
Abstract
People with Parkinson’s disease (PD) experience a range of progressive motor and non-motor symptoms, that negatively affect their daily functioning, social participation and quality of life. Allied health therapies have emerged as an effective treatment approach—complementary to pharmacological and neurosurgical treatments—which reduces the impact of PD in daily life. In this article, we propose criteria for what constitutes specialized allied health care for PD, and we review allied health research in PD in terms of meeting these criteria and its outcomes for monodisciplinary approaches as well as multi- or interdisciplinary allied health interventions. We focus on the three most studied allied health disciplines in PD: physical therapy, occupational therapy and speech-language therapy. Overall, the available evidence underscores the importance and potential benefits of specialized allied health care for people with PD. Our proposed criteria and recommendations for future research might help in further delineating specialized allied health care.
Keywords
INTRODUCTION
People with Parkinson’s disease (PD) experience progressive motor and non-motor symptoms, that negatively impact on their daily activities, social participation and quality of life.1,2, 1,2 Within multidisciplinary care, pharmacological and neurosurgical treatments are well established and effective in alleviating symptoms such as bradykinesia, rigidity and tremor. 3 However, these interventions have limited effect on other symptoms, such as impaired balance, cognition and oral motor functions. These symptoms negatively impact daily life functioning and can put patients at increased risk for potentially serious complications, such as hip fractures or aspiration pneumonia. 4 Over the past decades, allied health interventions have emerged as an effective complementary treatment approach in the multidisciplinary care of people with PD to reduce the impact of PD on daily functioning and to prevent medical complications. While there is no universally accepted definition of allied health care, three allied health disciplines are commonly recognized and most frequently involved in the context of PD care. These are physical therapy, occupational therapy, and speech-language therapy. More recently, the role of other allied health professionals such as dieticians psychologists, social workers and sexologists is emerging.5,6, 5,6
Because of the complexity of PD, there is a growing awareness that the care for people with PD should be tailored to the specific needs of affected individuals. In this article, we describe what constitutes “specialized allied health care” for PD. We subsequently review studies of specialized physical therapy, occupational therapy and speech-language therapy, and evaluate the extent to which these studies meet the proposed criteria for specialized care. Our work includes an unstructured review of the literature on monodisciplinary allied health approaches as well as a structured review of the literature on multi- or interdisciplinary allied health interventions. Finally, we outline remaining knowledge gaps in further defining and supporting specialized allied health care for PD.
WHAT CONSTITUTES SPECIALIZED ALLIED HEALTH CARE IN PARKINSON’S DISEASE
Specialized care generally refers to high-quality care that is designed and tailored for a specific disease or patient population and delivered by professionals with a special interest and competence in that area. 7 As far as we are aware, there is no consensus statement on specific criteria to distinguish “specialized” versus “generic” allied health care in PD. Here, we propose a set of criteria to operationalize “specialized allied health care” in PD (Table 1).
Proposed criteria of specialized allied health care in Parkinson’s disease
First, the allied health professionals (AHPs) providing specialized care must have expertise in PD to understand the specific clinical manifestations of PD, the (potential) working mechanism of interventions, and how to tailor and deliver these interventions. They need to integrate PD guidelines into their clinical practice, and be aware of what other disciplines contribute to care.8,9, 8,9 They need to be able to adapt the intervention if the diagnosis turns out to be atypical parkinsonism. There are different initiatives and opportunities to gain PD- specific expertise. PD-specific training courses and resources for AHPs are provided by specialist health professional organizations, such as the International Parkinson and Movement Disorder Society, or by PD associations, such as Parkinson’s UK. Specialized treatment approaches are offered through courses that include certification, such as SPEAK OUT, 10 LSVT LOUD® 11 for speech-language therapists and LSVT BIG® 12 for physical and occupational therapists. A step further is the provision of PD-specific training and certification as part of an infrastructure for specialized multidisciplinary network care, such as the ParkinsonNet model. 13 Within ParkinsonNet, an initial criterion for expertise is the completion of a dedicated training program to understand the causes, clinical presentation, and impact of PD symptoms, as well as the specific treatment options for each problem or need, according to the latest scientific evidence. To maintain the specialist designation, AHPs are required to maintain a substantial caseload of people with PD, participate in regular training, and attend multidisciplinary meetings where they both learn and meet with ParkinsonNet professionals in the local area. The rationale is that professionals who meet these criteria will develop expertise and provide better care. However, there is no international consensus on the minimum curriculum or caseload requirements for an AHP with specific expertise in PD.
Second, specialized allied health care must be personalized to the needs and context of the individual. Personalized care is important in allied health care for all chronic diseases, but it is essential for people with PD because there is considerable inter-individual variation in the motor and non-motor symptoms. There is also a great deal of variation in the presentation of symptoms within an individual, even on a day-to-day basis. In addition, the impact of these symptoms on daily life varies from person to person, depending on the personal context and values of the person with PD. 3 Recently, much attention has been given to the need to tailor care to the needs of the individual and to avoid a “one size fits all” approach.14,15, 14,15 However, tailoring allied health care for PD is a complex due to the many disease and personal factors to consider. Furthermore, intervention research often excludes subgroups with cognitive problems or advanced disease. Consequently, there is still a knowledge gap in how to personalize allied health care for PD in the most effective way.
Third, specialized care must take into account the specific characteristics and complexity of PD in assessment and treatment. Motor symptoms such as bradykinesia, hypokinesia, and freezing require a PD-specific approach that promotes goal-directed movement, amplitude, and explicit feedback.8,16, 8,16 The presence and impact of a potential wide range of non-motor symptoms, such as cognitive deficits, fatigue, orthostatic hypotension, urinary dysfunction, apathy, depression and anxiety must be considered or targeted in the interventions.8,17,18, 8,17,18 Another specific feature in patients with advanced disease is fluctuation in motor and non-motor symptoms in response to levodopa. 19 This needs to be considered in both the content and planning of assessment and interventions.
Fourth, it is essential to provide specialized in an appropriate treatment context. This is important because symptom presentation may be context-specific (e.g., freezing at a narrow basement door) and the transfer of newly acquired skills and strategies to a new context is generally impaired in PD.20,21, 20,21 Consequently, if the goal is to (re)learn skills or to use new compensatory strategies, training should be task-oriented and (also) take place in the person’s real-life context. In the event that therapy sessions cannot be conducted in the home or community setting, then the AHP must fully consider the activity and environmental context (e.g., by requesting video/photo’s) and facilitate unsupervised practice at home.
A fifth criterion for specialized care is the provision of an appropriate dose of treatment to optimize physiological adaptation or to acquire and consolidate new skills and strategies. For exercise, the dose depends on the type of exercise and the functions being addressed. Recommendations for the appropriate dose of exercise are available. 22 Consolidation of (motor) learning in people with PD requires greater intensity and repetition than in the healthy population.20,22, 20,22 Successful PD-specific programs such as LSVT LOUD and LSVT BIG are based on high-intensity treatment (4 weeks; 4 times per week) to achieve improvement in daily functioning.12,23, 12,23 An important gap exists in the evidence base regarding the optimal intensity, frequency, and duration of treatment for individuals with PD who are unable to adhere to such intensive programs.
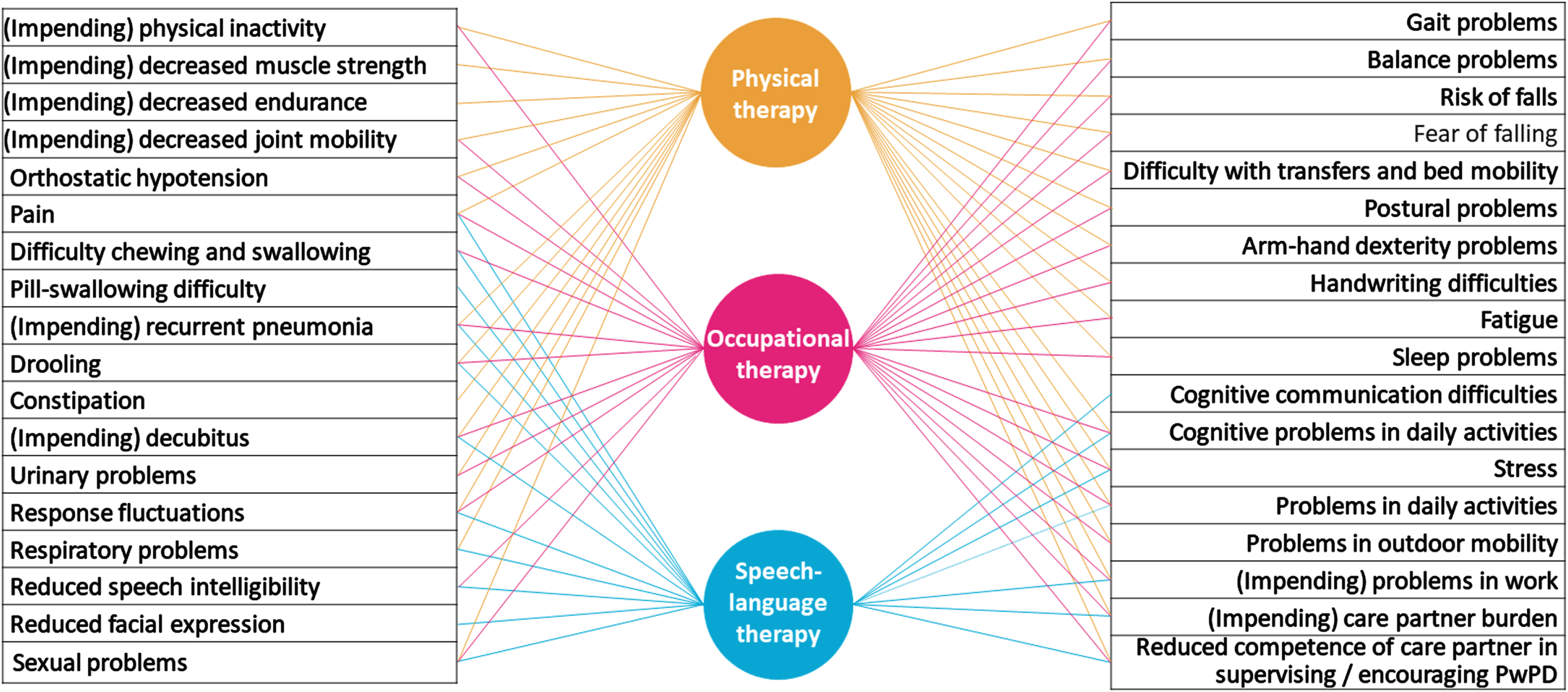
A final criterion is that specialized allied health care for PD is delivered within an appropriate multidisciplinary or interdisciplinary team. Individuals with PD often have multiple problems that require the input of different healthcare disciplines, both within and beyond the scope of allied health care. Indeed, some symptoms or areas of activity or participation may necessitate the simultaneous treatment of several AHPs (Fig. 1). In the case of interdisciplinary overlap, the contribution of each AHP will often be different, depending on the discipline-specific perspective and the availability of appropriate interventions.24,25, 24,25 An example is the management of a person with PD who has difficulty eating due to dysphagia and postural problems. For a speech-language therapist, upright posture is a prerequisite for efficient eating and swallowing. A physical therapist may provide an exercise program to train the muscles involved in postural control, or sensory cues or visual feedback strategies to improve sitting posture. Concurrently, an occupational therapist may integrate the utilization of these strategies into home mealtime activities, provide advice on meal timing, adjust positioning at the table, or provide additional external postural support while sitting. This example - albeit one of the many - illustrates how interdisciplinary care can have synergistic effects. In fact, there is currently widespread interest in developing training and guidelines for interdisciplinary care in PD with the aim of integrating knowledge and methods from different disciplines. In the Netherlands, an online, integrated allied health guideline with embedded decision support has recently been developed to facilitate interdisciplinary care. 26
EVIDENCE FOR MONODISCIPLINARY SPECIALIZED ALLIED HEALTH CARE
Based on an unstructured review, the following sections summarize the current state of evidence for physical therapy, occupational therapy, and speech-language therapy in relation to the criteria for specialized allied health care.
Physical therapy
Physical therapy aims to improve movement-related limitations in functions, activities and participation. Core areas of physical therapy include physical capacity, transfers, manual activities, balance, gait and posture. The main intervention modalities include tailored education, exercise, skills practice and strategy training.9,24,27, 9,24,27
There is a large and growing body of evidence on the effects of physical therapy. A multitude of studies have been conducted, and numerous systematic reviews and meta-analyses have been published on this subject. The majority of this research has focused on physical exercise interventions. While physical exercise is a part of physical therapy, and can be delivered according to the above mentioned criteria for specialization, it is often unclear in publications whether the exercise was delivered by specialized professionals, in a specific context, or as part of an individualized treatment plan. Moreover, specialized physical therapy includes not only exercise, but also focuses on specific motor- and non-motor symptoms of the disease. Examples of PD-specific treatment modalities include cueing, dual-task training, amplitude-oriented training and manual dexterity training.9,24,27, 9,24,27 Cueing has been shown to have positive effects on gait initiation and the spatiotemporal parameters of gait (i.e. step- and stride length). 28 However, the optimal cue (auditory, visual, tactile) and behavioral strategies to employ remain unclear. Dual-task training, which combines (physical) skill practice with a cognitive element, has been shown to have positive effects on multiple outcomes (e.g., spatiotemporal parameters, balance, and functional mobility) and does not seem to have serious adverse effects. 29 The evidence regarding amplitude-oriented training (i.e., LSVT-BIG) remains inconclusive. 30 Many physical therapy studies have combined different treatment modalities, such as exercise combined with strategy training. This is a common clinical practice, where the exact combination of physical therapy modalities depends on the specific symptoms, problems and goals of each individual patient. A comprehensive meta-analysis showed a positive effect of a combination of physical therapy treatment modalities on motor symptoms, fear of falling, and gait freezing, based on the pooled effects of 45 studies. 31 As with other studies in the field, the extent to which the professionals involved were specialized remains unclear, and conclusions about the effectiveness of specialization cannot be drawn based on the available evidence from prospective trials. However, a detailed analysis of registry data revealed that specialized physical therapy given via ParkinsonNet is more effective (i.e., fewer complications) and cost-effective than regular physical therapy. 32
Occupational therapy
Occupational therapy aims to maximize people’s participation in meaningful activities and roles at home, work and in the community.24,33,34, 24,33,34 In PD, occupational therapists may specifically address activity limitations and participation restrictions due to changes in functional mobility, manual dexterity, functional cognition, and fatigue. The main intervention modalities include a combination of tailored education, skills practice, compensatory strategy training, adaptation of tasks and daily activity patterns, and adaptation of the environment.9,24,34, 9,24,34 Given the specific motor symptoms associated with PD, it is essential that skills practice and strategy training to address functional mobility and manual dexterity must be PD-specific. While occupational therapy interventions to address functional cognition and fatigue are not unique to PD, it is important for treating therapists to be aware of all the factors that affect cognition and fatigue in people with PD in order to tailor education and strategies appropriately.
Occupational therapists have a distinct focus and approach, yet occupational therapy in PD is seldom delivered in isolation; it is naturally integrated into multidisciplinary programs. Some recent systematic reviews have focused on interventions that fall ‘within the scope of’ occupational therapy, namely those designed to improve activities and participation.35–37 However, other AHPs also aim to improve activity performance and participation. 38 Consequently, these reviews also include interventions delivered by other professionals, which precludes a clear insight into the unique contribution of occupational therapy. Recent systematic reviews that included studies in which the intervention was (mainly) delivered by occupational therapists, can only be cautious in their conclusions due to the limited number of studies included, the heterogeneity of interventions, outcomes and study design.39,40, 39,40 Three randomized controlled trials specifically examined occupational therapy as a single intervention. These are a trial of individualized, goal-directed home-based occupational therapy delivered within the context of ParkinsonNet, 41 a dexterity-focused home-based exercise program, 42 and a multicomponent PD-specific occupational therapy program focused on motor limitations in activities of daily living. 43 The interventions in the trials were PD-specific and delivered by AHPs experienced in PD. The dose was only appropriate if participants did the home practice. The interventions were either home-based41,42, 41,42 or focused on using what was learned at home. 43 Overall, the results suggest an improvement in (perceived) activity performance41,43, 41,43 and short-term improvements in dexterity-related ADL. 42 The results showed no effect on patients’ quality of life. However, the trial on individualized home-based occupational therapy, showed improvement for caregivers’ quality of life. 41 The study also showed that the intervention had no effect on total costs over six months, but there were significant savings in institutional care in the intervention group. 44
A recent study assessed whether adding a task-oriented LSVT-BIG® program to general occupational therapy has beneficial effects. 45 From the intervention description it is unclear what constituted “general occupational therapy”. However, the results suggest that adding PD-specific and task-oriented training may improve outcomes. More occupational therapy feasibility/ pilot studies have recently been done to address problems that affect daily life and participation in PD, such as functional cognition,46,47, 46,47 fatigue, 48 anxiety, 49 and work. 50 These studies advance the scientific evidence on occupational therapy in PD.
Speech-language therapy
Speech-language therapists focus on three oral motor domains that can deteriorate in PD: speech intelligibility (dysarthria), safe and efficient nutrition intake (dysphagia) and saliva control (drooling).9,51, 9,51 They also provide treatment options to compensate for communication disorders caused by cognitive decline, in particular word finding difficulties and bradyphrenia.52,53, 52,53 Speech-language therapists offer different types of treatment, including tailored education, exercise, skill training, and compensatory strategies; manuals and guidelines available for this.23,51, 23,51
There is a growing body of evidence supporting the benefits of specialized speech-language therapy for PD. The first studies of speech-language therapy evaluated the Lee Silverman Voice Treatment (LSVT LOUD) three decades ago. 54 A recent meta-analysis confirms the efficacy of this approach in improving voice loudness and functional communication. 11 However, the success of such programs depends on their high intensity over a brief period (three to four times per week for four weeks), which is reflected in the inclusion of participants with mild to moderate PD. 11 Meanwhile, large randomized controlled trials of personalized approaches are underway, including people with severe PD. 55 Importantly, tele-rehabilitation has been shown to be non-inferior to face-to-face treatment sessions, facilitating the delivery of intensive speech-language therapy in the home. 56 While speech-language therapy is generally delivered individually, PD-specific group treatments seem promising. A well-moderated weekly or monthly intensive therapeutic singing group, known as ParkinSong, requires a high level of respiratory and vocal effort and showed improved voice-related quality of life and well-being after 12 months. 57 However, replication of this approach is necessary, as is comparison with intensive individual treatment to better interpret the individual benefit.
Moreover, the treatment of cognitive communication disorders, which further affect communicative efficacy, has attracted scientific interest. Studies suggest that approaches such as Communication Partner Training (CPT) may also be valuable for caregivers of people with PD,58–60 but clear results and the evaluation of specific approaches for PD are awaited.
Treatment of dysphagia in PD depends on the timely compensation to prevent aspiration or to facilitate swallowing. 51 Specific exercises to practice swallowing skills or indirect exercises such as expiratory muscle strength training (EMST) may also be beneficial. 61 Expiratory strength training may also improve coughing as a protective response to aspiration of liquids or food, but intensive skills training to improve cough efficiency seems to be more effective. 62 Although the content of the treatments is not reported (e.g., exercise, compensations, or alterations of food consistencies), there is now convincing evidence that speech-language therapy in the community within the context of ParkinsonNet, reduces the rate of pneumonia in PD. 63 Behavioral treatment of drooling in PD is primarily based on education and identifying the right cues to improve swallowing frequency. Given that saliva is swallowed throughout the day, wearable devices are being investigated, 64 but results are pending.
The costs of specialized speech-language therapy in comparison to usual care have not been well studied. An exploratory economic evaluation conducted alongside the PD COMM pilot trial compared the costs and outcomes of LSVT LOUD, standard speech-language therapy, and no treatment. There were no differences in outcomes at 12 months, but the full study is awaited for a more definitive assessment of the cost-effectiveness of speech-language therapy for people with voice and communication problems due to PD. 65
EVIDENCE FOR MULTI-OR INTERDISCIPLINARY SPECIALIZED ALLIED HEALTH INTERVENTIONS
In order to review multi- or interdisciplinary allied health programs for people with PD, we conducted a structured literature search on randomized controlled trials that evaluated the effectiveness of the combination of two or more allied health disciplines compared with a control group that did not receive care from multiple allied health disciplines. The level of specialization was evaluated according to the proposed criteria (Table 1) and evidence for effectiveness. The exact search terms and evaluation criteria are presented in the Supplementary Material A and B.
The literature search yielded only nine studies.66–74 The interventions, outcome measures, and results are summarized in Table 2. All trials involved physical therapy; four trials involved all three allied health disciplines.69–72 Most trials included participants with mild to moderate PD, whereas two trials included “de novo” PD.68,69, 68,69 The number of participants per trial ranged from 36 to 762.
Trials on effectiveness of multi- or interdisciplinary specialized allied health care in Parkinson’s disease
AHPs, Allied health professionals; BBS, Berg Balance Scale; CG, control group; EQ-5D, EuroQol 5D; FIM, Functional Independence Measure; H& Y, Hoehn and Yahr; IG, intervention group; IG1, intervention group one; IG2, intervention group two; NEADL, NHPT, Nine hole peg test; Nottingham Extended Activities of Daily Living Index; OT, occupational therapy; PD, Parkinson’s disease; PDDS, Parkinson’s Disease Disability Scale; PDQ-39, Parkinson’s Disease Questionnaire-39; PT, physical therapy; SF-36, 36-Item Short Form Health Survey; 6MWT, six-minute walking test; ST, speech- language therapy; TUG, Timed Up-and-Go Test; UPDRS, Unified Parkinson’s Disease Rating Scale.
Three authors (BRM, IHWM, JGK) independently assessed whether the interventions in the studies met the six criteria of “specialized allied health care in PD” as listed in Table 1. In case of disagreement, consensus was reached by discussion. The results of the assessment are presented in Table 2; the detailed assessment in Supplementary Material C. If the characteristics of the interventions were not (clearly) described, we labeled it as uncertain or not (fully) reported. Only one study evaluated an intervention that met all the six criteria. 71 In the other eight studies, the authors did not (clearly) specify whether the AHPs were trained in PD. Only in four studies did the description of the intervention indicate a personalized approach.66,70–72, 66,70–72 Furthermore, although the programs were developed for the PD population, it was difficult to ascertain whether they were consistent with evidence-based interventions in most of the studies. Similarly, it was unclear whether the treatment context was appropriate in the majority of studies. Interventions were often provided in a clinical inpatient or outpatient setting. Only two interventions were (partly) delivered in the home-setting.66,71, 66,71 In two trials, the intervention dose was insufficient to expect improvement in symptoms or the utilization of new skills and strategies.66,72, 66,72
With regard to the selected outcomes, it is evident that the studies have made deliberate choices to limit the number of outcomes. Consequently, many studies employ an outcome that assesses the overall quality of life, such as the PDQ-39. In addition, several motor performance scores were selected. While speech-language therapy was incorporated into the treatment program in five studies, none of them included any outcome measures related to voice, speech, or communication, except for single items in the UPDRS. 75
With respect to the effectiveness of the interventions, six trials demonstrated improvements in primary outcome measures in the intervention group in comparison to the control group.67,68,70,71,73,74, 67,68,70,71,73,74 Thus, three trials showed no improvement.66,69,72, 66,69,72 Of the nine studies, the two trials who did not meet the criterium of appropriate dose showed no improvement.66,72, 66,72 We can only hypothesize that this played a role in the outcome, because other criteria might have played a role as well. Due to the heterogeneity of intervention characteristics and outcomes in the studies, it is difficult to determine other correlations between criteria and outcomes.
In addition to the evidence from randomized controlled trials, a recent large observational study in the Netherlands found that specialized occupational therapy was most effective in preventing PD-related complications, such as fractures, when combined with specialized physical therapy. The protective effects were larger than those observed in individuals who only received specialized physical therapy. These findings suggest that the combination of specialized AHPs may have synergistic protective effects. 63
Gaps and future perspectives
Although there is a growing body of evidence for specialized physical therapy, occupational therapy and speech-language therapy in PD, there is a need for further research to address key remaining gaps in knowledge. Table 3 presents specific recommendations for high-priority research questions that should be addressed. It is important that future collaborative studies build upon the working criteria for specialized allied health care in PD as presented in this article and expand to incorporate other allied health disciplines, such as psychology and dietetics. Ideally, future refined criteria should include the perspectives of specialized AHPs across the world. In light of this, the recent publication of an international consensus statement on rehabilitation in PD is welcome development. 9 The statement includes key principles of rehabilitative care in PD and recommendations for the content and organizational aspects of rehabilitative care. Future collaborative studies should integrate these principles into a refined set of criteria for specialized allied health care in PD. Once established, the criteria for specialized allied health treatment can serve as a foundation for intervention protocols, systematic review protocols and meta-analyses.
Recommendations for future research on specialized allied health care for Parkinson’s disease
Aside from further research into its effectiveness, the implementation of specialized allied health programs in the care of people with PD across different populations will present significant challenges. Potential barriers may include both person-level and system-level factors. 76 Future implementation studies should therefore also examine specific facilitators and barriers of implementation by country, region, setting, stage of disease, gender, socioeconomic status or racial and ethnic group.76–80 Due to the growing number of people living with PD worldwide,81,82, 81,82 the demand for access to specialized allied health care for PD is likely to increase in the coming years. This highlights the need for studies that address the existing gaps in this area.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
Ingrid Sturkenboom has received research grants from The Netherlands Organisation for Health Research and Development.
Amir Talebi has no conflict of interest to report.
Bart Maas has no conflict of interest to report.
Nienke de Vries has received research grants from The Netherlands Organisation for Health Research and Development, the Michael J Fox Foundation and Verily Life Sciences. She serves as an associate editor of the Journal of Parkinson’s disease.
Sirwan Darweesh has received funding from the Parkinson’s Foundation (PF-FBS-2026), ZonMW (09150162010183), ParkinsonNL (P2022-07 and P2021-14), Michael J Fox Foundation (MJFF-022767) and Edmond J Safra Foundation.
Johanna Kalf has received research grants from the Michael J Fox Foundation, The Netherlands Organisation for Health Research and Development and the Dutch Association for Speech and Language Therapy.