
Abstract
BACKGROUND:
Medication reconciliation is advocated to ensure the continuity, safety, and effective use of medicines across transitions of care.
CASE REPORT:
In this report, we describe the case of a 90-year-old female with previous diagnoses of atrial fibrillation and cutaneous metastatic breast cancer presenting with bilateral ulcerative lesions on the chest wall. The patient was diagnosed with Deep Vein Thrombosis at the Emergency Department and started on rivaroxaban, although the patient was already taking edoxaban. This therapeutic duplication was noticed only one week later, even though she was already experiencing significant bleeding managed through a prescribing cascade. Despite the technical error (action-based), it is possible to identify several weaknesses in the organisation’s structure, which provided a trajectory of accident opportunity.
CONCLUSION:
Anticoagulants are ranked first for the highest priority to receive a medication reconciliation. To achieve an optimal level of medication reconciliation, we ought to recognise and correct latent failures.
Keywords
Background
Medication errors following discharge, such as unintentional medication discrepancies, are present in around 50% (interquartile range 33–60.5) of adult and older patients [1]. Numerous organisations worldwide advocate for medication reconciliation to ensure the continuity, safety and effective use of medicines [2–4]. This is all the more imperative for older adults with multimorbidity and polypharmacy [5].
Several factors may hinder the implementation of medication reconciliation interventions. Specifically, there is a lack of agreement about the scope and specific tasks to be included in these interventions [6]. In addition, context-dependent variables accrue to difficulties in the implementation process [7]. Nonetheless, ordering providers are ultimately responsible for verifying the accuracy of medication reconciliation processes to meet safe medication orders [7].
Some medicines, such as anticoagulants, carry a distinct risk of adverse drug reactions and medication errors which is increased through transitions of care [8] and are therefore ranked first for the highest priority to receive a medication reconciliation [6].
Bleeding is the most relevant adverse drug reaction when using oral anticoagulants [9,10]. The first step in approaching such an event is to assess and identify the bleed severity. When the bleed is non-major (non-critical site, hemodynamic stability, no significant clinical bleeding) [11], non-pharmacological measures are usually sufficient [12]. Specialised testing is not widely available and specific reversal agents are usually reserved for major bleedings [11].
As for medication errors under anticoagulant therapy, we can refer to recent literature concerning direct oral anticoagulants (DOAC), a class increasingly used for treating and preventing thromboembolic diseases. Common prescribing errors include dosing errors, missed doses, inappropriate prescribing and duplicate therapy from different DOAC [8].
Here, we report the case of a therapeutic duplication of DOAC that arose after a care transition following an emergency department (ED) admission with subsequent harm to the patient. We complement the case summary with a medication error analysis, considering an individual and systemic approach.
This case occurred within the Portuguese National Health Service (NHS), tax-funded and universal, predominantly providing primary care and acute general and specialised hospital care and ensuring medication coinsurance [13,14]. Community pharmacies in Portugal are private providers responsible for dispensing pharmaceutical products requiring a prescription. Since 2012 there has been a mandatory electronic prescription system, although a complete data integration across the care continuum has yet to be achieved.
We hope this case report illustrates the complexity of clinical care and highlights that implementing safe medication practices, such as medication reconciliation interventions, is a pressing need across the patient care continuum and, ultimately, dependent on many forces besides the individual ordering prescriber.
Case summary
A 90-year-old female was referred to the Family Physician (FP) by the Family Nurse because of pain, swelling and redness in the left calf. The patient, who lived with her daughter for partial care, had a medical history of atrial fibrillation and cutaneous metastatic breast cancer presenting with bilateral ulcerative lesions on the chest wall. The FP suggested an ED visit to exclude Deep Vein Thrombosis (DVT).
In the ED, the patient was unaccompanied because of COVID-19 restrictions. The presence of a thrombus in the left popliteal was confirmed by ultrasonography, despite a slight increase in D-Dimers (381.0 ng/m; normal range 45.0–250.0 ng/mL).
Following the DVT diagnosis, the patient was discharged home on rivaroxaban (15 mg bid for 21 days, followed by rivaroxaban 20 mg id).
Six days post-discharge, the primary caregiver requested a refill of edoxaban 60 mg and delivered the ED discharge letter to the primary care unit. The ED discharge letter mentioned that the patient was newly medicated with rivaroxaban and that there were “no current medications”.
The FP contacted the caregiver to clarify the situation. When questioned about the medications, the primary caregiver reported that the patient had been taking rivaroxaban following the recent DVT diagnosis and edoxaban, which had been previously prescribed for atrial fibrillation. The caregiver also added that the patient had recently started oral aminocaproic acid as prescribed by the oncologist because of worsening blood loss from the ulcerated lesions on the chest wall. After collecting thorough medication history, the FP advised the caregiver to suspend rivaroxaban and discuss the maintenance of the oral aminocaproic acid with the oncologist. The caregiver was also empowered to speak about the medications to healthcare providers in subsequent health visits.
Home visits by the nursing team and the FP were maintained, and haemostasis was achieved approximately one week later.
Table 1 provides an overview of the relevant case report timelines. The patient died seven months later due to the natural course of her oncological disease.
Case report timelines
Case report timelines
In the present case, the therapeutic duplication of DOAC ensued when the ED physician prescribed rivaroxaban, despite the patient being under edoxaban treatment as prescribed by the FP. The consequent worsening blood loss from the active chest wall ulcers was erroneously attributed to the underlying disease by the oncologist and managed through the prescription of aminocaproic acid and wound care, ensuing a therapeutic cascade. The medication error became evident only one week later, when the caregiver sent a prescription renewal request to the FP.
The Portuguese National Health Service (Centre Administrative Health Region) provided both levels of care (Hospital and Primary care) involved in this incident. All prescriptions were made via the national electronic prescription system.
Obtaining the best possible medication history is the first step in medication reconciliation. In this case, there was evidence of a tentative medication history collection by the ED physician, as “no current medication” was stated in the discharge summary. An inaccurate medication history translated into a medication reconciliation failure with a subsequent medication error at the prescribing level [15,16]. From a human standpoint, if one assumes the ED physician started the medication history collection but failed, this error can be further classified as technical, a subset of action-based errors (slips) [15,16]. Nevertheless, it is arguable that a true medication reconciliation took place as there is no clear evidence that a systematic process was in place to create an accurate list of the patient’s medicines [6].
The complexity of clinical care and healthcare systems [17] calls for a systems approach to this incident. As proposed by James Reason (Theory of Active and Latent Failures, also known as the “Swiss Cheese Model”), latent failures are weaknesses in an organisation’s structure [18]. Latent failures usually only become apparent when they occur in proper sequence and combine with active failures of individuals (unsafe acts).
The active failure was the incorrect prescription of rivaroxaban on top of edoxaban. Information on edoxaban compliance was mandatory if the correct medication list had been obtained. If the patient was compliant, an anticoagulation switch might have been considered [19].
In addition to the active failure, several latent failures provided a trajectory of accident opportunity [18] (Fig. 1).
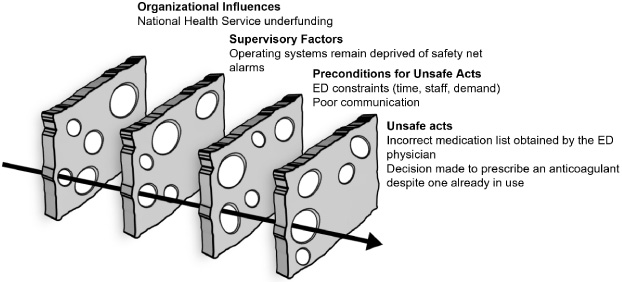
Patient harm (haemorrhage following a medication error) represented through the “Swiss cheese model”.
Considering “organisation influences”, significant steps have already been taken to promote communication and learning from medication errors. For instance, since 2012, European legislation has required information on medication errors to be collected and reported through national pharmacovigilance systems for evaluation and assessment [20]. However, there is little room to consider medication safety practices when teams are unstaffed and the healthcare system is chronically underfunded [21].
Introducing alerts in electronic prescribing systems could be helpful at the “supervisory factors” level. Encouraging evidence comes from a recently published study evaluating the impact of a duplicate “Anticoagulant Alert” on the prevention of prescription of low molecular weight heparins to patients already prescribed DOAC at a 950-bed acute teaching hospital in the UK [22]. The electronic alert prevented duplicate anticoagulant prescribing for 46 cases (representing 41% of the 111 triggered alerts), reducing the risk of patient harm. In addition, most overridden cases were appropriate and justified [22]. Neither the Hospital Centre, the Primary Care Unit, nor the national electronic prescription system have any safety net alarms to prevent medication duplication.
At the “preconditions for unsafe acts” level, the demand for urgent solutions for complex problems in the ED can exacerbate communication issues, both in the doctor–patient relationship and between professionals. As such, policies and procedures could be enforced to mitigate communication problems. With the support of the North of England Strategic Clinical Network (NESCN), Thomas and Smyth developed a standard alert card for patients on direct-acting anticoagulants [23]. The objective was to provide key safety information for patients and healthcare professionals across primary and secondary care [23]. Besides facilitating patient access to clear and consistent written instructions about these medications, this tool might also contribute to patient capacitation, increasing health literacy and awareness for future shared decision-making scenarios. This patient navigated alone through the ED and parted from the caregiver because of COVID-19 restrictions. An alert card could have served as a passport for a safer medical encounter.
In Portugal, national efforts have been put in place to prevent unsafe acts. Such efforts include, for instance, the publication of a national guideline for medication reconciliation across all levels of care [4]. Strategies to reinforce the organisational influences, supervisory factors, and preconditions for unsafe acts remain unfulfilled despite recent changes to the National Plan on Patient Safety [24]. This case report and incident analysis highlight the potential benefit of including transition of care as one of the targets for a national medication safety system.
To the best of our knowledge, this is the first published case reporting a medication error resulting from a medication reconciliation failure, alongside an incident analysis. With this case report, we conclude on the importance of moving beyond finding the individual culprit and focusing on the multiple underlying system failures that set the stage for active medication reconciliation failures, ultimately resulting in patient harm. While the evidence is lacking on the best premises to guide the implementation of medication reconciliation interventions, a systems approach might help to recognise different weaknesses or strengths in the care continuum, moving beyond the quick fixes of active failures.
In sum, to achieve an optimal level of medication reconciliation, we ought to recognise and correct latent failures. The implications for patient safety are of paramount importance.
Footnotes
Acknowledgements
None to report.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethics statement
The patient’s next of kin provided written consent for permission to publish this case.
Funding
There was no funding for this case report.