
Abstract
BACKGROUND:
Medical ethics guidelines require of clinical trial investigators and sponsors to inform prospective trial participants of all known and potential risks associated with investigational medical products, and to obtain their free informed consent. These guidelines also require that clinical research be so designed as to minimize harms and maximize benefits.
OBJECTIVE:
To examine Merck’s scientific rationale for using a reactogenic aluminum-containing “placebo” in Gardasil HPV vaccine pre-licensure clinical trials.
METHODS:
We examined the informed consent form and the recruitment brochure for the FUTURE II Gardasil vaccine trial conducted in Denmark; and we interviewed several FUTURE II trial participants and their treating physicians. We also reviewed regulatory documentation related to Gardasil vaccine approval process and the guidelines on evaluation of adjuvants used in human vaccines.
RESULTS:
It was found that the vaccine manufacturer Merck made several inaccurate statements to trial participants that compromised their right to informed consent. First, even though the study protocol listed safety testing as one of the study’s primary objectives, the recruitment brochure emphasized that FUTURE II was not a safety study, and that the vaccine had already been proven safe. Second, the advertising material for the trial and the informed consent forms stated that the placebo was saline or an inactive substance, when, in fact, it contained Merck’s proprietary highly reactogenic aluminum adjuvant which does not appear to have been properly evaluated for safety. Several trial participants experienced chronic disabling symptoms, including some randomized to the adjuvant “placebo” group.
CONCLUSION:
In our view, the administration of a reactive placebo in Gardasil clinical trials was without any possible benefit, needlessly exposed study subjects to risks, and was therefore a violation of medical ethics. The routine use of aluminum adjuvants as “placebos” in vaccine clinical trials is inappropriate as it hinders the discovery of vaccine-related safety signals.
Keywords
Background
Clinical trial patients put themselves in harm’s way often because they wish to contribute to the progress of medical science and trust that the risk of their participation is minimized. Codes of medical ethics treat informed consent as an essential safeguard to this risk. The very duty to obtain free and informed consent arises out of the respect for the autonomy of the person in deciding whether to participate in an experiment [1]. It is paramount that every known risk is disclosed to the patient, and it is for this reason that violations of informed consent are an egregious ethical transgression.
Randomized double-blind placebo-controlled studies are considered the “gold standard” of clinical studies, and when well designed and conducted provide the strongest evidence of causation. In such studies, the control is a placebo, an “inert” substitute for a treatment or intervention which by definition means “the compound has no known activity that would be expected to affect the outcome” [2]. As Rid et al. make clear with regard to vaccine trials: “Randomization and the use of placebo interventions are designed to control for confounding effects, such that significant differences in disease incidence or adverse effects between the vaccine and control groups can likely be attributed to the vaccine” [3]. A reactogenic placebo however, is a pharmacologically active substance masquerading as a “placebo control”; its use in clinical trials nullifies the very concept of a placebo-controlled trial.
The exceptional instances in which it is considered unethical to give an inert placebo are when withholding an active treatment from a patient could result in irreversible harm, and in therapeutic clinical trials which in terms of efficacy and safety aim to establish the superiority of new treatments over existing treatments in diseased patients [2]. However, administering an active control which may expose healthy trial subjects to risks only without any benefit is a violation of medical ethics guidelines which require that research involving human subjects be so designed as to minimize harms and maximize benefits [1].
In vaccine trials the use of inert placebos is clearly acceptable when no relevant safe and efficacious vaccine exists, and conversely, it is clearly unacceptable when (1) such a vaccine exists and is accessible to trial participants, and (2) the risks to participants of delaying or foregoing the available vaccine cannot be adequately minimized or mitigated [3]. Merck’s quadrivalent human papilloma virus (4vHPV) vaccine Gardasil was the first prophylactic HPV vaccine that gained regulatory approval for use in healthy girls and women [4,5], primarily for the prevention of cervical cancer: a disease which has been successfully prevented for many decades in the developed world through regular Pap smear screening procedures [6]. Given these facts, the use of an inert placebo in Gardasil clinical trials preceding regulatory approval appears to have been clearly warranted. Nonetheless, in all but the V501-018 trial in the V501 placebo-controlled pre-licensure clinical trial program (Table 1), Merck used their proprietary amorphous aluminum hydroxyphosphate sulfate (AAHS) adjuvant as the “placebo”. The V501-018 trial however, did not use a saline placebo either, but rather the Gardasil vaccine’s carrier solution which includes L-histidine, polysorbate 80, sodium borate and residual yeast protein which is a potential allergen [7,8]. Moreover, only 1,781 children between 9 and 15 years of age were included in this trial; both male and female who were randomized in a 2:1 ratio to receive either Gardasil or the “placebo” [8]. By contrast, the largest pre-licensure Gardasil trial V501-015 (the FUTURE II trial), recruited 12,167 subjects, all females between 15 and 26 years of age, who were randomized in a 1:1 ratio to receive either Gardasil or the AAHS injection [9]. It is thus highly questionable whether the V501-018 trial provided a reliable measure of safety for Gardasil given the small size of its study population. In this article, we examine Merck’s use of a pharmacologically active aluminum-containing “placebo” in the remaining Gardasil pre-licensure clinical trials that we believe compromised vaccine safety assessment, and was both scientifically and ethically unjustifiable.
List of pre-licensure randomized double-blind placebo-controlled clinical trials in the V501 clinical trial program
List of pre-licensure randomized double-blind placebo-controlled clinical trials in the V501 clinical trial program
AAHS: amorphous aluminum hydroxyphosphate sulfate; 4vHPV: quadrivalent HPV vaccine (HPV6/11/16/18 L1). *V501-011 and V501-012 were sub-studies within the V501-013 clinical trial protocol. V501-013 study includes all participants from the two sub-studies except for the 304 from V501-012 who were vaccinated with the monovalent HPV16 L1 vaccine. †Of the 939 V501-011 study participants who were randomized to receive the 4vHPV vaccine, 468 were randomized to receive a hepatitis B vaccine concurrently. ‡Of the 938 V501-011 study participants who were randomized to receive the AAHS placebo, 467 were randomized to receive a hepatitis B vaccine concurrently.
The immunostimulatory effects of aluminum adjuvants were discovered in 1926 [10]. Since then, two main types of aluminum-based adjuvants have been used in human and veterinary vaccines: aluminum oxyhydroxide and amorphous aluminum hydroxyphosphate. The former is often inaccurately referred to as “aluminum hydroxide”, although it is chemically AlO(OH) rather than Al(OH)3, while the latter is often inaccurately referred to as “aluminum phosphate”, although it is chemically Al(OH) x (PO4) y , rather than AlPO4 [11,12]. Merck’s AAHS has been used in licensed human vaccines since 1987 [13,14]. It is the sulfated form of aluminum hydroxyphosphate, and although both share a similar amorphous structure, AAHS has unique properties that may explain its ability to induce exceptionally high and long-lasting antibody responses [15–17].
Numerous studies confirm that adjuvants are intrinsically tissue damaging and proinflammatory agents, and that inflammation is essential for the development of humoral immunity [11,18–23]. Accordingly, Cain et al. showed that the magnitude of humoral immune responses elicited by three different aluminum adjuvant formulations was correlated with the quantity of induced proinflammatory cytokines and the numbers of inflammatory cells at the injection site [23]. A study in guinea pigs shows that in comparison to vaccines adjuvanted with traditional aluminum adjuvants, Merck’s Gardasil caused necrotic tissue damage and massive inflammation that persisted beyond one month post-injection [24]. These effects are consistent with the demonstrated role of damage-associated molecular patterns (which are biomarkers of tissue damage), in promoting the immunopotentiating effect of aluminum adjuvants [11,19,22,25,26]. Notably, at one month post-injection Gardasil-injected guinea pigs also showed significantly elevated levels of the liver damage marker gamma-glutamyl transferase [24]. Similarly, Wang et al. [27] found that mice that received multiple injections of the AAHS adjuvant, or a hepatitis B immunogen adsorbed to AAHS, both showed a higher immuno-inflammatory response and a higher number of necrotic foci in the liver compared to saline-injected mice. Interestingly, the pro-inflammatory and pro-necrotic effect of AAHS alone was greater [27].
The above-cited research confirms that increased immunopotency inevitably comes at the cost of increased inflammation-driven reactogenicity and reduced safety [18,19,22,28]. Accordingly, it is acknowledged that, “in animal models of autoimmune disease induction, inflammation is essential to break tolerance to self-antigens” [28]. This means that potent inflammatory adjuvants have the necessary biochemical properties to induce chronic systemic immune-mediated diseases in susceptible individuals. It is thus of concern that in comparison to traditional aluminum adjuvants AAHS was shown by Merck to be the most potent inducer of antibody responses [15].
Merck’s clinical trial data indicate that the 4vHPV vaccine’s systemic reactogenicity is largely driven by the AAHS adjuvant, since a similar percentage of systemic effects, including headache, fever, nausea and dizziness, have been observed in both Gardasil and AAHS-“placebo” recipients [29]. In various animal species injections of traditional less potent aluminum adjuvants at doses relevant to human exposure have resulted in neurophysiological impairments [30–42]. Moreover, gene expression analysis of spleen lymphocytes isolated from mice injected with either aluminum phosphate-adjuvanted tetanus vaccine or the adjuvant alone showed that the latter significantly upregulated many markers indicative of systemic toxicity, including inflammatory disease-related genes, oncogenes, and genes involved in cell stress and apoptosis [43]. The fact that these changes were observed in the spleen and far from the injection site warrants further research on the systemic immune-mediated effects of aluminum adjuvants as they may be related to the reported side-effects in humans [43]. In particular, besides injection-site reactions, aluminum adjuvants have been associated with allergic reactions, contact dermatitis, headache, arthralgia, myalgia, cognitive dysfunction, chronic fatigue syndrome, muscle weakness and delayed motor milestones [22,44–46]. There is therefore no scientific validation for the use of aluminum adjuvants as “placebos” in vaccine clinical trials. As Gøtzsche et al. argued: “The use of active comparators may make it impossible to detect serious harms of the HPV vaccines in the randomized trials if comparators cause the same or similar harms” [47]. Quite paradoxically, saline placebos are routinely used in animal studies of autoimmune disease induction that employ aluminum as the choice adjuvant for the purpose of breaking tolerance to co-injected protein or peptide antigens [48–51]. It is therefore highly problematic that a saline placebo control is considered a standard of good research in animal studies, but not in clinical trial studies involving human subjects.
Merck’s rationale for using AAHS as a “placebo” in Gardasil clinical trials
To investigate how Merck justified the use of the AAHS adjuvant “placebo”, Doshi et al. assembled the available information on five randomized 4vHPV Gardasil vaccine trials described as “placebo-controlled” [52]. They used six data sources: trial publications, register records, clinical study report (CSR) synopses, CSR main bodies, CSR protocols and informed consent forms. The results revealed a high degree of inconsistency in the terms used to describe the control arm across all trials and types of documents. For example, the published abstracts and register entries for four trials only referred to the control arm as “placebo” or “matching placebo”. Among all six data sources for all five trials (i.e., 30 documents in total), the accurate information on the AAHS “placebo” was found only in one CSR synopsis and two main CSR bodies.
Notably, in the informed consent forms for two trials Merck did not provide participants with any information regarding the contents of the control arm; while in the forms for three other trials Merck described the “placebo” with the following terms: (1) “placebo (which is a dose that contains no active ingredients)”; (2) “placebo … an inactive substance” or “placebo … an inactive solution”; and, (3) “inactive solution (containing aluminium 225 mcg/dose)”. As Doshi et al. [52] noted, this phraseology would have led many trial participants to conclude falsely that the placebo did not contain pharmacologically active ingredients.
The rationale for using an aluminum containing “placebo” was provided only in the CSRs of three trials (V501-012, V501-013 and V501-015), and was stated as follows: “The inclusion of aluminum adjuvant in both vaccine and placebo preserved the blinding of the study because it allowed the vaccine and placebo to be visually indistinguishable”. “The safety profile of Merck’s aluminum adjuvant is well characterised. On the other hand, the safety profile of the HPV 6, 11, 16 and 18 L1 VLPs required further evaluation in humans” [52].
The stated rationale that the AAHS “placebo” was necessary in order to preserve blinding is inaccurate and contradicted by the fact that Merck did use a carrier solution without the AAHS adjuvant in V501-018 4vHPV vaccine trial [7], and a saline placebo in a later nonavalent (9v)HPV vaccine trial. With regard to the latter, Garland et al. stated: “Because the 9vHPV vaccine (a whitish, semi-translucent suspension) and saline placebo (a clear colorless liquid) are visually distinguishable, they were prepared and administered by designated unblinded study personnel not otherwise involved in the care and management of the study participants. Integrity of the blinding procedures was assessed by designated unblinded sponsor and study site personnel not involved in any way in the conduct of the study”. “Saline placebo was used as the control which allowed an overall assessment of the safety/tolerability profile of all vaccine components, including antigenic proteins and adjuvant” [53].
Thus, if by Merck’s own admission, the use of a visually distinguishable saline placebo did not compromise blinding (much less the assessment of vaccine safety), in one trial, then there appears to be no legitimate reason why the same placebo could not have been used in all Gardasil trials.
In the protocols for three of the five 4vHPV vaccine trials, Merck described the “placebo” as a “standard aluminum diluent” [52]. It appears misleading to describe the proprietary AAHS adjuvant that is only used in a handful of Merck’s vaccines as a “standard aluminum diluent”. Moreover, Merck’s claim that “the safety profile of AAHS is well characterised” [52] appears to lack scientific support. In fact, all clinically approved aluminum-based adjuvants currently in use in human and veterinary vaccines require further validation of their safety.
Aluminum adjuvant safety: What are the facts?
A comprehensive review of the existing literature on toxicology of aluminum adjuvants points to a glaring lack of scientific data validating their often claimed excellent safety record [54–56]. For example, in a 2022 systematic review and meta-analysis of studies assessing biodistribution, clearance and neurotoxicology of aluminum adjuvants in animal models, Masson et al. identified 31 eligible studies, of which 17 focused on neurotoxicological impacts [30]. Of these 17 studies, 13 showed numerous detrimental effects [31–38,40–42,57,58], 12 of which mimicked human or veterinary levels of aluminum adjuvant exposure [31–37,40–42,57,58]. Notably, studies in sheep demonstrated that accumulation of aluminum in the spinal cord was higher after the injection of the adjuvant alone than after the injection of adjuvanted vaccines [59]. Furthermore, although compared to phosphate-buffered saline injected controls, animals injected with aluminum-adjuvanted vaccines, and those injected with aluminum only, both displayed behavioral abnormalities [32], the latter group showed significantly greater alterations in brain gene expression [31]. In these animals aluminum altered genes linked to neurodegenerative and autoimmune disorders, and genes involved in neuronal cell survival, mitochondrial energy metabolism, inflammatory responses, oxidative stress and DNA damage control [31]. Unlike sheep, small rodent species are routinely dismissed by drug regulatory agencies as irrelevant to human immunobiology [22]. Nonetheless, some vaccine developers argue that there remains a need for a better scientific explanation as to why small animal data showing adjuvant toxicity are not relevant to human use [22] [emphasis added]. Supporting this argument, numerous studies have shown that irrespective of the species used, injectable aluminum (unlike that ingested), is neither efficiently excreted, nor does it remain localized at the injection site. Rather, it can migrate to distant organs (including the brain), where it accumulates and persists long-term, exerting toxic effects [30,31,35,39,41,42,44,58–64].
Although adjuvants have been in use for over eight decades, research of their safety remains scarce. In fact, in 2004 the World Health Organization (WHO) Global Advisory Committee on Vaccine Safety (GACVS) stated regarding the safety of adjuvants, that, “This hitherto neglected subject is becoming increasingly important given modern advances in vaccine development and manufacture” [65]. At an earlier meeting GACVS noted that, “Safety issues will require a thorough understanding of the effects of adjuvants on the immune response and related mechanisms … Adjuvant safety is an important and neglected field” [66]. Although the statements at this meeting relate to the research and development of new adjuvants, they nonetheless apply equally to aluminum adjuvants. This is because to date, after almost 100 years of use, the way in which aluminum adjuvants interact with the immune system remains obscure [11,54,67–69]. For this reason, in the contemporary scientific literature, aluminum adjuvants are still sometimes referred to as the immunologists’ “dirty little secret” [70]. This catchy phrase was coined by one of the leading immunologists of the 20th century, Charles A. Janeway [71], who began to unravel the mechanisms by which adjuvants enhance immune responses to foreign antigens [70]. Unsurprisingly, mechanisms of adjuvant toxicity are even less well understood than the mechanisms by which adjuvants enhance vaccine immunogenicity [22]. It is thus perplexing that the allowable amount of aluminum in human vaccines was selected exclusively on the basis of efficacy, not safety considerations [56], even though it is acknowledged that for prophylactic vaccines given to predominantly healthy individuals safety is to be prioritized over efficacy [72,73].
The reason why mechanisms of adjuvant toxicity remain poorly understood is revealed in the following disclosures by the world’s top regulatory health agencies and vaccine experts: (1) “historically, the non-clinical safety assessment for preventive vaccines has often not included toxicity studies in animal models because vaccines have not been viewed as inherently toxic” [72]; (2) pharmacokinetics/biodistribution, immunotoxicity carcinogenicity and genotoxicity assessments are not required for vaccine formulations that include existing aluminum adjuvants [69,74,75]; (3) although animals cannot be dispensed with in preclinical safety testing of adjuvants and notwithstanding significant progress to date in this area of research, there are currently no validated animal models that can accurately predict the immunotoxicological risks associated with adjuvants intended for human use [22,66,69]. Accordingly, vaccine developers have acknowledged that “it is not currently known what types of pre-clinical tests would be appropriate in determining whether an adjuvant is immunologically safe or not” (i.e., whether it can either induce or exacerbate immune disease in susceptible individuals) [22]. From these statements it is apparent that significant hurdles still need to be overcome before the safety of both existing and new adjuvants can be adequately assessed. The often heard claims that aluminum adjuvants have a long “established” and “demonstrated” safety record [54–56] are thus unsupported.
Informed consent in Merck’s FUTURE II trial of Gardasil in Demark
The FUTURE II trial (V501-015) was Merck’s largest Gardasil clinical trial in which the “placebo” contained the AAHS adjuvant (Table 1). In Denmark trial participants were not informed about the AAHS in the “placebo”, instead, the informed consent form and the recruitment brochure stated that the “placebo” was either a vaccine without an active substance or saline [76]. As shown in Fig. 1, the key passage in the informed consent form states, “One half of the participants will receive the active vaccine, while the other half will get the placebo vaccine (meaning a vaccine without active substance)”. Figure 2 shows Merck’s advertisement informing potential participants that they would be receiving a saline placebo (“saltvand”). In contrast, the study protocol explained that the “placebo” contained AAHS, and so trial investigators, unlike trial participants, knew that the control was not saline [52,76].
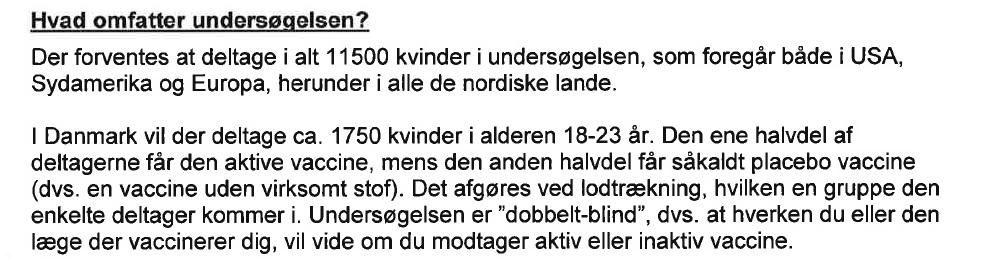
Excerpt from Merck’s informed consent form in Denmark for the FUTURE II Trial. Translation: “In Denmark there are 1750 women that will participate, between the ages of 18 and 23. One half of the participants will receive the active vaccine, while the other half will get the placebo vaccine (meaning a vaccine without active substance). It is decided by lottery, which group the participant will be in. The test is ‘double-blind’, meaning that neither you nor the doctor that vaccinates you, will know if you receive an active or inactive vaccine”.
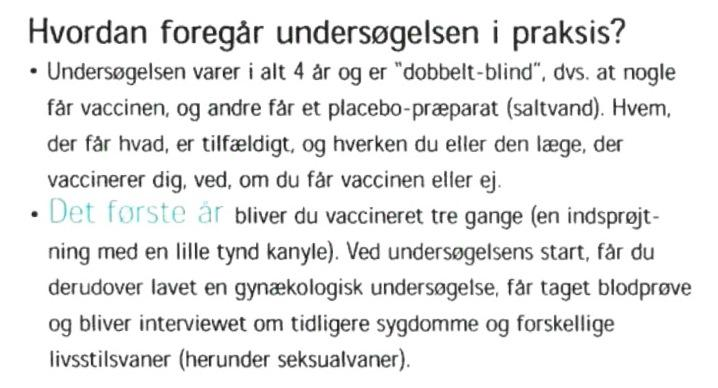
Excerpt from Merck’s recruitment brochure in Denmark for the FUTURE II Trial. Translation: “How is the study conducted in practice? The study lasts four years total. Some get the vaccine, and others get a placebo preparation (saline). Who gets what is random, and neither you nor the doctor who vaccinates you knows if you get the vaccine or not. The first year you get vaccinated three times (an injection with a little, thin needle). At the start of the study, you additionally get a gynecological examination, a blood test, a urine test, and will be asked about previous illnesses and various lifestyle habits (including sexual habits)”.
It is important to note that the Danish Medicines Agency and the Danish National Committee on Health Research Ethics were presented with contradictory information about the “placebo” in the FUTURE II trial, since they were given the study protocol which stated that the “placebo” contained the aluminum adjuvant, whereas the recruitment brochure and the informed consent form stated that the “placebo” contained saline [76]. Additionally, in the recruitment brochure Merck stated that FUTURE II was “NOT a side effect study” and that the HPV vaccine had no side effects apart from slight redness and soreness at the injection site (Fig. 3). However, the clinical study protocol specified that safety testing was one of the trial’s primary objectives. Therefore, in this instance also, the informed consent seemed to be compromised, as consenting participants were inaccurately informed that the HPV vaccine had already been proven safe [76].
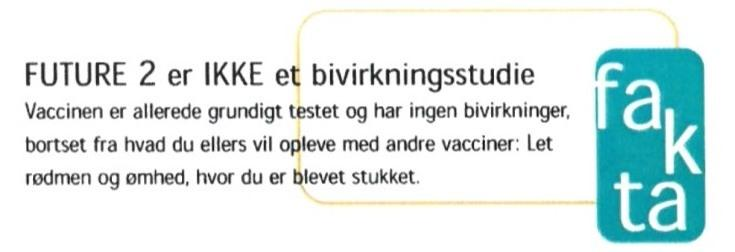
Excerpt from Merck’s recruitment brochure in Denmark for the FUTURE II Trial. Translation: “FUTURE 2 is NOT a side effect study. The vaccine is already thoroughly tested and has no side effects, apart from what you otherwise experience with other vaccines: Slight redness and soreness, where you got the shot”.
We have had extensive correspondence with physicians treating patients with suspected serious injuries after HPV vaccination, which included discussions of six FUTURE II trial participants. We have also interviewed some of these patients, and found that three of the six who were randomized to the “placebo” group and received three doses of AAHS were subsequently given three doses of Gardasil after the trial. Thus, these three participants unknowingly received six doses of AAHS. At least two of the participants received the recruitment brochure shown in Figs 2 and 3. Even though all six girls experienced similar incapacitating symptoms during the trial, the symptoms were dismissed by Merck’s clinical investigators as unrelated to the vaccine. Consistent with the report by Sørensen and Andersen [77], many also experienced stigmatizations by their family physicians who likewise dismissed their symptoms, and in some cases labeled them hypochondriacs.
The problem of complex conditions with neurological and dysautonomic components linked to Gardasil is not confined to Denmark. However, the novelty of the alleged HPV vaccine-induced syndrome led to difficulties in its classification and identification worldwide. Similar combinations of symptoms have led to different diagnoses depending on the country, thus diluting the potential safety signal [78]. The most common diagnoses include postural orthostatic tachycardia syndrome, chronic fatigue syndrome, complex regional pain syndrome, fibromyalgia and small fiber neuropathy [44,78–92]. In Japan, Human Papillomavirus Vaccination Associated Neuroimmunopathic Syndrome (HANS) has been suggested as a diagnostic term for the alleged HPV vaccine-induced syndrome [93]. Given that HPV vaccines contain a unique combination of potent aluminum adjuvant formulations, and highly immunogenic virus-like particles with many peptide sequences similar to those found in human antigens [94–97], it is not implausible that they might cause a variety of immuno-inflammatory manifestations that are difficult to diagnose.
According to the European Medicines Agency (EMA), “For both vaccines development, the use of Al(OH)3 (500 μg) rather than a true placebo (inactive control) was found acceptable by the CHMP [Committee for Medicinal Products for Human Use] in order to maintain the double blinding of the studies and consequently the validity of data ... The approach taken for both vaccines was found by the CHMP as a reliable way to establish the safety profile of the vaccines at the time of authorisation” [98] [emphasis added].
In this statement the EMA apparently admitted that an aluminum adjuvant is not a true placebo. Moreover, the Agency uncritically reproduced the rationale given by Merck to justify the use of a fake placebo in order to preserve blinding [52], elaborating that: “indeed an inactive placebo would have induced little local reactogenicity … As the control product contained the same amount of Al(OH)3 as the study vaccine, it induced some level of local reactions that would have not allowed subjects or study personnel to readily distinguish whether a HPV vaccine or control was administered” [99] [emphasis added]. Therefore, since the EMA admits that in comparison to a true inert placebo, an aluminum formulation causes greater reactogenicity (which, however, can be systemic, not just “local” [19,22]), it follows that trials using aluminum “placebos” are not—as the Agency claimed—“a reliable way to establish the safety profile of the vaccines” [98].
As noted by the Nordic Cochrane Centre, the outcome of primary interest in HPV vaccine trials are cervical cell changes, the assessment of which in routine practice is highly unlikely to be influenced by lack of blinding many years earlier when the children were vaccinated. Therefore, the alleged priority to maintain blinding, while at the same time losing the ability to investigate adequately vaccine-related harms, raises legitimate concerns about both the EMA’s and the vaccine manufacturers’ scientific and ethical standards [99,100]. Merck’s inconsistency in this context is apparent from the fact that, according to their own manual, “Giving an active treatment solely for placebo effect may be further considered unethical because it exposes patients to actual adverse effects” [101] [emphasis added].
We further note that contrary to the EMA’s statement cited above, “the control product” in Gardasil vaccine trials did not contain “the same amount of Al(OH)3 as the study vaccine”, because the adjuvant in Gardasil is AAHS, not Al(OH)3. The reason for confusing AAHS with aluminum hydroxide is revealed in the EMA’s statement regarding Merck’s AAHS-adjuvanted vaccine Procomvax, which the Agency authorized in 2004. According to the EMA, “the adjuvant AAHS [in Procomvax] is the same chemical compound as the one initially called ‘aluminium hydroxide’ used in trials leading to the initial authorization … The change in name reflects a change in nomenclature that occurred after the initial authorization of Procomvax” [55]. However, AAHS is not the same chemical compound as aluminum oxyhydroxide (inaccurately referred to as “aluminum hydroxide”). These two adjuvants have totally distinct physicochemical properties [12] and their nomenclatures are therefore not interchangeable. Merck’s own study confirms that fact [15].
Nonetheless, it is Merck that originally misidentified AAHS with aluminum oxyhydroxide, as during the marketing renewal of Procomvax in 2004 Merck proposed to the EMA “to update the excipient name of aluminium hydroxide to amorphous aluminium hydroxyphosphate sulphate”. This change was apparently requested by Merck, in order to “to align the nomenclature of the adjuvant in all relevant, authorised Merck vaccines at that time” [55]. The original Procomvax product information leaflet from 1999 lists “aluminium hydroxide” as the adjuvant component of Procomvax [102], while the 2004 version lists AAHS [103]. The 2010 product information leaflet of the same vaccine, which in the U.S. was approved in 1996 under the name Comvax, is more transparent, as it states that the antigenic component of the vaccine is “adsorbed onto an amorphous aluminum hydroxyphosphate sulfate adjuvant (previously referred to as aluminum hydroxide)” [emphasis added] [104]. Similarly, the 2010 product information leaflet of another AAHS-adjuvanted vaccine licensed before Gardasil states: “Each 0.5 mL dose of Liquid PedvaxHIB is … formulated to contain … 225 mcg of aluminum as amorphous aluminum hydroxyphosphate sulfate (previously referred to as aluminum hydroxide)…” [emphasis added] [105]. The 1991 publication of a clinical trial that led to the approval of Pedvax by the U.S. Food and Drug Administration (FDA) [106], accordingly states that the vaccine was reconstituted with an aluminum hydroxide diluent [107].
As in previous cases, the 2018 product information leaflet of Merck’s first licensed AAHS vaccine Recombivax states that all formulations of this vaccine, “contain approximately 0.5 mg of aluminum (provided as amorphous aluminum hydroxyphosphate sulfate, previously referred to as aluminum hydroxide)…” [emphasis added] [108]. Consistent with this, both the 1987 Summary of Basis for Approval of Recombivax [109], and the 1987 U.S. Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices (ACIP) update on hepatitis B prevention, list “aluminum hydroxide” as the adjuvant in Recombivax [110]; while current National Institute of Health (NIH)-supported web-resources reveal that AAHS was the adjuvant approved in 1986 as a component of Recombivax [14,111].
Notably, in a 2002 article entitled Aluminum salts in vaccines—US perspective, the adjuvant component of all Merck AAHS-containing vaccines licensed prior to Gardasil—Recombivax, Pedvax, Comvax and Vaqta—is listed as aluminum hydroxide [56]. The authors of this article were Norman W. Baylor, who at the time was the Director of the Office of Vaccines Research and Review (OVRR) in the Center for Biologics Evaluation and Research (CBER), and his two colleagues from the same Office.
It therefore appears that Merck’s proprietary adjuvant AAHS was first licensed under the erroneous term “aluminum hydroxide” in 1986, or 20 years prior to the licensure of Gardasil, as a component of a pediatric hepatitis B vaccine that is administered as a first of three dose series at birth [14,108,111]. The key question is why did Merck ever refer to AAHS as “aluminum hydroxide”? And how in such a case can Merck claim that the safety of AAHS is “well characterised”, when the first vaccines in which AAHS was used as an adjuvant were apparently described to both the U.S. and the European regulators as containing “aluminum hydroxide”?
If the safety of AAHS had been well characterized and Merck had solid data to that effect, then why did Merck not disclose the fact that they had used AAHS in vaccines that predated Gardasil, but rather incorrectly stated to the regulators that the adjuvant was “aluminum hydroxide”? A disclosure that Merck had used a novel proprietary adjuvant might have triggered a request by the regulators for additional safety studies. Indeed, according to the EMA, “toxicology studies of AAHS alone were not performed because this adjuvant has been used before in several other Merck vaccines and has an established safety profile” [55]. However, if Merck had only disclosed to the EMA in 2004 that AAHS was used in Procomvax, then the EMA licensed those prior vaccines under the mistaken assumption that the adjuvant component was aluminum hydroxide and not AAHS. The same applies to the U.S. FDA, for as late as 2002, as evidenced by the Baylor et al. article [56], CBER was apparently under the false impression that Merck’s vaccines that the Agency licensed—Recombivax, Pedvax, Comvax and Vaqta—were adjuvanted with aluminum hydroxide. Publicly available documents neither reveal when Merck disclosed to the FDA that the adjuvant in all these vaccines was actually AAHS, nor the FDA’s reaction to that disclosure.
We further note that the clinical safety assessment that led to the approval of these vaccines was very limited. For example, the Recombivax product information leaflet states that, “In three clinical studies, 434 doses of Recombivax, 5 mcg, were administered to 147 healthy infants and children … who were monitored for 5 days after each dose … In a group of studies, 3258 doses of Recombivax HB, 10 mcg, were administered to 1252 healthy adults who were monitored for 5 days after each dose” [112]. In a key pre-licensure clinical trial of Pedvax, in which 2056 infants received the second dose of the vaccine and 2105 received the placebo, safety monitoring for serious adverse events (AEs) was 30 days [107], which is still insufficient to detect autoimmune events with insidious onset that may take many months to manifest [69,113]. Interestingly, in this trial the placebo contained 2 mg lactose, which ensured that, “the appearance of the vaccine and placebo were identical”, so as to preserve blinding [107]. Therefore, Merck’s clinical trial of Pedvax that predated Gardasil trials clearly shows that there was never a need to use an aluminum adjuvant for blinding purposes.
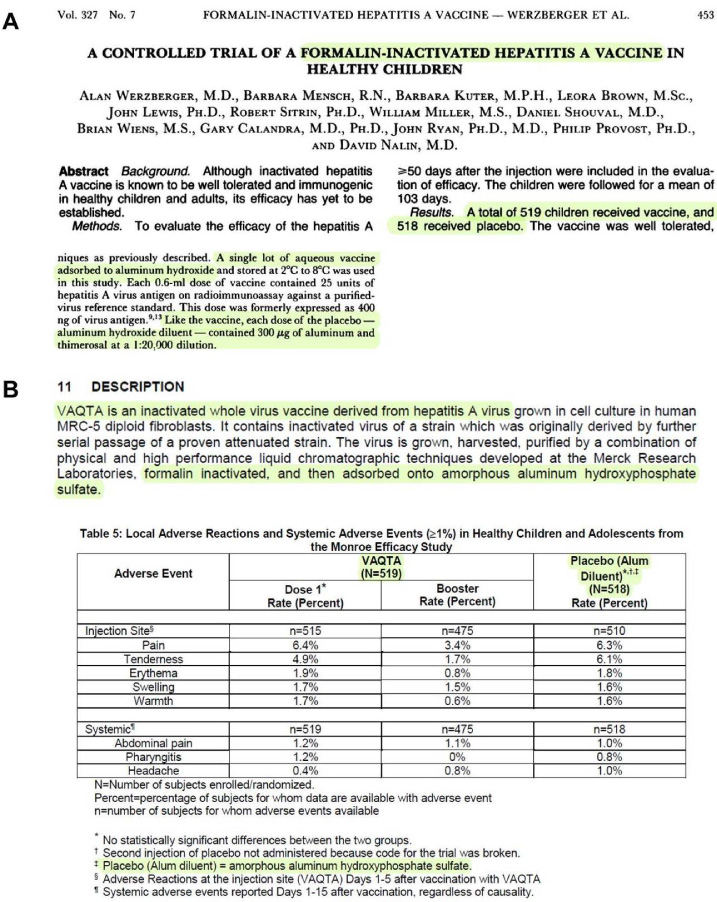
In a later key trial that led to the licensure of the hepatitis A vaccine Vaqta, Merck nonetheless used an aluminum “placebo”. In this trial, also known as the Monroe Efficacy Study, a total of 519 healthy children and adolescents from 2 to 16 years of age received the vaccine and 518 received the aluminum “placebo” diluent [114–116]. The 1992 publication of the Monroe Study states that, the vaccine was “adsorbed to aluminum hydroxide”, and, “like the vaccine, each dose of the placebo—aluminum hydroxide diluent—contained 300 μg of aluminum” [114]. However, page 7 of the product information leaflet reveals that the aluminum “placebo” diluent used in the Monroe Study was actually, “amorphous aluminum hydroxyphosphate sulfate” [115] (Fig. 4).
It thus appears that Gardasil trials were not the first clinical trials in which Merck used AAHS as a “placebo”. It also appears that Gardasil trials were not the first trials in which Merck was not transparent about the composition of the placebo, since the cited documentary trail shows that AAHS was at the time of these trials—i.e., “previously”—“referred to as aluminum hydroxide”. Moreover, it appears that both the U.S. and the European regulatory agencies were led by Merck to believe that the adjuvant used in several manufacturer’s vaccines that were licensed prior to Gardasil was not a novel aluminum compound, but rather, one of the conventional aluminum adjuvants that has been in use in human vaccines for many decades.
Nonetheless, even if there was good assurance from post-marketing surveillance that there are no significant safety issues with AAHS-adjuvanted vaccines that predated Gardasil (which the EMA argues is the case [55]), it would still be false to conclude that all AAHS-adjuvanted vaccine formulations are equally safe. In fact, according to the WHO guidelines on nonclinical evaluation of adjuvants and adjuvanted vaccines, individual antigens may vary in their immunogenic properties. For this reason, an adjuvant-mediated enhancement of the immune response to one vaccine antigen cannot be extrapolated to another antigen [117]. Vaccine manufacturers have likewise affirmed that, “it does not appear acceptable to extrapolate reactogenicity of an adjuvant in a given antigen/adjuvant formulation to another one”, given that discordant reactogenicity patterns have been observed for a specific adjuvant when it was combined with different antigens [69]. In spite of this, in reference to Merck’s AAHS, the EMA stated that since it was used in other Merck vaccines, which had been previously licensed by the Agency as having an acceptable efficacy and safety profile, there was no safety concern related to its use in the Gardasil vaccine [55].
Elsewhere the EMA appears to acknowledge that AAHS-induced immune response might be a risk for autoimmunity. In particular, in a 2015 report summarizing the results of Merck’s 9vHPV vaccine repeat-dose toxicity study in Sprague-Dawley rats, the EMA noted that, “the change observed in the draining lymph nodes was of similar frequency and severity in adjuvant-placebo versus high-dose vaccine groups, and was considered secondary to stimulation of the immune system by the adjuvant … Theoretically, lymphoid stimulatory effect … might cause/exacerbate autoimmune diseases, but such a risk can only be characterized in post-marketing setting in humans” [118] [emphasis added].
The pooled results from the Gardasil trials in the Gardasil package insert show that the occurrence of “new medical conditions” indicative of an autoimmune disorder among the vaccine and the AAHS recipients was the same (2.3%) [29]. However, instead of being interpreted as an assurance of Gardasil safety, these results, in view of the cited EMA’s admission, may have indicated a possible autoimmune risk signal attributable to the highly immunostimulatory adjuvant component of the vaccine.
In 2019 the EMA affirmed the safety of aluminum-adjuvanted vaccines by stating that, “the safety data gathered from the use of aluminum containing vaccines over six decades have shown that their safety profile is acceptable, with only local reactions as possible side effect linked to aluminum, which normally resolve in a short timeframe … For marketing authorization purposes, no new clinical safety studies are needed comparing aluminum alone versus inactive control” [55] [emphasis added]. Accordingly, in 2016 the EMA stated that, “The safety of aluminum adjuvant is considered well characterised … In addition non-clinical studies for HPV vaccines, such as conventional studies of safety pharmacology, acute and repeated dose toxicity … revealed no potential risk for humans” [98] [emphasis added]. Other than contradicting their former acknowledgment that there was a theoretical (i.e., potential) risk of AAHS causing or exacerbating autoimmune diseases [118], it is troubling that the EMA in this instance repeated almost verbatim Merck’s statement regarding the safety profile of the “aluminum adjuvant” as “well characterised” [52].
Another glaring inconsistency is that even though vaccine adjuvants are recognized and regarded as active components of a vaccine formulation from an immunological standpoint, for regulatory purposes they are regarded as inactive ingredients or excipients by both the U.S. FDA and the EMA [69,119]. Since such an inherently illogical position cannot be evidence-based, the reason for it has to be sought elsewhere. Admittedly, according to a 2013 report of a workshop on adjuvanted vaccines which gathered scientists from academia, regulatory agencies and the vaccine manufacturer industry, “if adjuvants were to be considered active ingredients from a regulatory perspective, clinical trials demonstrating that each active ingredient in the vaccine formulation contributes to the claimed effect would be required. Thus, this may significantly increase the size and cost of clinical trials. If considered excipients, such clinical studies would not need to be required” [69].
Therefore, it appears that the reason why regulators regard adjuvants as “inactive” ingredients is to spare the vaccine manufacturers the cost and logistical hurdles associated with the conduct of larger clinical studies. What makes this situation even more bizarre is the fact that the WHO acknowledges that, “since adjuvants have their own pharmacological properties, which might affect both the immunogenicity and the safety of vaccines, safety assessment is essential” [66]; and further, that, “short-term and long-term safety evaluation and prediction are important, as is the evaluation of the pharmacokinetics of the adjuvant alone” [66] [emphasis added]. Similarly, in section 4.3 of the 2004 guidelines on adjuvants in vaccines for human use the EMA affirmed that, “the adjuvant should be tested alone” [73] [emphasis added]. Finally, during the discussion on HPV vaccines at the U.S. CDC ACIP meeting in October 24–25, 2007, one ACIP member (Franklyn Judson) commented that, “experience over the years with hepatitis B and other protein-alum combinations indicates that the reactogenic part is predominantly the alum and that studies that use alum minus the active protein are not really placebos in terms of reactogenicity” [120]. Given these statements, it is difficult to understand why vaccine manufacturers are still permitted to use aluminum adjuvants as “placebos” in vaccine clinical trials.
In a 2020 systematic review with meta-analyses of clinical trial data from CSRs of Merck’s Gardasil and GlaxoSmithKline’s Cervarix HPV vaccines, Jørgensen et al. [121] found that at 4 years follow-up the HPV vaccines reduced HPV-related carcinoma in situ, external genital lesions, and HPV-related treatment procedures. However, the HPV vaccines increased serious nervous system disorders and general harms. Jørgensen et al. [121] judged all 24 CSRs they reviewed to be at high risk of bias for the following reasons: 99% of the study participants received an active comparator that included the adjuvant component of trial vaccines; Despite the fact that vaccine manufacturers regard aluminum adjuvants as safe, 52% of the participants were only included in the trials if they had never received the study adjuvants before; Two thirds of the participants were only included in the trials if they had no history of immunological or nervous system disorders, however, such conditions are not listed as warnings or contraindications in current HPV vaccine package inserts; Serious AEs were incompletely reported for as many as 72% of study participants (all 24 CSRs contained redactions–especially of harms–and lacked parts such as serious harm narratives and case report forms); Serious AEs in Merck’s clinical trials were only collected up to 14 days following each Gardasil injection; beyond that period serious AEs were only collected if they were judged by the study investigators to be related to the injection; Extended follow-up was not possible for 75% of “placebo” recipients, as they were offered HPV vaccination at trial completion.
The authors concluded that as the reviewed trials were primarily designed to assess benefits and were not adequately designed to assess harms, the extent to which the HPV vaccines’ benefits outweigh their harms is unclear [121].
To date, the most cited study allegedly demonstrating significant “real world” reduction of invasive cervical cancer in Gardasil recipients included 528,347 unvaccinated and 518,319 vaccinated Swedish girls and young women between 10 and 30 years of age [122]. During the study period, 538 women who had not received the Gardasil vaccine were subsequently diagnosed with cervical cancer compared to only 19 who had been vaccinated (adjusted incidence rate ratio (IRR) 0.37, 95% CI 0.21-0.57). The fully adjusted IRR for cervical cancer among women who were vaccinated before 17 years of age was 0.12 (95% CI 0.00-0.34). These results were hailed in the press as showing nearly 90% reduction in invasive cervical cancer incidence in girls vaccinated before 17 years of age [123]. Nonetheless, when the trumped reduction of the relative risk of invasive cervical cancer (96.4% for the total study population, Table 2) is translated to a reduction of absolute risk (0.098%, Table 2), the benefit of HPV vaccination becomes practically negligible in terms of public health impact. The absolute risk reduction figures stratified per birth cohort are even less impressive, ranging from negative 0.008% for the older 1980-1984 cohort, to 0.027% for the younger 1990-1994 birth cohort (Table 2). Of note, the rate of serious AEs in the largest pre-licensure clinical trial of Gardasil—the FUTURE II trial—was 0.7%, of which less than 0.1% were judged by Merck-sponsored study investigators as vaccine related [9]. Bearing in mind that the rate of serious AEs will be much higher in real world setting due to vaccination of subjects with pre-existing medical conditions who were excluded from Gardasil clinical trials, it appears that the benefit to risk ratio of Gardasil vaccination is not as overwhelmingly in favor of vaccination in developed countries as claimed by the health authorities [124]. This is because in the developed world, where cervical screening practices are well established, the incidence of cervical cancer is very low (4.9-6.9/100,000 [6]). Moreover, regular cervical screening must be maintained given that the currently licensed HPV vaccines do not cover all oncogenic HPV strains.
Relative (RRR) and absolute risk reduction (ARR) of invasive cervical cancer in relation to HPV vaccination by birth cohort
Relative (RRR) and absolute risk reduction (ARR) of invasive cervical cancer in relation to HPV vaccination by birth cohort
Birth cohort, vaccination status, number of subjects, number of invasive cancer cases and crude incidence rate of cervical cancer per 100,000 person-year were sourced from Lei et al. manuscript and supplementary appendix Table S4 [122]. RRR and ARR could not be calculated for the 1975–1979, 1995–1999 and 2000–2007 birth cohorts because the number of invasive cancers was 0 for the vaccinated (all three birth cohorts), and for the unvaccinated 2000–2007 birth cohort. *RRR = (CER - EER)/CER. CER: risk of event in control group; EER: risk of event in experimental group. †ARR = (CER - EER).
Due to a Protective Order in the case, we are prevented from discussing the contents of documents produced by Merck, including data from Merck’s clinical trials which are proprietary information.
Conclusions
The informed consent forms for Merck’s Gardasil vaccine trials appear to be seriously misleading, as a highly reactogenic adjuvant with a questionable safety record was described as an inactive placebo. Thus, in our opinion, there was a violation of the scientific principle in the failure to use a true placebo, and of ethics in the failure to disclose the true composition of the “placebo”. Additionally, in contradiction to the information in the FUTURE II Gardasil clinical study protocol, Merck informed potential participants that FUTURE II was not a safety trial, but that the vaccine had already been thoroughly tested and proven safe. Further, in our view Merck was not transparent about the identity of AAHS, as the first vaccines in which AAHS was used as an adjuvant were described in journal publications and in documents apparently submitted to the U.S. and the European regulators as containing “aluminum hydroxide”. In light of this fact, any claim made by Merck and the regulators that the safety of AAHS is “well characterised” lacks support. Current animal and human research indicates that aluminum adjuvants may be associated with persisting and disabling systemic symptoms and neurological impairments [30–32,34–37,40–42,44–46,58,63]. It is therefore unclear why the drug regulatory agencies continue to endorse the use of aluminum adjuvant “placebos” in vaccine clinical trials. This practice hinders proper assessment of vaccine harms, and appears to violate medical ethics guidelines as it exposes research subjects to potential risks only without any benefit [1].
Footnotes
Acknowledgements
The authors wish to thank Ronald Goldman, Esq., for legal review of the manuscript; Anna Pedersen for the English translations of Danish documents; Sesilje B. Petersen for providing Merck recruitment and clinical trial documents from the FUTURE II trial; Christopher Exley, PhD, Lluis Lujan, PhD, Guillemette Crépeaux, PhD, Rokuro Hama, MD, and Kim Mack Rosenberg, Esq., for suggested improvements in presentation of factual information, and four anonymous reviewers for their critical evaluations of the manuscript.
Conflict of interest
LT and LBM are remunerated as research consultants for the Los Angeles law firm Wisner Baum in an ongoing Gardasil litigation. Robert F. Kennedy, Jr., founder and chairman-on-leave of Children’s Health Defense (CHD) is a co-counsel in this litigation. LT is a paid research consultant for CHD and has previously served as an expert witness in court cases involving adverse reactions to vaccines, including HPV vaccine. The views expressed herein are those of the authors alone and not those of any other person, firm or entity. CHD and Wisner Baum did not have any input in this article, apart from Kim Mack Rosenberg, Esq. (private practice attorney and CHD Acting Outside General Counsel), as listed in the Acknowledgments.
Funding
No specific funding supported the preparation of this manuscript.