
Abstract
BACKGROUND:
To date, the Individual Placement and Support (IPS) model is the only vocational intervention that has been rigorously studied and shown to be effective with Veterans with spinal cord injury (SCI). Customized Employment (CE) is an innovative vocational intervention with promising results among people with disabilities which has yet to be tested in persons with SCI.
OBJECTIVE:
To determine whether a Customized Employment (CE) intervention adapted for SCI rehabilitation is more effective than the standard care (IPS) for helping Veterans with SCI obtain and maintain employment.
METHODS:
A 4-year, 2-site randomized clinical trial (RCT) with concurrent mixed methods using an intent-to-treat (ITT) approach. The primary outcome is competitive integrated employment as defined by the Work Innovation and Opportunity Act. Secondary outcomes are employment indicators, quality of life (QOL), and participation.
RESULTS:
This is a methods paper so there are no results to present at this time.
CONCLUSION:
The proportion of Veterans who attain employment will be greater for the CE group than the IPS group and they will outperform the IPS group on other employment-related metrics (e.g., higher job satisfaction, wages, and retention). Employed Veterans will demonstrate significant improvements in self-sufficiency, QOL, and participation. Qualitative data obtained from interviews will assist with adaptation strategies and will identify barriers to implementing CE.
Keywords
Introduction
Background
Restoring employment is critical for Veterans with spinal cord injury (SCI). People with SCI view gainful employment as key to social reintegration (Cotner et al., 2018, Ottomanelli, O’Connor, Njoh et al., 2018; Hilton et al., 2018). Central to social participation, employment is a feature of overall functioning according to the International Classification of Functioning, Disability, and Health (World Health Organization, 2013). In a recent study of a large national cohort of Veterans with SCI (N = 1,047) treated by the Veterans Health Administration (VHA), less than 10% were currently employed (Goetz et al., 2018). This unemployment rate is alarming because it is associated with decreased quality of life (QOL) (Krause et al., 2012; O’Neill & Ottomanelli, 2018) and increased mortality, including suicide (Kennedy & Garmon-Jones, 2017). Employment improves QOL, well-being, and independence. Employed Veterans with SCI have greater social integration, productivity, and participation (Ottomanelli et al., 2013), all highly valued outcomes for Veterans (Cotner, 2018).
The VHA Vocational Rehabilitation Service provides recovery-oriented clinical services for Veterans with disabilities for whom the primary objective is competitive employment (Department of Veterans Affairs, 2019). Department of Veterans Affairs medical centers have Compensated Work Therapy programs offering Supported Employment (SE) and other vocational programs. In a recent study of Compensated Work Therapy for Veterans with mental health disabilities (N = 38,199) (Abraham et al., 2017), competitive employment outcomes were modest, but the highest rates resulted from emphasizing community employment. Research is needed to assess modifiable factors in VHA vocational services and to evaluate effective private sector vocational services not yet available within VHA (Drebing et al., 2012).
For Veterans with SCI, the Individual Placement and Support (IPS) model of SE (Roels et al., 2016; Trenaman et al., 2014), which integrates vocational services into rehabilitation and health care, demonstrates the best outcomes (Bond & Drake, 2014; Ottomanelli et al., 2012). IPS includes rapid job search and job development guided by consumer preferences, benefits counseling, and time-unlimited supports (Marshall et al., 2014). In two multi-center VHA studies of IPS for Veterans with SCI, employment rates were 25 and 43% (Ottomanelli et al., 2017). Although significantly better than usual care, these rates are lower than those for persons with mental health disabilities who receive IPS. After SCI, significant comorbidities and impairments likely contributed to a lower employment rate than other populations. Despite SE, Veterans with SCI take longer to locate and secure a job, and the majority do not obtain competitive employment (Post et al., 2020).
Customized employment as an innovative strategy to address barriers
Customized Employment (CE), a vocational rehabilitation intervention for people with complex disabilities (Smith et al., 2017) and an evolution of SE (Griffin et al., 2008), is “a flexible process designed to personalize the employment relationship between a job seeker and an employer in a way that meets the needs of both” (Office of Disability Employment Policy, 2002). It involves additional customization of job responsibilities and the workplace environment (Wehman et al., 2018) and a Discovery process that identifies individual interests, skills, and support needs prior to the job search. Personal networks and interpersonal relationships (social capital) are leveraged to forge workforce connections and engage a natural support system. CE emphasizes employer engagement to match specific needs of targeted employers with an individual’s skills and talents and ensures “the provision of reasonable accommodations and supports necessary for the individual to perform the functions of a job that is individually negotiated and developed” (Disability Employment Policy Office, 2002). The comprehensive process also integrates disability benefits analyses to identify appropriate work incentives and to enable informed decision-making on the part of the job seeker. CE strategies of employment matching and employment customization may provide additional means to help Veterans with SCI overcome employment barriers.
Discovery is the foundation of CE and distinguishes it from other employment interventions (Inge et al., 2018). Qualitative interviewing and observation are used to discover strengths and employability by interacting with the jobseeker, support systems, and communities to customize competitive, integrated employment (Workforce Innovation and Opportunity Act, 2014). Hence, CE differs from current practices by: (1) engaging the jobseeker in Discovery prior to initiating job development, (2) aligning with qualitative research approaches, and (3) relying heavily on social capital to connect job seekers with employment opportunities. Engaging Veterans in their natural social contexts using these distinctive CE strategies could enhance employment outcomes for Veterans with complex disabilities who need more intensive and customized services to address their unique employment barriers.
State of the science on customized employment
Despite the longstanding availability of CE, it has only recently become available through public vocational rehabilitation and VA systems. Although evidence indicates CE may be a promising strategy to support employment among persons with complex disabilities, it has not yet established the threshold of an evidence-based practice (Smith et al., 2019; Wehman et al., 2016; Citron et al., 2008; Luecking et al., 2008; Ellison et al., 2008; Luecking et al., 2006; Staines et al., 2004). Early studies, funded through the Office of Disability Employment Policy, showed promise for CE and informed Workforce Innovation and Opportunity Act legislation (Rogers et al., 2008; Riesen et al., 2015; Wehman et al., 2016). More recently, the Achieving Competitive Customized Employment through Specialized Services (ACCESS) intervention was developed as part of a National Institute of Mental Health (NIMH) pilot study to test a CE intervention for its utility in improving competitive employment outcomes for adults with autism spectrum disorders (Smith et al., 2019). The ACCESS model protocolizes the CE process and integrates a fidelity instrument, the Benchmarks of Quality Checklist (BQC), to measure the level of adherence to the CE process at the individual participant level. In Phase 1, open trial (N = 10), the study tested feasibility and acceptability of ACCESS. During the open trial, 100% of those who completed the ACCESS intervention achieved competitive integrated employment outcomes that align with the job seekers’ interests, skills, and talents. Phase 2 preliminary data analyses show linear increases in competitive, integrated employment rates, average weekly hours worked, and hourly wages (Smith et al., in development).
A recent review of the literature identifies 18 studies that 1) were published in a peer-reviewed journal; 2) clearly stated a research question or objective related to CE; and 3) included a summary of quantitative or qualitative data regarding employment outcomes or procedures (Riesen et al., 2022). Findings indicated that most CE research remains descriptive in nature, is not well defined, relies on small sample sizes with homogeneous populations, and has a shortage of RCT studies (Riesen et al., 2022). Furthermore, additional research is needed to determine which CE elements lead to competitive, integrated employment outcomes, and to examine how CE services impact people with disabilities (Inge et al., 2022; Riesen et al., 2022). Inconsistent implementation of the CE process has created an additional barrier to fully understanding this service strategy (Inge et al., 2022). In summary, while study findings support CE as a promising intervention to improve employment outcomes, future studies will benefit from increased scientific methodological rigor to establish a solid foundation of evidence of its effectiveness for Veterans with disabilities.
Critical gaps in the literature
There is consensus by vocational researchers and implementation experts in both the private sector and VHA that further research is needed on specifying and defining the evidence-based practices for CE (Inge et al., 2018) by: (1) evaluating how Discovery could translate into provision of ongoing job supports after job acquisition to ensure job retention, (2) determining how to train CE providers on the use of qualitative interviewing and participant observation skills and how to ensure fidelity when implementing CE, and (3) understanding how to facilitate the use of social networks (social capital) to improve employment outcome. These recommendations are consistent with the call for research among VHA vocational experts and researchers who state that CE is one of the most promising directions in the field and warrants study within the VHA (Drebing et al., 2018; Drebing et al., 2012; Staines et al., 2004; Wewiorski et al., 2018). Specifically, future vocational research in VHA is recommended on (1) efficacy of CE with a range of target populations, and (2) development and inclusion of fidelity measures assessed at the participant level.
To address these gaps, the ACCESS-Vets study will evaluate the effectiveness of CE in VHA for Veterans with SCI. The purpose of this study is to determine whether a Customized Employment (CE) invention adapted for SCI rehabilitation is more effective than standard care (IPS) for helping Veterans with SCI obtain and maintain employment. Specifically, this study examines the effects of a Veteran-driven CE intervention adapted from the studies of Achieving Competitive Customized Employment through Specialized Services (ACCESS) model with SCI. As the next step in developing evidence on CE, this research will evaluate whether CE can be adapted for use with fidelity within VHA vocational services. This mixed methods study will address knowledge gaps by obtaining data on (1) the CE process from Discovery through ongoing job supports and its impact on outcomes; (2) how standardized training in qualitative skills and well-specified benchmarks facilitate CE fidelity; and (3) how CE, including the use of social networks, reduces barriers to employment goals. This study is innovative in examining CE within healthcare and will determine whether collaboration between CE providers and VA rehabilitation teams strengthens CE practice and reduces or eliminates barriers to employment for Veterans with SCI. The goal of this paper is to present the methods followed for this study in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines (Chan, 2013; Chan, 2013).
Research hypotheses and qualitative questions
To determine the effectiveness of CE in the VHA clinical setting, our primary hypothesis is that compared to the IPS Supported Employment group (treatment as usual, [TAU]), the CE group will show a greater proportion of employment attainment (H1.1). The secondary hypothesis states that for Veterans who attain employment, the CE group will achieve higher job satisfaction, wages, and job retention, than the IPS group (H1.2). Regardless of intervention, we hypothesize that Veterans who attain employment will demonstrate greater improvements in self-sufficiency, quality of life, and participation in life roles, compared to Veterans who do not (H2.1).
Veteran and provider qualitative interviews will improve understanding of impact of employment on Veterans’ lives (Q2.1), and identify strategies used in CE and TAU, to address barriers to employment (Q3.1). Qualitative data will also identify how practitioners adapt the CE intervention for use in the VHA clinical setting (Q3.2).
Methods
Participants
The study is open for enrollment at two VHA SCI/D Centers and their affiliated clinics located in the eastern region of the United States who serve a combined active registry of 2,747 Veterans with SCI. Recruitment for the study will be restricted to English-speaking Veterans over 18 years of age who want to find work in their community and who have received or are currently receiving IPS. Veterans will be excluded if they live more than a two-hour drive from the recruited VA medical center, have a progressive or terminal spinal cord disorder (e.g., multiple sclerosis), moderate to severe traumatic brain injury, a psychosis diagnosis within the previous 6 months, or an untreated substance use disorder. Any visual, hearing, or cognitive impairment that would prevent providing informed consent or being able to participate in essential study and intervention activities will also be used as criteria for exclusion from the study sample. To ensure adherence to human subjects’ protection regulations, this study was reviewed by the VA Central Institutional Review Board (CIRB), and the local VA Research and Development Service (R&D) committees.
Quantitative sample size
The sample size was determined from power calculations drawn from expected group differences in competitive and integrated employment attainment (H1.1). An assumption of a 37% probability of employment for the IPS group was drawn from previous studies (range: 25% -43%). Unpublished results of the ACCESS program have shown success rates of over 75%. A conservative competitive and integrated employment attainment rate of 65% for the CE group was assumed. A sample size of 100 subjects (50 per treatment arm) will provide 80.9% power (2-sided α= 0.05) to detect a difference in proportions of 0.28 (i.e., difference between 0.65 and 0.37). The sample size calculation accounts for this difference between the two treatment arms occurring at any of the employment assessment timepoints. Using effect sizes and notations from Cohen (1988), the sample size is sufficient to detect a moderate standardized effects size of 0.4.
Statistical power for testing the secondary hypotheses was calculated with an N = 100 for each of the proposed models and by treating all secondary outcomes as continuous. Attrition was ignored in all power analyses as all randomized Veterans will be included in the analysis by performing missing data imputation. The hypothesized employment attainment rates and sizes of treatment arms were used to estimate a subsample of 32 veterans assigned to CE and 18 to IPS who will attain competitive and integrated employment and be assessed under H1.2. Under the assumptions of a first-order autoregressive covariance structure, 1.0 standard deviation of a single observation, alpha level of 0.05, and correlation between observations on the same subject ranging from 0.3 to 0.5, the study is expected to be sufficiently powered to detect a minimum standardized difference between 0.5 and 0.6 (medium effects size).
Additionally, a power analysis was performed for longitudinal linear mixed-effects models. Due to multiple outcomes with potentially different and unknown parameters, the application’s default value of 0.5 was accepted for the amount of baseline variance at the subject level and 0.03 for the ratio of the random slope variance to the within-subject variance. On these assumptions, an N = 100 achieves 83% power to detect a medium Cohen’s d effects size of 0.6.
Qualitative sample size
At each of the two sites, 15 Veterans and 10 Providers (vocational providers a SCI interdisciplinary team members) will be purposively sampled and invited to be interviewed via telephone. Qualitative interview sample size was determined with the goal of achieving conceptual saturation. Saturation has been noted to occur within the first 12 interviews (Sandelowski, 1995; Strauss & Corbin, 1998). Purposive sampling of providers will be completed with input from study-wide team members and vocational providers to facilitate representation of interdisciplinary team members.
Measures
Quantitative
The primary quantitative outcome is competitive integrated employment defined as “full or part-time work at minimum wage or higher, with wages and benefits similar to those without disabilities performing the same work, and fully integrated with co-workers without disabilities” (Civic Impulse, 2015, p. 571). Veteran data on rates of attainment of competitive and integrated employment (H1.1), employment-related metrics, and QOL metrics will be collected via Qualtrics, a remote and secure data collection platform for completing online self-reported surveys. Participants who achieve employment will be followed up until we have 3 post-employment data points, at 3-month intervals extending up to 18 months from baseline. Quantitative measures are outlined in Table 1.
Quantitative domains, measures, and timepoints
Quantitative domains, measures, and timepoints
1Measures will be collected from employed participants beyond 12 months from Baseline through 3 post-employment time points or until the data collection period ends.
To address the study’s qualitative questions, three sources of data will be used: (1) telephone interviews will be conducted to evaluate CE and IPS experiences among Veterans, and to collect implementation data from providers; (2) open-ended question responses from the Benchmarks of Quality Checklist will provide information on how CE providers adapted or modified the intervention, and (3) open-ended question responses from the online Employment Questionnaire will provide information on accommodations, supports, transportation, and barriers. Demographic information (e.g., sex, race, ethnicity, age) to describe the provider sample will be obtained using a short demographic survey via telephone.
Interviews will be scheduled for 30–45 minutes and conducted via telephone. Veteran participants will be interviewed up to 3 timepoints, baseline, 9 months, and 12 months to capture their experiences over time. Provider participants will also be interviewed at three implementation timepoints during the study intervention period: To guard against bias, two qualitative researchers, who are not involved in development or delivery of the interventions will conduct the interviews. A team-based approach to interviewing will be used to increase reliability and the potential for new insights (Eisenhardt, 1989).
Interviews will be open-ended and conversational but will follow specific questions developed with input from the research team to ensure all topics are covered. Interviewers will solicit attitudes, opinions, and reports about preferences and pros and cons of CE, including perceptions of usefulness, facilitators and barriers to employment, perceived value of the intervention in addressing quality of life and participation; and for provider interviews, how the intervention was adapted.
Standard communication techniques will be used to stimulate discussion, with prompts, summarizing statements, and silence. Interviews will be recorded using a VA-approved encrypted recorder with a telephone interview adaptive device. These recordings will be downloaded and stored on a secure network server at the primary site. Recorded documents will be remotely retrieved, and professionally transcribed and reviewed by the study team for completeness of information. Open-ended responses from the Employment questionnaire and BQC provider notes will be extracted for analysis.
Fidelity measures
Fidelity measures will be collected every six months after the intervention period begins to assess adherence to the treatment methodologies, and to describe constancy of treatment across the participant pool. CE practitioners will complete the Benchmarks of Quality Checklist (BQC) to document fidelity to the CE model. Additionally, data obtained from the BQC will guide practitioners as they implement CE by providing information on common barriers to implementation, and by providing creative solutions and alternative approaches to CE steps. Fidelity to IPS will be measured by the IPS Fidelity Scale (Bond et al., 1997) which will be completed by the supervisors of the IPS vocational specialists at each site.
Procedures
Prospective participants will be drawn from the pool of participants listed in the SCI registries at both study sites. Veterans will be contacted through IRB-approved letters. Additional recruitment will be performed through SCI team member referrals and self-referrals obtained through flyers located in SCI clinic areas and via VA approved social media. Veterans who are screened eligible for inclusion/exclusion criteria will be referred to the study coordinator for further screening and consent (see Fig. 1).
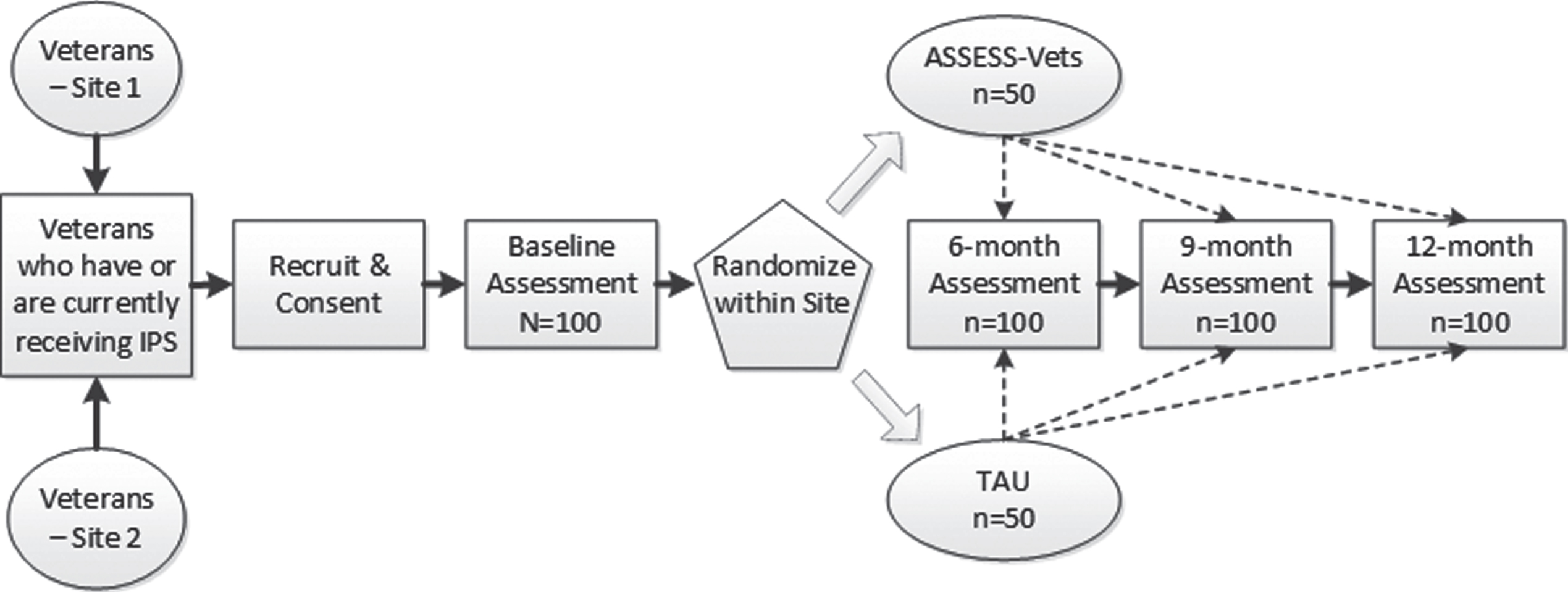
Study flow chart.
The CE treatment arm elements include Discovery, CE planning, job development, CE negotiation, and accommodations and job retention supports (see Table 2). CE intervention will follow the ACCESS model and will be informed by The Essential Elements of Customized Employment for Universal Application. ACCESS improves upon CE by standardizing its application via tools, templates, and logs, and is supported by the BQC fidelity instrument.
Customized Employment (CE) intervention
Customized Employment (CE) intervention
The IPS treatment arm, also known as evidence-based supported employment, will serve as an active control group consistent with TAU. IPS treatment includes the elements of zero exclusion, integrated services, competitive employment, rapid job search, worker preferences, systematic job development, benefits planning, and time-unlimited supports.
Participants will be randomly assigned to the CE or IPS treatment arms based on an a priori generated matrix, stratified by (1) site and (2) by functional severity of the SCI. SCI functional severity was based on the American Spinal Injury Association Impairment Scale (AIS) rating of SCI impairment (AIS A, B, or C vs AIS D) (Scivoletto et al., 2014). The AIS stratification reflects the relatively good prognosis for functional walking among individuals with AIS D SCI (Scivoletto et al., 2014). Participants, clinical team members, and project managers will be blinded to the participants’ assigned treatment groups until after baseline data collection. The data manager assigned to the study will ensure blinding and use the matrix to assign treatment in temporal order of study enrollment.
Treatment will be administered by vocational specialists trained in content modules associated with the treatment groups. Both treatment arms are expected to take 8 months or less depending on individual participants needs. The ACCESS intervention developers (two study Co-Investigators) will provide intensive training to vocational specialists providing the CE treatment. VA clinical vocational specialists already trained in IPS will be used to administer the IPS treatment. Ongoing technical assistance and mentorship for vocational specialists providing the CE treatment will be provided both in group settings and individually and through in-person, email, and phone mediums. IPS assistance will be provided through extant staff meetings, conference calls, and monthly field call.
To test the primary hypothesis (H1.1), chi-square test analyses will be used to compare rates of competitive integrated employment between the treatment arms at baseline and by 6-, 9-, and 12-months (See Fig. 2).
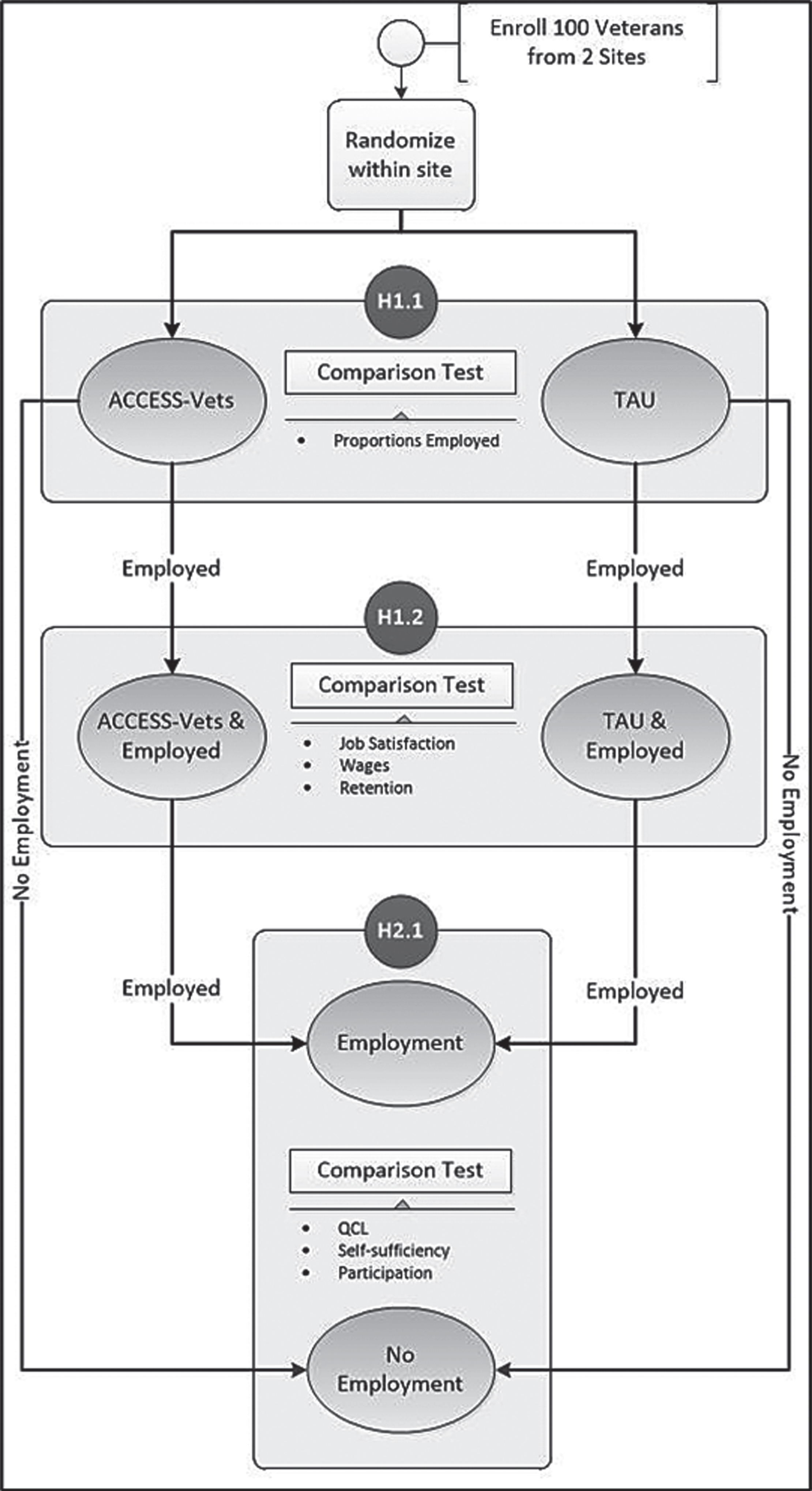
Binary group comparisons proposed for hypothesis testing.
To test whether CE results in higher job satisfaction, wages, and retention than IPS (H1.2), generalized estimating equations will be used to test the time-averaged difference in both groups by specifying an auto-regressive [AR(1)] correlation structure for the longitudinal continuous data. Intervention will be the main explanatory variable while clinical site, contact time, and other explanatory variables that show significant group differences will be included as covariates. A significantly positive coefficient of the intervention variable will support the hypothesis.
H2.1 will be tested using data from all Veterans who attain employment, regardless of intervention assignment. We will test whether the employed group shows greater improvement over time than the no-employment group separately for each continuous outcome (self-sufficiency, quality of life, and participation) by fitting linear growth models specifying random intercept and slope. Each model will include an intervention-by-time interaction term that tests for significant difference in the two group slope trajectories (improvement) of the outcome.
Missing data will be investigated by tabulating attrition of Veterans stratified by intervention group and dropout time. Missing completely at random principles will be assumed if there are no significant differences between the stratified trajectories of the missing data. Missing outcome values will be imputed using multiple imputation with chained equations. Additionally, Veterans who drop out will be compared with those who do not on each outcome, intervention group, and baseline variables by using cross tabulations with correlation tests (Cramer’s V, point-biserial), t-tests, or chi-squared tests as appropriate.
Matrix analysis, a rapid assessment approach (Beebe, 2001), will be used to identify and summarize themes from open-ended responses from the employment questionnaire and BQC provider notes. Interview transcript data will be managed and coded in Atlas.ti, a qualitative analysis software program, using descriptive content analytical methods to identify domains and taxonomies of participant CE experiences (Drebing et al., 2012). Systematic coding of text is a key to qualitative data analysis as codes represent underlying assumptions (Miles & Huberman, 1994). An initial set of codes for research domains will be identified and defined a priori. A codebook will be developed to include code names, definitions, inclusion and exclusion criteria, and an exemplar that illustrates how code may be presented within the text codebook (Guest & MacQueen, 2008). New codes will be developed if unidentified themes arise during analyses. Categories will be compared, and relationships identified. As coding schemas are developed to create domains and taxonomies, data samples will be extracted and coded by qualitative research team members and evaluated for inter-rater reliability at 80% with periodic checks of reliability to ensure consistency and limit potential drift in coding (Huberman & Miles, 2002). Initial themes will be reviewed by the team to enhance credibility, and alternative explanations for data patterns will be discussed to strengthen internal reliability and build explanatory power (Yin, 2003). Any discrepancies will be discussed and resolved. Descriptive and comparative matrices that identify patterns of regularities (shared) and inconsistencies (unique or varied) will then be constructed for Veterans and providers. Comparative matrices enable identification of the most relevant, shared, and perhaps representative components and, thereby, enhance the potential representation of the findings. Finally, a complex cross-case data matrix will be developed to summarize the significant taxonomic outcome structures identified within and between Veterans. This process of descriptive and comparative matrix analysis will enable detection of the most salient and representative components identified by Veterans and providers. This analysis will examine site variations in adapting the intervention for use in VHA.
This clinical trial provides an opportunity to establish an evidence base for customized employment which is currently considered a best practice (Riesen et al., 2022). The protocolized ACCESS intervention includes a fidelity measure to ensure the CE process is implemented consistently across time and place. By conducting this study with a novel population (Veterans with SCI) within the VA system, public sector VR programs may benefit from data that identifies practices and approaches unique to the VA system including interdisciplinary team involvement to provide more seamless services and supports, a primary vocational rehabilitation specialist who works with the Veteran through the full CE process, and a post-employment support system that is not time limited. It is anticipated that collection of qualitative data from Veterans and interdisciplinary team members will provide additional insight regarding strengths and weaknesses of the intervention and aid in the process of identifying specific variables that contribute to successful attainment of competitive, integrated employment.
Conclusion
The expected outcomes based on study hypotheses are that proportion of Veterans who attain employment will be greater for the CE group than the IPS group and they will outperform the IPS group on other employment-related metrics (e.g., higher job satisfaction, wages, and retention). It is expected that employed Veterans will demonstrate significant improvements in secondary measures of self-sufficiency, QOL, and participation. Qualitative data obtained from interviews will assist with adaptation strategies and will identify barriers to implementing CE. These outcomes will be reported in future publications and presentations to the field and disseminated through VHA communication channels.
Footnotes
Acknowledgments
The authors acknowledge the leadership support of this work by their steering committee and clinical partners which include: the VHA National Program Offices of Spinal Cord Injury and Disorders Services and Vocational Rehabilitation; local Compensation Work Therapy Programs at the Tampa and Richmond VA Medical Centers; and the Physical Medicine and Rehabilitation Service Vocational Rehabilitation staff at the Tampa VA Medical Center; along with consultative support from the Director of the Rehabilitation Research and Training Center at Virginia Commonwealth University.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics statement
This study was approved by the Department of Veterans Affairs, VA Central Institutional Review Board Panel 2, James A. Haley Veterans Hospital (no. 1643929-1; 21-11 Tampa).
Funding
This paper represents research funded by the VA Office of Research and Development, VA Rehabilitation Research and Development (RR&D) grant #D3349 R. The views expressed in this paper are those of the authors and do not represent the views of the Department of Veterans Affairs or the United States Government.
Informed consent
This minimum risk study received a waiver of documentation of informed consent approved in the VA Central IRB Form 112b. Verbal consent was provided by study participants after they were informed of the study procedures and requirements, and had all questions and concerns addressed. Participation in the study was voluntary and participants could withdraw from the study at any time without adverse consequences.