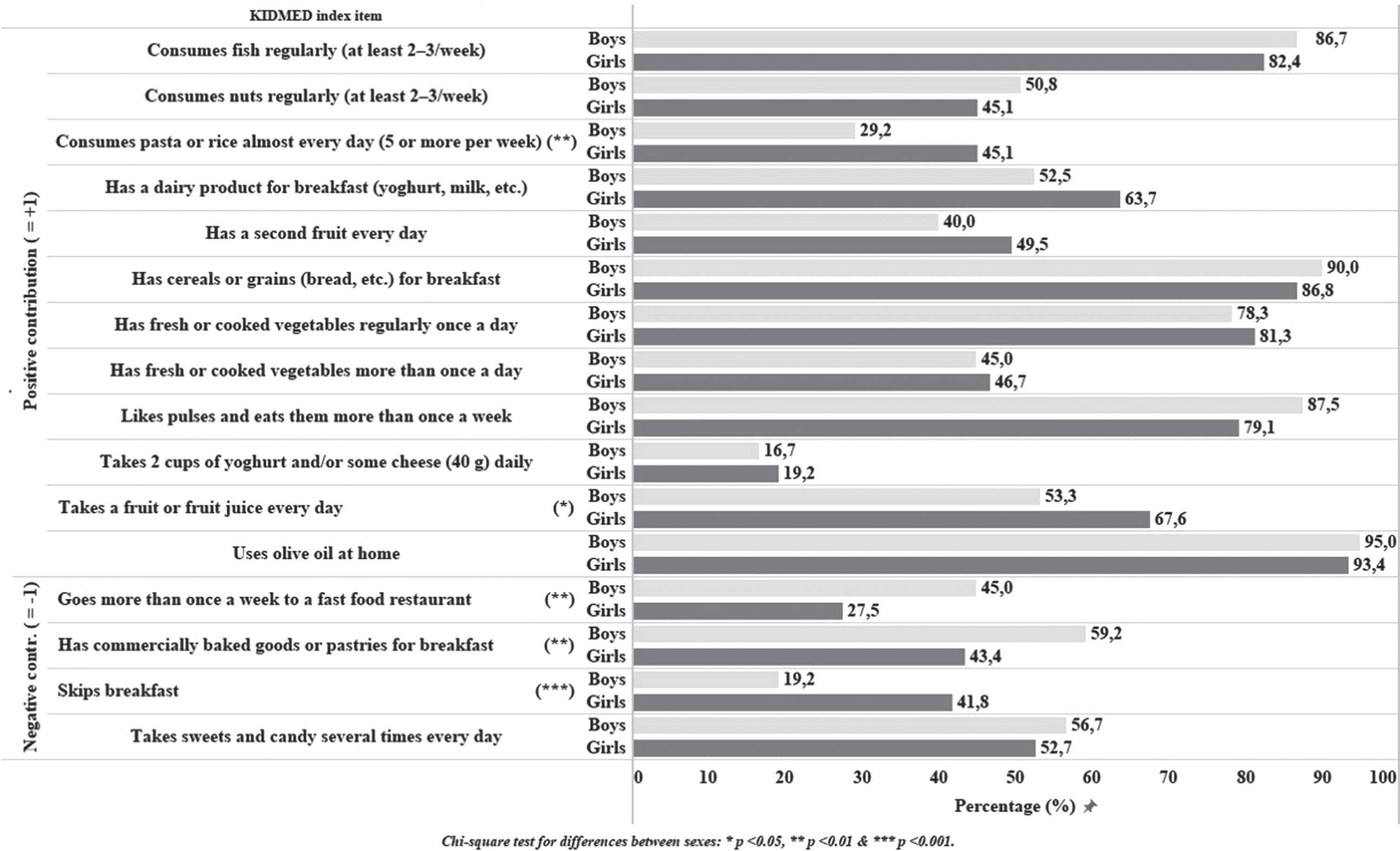
Percentage of affirmative responses to each item of the KIDMED index by sex.
Figure 3 shows the frequency of responses to each KIDMED item by KIDMED score. Overall, among items with a positive association with MD adherence, the items with the highest frequencies of response were the consumption of olive oil (94.0%), cereals or grains (88.1%), fish (84.1%), pulses (82.5%), fresh or cooked vegetables (80.1%) and fruit or fruit juice (61.9%). The item with the lowest frequency was consumption of yoghurt and/or cheese (18.2%). For items with a negative association with MD adherence, the lowest frequency of affirmative response was observed for skipping breakfast (32.8%), going to fast-food restaurants (34.4%) and taking sweets and candy several times every day (45.7%). The negative item with the highest frequency was having commercially baked goods or pastries for breakfast (50.3%).
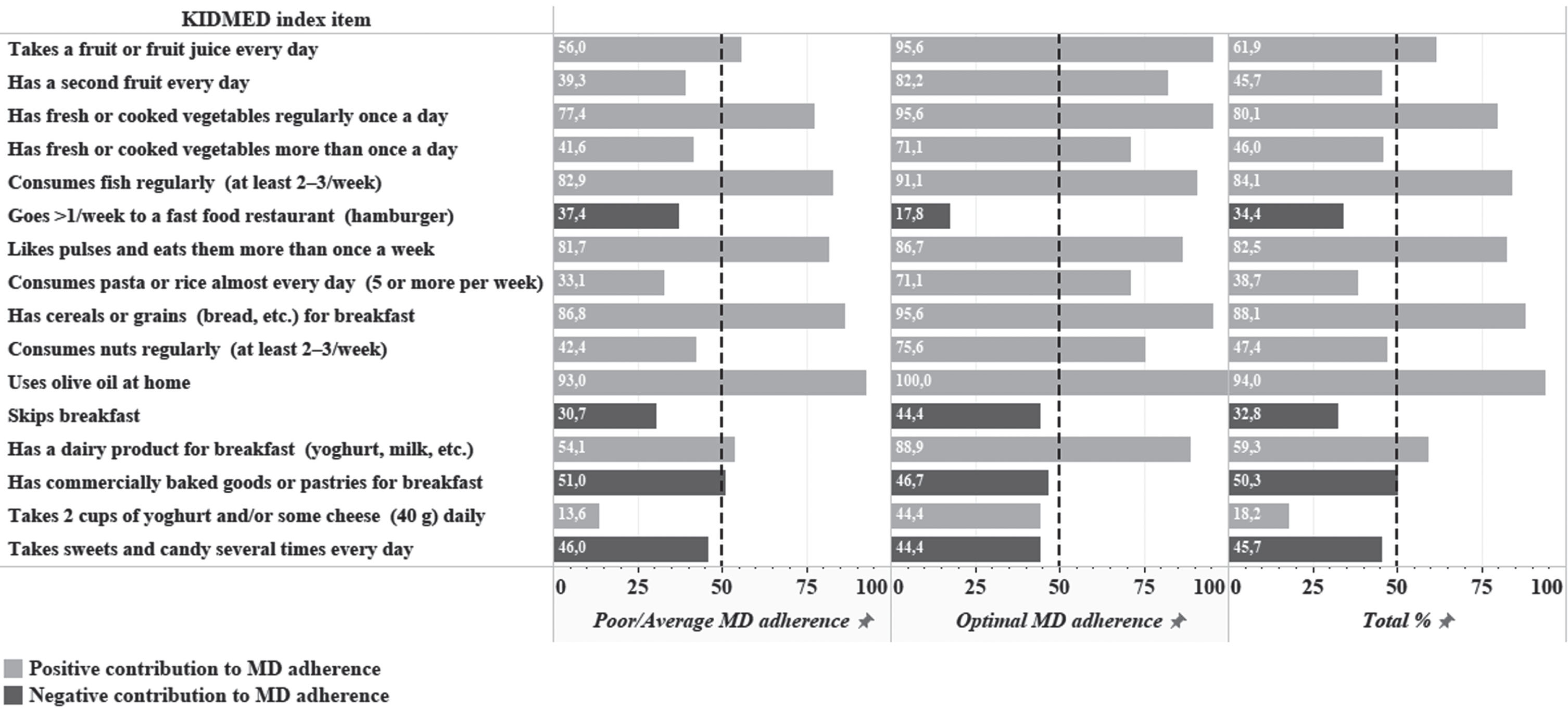
Percentage of affirmative responses to each item of the KIDMED index by Mediterranean Diet adherence category.
Concerning the KIDMED score categories, adolescents with poor/average adherence had high percentages of affirmative responses for the consumption of olive oil (93.0%), cereals or grains (86.8%) and pulses (81.7%). The items with the lowest frequency were the consumption of nuts at least two or three times per week (42.4%), fresh or cooked vegetables more than once daily (41.6%), a second fruit (39.3%), pasta or rice almost every day (33.1%) and two cups of yoghurt and/or some cheese (40 g) daily (13.6%). For negative items, the highest percentage was recorded for eating commercially baked goods or pastries for breakfast (51.0%) and the lowest for skipping breakfast (30.7%), attending fast-food restaurants (35.4%) and taking sweets and candy several times every day (46.0%).
In the optimal adherence category, all positive items had high percentages of affirmative response, except for the consumption of two cups of yoghurt and/or some cheese daily (44.4%). The negative item with the lowest frequency was going more than once a week to a fast-food restaurant (17.8%), whereas for the three remaining items, the percentage was between 44.4 and 46.7% .
With the exception of skipping breakfast and the consumption of legumes, cereals or grains, commercial baked goods for breakfast, sweets and candies, and fish, the differences between the two adherence categories for the remaining ten items of the KIDMED index were statistically significant.
Analysis of daily intake of energy, macronutrients and micronutrients with respect to the KIDMED score category (Table 3), revealed that, apart from an almost equal daily energy intake, pupils with optimal MD adherence had a higher intake of protein, lipids, saturated fatty acids, poly- and monounsaturated fatty acids, vitamins and minerals compared with the poor/average MD adherence group. However, the differences were not statistically significant.
Daily energy and nutrient intake by KIDMED score category
Daily energy and nutrient intake by KIDMED score category
SD: standard deviation; kcal/d: kilocalories per day; SFA: saturated fatty acids; MUFA: monounsaturated fatty acids; PUFA: polyunsaturated fatty acids; mg Eq. de α-toco: mg equivalent of alpha-tocopherol; DFE: dietary folate equivalents; RE: retinol equivalents. Differences between KIDMED score categories were examined using Student and Mann-Whitney tests.
Table 4 shows the association of MD adherence with sociodemographic and anthropometric variables. The variable “parents’ education” was created by grouping participants into two categories: both parents illiterate, and at least one parent literate. There was no significant association between MD adherence and parents’ education, father’s occupation, family size, family structure, residential area and nutritional status. However, MD adherence was significantly associated with sex, monthly family income and housing type. In a binary logistic regression (Table 5), female sex, monthly family income and housing quality were significant predictors of adherence to the Mediterranean diet. Girls were 2.3 times more likely to attain an optimal KIDMED score than boys (95% CI 1.1 –4.9; p = 0.031). Participants whose families had a high monthly income > 8000 MAD were 7.1 times more likely to have an optimal KIDMED score than those in lower income categories (95% CI 1.5 –33.1; p = 0.013). Living in an apartment significantly increased the odds of an optimal KIDMED score by 3.9 (95% CI 1.43 –10.3; p = 0.007). For other factors such as nutritional status and dietary intakes, no significant associations were observed.
Sociodemographic and anthropometric variables and adherence to the Mediterranean diet
Sociodemographic and anthropometric variables and adherence to the Mediterranean diet
χ2 test for differences between categories: *p < 0.05, **p < 0.01.
Binary logistic regression analysis of factors associated with optimal Mediterranean Diet adherence (KIDMED score ≥8)
β: regression coefficients; SE: standard error; OR: odds ratio; 95 % CI: confidence intervals; statistically significant differences: * p < 0.05; **p < 0.01.
The main objective of this study was to assess the level of adherence to the Mediterranean Diet among adolescents attending public schools in the Rif region of Morocco and to examine the factors associated with optimal adherence.
The population in this region consists primarily of Amazigh ethnic tribes. The most commonly spoken languages are the Tarifit dialect, followed by the Moroccan dialect of Arabic. One of Morocco’s most disadvantaged areas, this rural region is characterised by high rates of poverty and unemployment, particularly in the mountain communities, high infant mortality, low literacy levels, and limited access to basic sanitation and health services [42].
Most of the adolescents (72.8%) in the present study had average adherence to the MD, based on the KIDMED score, while 14.9% of adolescents had optimal adherence. These results are in line with a previous study conducted in Ouarzazate in the south of Morocco, which found a prevalence of optimal adherence of 10.5% in a sample of 495 teenagers aged between 15 and 20 years old [30]. However, a study conducted between May 2015 and November 2017 in Tafilalet Oasis located in the southeast of Morocco in a sample of 3684 children and adolescents aged 9–13 years found optimal adherence to the Mediterranean Diet in 39.9% of participants and poor adherence in only 2.1% [31].
The situation in Morocco appears to differ from that of other Mediterranean Arab and southern European countries. A cross-sectional study of 600 adolescents aged 15–18 years in Lebanon found 43% with poor and 41.2% with average adhesion to the Mediterranean Diet [43].
Compared with southern European countries, our study sample had the lowest percentages of adolescents with poor MD adherence, followed by the adolescents of Spain (15.7%), Greece (17.5%), Italy (29.9%), Cyprus (37%), and Turkey (40.6%) [16, 44–46,].
On the contrary, higher proportions of adolescents with optimal MD adherence have been found in Spain and Cyprus [44, 46] (28.4% and 21%, respectively compared with 14.9% in the present study). The lowest percentages of optimal MD adherence have been observed in Italy (9.1%), Turkey (7.7%), and Greece (6.7%) [16, 45].
In the optimal adherence category, all positive KIDMED items had high frequencies of affirmative response, except for the consumption of two cups of yoghurt and/or some cheese (40 g) daily, with less than 50% answering positively to this item. The values observed in this study are similar to or higher than those observed in previous Moroccan [30, 31] and Spanish [47] studies. Anzid et al. [30] found, in addition to the exception concerning the consumption of yoghurt and/or cheese (40 g) per day, a second exception for the consumption of pasta or rice more than once a day (17%). Similarly, Fernández-Iglesias et al. reported the exception of pasta consumption, as well as the exception of vegetable consumption more than once a day [47]. The desirable habits that do not differentiate significantly between adherence categories are regular fish consumption, pulse consumption and the consumption of cereals or grains for breakfast.
The negative KIDMED item that best distinguished the poor/average adherence group from the optimal adherence group was attending a fast-food restaurant more than once a week. In contrast to our results, in which boys eat fast food more frequently than girls, Fazelpour et al. reported that Iranian girls were significantly more likely to have a positive attitude towards eating fast foods than boys [48]. However, our results concord with those of the Iranian study in that the mean attitude score for eating fast food was higher in older than in younger adolescents. Arcila-Agudelo et al. have suggested that a lower level of parental supervision due to adolescents’ growing independence might explain in part this lower MD adherence [15]. The three other negative items that do not help to differentiate significantly between adherence categories are skipping breakfast, consumption of commercially baked goods or pastries for breakfast, and eating sweets and candies several times a day.
Although no significant differences in daily nutrient intake were observed between MD adherence groups, there is evidence of a monotonic relationship between nutrient intake and the MD adherence score. This may be explained by the high intake of healthy sources of protein in the MD, with cereals as the base, supplemented by fish, dairy products, legumes, and nuts. Olive and vegetable oils are the main source of mono- and polyunsaturated fatty acids and lipids, while legumes, fruit and whole grain cereals are a source of micronutrients [49]. Typical Moroccan dishes (bissara, harira, zaâlouk, couscous, mechoui, tajine, kefta and salads) use a wide variety of ingredients, ensuring plentiful macronutrients and essential micronutrients [50, 51]. A further benefit of traditional dishes is that lower cooking temperatures are generally used, thereby minimizing the molecular modification of nutrients and preserving their nutritional qualities [52]. Similarly, Moroccan dishes are commonly prepared with little water, further enhancing the concentration of nutrients [53]. Another feature of the cuisine of this northern Moroccan region is that fruit skins and vegetable tops, which have a micronutrient content 6 to 8 times higher than the flesh of the fruit or vegetable, are not discarded [54].
However, our results bring into question the ability of the KIDMED index to distinguish between two groups based on the adequacy of their nutrient intake. In the present study, adherence to the MD as indicated by the KIDMED score was not associated with nutrient intake. A similar observation was made in a Greek cross-sectional study, which evaluated MD adherence using the KIDMED index and nutrient adequacy in children and adolescents with cystic fibrosis [55]. However, in a sample of obese Spanish children and adolescents, plasma levels of certain trace elements (selenium, zinc, cobalt, molybdenum) were higher in those who were more adherent to MD, than their less adherent peers [56].
Further studies are needed to update the questionnaire for generating comparable data in other south Mediterranean countries and in different regions. Other researchers have suggested rewording several items of the KIDMED index [57]. For example, two items are not relevant to Moroccan dietary habits: item 14 “has commercially baked goods or pastries for breakfast” and item 15 “takes 2 cups of yoghurt and/or some cheese (40 g) daily”.
No statistically significant association was found between nutritional status indicated by BMI and the KIDMED score. Similarly, a study of a stratified sample of 4786 children in 10 regions of Greece found no relationship between BMI and the KIDMED score [58]. Other studies, however, have observed an inverse relationship between the Mediterranean dietary pattern and BMI [48, 59].
In the present Moroccan study, girls (18.7%) were twice as likely as boys (9.2%) to show optimal adherence to the MD. However, previous studies have reported conflicting results. Mariscal-Arcas et al. [60] found that MD adherence was higher in Spanish girls, whereas del Mar Bibiloni et al. [44] showed that boys in the Balearic Islands were more compliant than girls with the MD. No significant sex differences in optimal MD adhesion were found in two cross-sectional studies carried out in Spain, the first conducted on 1177 children and adolescents aged 6 to 18 years [15] and the second on 309 participants aged 8 to 13 years [47]. Our finding might be explained by the fact that girls tend to have better dietary habits than boys [61], and rarely eat outside the home. Zhang et al. found that Chinese girls were more likely to engage in healthy eating (fruit and vegetables) and to meet nutritional recommendations every day, whereas boys were more likely to consume high-energy food (fast-food, fried and sugary foods) [61].
Monthly family income and housing type were significantly associated with MD adherence assessed by the KIDMED index. Adolescents from low-income families and living in traditional Moroccan housing were less likely to have optimal adherence to the MD. This concords with previous studies that correlated high consumption of non-Mediterranean food with low socioeconomic status [31, 63]. There were no significant associations between MD adherence, parental education, parental occupation, family size, family structure and area of residence. A Turkish study of a group of boys aged 10–14 years found that parental education had no significant effect on nutritional status or the KIDMED score [64].
Regarding housing types, we found an association between optimal MD and living in an apartment. El Rhazi et al. [27] showed that people living in the old and new medina were more likely to follow a MD than those in both superior quality housing and poor housing, while Mohtadi et al. [28] reported that living in superior housing was associated with a high adherence to MD. Additionally, we found that a monthly family income of over 8000 dirham was positively associated with higher MD adhesion. Similar results have been reported in other studies [65]. A higher socioeconomic status is concomitant with a higher educational and cultural level, and consequently greater knowledge about health issues and healthy eating behaviours. Consumers at this level of income can easily satisfy their nutritional needs and concerns about food quality and safety [66].
The limitations of our study include its cross-sectional design, which allows only the interrelationships between the various factors studied and not causality to be established. Further, the KIDMED index, developed for Spanish children and adolescents, has not been validated for Moroccan adolescents. Nevertheless, given the lack of a specific tool to assess MD adherence in Moroccan adolescents, we believe that the KIDMED index is adequate, since it is based on general principles that are widely applicable to different Mediterranean populations. However, some KIDMED index items are difficult to translate into Arabic or Moroccan dialects, hence the need for input from a linguistic expert in the future. The response rate was low because enrolment was voluntary. Since the survey was conducted in only three municipalities of the Moroccan Rif, and the study sample relatively small, homogenous, and restricted to school-attending adolescents, with an over-representation of girls, these results may not be generalizable to all adolescents of the region.
Although dating back to 2012, the data provided by the present study have scientific value as they provide a baseline for future research and for the evaluation of national or international nutrition programmes and interventions.
This study has several strengths. Participants were especially motivated by trained interviewers to complete the detailed questionnaire correctly. The results represent the first report of MD adherence among Moroccan adolescents in the Rif region. This information is particularly useful, in the absence of comparable data, for the development of dietary guidelines and public health interventions involving nutrition policies.
Conclusion
This study found a low level of adherence to the MD among adolescents in the Rif region, supporting the hypothesis that the dietary pattern of these Moroccan adolescents is in a transitional state characterized by a shift away from the traditional MD. The results of this study also indicated a positive relationship between adherence to the Mediterranean Diet and female sex, monthly income and housing quality. Associations with others factors such as nutritional status were not observed, but as the literature has shown conflicting results, more research is needed on this issue. We suggest that the KIDMED index should be adapted to provide a more valid tool for southern Mediterranean populations, to allow a better distinction between groups based on the adequacy of their nutrient intake and to generate comparable data. Specific interventions are required to show adolescents the benefits of the MD and to give practical advice on improving their MD adherence.
Footnotes
Acknowledgments
The authors thank the Ministry of National Education, Preschool and Sports, participating teenagers and their families.
Funding
None.
Declaration of interest
The authors have no conflicts of interest to declare.
Authors’ contributions
AH, MC and PML planned the study and data collection, contributed to data interpretation and manuscript revision. OE managed the data collection. OE, KA and SL analysed data, and wrote and revised the manuscript. SL supervised the linguistic correction.