
Abstract
Since the dawn of time human beings have been trying to improve the quality of the existence and extend their lifespan. Genetic, environmental, behavioral and dietary factors influence the pathways that regulate aging and life expectancy, thus rendering longevity a very complex phenomenon. Although a long-lived elixir has not yet been found, physicians and scientists agree that nutrition has a major impact on the overall mortality and morbidity, hence becoming the subject of a widespread scientific research.
This review describes, analyzes and compares the effects of different types of diets in reducing the onset of typical Western countries non-communicable diseases (NCDs) (cardiovascular diseases, tumors, chronic respiratory diseases, diabetes, etc.), thus increasing the average lifespan. It will first depict the most relevant characteristics, nutraceutical properties and effects on the populations of the Mediterranean, Japanese, Vegetarian and New Nordic Diet. Finally, it will describe the impact of different dietary restrictions in modulating the genetic pathways that regulate metabolism and aging.
Overall, this work reinforces the evidence that specific eating habits, in addition to healthy and active lifestyles, are crucial to increase people’s health span and to achieve an optimal longevity.
Introduction
At the beginning of this century, the World Health Organization (WHO) found that the so-called non-communicable diseases (NCDs), also known as chronic diseases, are responsible for the death of forty million people every year, equivalent to 70% of all deaths globally. Cardiovascular diseases (CVDs) account for most NCDs deaths (17.7 million people annually), followed by cancers (8.8 million), respiratory diseases (3.9 million) and diabetes (1.6 million) [1]. The fact that the world’s older population continues to grow at an unprecedented rate renders this circumstance even more worrying. According to the report “An Aging World: 2015” the 8.5% of the world’s population is more than 65 years old and, if this growing trend continues, by 2050 almost the 17% of the global population will be aged over 60 [2]. Changes in lifestyle, technological improvements and the recent medical discoveries have contributed to the rapid rise in the proportion of older people in the society [3]. Among the individuals aged 60 and over, NCDs account for more than 87% of the disease burden, with an higher age-related occurrence of chronic diseases, disabilities, morbidity and mortality [4–7]. Combining the phenomenon of aging and good health is therefore one of the biggest social challenges of today’s world. Currently, the major medical strategy for the treatment of NCDs is pharmacological; however, a progressive increase of sick people, elderly people in particular, which are affected by multiple chronic conditions [8], will render this approach less and less sustainable. Moreover, the simultaneous usage of different types of drugs for the treatment of various chronic diseases makes the patient health status even weaker [4]. Rather than dealing with the symptoms of the aging-related diseases, it is necessary to preventively act on the process of aging itself [3, 9]. The achievement, at a global level, of a “healthy aging phenotype” defined as “the condition of being alive, while having highly preserved functioning metabolic, hormonal and neuroendocrine control systems at the organ, tissue and molecular levels” [10], is the most ambitious objective that modern science should achieve. Extending people’s health span, in order to attain an optimal longevity, is possible through specific preventive actions. Life expectancy, in fact, is strongly influenced by environmental and behavioral conditions, which affect, more than genetics, the onset of chronic diseases [11]. Several medical and scientific evidences have shown that proper nutrition, together with a healthy lifestyle, are crucial to counteract NCDs development hence enabling people to lead longer disease-free lives.
This review describes and compares specific diet models namely the Mediterranean Diet, the Japanese Diet, the Vegetarian Diet and the New Nordic Diet, which have been shown, by experimental, epidemiological and clinical evidences, to be able to increase life expectancy, reducing morbidity and total mortality (lowering the incidence of chronic diseases), thus allowing people to live a longer and healthier life. Indeed, the so-called “Blue Zones” (Sardinia in Italy, Icaria in Greece, Okinawa in Japan, Nicoya in Costa Rica and Loma Linda in California [12, 13]) are demographic and/or geographical areas populated by the world’s longest-lived individuals who feed themselves following the dictates of the Mediterranean, the Japanese or the Vegetarian diet. Moreover, it illustrates the effects of caloric restriction, fasting and mimicking fasting diets on people health, showing that even these dietetic strategies can boost longevity.
The purpose of this review is to demonstrate, with proven clinical and scientific evidences, that specific lifestyles and eating habits are absolutely crucial to achieve a longer and healthier life.
The aging process
The dream of eternal youth goes back to the most remote times of humanity, belonging to the sphere of the sacred, the myth, the alchemy and the magic. Even in our modern and technological times this desire has remained unchanged and, owing to scientific research, we are trying to reach, not immortality, but at least a healthy longevity. Hippocrates (Coo, 460 BC - Larissa, 377 BC), the father of medicine, was the first to understand the importance of proper nutrition in maintaining wellbeing by declaring: “Let food be thy medicine and medicine be thy food”. To date, an increasing number of evidences, accumulated in particular in the last decades, confirm that the promotion of a balanced diet, combined with a healthy lifestyle, is the most effective recipe to promote a successful aging.
Aging is a multifactorial, progressive, universal and irreversible process, affecting all living organisms. This phenomenon is characterized by multiple changes in the functions of organs, energy metabolism and cell physiology and it is associated with a reduced ability to respond to environmental stress, thus increasing the probability to develop chronic diseases that are the leading causes of death and disability [14].
Over three hundred hypotheses try to explain the phenomenon of aging, one of the most accredited states that the alterations caused by aging are due to the imbalance between the effects of the factors responsible for biological damages (endogenous or exogenous) and the effectiveness of the reparative processes of the cell [15]. Due to defects in cell repair mechanisms, mutations occur in DNA, protein structures and organelles, progressively reducing the overall functionality of the organism. The greater the imbalance between biological damage and repair processes, the faster the aging of the individual.
One of the most frequent causes of endogenous biological damage is determined by the production of reactive oxygen species (ROS) [16]. Specific antioxidant mechanisms, both endogenous (glutathione peroxidase, catalase, superoxide dismutase) and exogenous (vitamin A, C, E, minerals and bioactive compounds) can counteract the toxic action of ROS [16]: when these systems fail, ROS accumulation induces cell damage (oxidizing membrane lipids, changing the conformation of proteins, damaging nucleic acids) eventually speeding up the process of aging [17]. It has been shown that an excess of oxidative stress is implicated in the pathogenesis of many chronic diseases linked to aging (hypertension, cardiovascular diseases, type II diabetes, atherosclerosis, Alzheimer’s and cancer) [18]. In the specific case of atherosclerosis, elevated levels of ROS favor the oxidation of low-density lipoproteins (LDL) and the formation of atherosclerotic plaques [11, 19].
A crucial consequence of the excessive accumulation of ROS is the increase in pro-inflammatory cytokines expression (TNF-α, IL-6), resulting in a chronic systemic inflammation able to promote cellular senescence [20, 21]. In contrast, elevated levels of anti-inflammatory cytokines, such as interleukin 10 (IL-10), are associated with longevity: of note, genotypes characterized by high levels of IL-10 are more common in centenarians [22, 23]. According to these observations, it has been shown that, in the elderly, a wide spectrum of degenerative aging-related diseases (Alzheimer’s disease, Parkinson’s disease, amyotrophic lateral sclerosis and age-related macular degeneration), is caused by a previous and persistent systemic inflammatory state, thus supporting that chronic inflammation is a predictor of senescence [11].
Metabolic ROS are generated in several cellular systems localized on the plasma membrane, in the cytosol, in peroxisomes, and on membranes of mitochondria and endoplasmic reticulum. Functional alterations of these organelles generate excessive quantities of free radicals, stimulating the aging processes [24]. However, cells are equipped with repair mechanisms that allow the maintenance of a structural integrity, such as autophagy, a process that identifies, isolates in vacuoles and degrades the damaged organelles. Nevertheless, with ageing also this repair mechanism undergoes a physiological decline [25, 26], leading to a greater accumulation of altered organelles, thus conditioning the longevity of individuals. The process of autophagy, which is essential to allow organelles replacement, is activated when cells have to compensate for the lack of exogenous nutrients by degrading their components; normally this happens when the organism is fasting [27]. This explains why a dietary approach that reduces caloric intake, but still rich in crucial nutrients, can have a positive influence on lifespan elongation, as discussed next.
Irreparably damaged cells are replaced through cell replication: however, this is not an infinite process and, after a characteristic number of divisions, cells reach the so-called replicative senescence status (or Hayflick limit), remaining in a state of stable irreversible growth arrest [28]. This phenomenon depends on the shortening of telomeres, specialized structures composed of repeated nucleotide sequences and positioned at the end of each chromosome in order to prevent its degradation during cellular duplication. Each cell division determines a progressive structural alteration of telomeres, which become progressively shorter until reaching a point after which cells are no longer able to replicate [29]. The shortening of telomeres makes the cell more sensitive to mutations and has been associated, in humans, with aging and age-related diseases (tumors, autoimmune diseases, cardiac diseases, dementia, obesity and diabetes) [30]. Therefore, telomere length can be seen as an indicator of an individual biological age: the longer they are, the younger is the organism, the shorter they are, the higher is the risk of aging-associated diseases. However, a compensatory mechanism for the reduction of telomere length exists that is based on the action of telomerase, a specific enzyme able to catalyze the lengthening of these repeated DNA structures [31, 32]. Interestingly, telomerase activity can be influenced by nutrition and lifestyle [33–35].
The mediterranean diet
The Mediterranean diet is a nutritional model inspired by the diet consumed, immediately after the Second World War, by the populations of the Mediterranean area (such as Italy, Greece, Spain and Morocco). However, the Mediterranean diet (from the Greek “δíαιτα”, “díaita”, way of life) encompasses more than just food, representing a set of knowledge, social habits and cultural traditions historically spread by the communities overlooking the “Mare Nostrum”. This nutritional model, always respecting beliefs of each community, consists mainly of plant-based food (olive oil, whole grains, vegetables, legumes, fresh fruits, nuts, seeds, herbs and spices), a moderate amount of fish, dairy and poultry, low consumption of red meat, sugars and pastry [36, 37]. Owing to the commitment to natural resources and reduced emission of agricultural greenhouse gasses (centered mostly on plant-based foods), respecting seasonal cycles of crop, territory and biodiversity (using crop rotation and different seeding times), the Mediterranean diet guarantees a correct balance between nature, mankind and renewal of resources [38]. For all these reasons, the Mediterranean diet is a healthy and sustainable dietary model, proving to be one of the most sustainable nutritional patterns for both the environment and our health.
The mediterranean diet pyramid
The diet pyramid characteristics of different Mediterranean countries (Greece, Italy, Spain, etc.) slightly differ from each other: however, given the recognition attributed to the Mediterranean diet, several versions of pyramids have been realized, representative of this specific nutritional model [39–42]. Figure 1 summarizes the rules expressed by one of the more detailed and complete version of the Mediterranean Diet Pyramid officially recognized worldwide and that proficiently represents this dietary habit [41]. This version of the pyramid incorporates also social, ecological and cultural elements, paying attention to the kind and origin of food, together with the way in which it is produced, selected, cooked and eaten. The preference for seasonal, fresh and minimally processed foods maximizes the content of protective nutrients and substances in the diet. Moreover, the choice of local, eco-friendly and bio-diverse products contributes to the preservation of the environment. The Mediterranean diet contains approximately 60–65% of the calories as carbohydrates (less than 10% simple sugars), 10% of proteins and 25–30% of fats (7–10% of saturated fatty acids, SFAs, up to 20% of monounsaturated fatty acids, MUFAs, and 7% of polyunsaturated fatty acids, PUFAs, with an omega-6/omega-3 ratio from 2:1 to 4:1 [36, 43]). The pyramid is built upon daily physical activity and exercise (at least 30 minutes every day), rest (to counteract stress), conviviality and to an adequate daily water balance (1.5–2 liters a day). The value of a frugal, moderate and varied diet is pointed out: at the base of the pyramid are vegetables, fruits, extra virgin olive oil (primary source of unsaturated fats), wholemeal grains and derivatives. Legumes, spices and aromatic herbs (which contribute to the reduction of salt addition and contain important micronutrients), olives, nuts and oil seeds are located on the second step: they should be consumed daily like low fat dairy products, which are found at the level above. A moderate intake of fish, poultry and eggs is recommended, while red meat, processed food, products rich in sugars and fats must be eaten only on rare occasions. A moderate intake of wine (better if red) is allowed in the respect of traditions (Fig. 1). The Mediterranean diet is hence characterized by the high usage of unsaturated fats, foods rich in fiber, antioxidants and anti-inflammatory compounds, which are critical to slow down ageing process and decrease the risk of several chronic diseases.
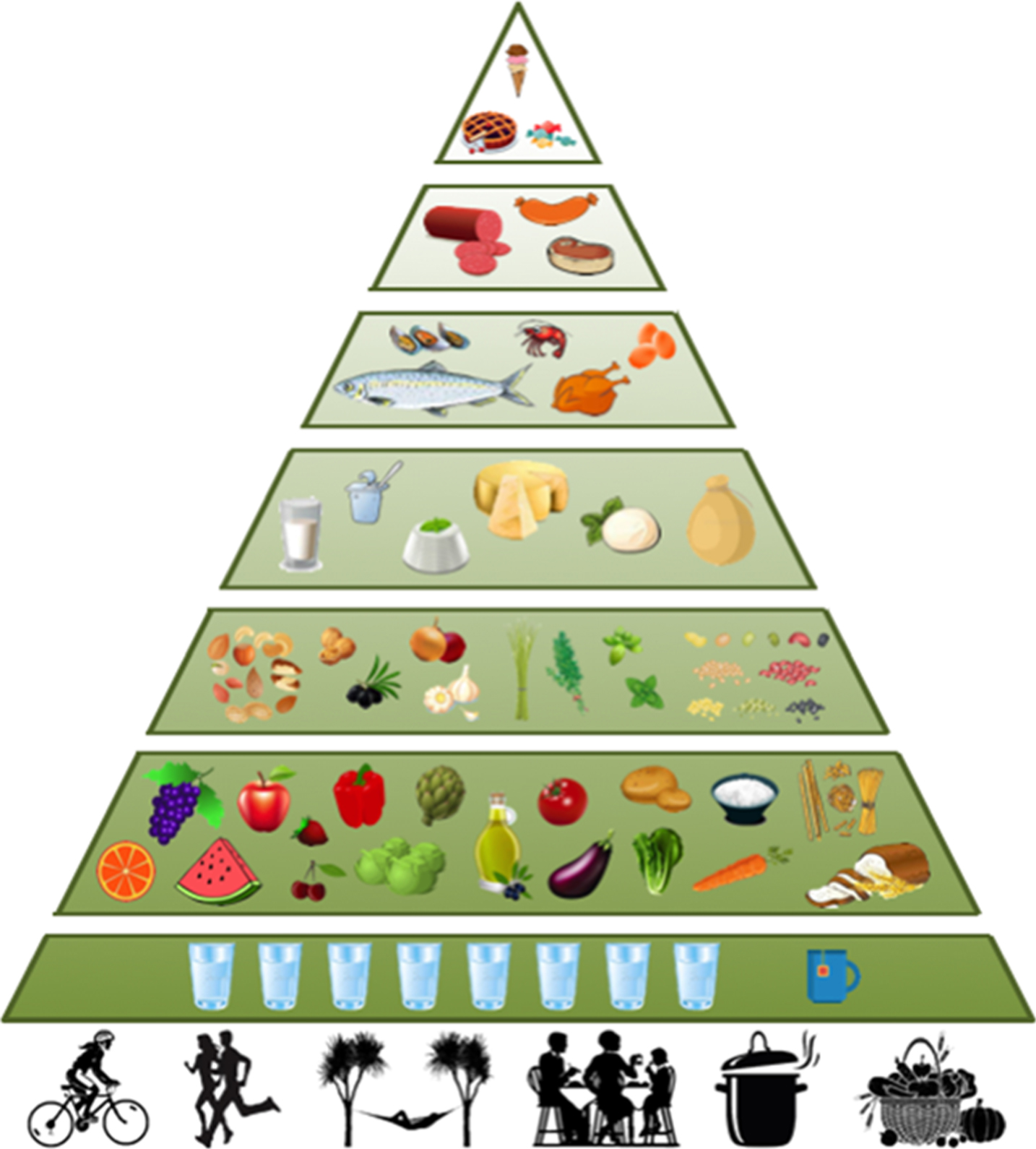
The Mediterranean Diet Pyramid. Schematic representation of the rules expressed by the Mediterranean Diet Pyramid described by Bach-Faig et al. in 2011 [41].
The definition of “Mediterranean Diet” was coined for the first time by the American physiologist and biologist Ancel Benjamin Keys (Colorado Springs, 1904 - Minneapolis, 2004). Until the early 1900 s, in fact, there were not any robust scientific evidences showing that nutritional habits could play a role in health maintenance and diseases prevention. Only after World War II, Ancel Keys proposed and demonstrated, for the first time, that eating habits can influence the global health status and, in particular, the epidemiology of cardiovascular disease [44–46]. In 1957, he launched the project known as “The Seven Countries Study of Cardiovascular Diseases” [46–49], defining, for the first time, the concept of “Mediterranean Diet” and documenting its benefits in decreasing cardiovascular diseases risk and expanding the general healthspan. The Seven Countries Study of Cardiovascular Diseases comprised 16 groups (cohorts) of men aged 40 to 59 in eight nations from seven different countries (US, Finland, Netherlands, Italy [50], ex-Yugoslavia [51], Greece [52] and Japan), including more than 12000 individuals [48, 51]. The aim of this work was to assess connections of different lifestyles to the risk of developing or dying for cardiovascular diseases. The different food models were characterized by a high consumption of saturated fats in America and Northern Europe populations, in contrast to the Mediterranean and Japanese areas, where the ingestion of this kind of lipids was negligible [53]. The populations were analyzed every 5 years, for several decades (up to 40 years in some cases) and data on the incidence of cardiovascular diseases and mortality were systematically collected [45, 54]. The analysis showed that saturated fats consumption strongly correlated with severe coronary heart disease (CHD) and increased risk of death, while the high intake of monounsaturated fats and flavonoids (typical of the Mediterranean diet) resulted in a lower incidence of mortality due to ischemic heart disease and tumors [55]. The results of this huge epidemiological study were evaluated over the years by different groups of researchers with various and complex statistical methods [47–50, 56]. More recently, observations on the relationship between individual food groups and coronary mortality suggested that, in general, food of animal origin and sugar (mainly consumed by North American and North European cohorts) were directly related to an increased coronary mortality, while food of plant origin, fish and moderate alcohol consumption (typical of Mediterranean populations and Japan) showed an inverse statistical correlation [57]. From this study emerged clearly as the populations that had adopted a Mediterranean and a Japanese diet presented a minimum percentage of incidence and mortality from cardiovascular diseases and a long-term survival. This was mainly due to the food patterns chosen by these people that were mostly of plant origin, rich of mono- and polyunsaturated fats, fiber and phytonutrients and poor of sugars, meat and saturated fats.
The benefits of mediterranean diet: Scientific evidences
In the last 50 years, many epidemiological and physiopathological evidences confirmed that the Mediterranean diet has beneficial effects on health and longevity [58–64]. A meta-analysis of prospective cohort studies published from 1966 to 2008 (which included more than 1.5 million subjects) showed that a strict adherence to the Mediterranean diet “is associated with a significant improvement in health status, as seen by a significant reduction in overall mortality (9%), mortality from cardiovascular diseases (9%), incidence of or mortality from cancer (6%), and incidence of Parkinson’s disease and Alzheimer’s disease (13%)” [65, 66].
Specifically, a strict adherence to the Mediterranean diet has been shown to have positive repercussions on various chronic diseases, as briefly listed below.
Tumors. Overall, the Mediterranean diet revealed strong preventive effects on all types of tumors. This emerged in particular from the European Prospective Investigation into Cancer and Nutrition (EPIC) epidemiological study, which highlighted that the Mediterranean nutritional model is the most effective in reducing cancer risk [67]. The preventive action of the Mediterranean lifestyle on the onset of tumors [68, 69] is particularly robust on stomach cancer [70, 71], esophageal tumors [72], colon-rectal tumors [73], mammary and endometrial cancers [74–76].
Cardiovascular Diseases. A number of studies have emphasized the protective and preventive effects of the Mediterranean diet on hypertension [77], cardiovascular diseases, myocardial infarction and its follow-up [78–84]. In a multicentric and multinational Spanish study of large-scale prevention (Prevention con Dieta Mediterránea, PREDIMED), conducted between 2003 and 2011, patients at high risk of cardiovascular diseases, were randomly assigned to low fat diet, Mediterranean “rich in olive oil” diet and Mediterranean “rich in nuts” diet. The Mediterranean diets, without restriction of calories, supplemented by extra virgin olive oil or nuts, were the most effective in reducing by 30% the risk of major cardiovascular events [83, 85].
Type II Diabetes. Mediterranean diet demonstrates also a beneficial effect in both the glycemic control and on primary prevention and complications of type II diabetes [86–91]. In particular, an epidemiological study of 2013 showed how a Mediterranean diet, which involved the consumption of carbohydrates with low glycemic load, is able to reduce the risk of diabetes by 20% [92].
Obesity. Obesity is a chronic disease associated with several pathological conditions: hypertension, dyslipidemia, cardiovascular diseases, alterations of glucose metabolism and type II diabetes, which when simultaneously present result in the metabolic syndrome (MetS). A link between obesity and the risk of developing different types of cancers was also established. Several epidemiological studies clearly demonstrated that a strict adherence to the traditional Mediterranean diet is inversely associated with an increase in body mass index (BMI), overweight, obesity and onset of MetS [93–95]. Furthermore, a hypocaloric version of this nutritional approach, combined with regular physical activity, represent a safe strategy for an effective and stable weight loss [58, 96].
Chronic Respiratory Diseases. Chronic obstructive pulmonary disease (COPD), the fourth leading cause of death in Europe and in the US, is a chronic pulmonary disease characterized by long-term breathing problems and poor airflow. This pathology is strongly influenced by both genetics and environmental factors, physical inactivity and diet. In the last twenty years, several studies have shown that a Mediterranean diet, particularly rich in fruit, nuts, vegetables, fish and whole grains is associated with a reduced risk of COPD [97–99].
Neurodegenerative Diseases. The richness of antioxidant and anti-inflammatory foods, characteristic of Mediterranean nutrition, together with the beneficial effects exerted by this dietetic regimen on cardiovascular health, allows to counteract both the simple cognitive decline related to age and the onset of more serious neurological disorders, like Parkinson’s and Alzheimer’s diseases [100–105].
Osteoporosis. A strict adherence to the traditional Mediterranean diet has shown protective effects on the onset of osteoporosis [106–108]. A trial PREDIMED conducted on cardiopathic individuals between 55 and 80 years established that a Mediterranean diet, rich in extra virgin olive oil, is associated with a lower risk of osteoporotic fractures [109].
Microbiota and Mediterranean Diet. A high adherence to a Mediterranean diet guarantees the presence, in the feces, of an elevated concentration of short chain fatty acids, microbial metabolites with a recognized anti-inflammatory and antitumor effect. In contrast, individuals with low adherence to the Mediterranean nutrition model present a significant concentration, in the urine, of N-oxide of trimethylamine (TMAO), a microbial product associated with the development of atherosclerosis and cardiovascular disease [110, 111].
Mediterranean diet and longevity
The Mediterranean diet, as discussed previously, is able to exert a protective effect on the onset of NCDs that cause the main events of morbidity and mortality in industrialized countries. Therefore, it is not surprising that this type of diet, together with a healthy lifestyle, can prolong life expectancy [112–117]. Indeed, a Mediterranean diet regimen ensures the regular intake of foods containing numerous substances with antioxidant and anti-inflammatory properties, which hinder not only the onset of various diseases, but allow to delay the aging process and promote a healthy longevity, combating some of the main causes of ageing as oxidative stress, inflammation and shortening of telomeres [118–121]. Therefore, it is not surprising to find out that Sicanian Mountains (Sicily), Cilento, Sardinia, Icaria are among the areas where people live the longest [12, 122–124].
Several researches have tried to understand how the Mediterranean diet could contribute to the achievement of a healthy aging [114, 125–127]. The Healthy Aging: a Longitudinal study in Europe (HALE), which aimed to evaluate the association of a specific diet and lifestyle with the mortality rate in the elderly population, showed that, even at an age between 70 and 90, following a Mediterranean diet in the context of a healthy lifestyle reduces all causes of death by more than 50% [128]. A very recent European project, the New Dietary Strategies Addressing the Specific People of Europe for Healthy Aging in Europe (NU-AGE; Grant Agreement 266486, www.nu-age.eu) [129–133], coordinated by the University of Bologna, is preliminarily confirming the beneficial effect of those eating habits. More than one thousand and two hundreds volunteers over the age of 65 from five different European countries were recruited and only those following a Mediterranean diet showed: (i) a decrease in levels of C-reactive protein, a well-known marker of systemic inflammation and cardiovascular risk factor; (ii) an improvement of the lipid profile, in terms of triglyceride levels and of the ratio between total cholesterol and high density lipoproteins (HDL); (iii) attenuation of bone loss [132].
Mediterranean diet and nutraceuticals
Foods containing bioactive molecules are considered “nutraceuticals”, namely “a food or part of a food that provides medicinal or health benefits, including the prevention and treatment of disease”. The term was coined in 1989 by Stephen De Felice and represents the link between nutrition and pharmaceutics [134]. The antioxidant and anti-inflammatory properties of bioactive molecules contained in several Mediterranean foods are identified as the main factors responsible for the beneficial effects of this diet on longevity and against the development of chronic diseases associated or not with ageing [91, 135–137]. The effects exerted by these nutrients are mostly due to the combined action and integration of antioxidant elements (polyphenols, flavonoids, phytosterols, vitamins, minerals and micronutrients, etc.), fibers and unsaturated fatty acids (omega-3, omega-6 and omega-9) [11, 75].
The main important features of the most common Mediterranean foods, nutrients and phytocompounds and their beneficial health effects are briefly resumed in Table 1.
Nutraceutical properties and health benefits of the most representative Mediterranean Diet foods
Nutraceutical properties and health benefits of the most representative Mediterranean Diet foods
As previously mentioned, “The Seven Countries Study of Cardiovascular Diseases” showed that, together with a Mediterranean, the Japanese dietary pattern was associated with low rates of coronary heart disease and all-cause mortality [56, 138]. Recent cohort observational studies have confirmed these findings, demonstrating that adherence to a Japanese diet results in a lower risk of cardiovascular mortality [139, 140]. Consistently with these data, the life expectancy of the Japanese population has steadily increased over the last few decades and is currently among the longest in the world [140]. Thus, for the scientists, understanding the relationship among Japanese diet, low risk of mortality and longevity has long been a source of clinical interest. Japanese mainly consume small portions of fresh seasonal traditional foods (fish, rice, seaweeds, soy and derivatives, vegetables and green tea), practicing the “hara hachi bu”, meaning “eat until you are 80 percent full”. Carbohydrates are widely represented, due to the high rice intake, making up about 60–65% of total calories, the consumption of fats represents about 20–25% and the intake of proteins, especially of plant origin, covers the remaining 5–10% [141]. Compared to Mediterranean people, Japanese consume lower amount of fats and the omega-6/omega-3 ratio is about 2:3 [142].
Japanese food guide spinning top
The peculiar conformation of the Japanese archipelago (consisting of over 3000 islands), together with historical and cultural events, religious influences and contacts with many foreign countries, contributed to the creation of a unique and peculiar dietary style, characterized by a wide variety of foods and culinary specialties [143]. Only in 1980 the Ministry of Agriculture, Forestry and Fisheries of Japan proposed for the first time the concept of a “Japanese Diet” and recognized it as generally superior to Western diets in order to obtain an optimal state of health [144]. Twenty-five years later, in 2005, the Japanese government developed a series of food recommendations, later revised in 2010, represented by a rotating spinning top (summarized in Fig. 2), a traditional Japanese toy [145].
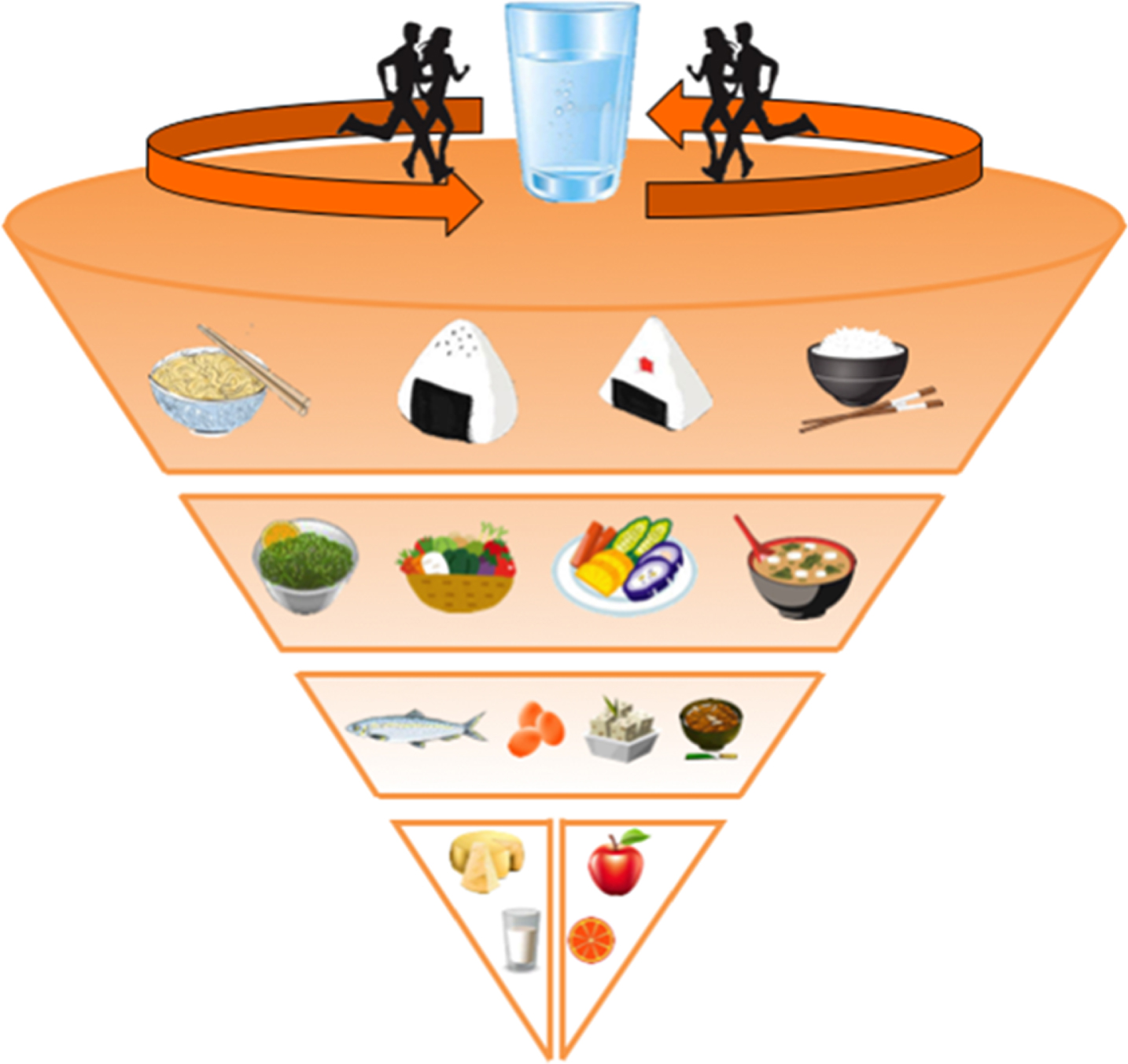
The Japanese food guide spinning top. Schematic representation of the food recommendations expressed by the Japanese government in 2005 and later revised in 2010 [145].
This sort of rotating inverted cone is divided from the top down into four group layers whose order is given by the recommended daily servings. At the top there are grain-based dishes (rice, noodles), followed by plant-based dishes (raw and cooked vegetables, soups), fish, eggs, meat and soy-bean dishes. At the bottom are dairy products and fruit. As in the Mediterranean Diet pyramid, people running on summit of the spinning top represent the importance of a regular physical activity. Finally, the guide recommends drinking plenty of water or tea and to moderate the consumption of highly processed snacks, confectionary and sugar-sweetened beverages (Fig. 2).
Okinawa Island is the largest of the Okinawa archipelago and the Ryukyu (Nansei) Islands of Japan and is one of the five “Blue Zones”, being home to some of the world’s longest-lived people whose present the lowest risk of aging-associated diseases [13]. This is mainly due to adherence to a healthy and sober diet, but also to the synergy with a relaxed lifestyle, low levels of pollution and population-specific genetic determinants [146].
The traditional Okinawa diet is low in calories yet nutritionally dense, particularly with regard to vitamins, minerals, and phytonutrients with nutraceuticals activity. Although it differs from the Japanese diet for some characteristics, there are many elements in common, such as the high intake of vegetables and soy derivatives, the low consumption of fat, the usage of seaweeds and miso and the almost total absence of dairy products. The most striking differences are represented by the fact that the traditional Okinawa staple carbohydrate is not rice but sweet potato, while herbs and spices are used instead of salt. In addition, only moderate quantities of fish are consumed. The traditional cuisine of this island is laden with vegetables and fruits (therefore phytonutrient and antioxidant rich) but reduced in meat, refined grains, saturated fats, sugar, salt, and full-fat dairy products [147, 148]. Indeed, the total quantity of animal products in the traditional Okinawan diet is very low, representing less than 10% of the total calories [147, 148]. The traditional dietary pattern in Okinawa has the following characteristics: (i) high consumption of vegetables, spices and herbs (many of which have medicinal properties); (ii) high consumption of legumes (mostly soy); (iii) moderate consumption of fish products (especially in coastal areas), (iv) low consumption of meat and meat products (mainly lean pork); (v) low consumption of dairy products; (vi) moderate alcohol consumption; (vii) low caloric intake; (viii) low fat intake (high mono and polyunsaturated-to-saturated fat ratio; low omega-6/omega-3 ratio); (ix) high fiber intake; (x) emphasis on low-glycemic index (GI) carbohydrates and (xi) high consumption of tea and moderate consumption of alcohol [147, 148].
The benefits of Japanese diets: Scientific evidences
Following Ancel Keys pioneering study [56, 138], several evidences have demonstrated that Japanese diet reduces the incidence of many chronic diseases, allowing the achievement of healthy longevity.
Tumors. Data published by the British Medical Journal showed that a closer adherence to Japanese dietary guidelines was associated with a reduction of total mortality and mortality from tumors [149]. Consistently, the onset of obesity-related tumors was lower in the Japanese population, compared with people from US. [150]. Among Okinawans, in particular, the onset of colon, prostate and breast cancers is about 50% lower than in the rest of Japan [147]: this effect could be largely due to the limited intake of fats, the very low omega-6/omega-3 ratio and the large amounts of antioxidant and anti-inflammatory substances ingested with the diet [147, 151].
The high intake of salt and salt preserved foods have been correlated with the onset of stomach cancer that occurred in the past in Japan (excluding the Okinawa prefecture) with a higher prevalence compared to European and North American countries; however, in recent years, due to the recommendations for healthy eating [145], this aspect has been gradually improved [152, 153].
Cardiovascular Diseases. The traditional Japanese diet has been associated with an extremely low rate of onset of coronary diseases, mainly owing to the high consumption of omega-3 fatty acids [151]. However, the risk of being affected by stroke and cerebrovascular disease is quite high in the Japanese metropolitan areas, excessive salt consumption, stress, smoking and alcohol may account for the higher prevalence of hypertension [139, 154]. The traditional Okinawa diet, on the contrary, further reduces the risk of coronary diseases and protects from the onset of strokes and cerebrovascular disease [147, 148].
Type II Diabetes. Traditional Japanese and, in particular, Okinawan foods guarantee an excellent control of glycaemia [147]. The very low GI, the presence of fibers, antioxidant compounds and the low omega-6/omega-3 ratio strongly prevent the onset of diabetes mellitus [151]. Accordingly, a low caloric intake diet, very similar to the traditional Okinawan regime, determine a 30% reduction, on average, of both glucose and circulating insulin levels [155].
Obesity. The prevalence rate of obesity in Japan is only 3-4%, much lower than in the United States and European countries, partially explaining why the percentages of other NCDs are also reduced [156, 157]. Even better results are achieved eating the Okinawan foods, which are very rich in bioactive substances that help to maintain an ideal weight management [147].
Neurodegenerative Diseases. A very recent clinical trial, involving more than a thousand Japanese followed up for a median of 15 years, has shown that a high intake of soybeans and derivatives, vegetables, seaweeds, fish and fruit and a low intake of rice is associated with a reduced risk of developing Alzheimer’s disease [158, 159].
Microbiota and Japanese Diet. The traditional Japanese diet, rich on fermented foods plenty of fiber and poor in fat, promotes the development of a healthy intestinal microbiota whose metabolites can exert anti-inflammatory and antitumor activities [160].
Japanese diets and longevity
Various scientific evidences have documented the beneficial effects of traditional Japanese and Okinawa diets against the onset of the major chronic diseases that affect the industrialized countries. Many characteristics of traditional Japanese diets are shared with the Mediterranean diet, including high intake of unrefined carbohydrates, low glycemic load, high consumption of phytonutrients and antioxidants compounds, healthy fat profile (high in mono/polyunsaturated fats, low in saturated fat, omega-3 rich), low caloric intake and a moderate protein intake (mainly of plant and fish origin). The combined action of all these elements may reduce global oxidative stress and inflammation, contributing, together with an active and healthy lifestyle, to maintain an excellent general state of health, diminishing the risk of developing aging-associated diseases and thus promoting healthy aging and longevity [141, 162].
Japanese diets and nutraceuticals
Table 2 illustrates some of the most frequently consumed foods of the traditional Japanese menu and their health benefits. Foods, nutrients and bioactive compounds shared with the Mediterranean diet (fish, vegetables, grains, fruit, dietary fiber, phytonutrients, etc.) are reported in Table 1.
Nutraceutical properties and health benefits of the most representative Japanese foods
Nutraceutical properties and health benefits of the most representative Japanese foods
The Vegetarian diet does not present a precise ethnic-geographical connotation but identifies, on the basis of ecological, ethical, religious or health motivations, a set of food practices that partially or totally exclude foods of animal origin. Nevertheless, all the different types of vegetarianism (Table 3) are characterized by an extremely high and varied consumption of plant-based foods (grains, legumes, vegetables, fruits, nuts, seeds, vegetable oils, herbs, and spices) [163].
Types of vegetarian diets [163]
Types of vegetarian diets [163]
According to a 2010 study, approximately half billion people are vegetarians, 75 million for choice and 1450 million for necessity, corresponding to 21.8% of the entire world population [164]. Ethics and ecology are two of the reasons why people in Western countries adopt a Vegetarian diet. The ethical motivations concern not only the respect for animals but also for human life: indeed several evidences support the health benefits of a Vegetarian diet. From the ecological point of view, the drastic reduction of meat consumption and animal origin foods present positive environmental repercussions. A plant-based foods diet, in fact, produces a strong decrease of greenhouse gas emissions, thus reducing the environmental damage [38, 166]. The ecological and the ethical questions are somehow closely associated: actually, the world population is projected to grow by 34% in 2050, raising the overall food demand of roughly 70%. The transition to eating habits with a higher content of vegetables, primarily the Vegetarian diets, could reduce this food gap by 30% [167].
The “Academy of Nutrition and Dietetics” stated that “ ... appropriately planned vegetarian, including vegan, diets are healthful, nutritionally adequate, and may provide health benefits in the prevention and treatment of certain diseases. These diets are appropriate for all stages of the life cycle, including pregnancy, lactation, infancy, childhood, adolescence, older adulthood, and for athletes. Plant-based diets are more environmentally sustainable than diets rich in animal products because they use fewer natural resources and are associated with much less environmental damage” [163].
The initial food recommendations for vegetarians have tended to be adapted from guides developed for non-vegetarians, instead of being designed to emphasize the healthy components of vegetarian dietary patterns. In order to develop a nutritionally adequate guide for vegetarians, various specific tools for planning meals have been recently developed, among which the food pyramids [168, 169] and the very newly defined VegPlate [170]. The vegetarian diet pyramid, similarly to the Mediterranean and Japanese food guides, recommends regular physical activity, adequate water and fluids intake (alcohol and sugar free), and a high consumption of variety of plant and unrefined foods. Moreover, it suggests sunlight exposure to stimulate vitamin D synthesis and vitamin B12 supplementation if no dairy or eggs are consumed. At the base of the pyramid are placed whole grains, legumes, vegetables and fruits, unsaturated fats as nuts, seeds and vegetable oils are located on the following step and, finally, at the top of the pyramid are positioned dairy products, eggs and sugars [168].
The benefits of vegetarian diet: Scientific evidences
A significant amount of studies has demonstrated the health benefits of vegetarian and plant-based diets, which have been associated with a reduced risk of diabetes, obesity, cardiovascular disease, different types of cancer as well as increased longevity, as described below [163, 171]. It is likely that these advantages result from both a reduced consumption of potentially harmful dietary components, such as saturated fat, cholesterol, animal protein, red meat, and heme iron, and an increased consumption of beneficial dietary components, including fruit, vegetables, whole grains, legumes, nuts and seeds, which are rich in dietary fiber, antioxidants and phytochemical compounds [171].
Tumors. The “Adventist Health Study-2” (AHS-2) showed that Vegetarian diets are associated with a lower risk of occurrence of all types of tumors, particularly gastrointestinal and prostate cancers [172]. Furthermore, vegetarians showed an 18% reduction in cancer incidence compared to non-vegetarians [173].
Cardiovascular Diseases. The most consistent evidence of the beneficial effects of plant-based diets is the strong decrease in cardiovascular disease risk factors. Several studies, in fact, have shown a lower incidence of coronary heart disease among vegetarians: in particular, in a combined analysis of 5 prospective studies, the mortality risk for ischemia in vegetarians was 24% lower compared to meat consumers [163, 171]. Moreover, a very recent comprehensive meta-analysis proved that a vegetarian diet shows a 25% reduction in ischemic heart disease incidence and/or mortality [174]. Interestingly, the adoption of a vegetarian diet is able to bring about regression of even severe coronary atherosclerosis without use of lipid-lowering drugs [175].
Type II Diabetes. Vegetarian diets provide also significant benefits for the prevention and management of type II diabetes. Several observational studies, in fact, have demonstrated a significantly lower risk of diabetes in individuals following Vegetarian diets when compared with non-vegetarians. For instance, in the AHS-2 people following vegan and lacto-ovo vegetarian diets had a reduced risk of developing type II diabetes between 50–68% and 38–46%, respectively, compared to non-vegetarians [171, 177]. Whether the reduction in risk of diabetes in vegetarians can be attributed to the absence of meat or to the higher intake of plant foods is still unclear. However, several works have shown a positive correlation between heme iron intake, red and processed meat, animal proteins and the risk of type II diabetes [171]. In agreement with this, red and processed meats are strongly associated with increased fasting glucose, insulin concentrations and diabetes risk [163]. In the past decades, several observational studies also provided significant evidences that Vegetarian diets improve glycemic control and blood lipids in patients with diabetes, being efficiently used as therapeutic tools in the management of type II diabetes [163].
Obesity. Plant-based dietary pattern are also associated with a lower BMI as shown in the AHS-2, in the EPIC-Oxford Study and in the Swedish “Mammography Cohort” study. Collectively, those observational researches identified the highest mean BMI among meat eaters and the lowest among vegetarians (vegans in particular [177]). In total agreement with those results, the therapeutic use of a vegetarian diet is more effective for treating overweight than omnivorous diets. Actually, foods related to a reduced risk of obesity, such as whole grains, vegetables and nuts are regularly consumed by vegetarians. On the other hand, a higher intake of red meat has been associated with an increased risk of weight gain [163, 171].
Microbiota and Vegetarian Diet. A well-functioning gut is essential to ensure optimal health preventing allergies, food intolerances and many other diseases. Adherence to vegetarian diets not only increases the concentration of anti-inflammatory and anti-tumoral short-chain fatty acids in the feces, but also determines a strong decrease in the concentration of the dangerous atherosclerotic compound TMAO [111, 178]. Moreover, a very recent publication highlighted that a lacto-ovo-vegetarian diet is particularly effective in modulating microbial activity, contributing to a significant reduction of the genotoxic and cytotoxic risk in the gut [179].
Vegetarian Diet and Longevity
Consistently with the above-mentioned data, several scientific researches provided significant evidences that vegetarian diets increase lifespan [171]. Therefore, it is not surprising that one of the world’s longest-living populations is represented by the vegetarians from the Seventh-day Adventist community of Loma Linda in California, a group of about 9000 people living in the core of the United States’ “Blue Zone” region [12, 13].
Since 1960, the University of Loma Linda have studied more than 150000 individuals of this peculiar community, in order to find a relationship between eating habits, lifestyle and their longevity. The first study, the “Adventist Mortality Study”, (1960–1965), demonstrated that the mean lifespan of these persons is approximately 5 years longer than other Californians, showing a 30% reduction in cancer incidence and an 18% decrease of CHD risk [180]. The purpose of the second study, the “Adventist Health Study 1”, (AHS-1) (1974–1988), which involved 34000 people over the age of 25, was to detect which features of the Adventist lifestyle were able to protect against diseases. In summary, this work demonstrates that not smoking, eating a plant based diet, consuming nuts several times per week, drinking more than 5 glasses of water a day, making regular physical activity and maintaining a healthy body weight increase lifespan up to 10 years [181]. The latest study, the AHS-2, whose aim is to include 125000 North American Adventists, started in 2002 and still ongoing, analyzes the relationship between lifestyle, eating habits and chronic diseases. Preliminary results have showed that vegetarianism has a potential protection against obesity and type II diabetes risk and that a vegetarian dietary pattern is associated with a lower risk of MetS [182–184].
Furthermore, other independent observational studies demonstrated both that a very low meat intake is associated with greater longevity [185] and that vegetarianism decreases the activity of Insulin-like Growth Factor-1 (IGF-1), a protein involved in aging regulation [186].
Tables 1 and 2 revise the most relevant health benefits offered by foods and nutrients characteristic of vegetarianism, which are shared with Mediterranean and Japanese diets.
The New Nordic Diet (NND)
The New Nordic Diet (NND), developed in 2004 in Copenhagen, is a paradigm of sustainable and healthy diet that integrates cuisine and dietary habits from the five Nordic countries: Denmark, Finland, Iceland, Norway and Sweden [187]. NND shares many elements with the traditional Mediterranean and Japanese diets: (i) it employs locally and organically grown foods such as fresh fruits (mainly berries, apples and pears), vegetables, legumes, nuts, seeds, whole grains, fish, aromatic herbs, mushrooms and seaweeds; (ii) it contains low amounts of fat, meat and sweets and avoids processed food.
Despite being a very recently developed diet, many clinical trials have already demonstrated that the NND is able to lower the incidence of several chronic diseases, thus increasing the overall life span. The New Nordic Diet can be therefore defined as another prototype of health, food culture palatability and environmental sustainability.
The new Nordic diet pyramid
In November 2004, the chefs Rene Redzepi and Claus Meyer, founders of NOMA restaurant in Copenhagen, invited chefs and food professionals from all the Nordic countries to a symposium on new Nordic Cuisine. This event gave rise to what is now known as the “New Nordic Cuisine Movement” and signed the promotion of the “The New Nordic Cuisine Manifesto”, which expresses in 10 aims the values on which a New Nordic cuisine must be based in order to define its flavors and identity in the world. The Manifesto promotes a cuisine based on purity, season, ethics, health, sustainability, quality, simplicity and freshness. Menus were inspired by traditional dishes and ingredients characteristic of the Nordic region, in order to create a common Scandinavian food culture, which could represent a healthy regional alternative to the Mediterranean cuisine [188]. A year after the creation of the Manifesto, the Nordic ministers of fisheries, agriculture, forestry and food announced their support for the New Nordic Food program, signing the Århus Declaration [188]. In northern Europe, as in the rest of the western world, the prevalence of overweight and obesity, among both adults and children, has increased enormously over the last 60 years, thus raising the risk of developing a wide range of serious NCDs. Promoting a healthy diet was therefore essential to prevent and solve many of these public health issues. For this reason, the Scandinavian institutions adopted the principles displayed in “The New Nordic Cuisine Manifesto” to establish the “New Nordic Diet” (NND) [189]. The 2011 Baltic Sea Diet Pyramid (summarized in Fig. 3) adequately represents the nutritional characteristics and recommendations of the New Nordic Diet [190]. The NND primarily encourages the consumption of local organic foods such as fruit (especially berries, apples and pears), vegetables (wild aromatic herbs, cruciferous vegetables, green leafy vegetables and edible plant roots), mushrooms and legumes. The complex carbohydrates intake comes from whole grains (rye, oats and barley) and potatoes. A regular unsaturated fat ingestion is also recommended eating mainly nuts and seeds. Other foods characteristic of this type of diet, which should be eaten with moderation, are skimmed dairy products, fish (salmon, sardines, mackerel, herring), eggs, white meat and canola oil (as substitute of the extra virgin olive oil typical of the Mediterranean cuisine). The consumption of local red meat and fat dairy products is allowed only in rare occasions. As usual, on the top of the pyramid are located processed food and products rich in sugars and fats (Fig. 3).
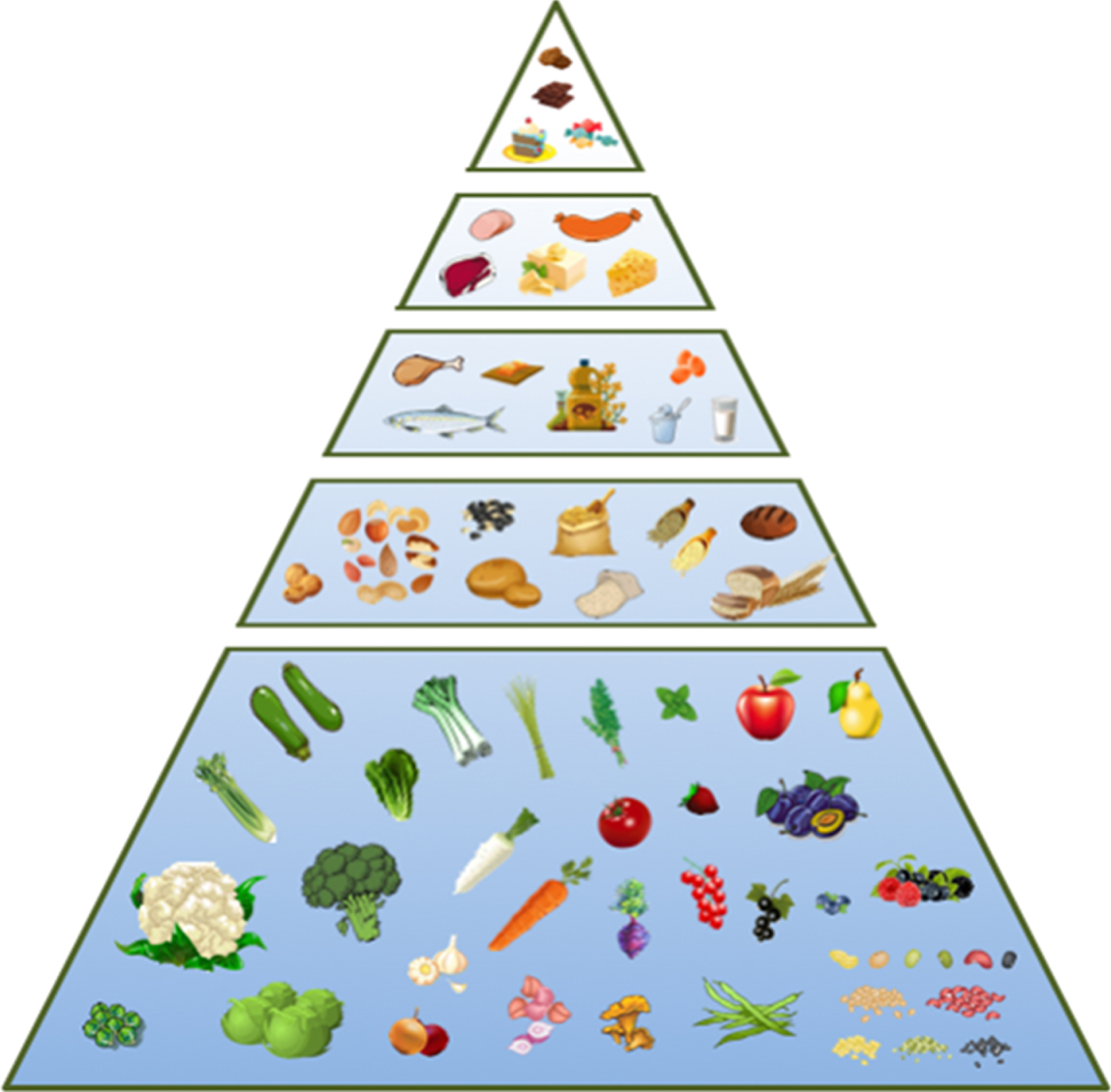
The New Nordic Diet Pyramid. Schematic representation of the nutritional characteristics established by the Baltic Sea Diet Pyramid, which adequately exemplifies the recommendations of the New Nordic Diet [190].
The messages underlying the NND guidelines are basically three: (i) more calories from plant foods and fewer from meat; (ii) more foods from the sea and lakes (including mollusca and seaweeds); (iii) more foods from the wild local countryside (plants, aromatic herbs, mushrooms and berries) [189].
The most recent revision of the Nordic nutrition guidelines, moreover, recommend to reduce salt consumption (do not to exceed 2.4 g of sodium per day), limit alcohol intake and avoid a sedentary lifestyle (at least 30 minutes of daily physical activity) [191]. They also suggested an adequate intake of carbohydrates, fats, and proteins: carbohydrates should provide up to 45–60% of the total energy, fat should constitute the 33% of the calories (10–20% MUFAs, 5–10% PUFAs and less than 10% SFAs) and proteins no more than 15% [191]. Finally, due to the limited sun exposure, vitamin D supplementation is strongly suggested, especially for newborns and adults aged 55 and over [191].
Despite its recent definition, the NND, which is naturally rich in fiber, omega-3 fatty acids and antioxidant compounds, has already been the subject of several epidemiological studies, which have shown the effectiveness of this eating habit in the prevention and treatment of major non-communicable diseases (type II diabetes, tumors, cardiovascular diseases, obesity), as listed below in detail [192, 193].
Tumors. The 2011 prospective cohort study, “Diet, Cancer and Health Study”, which involved more than 50000 Danish ages 50 to 64 surveyed for about 12 years, showed a significant reduction in overall mortality in those who followed the NND (which included fish, cabbage, rye bread, apples, pears and edible plant roots) [194]. Within the same cohort, a 9% decrease in colorectal cancer incidence was also observed [195]. Consistently with these results, consumption of fibers-rich NND foods was significantly associated with lower risk of colon cancer [193]. Finally, a very recent research has shown that a higher adherence to both Mediterranean and New Nordic Diet, after colorectal cancer (CRC) diagnosis, is associated with better overall survival in long-term CRC survivors [196].
Cardiovascular Diseases. Many clinical trials conducted on several Nordic European populations have shown that the healthy Nordic diets determine a reduction in several key cardiovascular disease risk factors of similar magnitude as those previously reported for the Mediterranean diet [197]. Specifically, the NND improves blood lipid profile [198], has a favorable impact on blood pressure in hypercholesterolemic patients [199], lowers diastolic blood pressure and mean arterial pressure in subjects with features of MetS under weight-stable conditions [200] and reduces blood pressure in centrally obese individuals [201].
Type II Diabetes. The whole grains-rich foods characteristic of NND demonstrated a probable protective effect against the onset of type II diabetes [193]. Moreover, a recent clinical trial, conducted for 6 months in Denmark on obese individuals, showed that NND improves insulin resistance index, yielding promising results for the treatment of both type II diabetes and metabolic syndrome [202].
Obesity. The New Nordic Diet is also effective in the control of overweight: the loss of fat mass, in the previously mentioned group of obese individuals, was more pronounced consuming the NND than an average Danish diet [202]. Similarly, ad libitum New Nordic Diet produces weight loss in centrally obese individuals [201].
Neurodegenerative Diseases. Some protective effects of the New Nordic Diet against neurodegeneration have been identified. Actually, the consumption of a NND diet appears to display a positive association with cognition in middle-aged and elderly individuals with normal levels of comprehension [203] and people who followed the dictates of a Swedish kind of NND are protected against memory loss or cognitive decline [204].
New Nordic diet and longevity
Although relatively young, NND positive health benefits have already emerged, thus is reasonable to assume that a high adherence to the New Nordic Diet can help to achieve a healthy longevity, as already preliminary demonstrated by Tjonneland’s group [194]. The aim of this research was to develop a food index based on traditional Nordic foods (with expected health-promoting effects) and relate it to mortality in a cohort of 57053 Danes aged 50–64 years: they found lower mortality among middle-aged individuals who scored high on a traditional healthy Nordic food index [194].
New Nordic diet and nutraceuticals
Table 4 illustrates some very frequently consumed foods characteristic of the New Nordic Diet and their health benefits. Foods, nutrients and bioactive compounds shared with Mediterranean and Japanese diets (fish, vegetables, legumes, seaweeds, whole grains, fruit, dietary fiber, phytonutrients, etc.) are reported in Tables 1 and 2.
Nutraceutical properties and health benefits of the most representative New Nordic Diet foods
Nutraceutical properties and health benefits of the most representative New Nordic Diet foods
Aging is not only the leading risk factor for major chronic diseases, but also the causal element of the overall decline of physical and cognitive performance. To unravel the biological mechanisms underlying causes of senility, many theories were developed and several researches conducted using different experimental models, from bacteria to primates. Caloric restriction (CR) is one of the most robust interventions able to extend life expectancy and delay the onset of multiple age-associated diseases in diverse species, from yeast to mammals. Specifically, CR refers to the reduction of total calorie intake by 20–40% without causing malnutrition or deficiency in essential nutrients. However, despite being so successful in health and longevity promotion in laboratory animals, long-term CR in humans can have both beneficial and detrimental effects [205].
CR belongs to the group of Dietary Restrictions (DRs), which encompass several other dietary interventions, such as: (i) normocaloric diets with specific macronutrient deficiencies (Protein Restriction, PR; sulfur amino acids restriction, known as Methionine Restriction, MR); (ii) Fasting (complete lack of food intake or a 60% or higher food restriction); (iii) Intermittent Fasting (IF), including fasting every other day (Alternate Day Fasting, ADF) and fasting two or more consecutive days every two weeks or every month (Periodic Fasting, PF) and (iv) Fasting Mimicking Diet (FMD) [206, 207].
The four categories of abovementioned dietary interventions, which do not necessarily imply a caloric decrease, have the potential to enhance lifespan and promote healthy aging in humans without producing any harmful health effects [205].
Brief history of caloric restriction
Although studies concerning the link between longevity and diet have increased over the last 30 years, this topic has interested scientists since the dawn of human origins. Hippocrates and Galen were the firsts to hypothesize that very fat persons might die suddenly than slim ones, while, in the mid of the 1500, the nobleman Alvise Cornaro, in his “Discourses”, theorized on the advantages of a radically reduced diet based on personal experience [208]. Cornaro’s theories influenced many later researchers: in 1914 Francis Peyton Rous demonstrated that reduction of energy intake decreased cancer occurrence in rodents [209]; subsequently, in 1917, Thomas Burr Osborne and Gregor Mendel proved that CR prolonged life and reproductive capacity of female rats [210]. In the same year, Loeb and Northrop showed that Drosophila melanogaster’s lifespan could be prolonged decreasing food availability [211, 212]. However, sustained research on caloric restriction began only in 1930, when Clive McCay demonstrated that reducing caloric intake without causing malnutrition nearly doubled lifespan in rats [208, 213]. Studies on caloric restriction expanded rapidly over the 20th century [212], in particular in the eighties, when Roy Walford and Richard Weindruch showed that dietary restriction in mice increases mean and maximum lifespans and inhibits the occurrence of many spontaneous cancers [214, 215]. Starting from nineties, the studies on CR moved on monkeys and humans, demonstrating reduced risk factors for age-associated diseases, but yielding conflicting results on life expectancy extension [212].
In general, however, the effects of CR on health and longevity have been confirmed in many organisms (yeasts, Caenorhabditis elegans, Drosophila melanogaster, zebrafish, rodents and dogs), suggesting that this dietary intervention could act on specific genetic pathways conserved across different species [205].
Effects of caloric restriction on biological and genetic mechanisms of aging
Although many hypotheses have been proposed, the fundamental biological and genetic mechanisms, which mediate CR effect on lifespan and health, are still unknown. Different hypotheses aimed at explaining these processes have been proposed.
Biological Mechanisms. The first hypothesis proposed is the Retardation of Growth Hypothesis, which claimed that CR increases the longevity of rats by retarding their growth [397]. This theory was challenged by different studies that found it wanting, however it can be possibly applied to mice but not to rats [216].
Although there is strong evidence against the Reduction of Body Fat Hypothesis, which assumed that CR’s life extension is due to a decrease in body fat content, efforts have recently been made to reconsider this theory after the discover that sirtuin, a protein playing an important role in the life-extending action of CR, is able to decrease fat mass in mammalian white adipose tissue [216].
The Reduction of Metabolic Rate Hypothesis is based on studies showing that reduction of food intake in humans decreases the metabolic rate and that mammalian interspecies inverse relationship between species longevity and its metabolic rate per kilogram body mass. Although several recent researches established that this theory is not supported by any robust experimental findings, it nevertheless still has advocates [216].
Currently, the most popular concept is the Oxidative Damage Attenuation Hypothesis: since 1956, in fact, it has been proposed that ageing is due to damage caused by free radicals originated mainly from mitochondria [217]. Several studies provide support for this hypothesis, showing that CR decreases the formation of ROS and increases the activity of enzymes that protect from oxidative damage. Despite the evidences indicating that caloric restriction protects from damage caused by oxidative stress, it remains to clarify whether CR’s ability to attenuate oxidative damage plays a major role in its life extending action [216].
The Altered Glucose–Insulin System Hypothesis and the Alteration of the Growth Hormone–IGF-1 Axis Hypothesis have been gaining favor, and data have emerged that link these two hypotheses. Thus, it may now be more appropriate to refer to them as the Attenuation of Insulin-Like Signaling Hypothesis. This theory is supported by the fact that fasting levels of plasma glucose, insulin and plasma insulin-like growth factor-1 (IGF-1) are lower in rodents on a CR regimen [216].
The last theory is the Hormesis Hypothesis, a concept that embraces many of the other proposed hypotheses. Hormesis refers to the phenomenon whereby a beneficial effect (improved health, stress tolerance, growth or longevity) results from exposure to low-intensity stressors (such as caloric restriction) that is otherwise toxic or lethal when given at higher doses. Recent findings suggest that CR activates hormetic defense mechanisms in organisms ranging from yeast to mammals, stimulating a response against a variety of stress thus retarding senescent processes [216].
Molecular and genetic mechanisms. Although the molecular and genetic mechanisms that mediate the effect of caloric restriction involve several systems and tissues, influencing thousands of genes, some of the pathways implicated in the resistance to stress and in the propagation of metabolic and insulin signaling have been investigated, characterized and related to the aging process. Depending on the organism and the type of dietary restriction applied, one or more of the following nutrient-sensing pathways are involved in life expectancy extension: (i) the kinase target of rapamycin (TOR); (ii) AMP-activated protein kinase (AMPK); (iii) sirtuins; (iv) insulin/IGF-1 signaling and (v) the Ras pathway [205, 218].
TOR. The kinase target of rapamycin TOR is involved in the regulation of autophagy and protein translation, playing a key role in cellular metabolism processes. In C. elegans, D. melanogaster and mice, chronic dietary restriction increases lifespan by downregulating TOR activity [205, 218]. In worms and flies, lifespan extension requires autophagy, while in all three species inhibition of translation, by TOR target ribosomal S6 kinase inactivation, increases lifespan [218]. Rapamycin, a known pharmacological inhibitor of TOR, can extend lifespan in yeast, C. elegans, D. melanogaster as well as in mice [218].
AMPK. This highly conserved enzyme works as a sensor of adenosine monophosphate (AMP) and adenosine diphosphate (ADP) levels. When AMP/adenosine triphosphate (ATP) ratio rises, AMPK is activated and inhibits TOR, thus triggering autophagy [219]. Indeed, in mammals, dietary restriction stimulates AMPK, while excessive nutritional intake hinders its action hence promoting the appearance of obesity, diabetes and cardiovascular disease. Recent studies have proved that the activation capacity of AMPK and its responsiveness to different insults decline during aging. Several researches on lower organisms have shown that increased AMPK functionality leads to an extended lifespan [219].
Sirtuins. Sirtuins are NAD+-dependent protein deacetylases whose overexpression has been described to extend lifespan in yeast, C. elegans and D. melanogaster. Silent mating-type information regulation 2 (Sir2), the prototype of sirtuins, was one of the first longevity genes to be identified in worms and flies. However, it is not yet clear how sirtuins influence life expectancy. In mammals, which express seven sirtuins variants (Sirt1-Sirt7), the Sirt1 enzyme, homologous to Sir2, regulates glucose and insulin production, lipid metabolism and cell survival, supporting a potential role for sirtuins in mediating caloric restriction effects on lifespan extension. Although a recent publication demonstrated that Sirt6 over-expression can extend lifespan in male mice [220], further studies are needed to clarify the role of these proteins in mammalian aging and longevity control [218, 221]. However, these enzymes are supposed to play an important role in improving healthspan and lifespan elongation [222]. Resveratrol, a non-flavonoid phenol with anti-inflammatory and antioxidant activity, is able to activate sirtuins and extend lifespan in worms and flies [223]. In addition, it protects human cells from a variety of stresses (including gamma radiation) and exerts a beneficial effect on age-associated diseases [223, 224].
The insulin/IGF-1 pathway. As previously described, this was the first pathway shown to influence ageing in C. elegans, D. melanogaster and rodents. Indeed, functional alterations in insulin and IGF-1 receptors or in the components of their downstream kinases cascade were effective in extending lifespan [218]; moreover, several researches demonstrated that dietary restrictions-related inhibition of the insulin/IGF-1 signaling pathway result in lifespan extension in worms, flies and mice [205, 218]. Interestingly, mutations known to impair insulin/IGF-1 pathway have been linked to an increased longevity in several groups of centenarians [218].
The Ras pathway. Activation of the insulin/IGF-1 pathway causes, in turn, the stimulation of Ras protein family members. These peptides belong to a superfamily of small GTPases that transmit signals from cell-surface in order to activate several downstream processes as proliferation, differentiation, apoptosis, senescence and metabolism [225]. Hyper-activation of Ras is highly oncogenic: approximately one-third of human tumors, in fact, present mutations in the Ras gene. Deletion of RAS2 in the budding yeast has long been known to extend chronological lifespan, while in D. melanogaster reduction of Ras or of its targets Erk activity is sufficient to increase longevity [225]. In mammals there is not enough data available to correlate the increase in life expectancy with Ras mutations: however, fibroblasts isolated from long-lived species of birds and mammals showed an altered Erk phosphorylation in response to stress, suggesting a possible link between Erk activity and longevity [225].
Effects of caloric restriction on human healthspan and lifespan
The biological, genetic and molecular mechanisms described above contribute to the complex etiology of aging and, if modified, can lead to a substantial increase in life expectancy in animal models. Many of these mutations decrease the activity of pathways linked to metabolism, insulin and insulin-like signals, simulating situations of starvation, which may occur in nature. Consistently, it has been observed that restriction on food intake without malnutrition extended the lifespan of yeasts, worms, flies, fish and rodents. Moreover, in rodents and monkeys, both dietary restriction and decreased nutrient-sensing pathway activity can lower the incidence of age-related non-communicable diseases [5].
Due to these promising findings, CR has begun to be tested in both monkeys and human volunteers. In macaques, CR significantly reduces the onset of many chronic and age-related disorders [5]: however, results on lifespan extension on these primates are quite contrasting, requiring further investigation to understand whether CR might efficiently increase longevity in monkeys [205, 226–228].
Consistently with the results obtained in apes, accumulating data indicate that, in humans, moderate CR with adequate nutrition exerts a powerful protective effect against chronic and age-dependent diseases [5]. Following the success of the CR experiments conducted in rats [214, 215], Roy Walford tested, for two years, on himself and 7 colleagues, the effects of CR during the natural experiment conducted in the Biosphere 2 study. A low caloric intake diet was able to reduce blood sugars of 21%, cholesterol of 30%, blood pressure of 23.5%, and body mass index of 12 to 22% [155]. More recently, new short-term studies of CR in humans have been conducted, in 2 phases, as part of the multicenter study Comprehensive Assessment of the Longterm Effects of Reducing Intake of Energy (CALERIE). In the first phase of CALERIE studies (CALERIE-I), the metabolic effects of 6 or 12 months of a restriction of calorie intake by 20–30% in overweight individuals showed favorable changes in BMI, body composition, glucoregulatory function, and serum risk factors for cardiovascular disease [224]. In the second phase of CALERIE studies (CALERIE-II), 2 years effects of 25% CR in healthy lean individuals were investigated. Results published so far indicate that the beneficial effects of caloric restriction observed in the CALERIE-I studies are sustained with prolonged restriction in energy intake for 24 months. CR individuals, in fact, displayed reduced inflammatory markers and a decreased risk of cardiovascular diseases [224, 229]. Additional studies on CR applied to humans demonstrated that this DR is highly effective in reducing the risk of atherosclerotic disease, C-reactive protein expression [230] and in attenuating oxidative stress while increasing verbal memory improvement in the elderly [231]. Moreover, physical activity, combined with CR, has additional benefits, decreasing more effectively blood pressure and circulating LDL, increasing bone mass in post-menopausal women and ameliorating insulin sensitivity [231]. However, long-term CR can have harmful consequences on human health, such as hypotension, loss of libido, menstrual irregularities, female infertility, weakness, impaired regulation of body temperature, bone mass reduction, psychological distress and impaired wound healing [205, 232]. Therefore, although CR can reduce the burden of several NCDs, long-term CR may cause a global weakness, increasing the risk of incurring even in disease-related premature deaths [233].
Effects of other dietary restrictions on human healthspan and lifespan
Other dietary interventions, which do not require an overall reduction in calorie intake, have emerged to be less invasive than CR and more effective to promote human healthspan and lifespan [205].
In particular, PF has the potential to reduce inflammation in patients with rheumatoid arthritis and to decrease chemotherapy side effects. IF is able to reduce body weight, visceral fat, circulating insulin and blood pressure levels and to improve insulin sensitivity. ADF improves autoimmune diseases, insulin sensitivity, asthma and seasonal allergy symptoms, central nervous system inflammatory lesions, cardiac arrhythmias and menopausal symptoms [231, 234–237]. Finally, Short Term Starvation (STS) protects patients against chemotherapy side effects, increases the efficacy of cancer therapies and helps to prevent malignancies [238, 239]. Another promising intervention that is emerging as a method to promote a healthy longevity is the reduction of proteins and amino-acid intake. For instance, a recent analysis of the National Health and Nutrition Examination Survey (NHANES) provided evidences that protein intake reduction was associated with decreased overall mortality for individuals under 65 years of age. Moreover, consumption of over 20% of calories from proteins had a 4-fold increased risk for cancer mortality and a 75% increase in overall mortality, compared to subjects which consume less than 10% of calories from proteins [205, 231]. However, in a plant-based derived protein source diet, the association between high protein intake and mortality was abolished, whereas that on cancer mortality attenuated [206].
In order to identify a dietary intervention that induces the abovementioned beneficial effects, while minimizing the risk of adverse effects and the burden of complete food restriction, some researchers developed a diet that mimics the effects of fasting, namely the Fasting Mimicking Diet (FMD).
The fasting mimicking diet (FMD)
A recent publication has described the effects of a fasting mimicking diet tested first on pre-clinical animal models and then in clinical trials [240]. The FMD, characterized by a very low calorie/low protein value, determined changes in markers associated with stress resistance or longevity (IGF-1, ketone bodies and glucose), similarly to those caused by fasting. Mice fed with the FMD (4 days, twice a month and then nourished ad libitum in the period between FMD cycles) showed a clear improvement in the general health status. Specifically, they displayed a decrease in visceral fat (preserving muscle mass), an attenuation of bone loss in old animals, muscles and hepatic regeneration, reduced tumors incidence, protection against inflammation and inflammation-associated skin lesions, regeneration and rejuvenation of the immune system, improved motor coordination, cognitive performance and long-term memory, promotion of neurogenesis and lengthening of life span in middle-to old mice [240]. To evaluate the feasibility and impact of this FMD in humans, a pilot clinical trial on 38 healthy adults was conducted (19 following the FMD and 19 consuming their normal diet, as controls). This plant-based diet, which was followed for 5 days every month, for 3 months, provided between 34 and 54% of the normal caloric intake with a composition of 11–14% proteins, 42-43% carbohydrates and 44–46% fat. The FMD subjects showed fat loss without reducing lean body mass, C-reactive protein expression decrease and reduction of risk factors/biomarkers for aging, diabetes, cardiovascular disease, and cancer [240]. These preliminary data indicate that fast mimicking diets have the potential to promote human healthspan. Further studies by Prof. Longo’s group provided additional evidences of FMD beneficial health effects, including an improvement of demyelination processes and symptoms of auto-immune encephalomyelitis in mice [241], the enhancement of chemotherapy efficacy in rodents [242], the restoring of insulin production in islets from type I diabetes patients and reverse both type I and type II diabetes phenotypes in mouse models [243] and the reduction of blood pressure, IGF-1, glucose, triglycerides and cholesterol in healthy individuals [244]. In order to confirm the effect of the FMD on disease prevention and treatment, it is crucial to further analyze a higher number of participants, including subjects presenting a diagnosis of a specific NCD and those at higher risk of developing cancers or aging-related diseases.
Conclusions
The scientific evidences presented in this review demonstrated that each of the described diets promotes the achievement of a healthy longevity, modulating the aging-related biological pathways and preventing the onset of the major NCDs, finally increasing lifespan. In agreement with that, residents of the “Blue Zones”, areas of exceptional longevity around the world, follow three out of the five dietary habits analyzed, namely Mediterranean, Japanese and Vegetarian Diet [12, 13]. Moreover, all the eating habits described here share several strong anti-aging effect features: (i) high usage of plant-based food and whole grain products with low GI, which are naturally rich in fibers, vitamins, minerals and phytonutrients with nutraceutical activity that protect against age-related diseases [245–252]; (ii) consumption of unsaturated fats with a high mono- and polyunsaturated-to-saturated fat ratio and omega-3 rich, which reduce the risk of cardiovascular pathologies [253–255]; (iii) moderate protein intake, mainly of plant origin, except for a modest ingestion of fish, which is an excellent source of omega-3 fatty acids [256]; (iv) extensive use of medicinal, aromatic plants, essential oils and spices, very rich in antioxidant and anti-inflammatory compounds [257]; (v) moderate- or no- alcohol ingestion; (vi) low- or no-consumption of meat (especially red meat), processed and packaged foods, simple sugars and saturated fats, which are all associated with an increased risk of obesity, type II diabetes, cardiovascular diseases, neuroinflammatory disorders and various cancer types [258–260].
The efficacy of some dietary restrictions in promoting human healthspan and lifespan is in agreement with the dietary habits of the traditional diets (Mediterranean and Japanese in particular), which are low in calories and recommend not eating until feeling full. In particular, after the Second World War, our ancestors for social, cultural and economic reasons used to skip meals or eat very frugal menu. Moreover, together with a limited caloric intake and unplanned intermittent fasting, they had a very active lifestyle, which increased the total energy expenditure thus subjecting the body to a positive stress (hormesis) able to counteract the aging processes [216]. Indeed, a regular physical activity is strongly recommended in all the dietary habits examined. Several scientific studies, in fact, provided evidences that habitual and moderate-intensity exercise primarily prevents, or delays, chronic diseases and decreases the risk of mortality being predictive of healthy longevity [261–263]. A regular physical activity reduces oxidative damage enhancing resistance to oxidative stress [264] and is positively associated with leukocytes telomere length (LTL). Actually, LTLs of most active subjects were longer than those of the least active ones; therefore, a sedentary lifestyle may accelerate the aging process [265].
All the above mentioned emerging evidences clearly demonstrate that a key strategy to reduce the burden of non-communicable diseases is to adopt a mostly plant-based diet, which favors the consumption of local organic foods, to reduce the environmental impact, and that is also suited to personal ethics, traditions and socio-cultural context. In order to further stimulate the metabolic pathways of longevity, it may be useful to insert regular supervised intermittent fasting periods.
Although recent and accumulating scientific evidences indicate that diet has prominent role in controlling the mechanisms of aging and aging-associated diseases, in order to become even more effective in preventing the risk of NCDs and slowing down the aging process, more work is needed to further understand how calorie intake, specific nutrients and bioactive compounds modulate the key metabolic pathways underlying aging and age-related disorders.