
Abstract
Background:
Parkinson’s disease (PD) is a complex neurodegenerative disorder impacting everyday function and quality of life. Rehabilitation plays a crucial role in improving symptoms, function, and quality of life and reducing disability, particularly given the lack of disease-modifying agents and limitations of medications and surgical therapies. However, rehabilitative care is under-recognized and under-utilized in PD and often only utilized in later disease stages, despite research and guidelines demonstrating its positive effects. Currently, there is a lack of consensus regarding fundamental topics related to rehabilitative services in PD.
Objective:
The goal of the international Parkinson’s Foundation Rehabilitation Medicine Task Force was to develop a consensus statement regarding the incorporation of rehabilitation in PD care.
Methods:
The Task Force, comprised of international multidisciplinary experts in PD and rehabilitation and people directly affected by PD, met virtually to discuss topics such as rehabilitative services, existing therapy guidelines and rehabilitation literature in PD, and gaps and needs. A systematic, interactive, and iterative process was used to develop consensus-based statements on core components of PD rehabilitation and discipline-specific interventions.
Results:
The expert-based consensus statement outlines key tenets of rehabilitative care including its multidisciplinary approach and discipline-specific guidance for occupational therapy, physical therapy, speech language pathology/therapy, and psychology/neuropsychology across all PD stages.
Conclusions:
Rehabilitative interventions should be an essential component in the comprehensive treatment of PD, from diagnosis to advanced disease. Greater education and awareness of the benefits of rehabilitative services for people with PD and their care partners, and further evidence-based and scientific study are encouraged.
Keywords
INTRODUCTION
Parkinson’s disease (PD) is a complex and progressive neurodegenerative condition occurring in over 10 million people worldwide and has both motor and non-motor symptoms that can affect functional abilities and quality of life [1–5]. Rehabilitative interventions play a crucial role in PD care and improving health outcomes, with growing evidence demonstrating benefit for motor and non-motor functioning, activities of daily living (ADL), and quality of life [6–10]. Several guidelines and quality standards propose incorporation of occupational therapy (OT), physical therapy/physiotherapy (PT), and speech and language pathology/therapy (SLP) in PD care, as well as exercise and physical activity [11–13]. Several research studies support multidisciplinary rehabilitative care to utilize basal ganglia circuitry, neuroplasticity, goal-based practice, and task-specific motor and cognitive training [14–22]. Despite these guidelines and increasingly recognized benefits of OT, PT, and SLP for PD, rehabilitation therapy referrals and utilization rates are low in many countries, even in expert specialty centers [23–26]. Data from the Parkinson’s Foundation Quality Improvement Initiative, reflecting over 5,000 participants from 4 countries, revealed that less than 1/3 of PD patients were referred for rehabilitation services, with rates of 30.4%, 8.0%, and 7.5% for PT, OT, and SLP, respectively [24]. Referral to rehabilitation specialists more often occurs late in the disease when complications such as falls or dysphagia occur [24], thereby missing critical opportunities to proactively limit or prevent functional decline even early in the course of PD.
At present, consensus is lacking regarding many fundamental topics and key points related to rehabilitative services in PD, ranging from the composition and integration of the rehabilitation team to the optimal setting, timing and delivery needed to inform best practices. While there are individual discipline-specific guidelines (e.g., OT, PT, and SLP) and papers on organizing multidisciplinary care, there are no integrated international guidelines outlining key principles of multidisciplinary rehabilitative care and practices in PD [17, 28]. This lack of guidance limits the appropriate inclusion of rehabilitative services in PD and the provision of optimal care for people living with PD. Developing a unified understanding of the role of multidisciplinary rehabilitative care in PD represents a key step in improving patient outcomes.
This paper aims to address these challenges by providing a consensus statement based on expert opinion, best available evidence, and a priori processes as an initial step toward international guidance and frameworks for comprehensive, integrated rehabilitative care-delivery models in PD. In this regard, consensus statements (in contrast to clinical practice guidelines, which are recommendations based on systematic reviews of evidence and assessment of benefits and harms of alternative care options [29]) are particularly helpful when there is variability in clinical practices and evidence, and opportunities to improve quality of care. To date, clinical practice guidelines for rehabilitation in PD typically focus on individual disciplines (i.e., PT, OT, or SLP) separately, rather than in an integrated, inter-related approach, and recommendations for timing, content, and delivery vary by geographical region (e.g., United States, Europe, United Kingdom, Canada) and organization (e.g., American Academy of Neurology and professional rehabilitation organizations) [11, 30–34]. Furthermore, despite these practice guidelines, rehabilitation services for PD have limited utilization and are inconsistently organized and implemented [23, 26]. Thus, the objective of our work was to achieve consensus among experts in multidisciplinary rehabilitation and PD regarding fundamental components of rehabilitative care for PD and optimal interventions for rehabilitation therapies most often encountered in PD.
METHODS
Purpose and overview
The Parkinson’s Foundation established a Rehabilitation Task Force to address the lack of consensus regarding use of and guidance for rehabilitation care in PD. The Task Force utilized a systematic approach to develop an international consensus statement regarding multidisciplinary rehabilitation in PD with the following steps: 1) defining goals and timeline, 2) conducting a literature search and narrative review, 3) defining scope of the consensus statement, 4) discussing the literature and drafting the consensus statement, 5) developing and refining the proposed statement using a systematic, interactive, and iterative process, and 6) manuscript development.
Task Force and Steering Committee
The Task Force was comprised of international PD clinical, research, and rehabilitation healthcare experts, a person with PD, and care partner of a person with PD. Multiple professional disciplines were represented, specifically including movement disorders neurology, neuropsychology, nursing, OT, physiatry, PT, rehabilitation science (the field of research related to rehabilitation, e.g., its scientific basis, delivery models, implementation, among other topics), and SLP (see Supplementary Material for Task Force members). In the context of this initiative, the term “expert” was defined as “healthcare professional, researcher, or academic with expertise in the treatment, service provision, research or analysis of multidisciplinary rehabilitation in PD or a person with first-hand lived experience with PD.” The panel was identified by the Parkinson’s Foundation project leads and Rehabilitation Task Force co-chairs based on their recognized clinical experience in PD across the disease spectrum, scientific research and scholarship contributions to the field of PD and rehabilitation, and lived-experience.
All members were considered to have relevant knowledge and experiences to share and equally weighted voices in the Task Force, reflecting the teamwork and multidisciplinary nature typical of the field of rehabilitation. An expert panel of approximately 15 participants was planned, in keeping with our aim of having representation across disciplines and international regions, gender balance, and previously recommended panel sizes [35, 36].
The Steering Committee was comprised of the Rehabilitation Task Force co-chairs and Parkinson’s Foundation project leads, along with external healthcare consultants (Avalere, based in Washington, D.C.), who provided oversight and input for the project. The consultants assisted with preparing discussion topics, workshop materials, and iterative feedback; facilitating group discussions to ensure participation from all members, listening for any dissenting opinions or areas for additional discussion, and helping achieve consensus; and distributing, receiving, and reviewing votes on the statements for consensus agreement.
Preparation for Task Force discussions
In preparation for the group discussions, a narrative review of the literature was performed, thereby reviewing published systematic reviews, meta-analyses, guidelines, and seminal articles regarding evidence for rehabilitative interventions in PD from 2002–2022. The purpose of the review was to provide a broad overview on the topic of rehabilitation in PD with critical, comprehensive, objective, and current knowledge and to help establish a framework for the Task Force and context for the proposed consensus statement. As the Task Force paper was not intended to be a clinical practice guideline, our methodology did not include a formal systematic review of PD rehabilitation literature, though it incorporated existing systematic reviews on this topic into its review and group discussions [8, 28–47]. Several primary PD guidelines were reviewed specifically for their reference to rehabilitative therapies [11, 37–41]. Limited emphasis on rehabilitation in existing guidelines, along with variability in the types of rehabilitation disciplines included and PD symptoms and treatments emphasized, further reinforced the rationale for our objective of developing a collective perspective on comprehensive, multidisciplinary rehabilitation approaches for PD.
Consensus-building process
Members participated in virtual workshops between February and October 2021 to discuss the current evidence for rehabilitation in PD and topics such as optimal interventions, team composition, and discipline-specific rehabilitation considerations. Workshops were used to develop the consensus statements regarding rehabilitative care and interventions for OT, PT, SLP, and psychology/neuropsychology (Fig. 1).
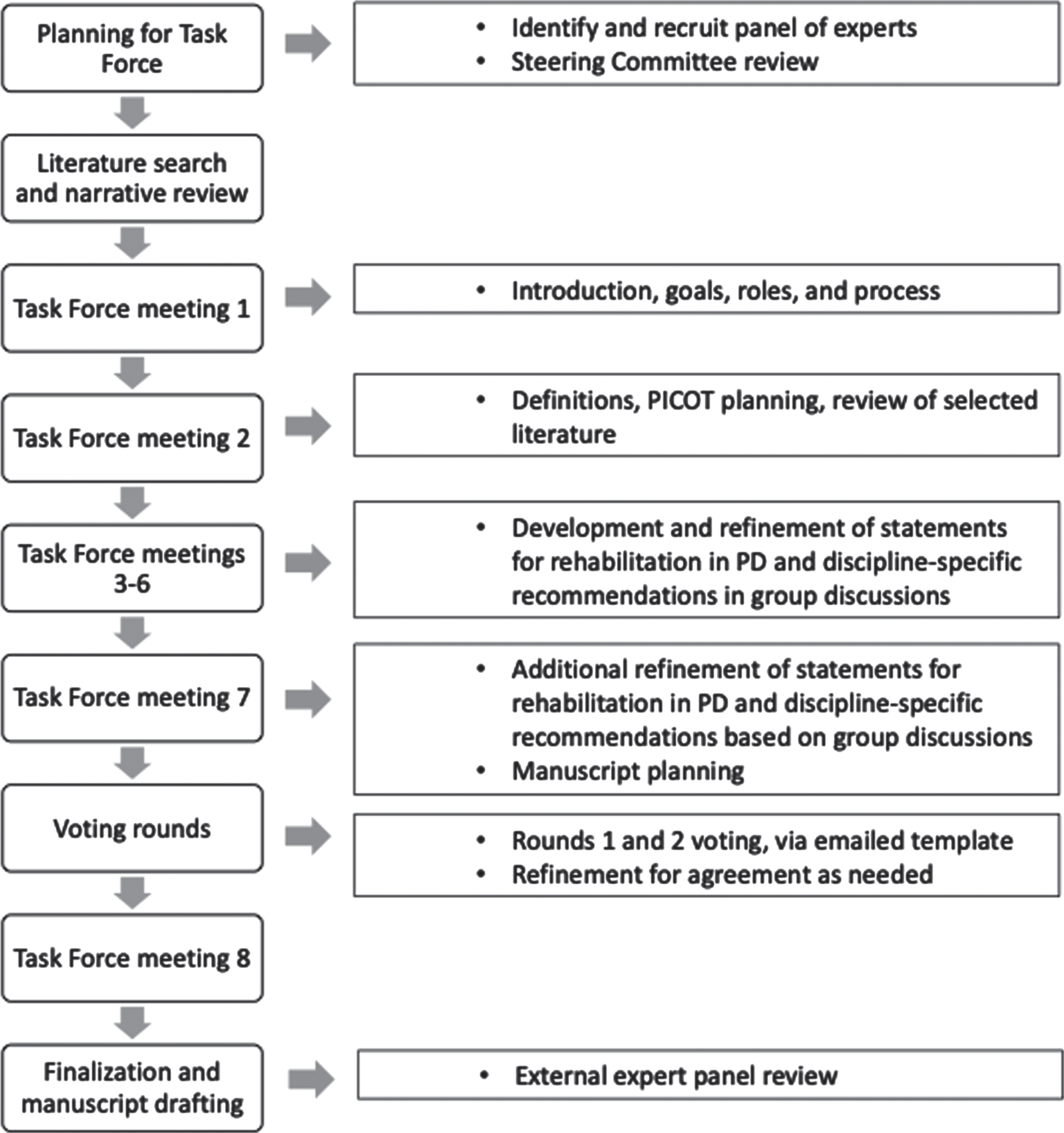
Task Force process.
The Task Force defined the scope and parameters of the consensus statement using the PICOTS framework (i.e., Population, Interventions, Comparisons, Outcomes, Timing, and Settings) [42]. As such, the following parameters for the work were identified: Population (PD, all stages), Interventions (rehabilitation services), Comparisons/Co-interventions (other care services such as medications, surgery, education, and supportive services often utilized in PD), Outcomes (functional outcomes, patient goals, quality of life, symptomatic therapies), Timing (all stages of PD, including at diagnosis and early PD), Settings (multiple locations including hospital, outpatient, and others).
The Task Force achieved consensus on items using a structured and iterative process of developing and refining key statements, incorporating the evidence reviewed and collective expert opinion via virtual face-face conversations and email correspondences. We collected and aggregated information from the expert panel through multiple iterations and feedback. These discussions were organized and guided by the Steering Committee, including the healthcare consultants who provided oversight and encouraged and solicited participation from all members. This process enabled the group to maintain effective communication and open expression of opinions, dialogue and critique of topics, and response to iterative feedback.
The proposed tenets and recommendations were voted on anonymously by Task Force members using an emailed voting template, to which each member responded individually to the healthcare consultants so that independence and anonymity was respected. The voting for the discipline-specific interventions for OT, PT, SLP, and psychology/neuropsychology additionally included the physician co-chairs of the Steering Committee to capture their perspectives on the rehabilitation disciplines. The voting template format consisted of an excel spreadsheet listing the proposed items, request to “mark yes or no for agreement” for each item, and opportunity to provide commentary. Votes were tallied and noted as achieving consensus when at least 80% approved. As percentages for agreement vary in the literature, we wanted to ensure majority consensus in our international panel where wide variations in practice might occur, and thereby adopted a more conservative approach [43–45]. Any dissenting opinions were discussed during virtual workshops and resolved with majority agreement. For analysis, we calculated counts and proportions for the voting. Taking a conservative approach, we counted missing data for individual items as a “no” vote. Building on the iterative process, feedback and discussion, two rounds of voting were performed.
RESULTS
Task Force and Steering Committee composition
The Task Force members represented movement disorders neurology (n = 3), neuropsychology (n = 2), nursing (n = 1), OT (n = 2), physiatry (n = 1), PT (n = 2), rehabilitation science (n = 1), SLP (n = 2), person with PD (n = 1, also a PT), and care partner (n = 1). The Steering Committee included a movement disorders neurologist with neurorehabilitation expertise and a physiatrist (Task Force co-chairs), along with Parkinson’s Foundation staff of whom 2 also had professional experience in OT and nursing. The total group included 12 females and 9 males, residing across 7 countries (United States n = 12, Australia n = 2, Italy n = 2, United Kingdom n = 2, Canada n = 1, France n = 1, Netherlands n = 1 participant). Of the Task Force members, 79% had over 20 years of experience in their discipline and 66% reported over 20 years focused on rehabilitation.
Definitions and terminology
Building on fundamental concepts of rehabilitation from the World Health Organization and British Society of Rehabilitation Medicine [46, 47], the Task Force proposes that rehabilitation in the context of PD be defined as a process of active changes through interventions designed to optimize physical, psychological, social, cognitive and behavioral functioning for individuals at all stages of PD.
Throughout this statement, the Task Force utilizes a schema delineating four clinical stages of PD in order to capture a functional point of view, adapted from Thomas and MacMahon [48, 49] as: “Upon Diagnosis, Early-Stage, Mid-Stage, and Advanced-Stage PD.” While other PD staging methods exist (e.g., Hoehn and Yahr) [50], they focus mostly on motor aspects of PD. Incorporating both motor and functional features of PD into rehabilitative therapy is essential to our approach. The Task Force also recognizes that various terminology, such as “multidisciplinary,” “interdisciplinary,” “integrated,” is often used interchangeably in the literature to describe similar yet nuanced concepts (Table 1) [51]. For consistency in this article, multidisciplinary is used to describe the integrated care model of the rehabilitation team.
Key definitions and terminology
Statements and guidance for rehabilitation in PD
The consensus-based statements presented here address fundamental components of rehabilitative care for PD, including A) key principles of rehabilitative care; B) composition of the rehabilitation care team; C) rehabilitation care planning; D) timing and settings for rehabilitative services; and E) education and training of rehabilitation professionals for PD (Table 2). These statements help establish paradigms for high-quality rehabilitative care for PD. Additionally, the Task Force proposes optimal rehabilitative interventions across four rehabilitation therapy disciplines: OT, PT, SLP, and psychology/neuropsychology (Tables 3–6). The Task Force also highlights several emerging rehabilitative therapies with examples provided in the tables, but given their current state of evidence-base, the Task Force does not offer formal recommendations for these areas.
Tenets and recommendations for rehabilitative care in PD
Optimal rehabilitation assessments and interventions for occupational therapy
ADL: activities of daily living; IADL: instrumental activities of daily living; LSVT: Lee Silverman Voice Treatment. *Meaningful activities include physical, social, and leisure activities that are tailored to the person’s needs and preferences. May include activities of daily living (ADL) or leisure activities, may be structured or spontaneous, and may provide emotional, creative, intellectual, and spiritual stimulation.[216]. NOTE: The assessments and interventions listed in this table are not a comprehensive list of all strategies used in PD. These are examples that may be used and tailored to a person with PD’s specific needs and goals. Not all treatment approaches listed in this table will be applicable for every individual. Furthermore, there may be items listed in later stages that may also be applicable upon diagnosis or in earlier stages, depending on the individual.
Optimal rehabilitation assessments and interventions for physical therapy
*Exercise defined as: “A subcategory of physical activity that is planned, structured, repetitive, and purposive in the sense that the improvement or maintenance of one or more components of physical fitness is the objective” [13]. NOTE: The assessments and interventions listed in this table are not a comprehensive list of all strategies used in PD. These are examples that may be used and tailored to a person with PD’s specific needs and goals. Not all treatment approaches listed in this table will be applicable for every individual. Furthermore, there may be items listed in later stages that may also be applicable upon diagnosis or in earlier stages, depending on the individual.
Optimal rehabilitation assessments and interventions for speech language pathology
NOTE: The assessments and interventions listed in this table are not a comprehensive list of all strategies used in PD. These are examples that may be used and tailored to a person with PD’s specific needs and goals. Not all treatment approaches listed in this table will be applicable for every individual. Furthermore, there may be items listed in later stages that may also be applicable upon diagnosis or in earlier stages, depending on the individual.
Optimal rehabilitation assessments and interventions for psychology/neuropsychology
NOTE: The assessments and interventions listed in this table are not a comprehensive list of all strategies used in PD. These are examples that may be used and tailored to a person with PD’s specific needs and goals. Not all treatment approaches listed in this table will be applicable for every individual. Furthermore, there may be items listed in later stages that may also be applicable upon diagnosis or in earlier stages, depending on the individual.
All Task Force members (n = 16) completed voting rounds for the statements regarding fundamental components of rehabilitative care. In round one, there was > 80% consensus on all items, except one, and comments provided. With feedback and discussion, the statements were revised and refined in their ordering and wording (e.g., to reflect an international audience, reduce repetition, etc.). After revisions, they received unanimous (100%) agreement. For the discipline-specific interventions, voting was completed by 15 of 18 group members and met with > 80% agreement on the suggested OT, PT, SLP, and psychology/neuropsychology strategies.
Fundamental components of rehabilitative care for PD
Rehabilitative care in PD is grounded in several key tenets: the recognition of the complexity and heterogeneity of PD symptoms and progression; the importance of an individually tailored, comprehensive, and collaborative therapeutic approach; and its role, alongside medical, surgical, experimental, and other strategies often utilized in PD, but also as monotherapy at times [12]. Given this complexity, rehabilitation for PD should involve the person with PD and care partners (if present) throughout the process, thereby adopting a person-centered approach and shared decision-making model to promote symptom management and self-efficacy [28, 52].
To ensure a comprehensive approach, the rehabilitation care team should include multiple disciplines working together in a coordinated fashion, along with the person with PD and care partners. The clinical team should have knowledge and expertise specific to PD and rehabilitation. Composition and structure of the rehabilitation team may vary across the world depending on patient needs related to their motor and non-motor symptoms, stages of disease, and individual goals and priorities; different practice settings; local or national health systems; and availability of trained personnel, but at its core may include those listed alphabetically in Fig. 2.
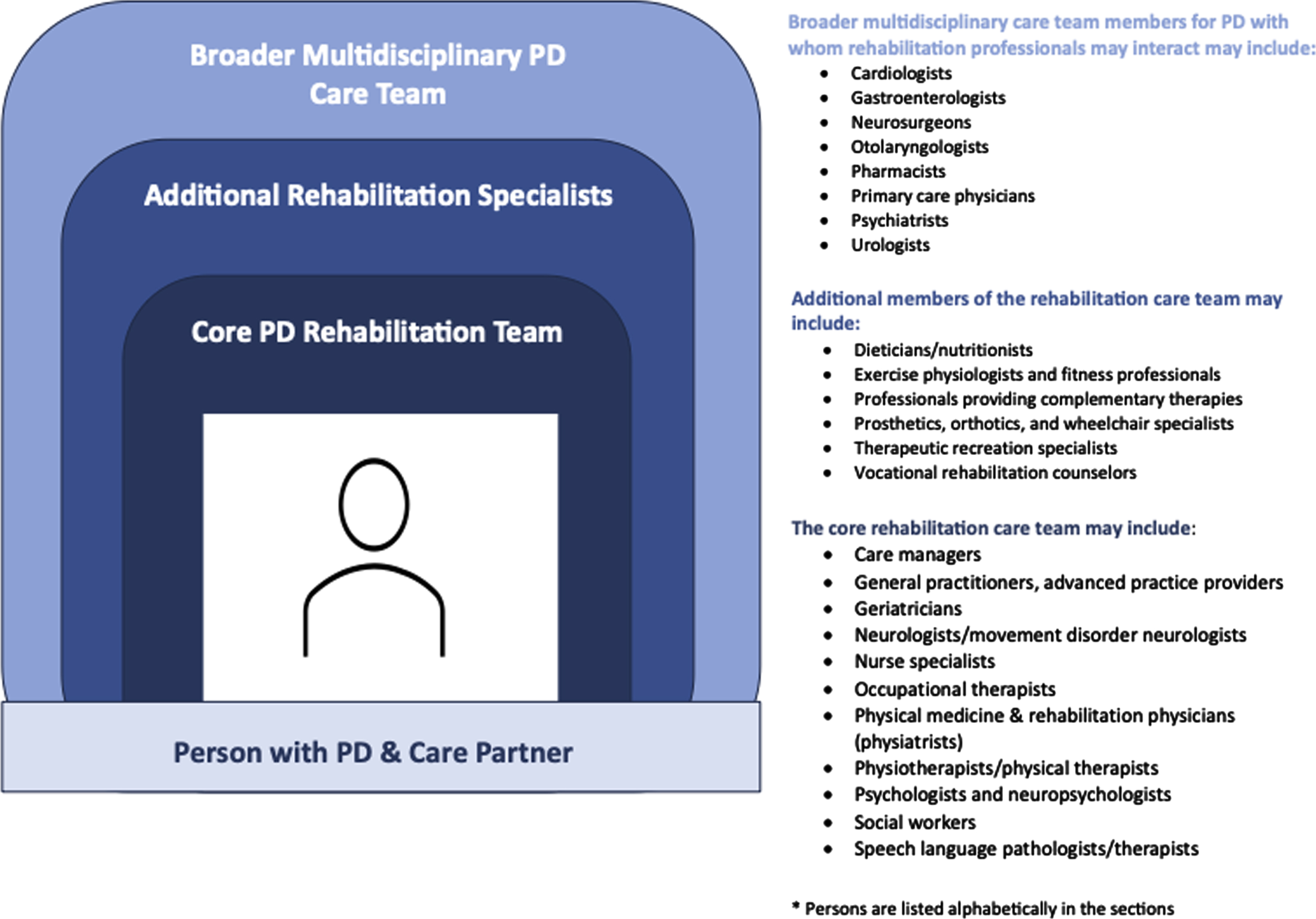
Core Rehabilitation Care Team and Other Relevant Healthcare Professionals for PD.
The rehabilitation team is anticipated to interact with other healthcare professionals of the PD multidisciplinary care team (e.g., cardiologists, gastroenterologists, neurosurgeons, pharmacists, psychiatrists), among others [27]. To date, the optimal combination of these multidisciplinary rehabilitation and other healthcare professionals in PD care is unknown [41] but should be tailored to each individual’s specific needs.
Care coordination and communication among the rehabilitation team, other PD-related multidisciplinary team members, the person living with PD, and care partners are critical to support an optimal approach to rehabilitation care [27, 53]. In some settings, the physiatrist plays a key role in coordinating and working with the multidisciplinary rehabilitation care team in PD; this teamwork may occur in different rehabilitation care settings (e.g., inpatient rehabilitation hospital, outpatient, or day rehabilitation) and may vary across geographical locations [26, 54]. However, in other locations and settings, this care coordination may be spearheaded by other team members such as movement disorder neurologists, geriatricians, nurses, case managers, social workers, or rehabilitation therapists.
A unifying principle of rehabilitative care is the integration of the multidisciplinary team. This integration may be facilitated on a practice level by scheduled and regular multidisciplinary rehabilitative team meetings in outpatient, inpatient rounding, and/or case conference settings [27, 56]. Examples from interprofessional, multidisciplinary rehabilitation care for stroke and other neurological conditions may provide insights for team-based opportunities for people with PD [57–59]. Additionally, the inclusion of people with lived experience and shared decision making into team settings is an actively growing area in PD [60, 61]. Ideally, clinical activities are supported by and combined with educational and research-related activities (e.g., interprofessional journal clubs, seminars, and projects involving various rehabilitative care team members, clinicians, and scientists working together and co-leading, where appropriate). These settings may enrich interactive discussions among team members regarding topics such as evidence-based and cost-effective interventions for integrated care and bridging clinical care and research. Clinical-research-patient partnerships may help advance the scientific and evidence-base of rehabilitation therapies, delivery models, and implementation in clinical settings. Successful multidisciplinary integration requires knowledge and skill building related to teamwork and communication.
Rehabilitative care planning should emphasize the needs and goals of the person with PD, develop strategies for self-management, and include care partners where appropriate [26]. Furthermore, the Task Force recommends that rehabilitative interventions occur across the continuum of PD, from the time of diagnosis through advanced disease stages. Baseline rehabilitation assessments and serial follow up are recommended with adjustments to goals as a person’s needs change in order to enable timely provision of continuous care in the context of a progressive disease [62].
Rehabilitative care may occur in a variety of settings depending on geographical and cultural diversity, available trained personnel, resources, and patient needs. Providing optimal PD rehabilitative care likely necessitates addressing potential barriers such as access, insurance coverage, availability of trained personnel, social and cultural factors, and other elements that may limit referrals and care utilization.
Education about the role of rehabilitative interventions, types of providers, and access to care is needed for the PD patient community and the healthcare professional community. For healthcare professionals, PD-specific education and training in rehabilitation disciplines is paramount. For example, the ParkinsonNet concept has proven that PT delivered by specialized therapists in PD leads to better quality of care and lower complication rates compared to PT delivered by general therapists [63]. Developing communication skills and effective teamwork among clinicians is also essential [64].
Guidance for discipline-specific rehabilitative interventions
Based on the available evidence-base and its expert opinion, the Task Force presents what it considers optimal rehabilitative interventions across the stages of PD for the disciplines of OT, PT, SLP, and psychology/neuropsychology. The Task Force chose to focus on these disciplines for this document given current literature supporting their roles in PD and their generally greater availability and accessibility to the PD community across diverse practice settings and delivery models, even though often under-utilized, at present [23, 56]. To date, the largest body of evidence exists for PT, and PT is more commonly represented among rehabilitation services used in PD compared to OT and SLP [23, 24]; however, for this document, we have chosen to present the rehabilitation disciplines in alphabetical order as OT, PT, and SLP, followed by psychology/neuropsychology. We acknowledge the important roles of other healthcare disciplines in rehabilitative care for PD, and future recommendations may highlight professionals such as care managers, dieticians/nutritionists, exercise physiology, nurse specialists, social workers, and therapeutic recreation, among others, as their evidence bases increase [53]. The interventions proposed for OT, PT, SLP, and psychology/neuropsychology are intended to be utilized in an integrated but flexible fashion that allows for cross-disciplinary collaboration to address specific needs and goals in PD, especially as these may change in a chronic, progressive condition. While beyond the scope of this work to depict, there are many examples where the rehabilitative team can communicate and work across different disciplines (e.g., SLP and OT for cognition and communication skills in everyday activities; SLP and nutrition regarding dysphagia; OT and PT for dual-tasking and navigating home or other environments; psychology and PT for motivation and exercise).
Regardless of discipline, rehabilitative care professionals should conduct PD-related baseline assessments upon diagnosis and at regular re-evaluations over the disease course and accordingly adjust interventions for different needs and goals [65], ensure collaborative teamwork and person-centered care to tailor interventions and enhance self-management strategies, and coordinate with multidisciplinary team members, as appropriate, to establish and deliver care plans. For the disciplines discussed here, assessments and interventions may occur in a variety of settings, including outpatient therapy, inpatient rehabilitation, day programs, home therapy, skilled nursing facilities, and via telehealth.
Occupational therapy
Occupational therapists help people restore, improve, and maintain skills and abilities to participate in meaningful activities [66]. For people living with PD, occupational therapists foster improvement, safety and independence in self-care, daily tasks, and functional mobility to support continued engagement in activities related to various environments such as the home, work, and community [65]. Occupational therapists play a role in educating and supporting care partners to safely and appropriately assist the person with PD in daily tasks while being mindful of their own safety and well-being [67]. Occupation-based performance assessments should be led by an occupational therapist skilled in the use of PD-specific intervention approaches [68]. The occupational therapist should collaborate with the person with PD and care partner to prioritize goals that are meaningful and relevant, select outcome measures that inform interventions, and support engagement in the therapy process. An individualized, goal-oriented approach—where OT intervention is focused on a specific set of personally meaningful goals—has been shown to yield greater improvement for people with PD compared to use of a generalized approach [69]. The role of OT in PD is supported by the American Occupational Therapy Association clinical practice guidelines [34] and systematic reviews with moderate to strong evidence for OT-related interventions for activities of daily living, instrumental activities of daily living, handwriting, physical activity, but lower evidence to date for cognitive rehabilitation [70–72].
Several categories of OT-related interventions for people with PD have been identified: 1) exercise or physical activity; 2) environmental cues, stimuli, and objects; and 3) self-management and cognitive behavioral strategies [34, 73]. Occupational therapy strategies may include a combination of personalized adaptation of tasks and daily routines, cues and compensatory strategy training, adaptations to the physical environment, and incorporation of concepts of motivation, reward, and learning [67].
Emerging areas of intervention in occupational areas include sleep, activities of daily living (ADL), instrumental activities of daily living (IADL), leisure, and social activities [34]. Systematic reviews identify several beneficial interventions for ADL such as multidisciplinary inpatient rehabilitation [16, 75], group multimodal exercise programs [74, 76–78], and home-based hand exercise programs [74, 79]. Cognitive behavioral therapy (CBT) focused on sleep hygiene and behaviors [80, 81], resistance training, multimodal exercise, and mindfulness meditation combined with exercise can be used to improve sleep [74, 82–84]. Evidence supports interventions for IADL including education, mentoring, social support, and behavioral change techniques to increase activity levels and multimodal exercise programs that promote IADL participation, function, and social engagement [34, 85–89]. Handwriting may improve with use of intensive amplitude training with visual targets [90, 91], hand exercises, and writing activities [92]. Dual-task training can be used to forge stronger connectivity between two task-specific networks to enable smoother performance of selected tasks such as carrying items while walking [93] which can link OT with PT interventions. Goal-oriented cognitive rehabilitation for dementia associated with PD was found to be feasible, with improved quality of life including care partners [1, 94]. As PD progresses, sensory and cognitive coping strategies may wane in effect, and goals may shift. Participation in work/employment, driving, and other home or hobby endeavors may change with PD progression, and OTs may play a role in these areas.
Physical therapy
Physical therapists are experts in human movement who diagnose, evaluate, and treat individuals to improve their ability to move, manage pain, and prevent or manage disability [95]. For people with PD, physical therapists play a role in areas such as physical movement, gait and balance, exercise interventions, daily activities, among others. The initial visit to a physical therapist may occur before or at the onset of medication initiation and may coincide with initial visits to other members of the rehabilitation team, including occupational therapists and speech language pathologist/therapist. The role of the PT in PD is supported by clinical practice guidelines [72, 96] and systematic reviews that include Class I and Class II randomized clinical trials. PT can improve gait, balance, and falls in early and moderate stages of PD, though additional evidence base in advanced PD is needed. Recently published PT clinical practice guidelines offer the highest strength of recommendation for aerobic exercise, resistance training, balance training, community-based exercise, gait training, task-specific training, and integrated care [96].
The components of PT intervention incorporate a variety of forms of physical and cognitive exercise and strategy training [8, 97]. Moderate to high-intensity aerobic exercise has been shown to reduce the severity of motor symptoms, increase oxygen consumption, and improve function [96, 98–100]. These benefits have been demonstrated in early (including de novo) PD, suggesting the importance of early engagement in aerobic exercise [99, 100]. Treadmill training and cycling yield similar results, thereby, suggesting that aerobic exercise benefits cross a variety of modalities [99, 100]. Resistance training has been shown to reduce bradykinesia and improve force production, cognition and function [101, 102]. Balance training (e.g., Tai Chi, dance, virtual reality, motor-cognitive training, multicomponent balance exercises) is a critical element of exercise in PD [103–106]. Evidence reveals improvements in balance outcomes with balance training, although the impact on falls is mixed [107–109]. Studies suggest that people in moderate (i.e., early fallers) rather than later stages of PD are more likely to respond to balance training, thereby reducing fall frequency [107, 111]. These findings support the initiation of early balance training to mitigate falls and secondary complicating conditions.
Strategy training in PT improves function in PD [112, 113]. For example, gait training encompassing cueing (e.g., metronome, music, instructional cues to “take long steps,” and vibrotactile feedback), strategies to overcome freezing of gait, and dual-task training (e.g., cognitive-motor interference) have been shown to improve a variety of gait outcomes, particularly when tailored to the individual’s needs [93, 114–119]. Exercises and strategy training also improve walking, turning, and general mobility such as chair and bed mobility [97, 120]. Many of these interventions encompass task-based or skill practice which needs to be implemented with sufficient dosing (e.g., high repetitions) to optimize motor learning [22]. Therefore, training should be initiated early in the disease process as persons with PD may require more time to achieve learning. In the later stages, explicit learning methods and cueing may enhance learning [121]. Context-specificity should be considered by matching the learning environment as closely as possible to the daily functional context to optimize learning [22].
Motor-cognitive approaches in PD, or “cognitive oriented physical therapy,” reflect techniques that incorporate dual-task training or multitasking, or use cognitive strategies in order to cope with motor disability. Principles related to the complex interplay between basal ganglia-cortical and cerebellar networks suggest that rehabilitative interventions geared to engage cognition may indeed harness motor learning schema leading to broad clinical, motor and functional benefits [122, 123].
Though evidence is limited, rehabilitation and exercise may improve postural deformities in PD, particularly if initiated early [124]. Increased exercise and physical activity have been shown to improve non-motor symptoms including depression, anxiety, cognition, and sleep [125], though more evidence is needed. Incorporating behavioral change and self-management strategies into PT interventions is important to sustain engagement in exercise with the goal of optimizing long-term functional outcomes.
Speech and language pathology/therapy
Speech and language pathologists/therapists are experts in communication who evaluate and treat communication issues, including speech sounds and production, volume, language, swallowing, and cognitive aspects. For people with PD, speech language pathologists/therapists play a role in optimizing speech production, voice function, dysphagia, language and cognition, and for some, saliva management [126, 127]. In their roles, speech language pathologists/therapists may readily interface with other rehabilitation team members such as dieticians/nutritionists, otolaryngologists, and occupational therapists. As speech language pathologists/therapists may work with people regarding cognitive-communication functions, coordination, and communication, collaboration with neuropsychologists is paramount. The role of SLP is supported by systematic review for improving hypokinetic dysarthria and dysphagia, though greater evidence base is needed in the literature [12, 128–131].
SLP therapy in PD utilizes strategies to improve voice and speech, particularly hypophonia; communication, such as attention to effort therapies [132]; and safety and efficiency of swallowing to minimize risk of aspiration such as expiratory muscle strength training (EMST). Meta-analyses and Cochrane reports on voice, speech, and language therapies highlight challenges of small sample sizes and lack of randomized control trials [133, 134]. Nonetheless, SLP interventions are selected on individualized needs and use techniques such as breathing control, vocal training, speech control training, articulation therapy, or even singing [135, 136]. As pharmacological and neurosurgical treatments may have variable and sometimes adverse, unpredictable effects on improving speech production, SLP evaluation and interventions play an important adjunctive role in these contexts [137]. Regular SLP outcome measures should be obtained for vocal loudness in conversational speech, pitch range, maximum phonation time, intelligibility rating, and for swallowing. Intensive speech programs with amplitude-based training should be considered, including the Lee Silverman Voice Treatment (LSVT®), which has the largest evidence-base to date [138, 139], pitch-limiting voice treatment, or SPEAK OUT! [140, 141]. Singing provides another modality to enhance voice and help people with PD engage socially and in leisure activities [142, 143]. Use of volume monitoring apps, audio recordings, and other technologies can provide ways to self-monitor voice and speech production, volume, and facial expression and thereby receive external feedback and cues for adjustments [144–148]. Referrals for augmentative alternative communication technology to supplement speech and optimize communication (e.g., alphabet and picture charts, communication apps with key words and phrases spoken out, text-to-speech apps, pacing boards) may be required if patients experience greater decline in communication ability.
Although dysphagia is highly prevalent in PD, it is often under-reported, and may lead to aspiration pneumonia and other consequences [116, 149–151]. It requires regular clinical assessment and potentially instrumental examinations such as video fluoroscopy or fibreoptic endoscopic examinations, if available. Treatment involves education regarding ways to optimize swallowing safety with food texture modifications, postural changes when eating or drinking, and exercises including LSVT [152], EMST [153], and chin-tuck against resistance [135, 154–157]. Speech language pathologists/therapists may play a role in managing drooling, particularly as oral medications to reduce sialorrhea may have adverse effects or contraindications in PD, and also in improving facial expression [12, 158–160].
Psychology/neuropsychology
Psychologists and neuropsychologists play a role in the assessment and management of cognitive, mood, and behavioral symptoms in PD (e.g., cognitive decline, depression, anxiety, apathy, psychosis, impulse control behaviors, fatigue, and sleep disturbances), and the impact of these issues on relationships, independence, work, and quality of life for the person with PD and care partner. Therapeutic strategies used by psychologists/neuropsychologists may overlap with other disciplines (e.g., social work, SLP, OT, vocational rehab) and may occur simultaneously or separately with medical and surgical interventions. Evidence for the role of psychology and neuropsychology in PD is growing but available evidence on effectiveness of interventions is heterogeneous due to the broad nature of types of symptoms and interventions, small number of studies, and limited robustness of studies at present [161]. Cognitive rehabilitation interventions may improve global cognition, executive function, and memory, but more randomized controlled trials are needed [162–164].
Optimal rehabilitative interventions for neuropsychiatric symptoms should focus on symptom screening, regular assessments, and management including psychoeducation and support for people with PD and their care partners. The screening and assessment for neuropsychiatric symptoms may involve brief screenings (e.g., bedside tests) or more comprehensive neuropsychological test batteries, depending on the needs of a patient, practices, and availability of neuropsychological services.
Management for depression may involve CBT, which has been noted as efficacious for depression whether delivered via in-person, telephone-based, or telehealth video [165–170]. While few randomized controlled studies of CBT for anxiety in PD exist, preliminary investigations report reductions in anxiety symptoms [165, 170].
Cognitive rehabilitation refers to a wide range of interventions focused on improving cognitive function or compensating for cognitive deficits by using individualized programs of specific skill training [171]. Evidence suggests that cognitive training (CT), physical exercise, and the combination of both can improve certain cognitive functions in PD [164, 172–174]. CT may be most effective for those with mild or moderate cognitive dysfunction rather than severe deficits. Evidence based on randomized controlled trials (7 RCTs, 272 pts), though limited, indicates efficacy on working memory, executive functioning, and processing speed domains [174]. CT can be performed using pen-and-pencil or computer-based exercises in individual or small group settings. Tailored “game-like” tasks (videogames and virtual reality) have the advantages of providing immediate feedback, motivating engagement, and being performed at home, which can increase frequency of training and reduce drop-out [175, 176].
In the setting of dementia, the clinical outcomes of a cognitive rehabilitation program should focus on maintaining cognitive competence, ADL, mood, and coping strategies; lessening social and psychological disability; and reducing the experience of ‘burden’ and stress in families. When considering disease-specific characteristics, effective cognitive programs need to be tailored to the PD stages, severity of cognitive dysfunction (i.e., dementia or mild cognitive impairment), and type of cognitive characteristics (e.g., executive function vs. memory) [177].
Emerging rehabilitation therapies in PD
Complementary medicine therapies, community exercise training, and other modalities have increased applications for PD [6, 178]. Examples include mind and body practices (e.g., massage, meditation) [179], dance therapies [180–182], aquatic exercise [78, 183], boxing [141], Nordic walking [184], acupuncture [185], relaxation techniques and mindfulness [185, 186], Tai Chi [187], yoga [188], music therapy [189], art therapy [190], and theater [191]. There are few evidence-based recommendations for the effectiveness of many of these modalities, though this is a growing area of study [192]. However, for some, the evidence supports integration into rehabilitative medicine for PD [6]. In particular, dance (e.g., Irish set dancing, Argentine tango, ballet, ballroom dancing) may improve mobility, gait, balance, fall rates, ADL, and quality of life [180, 194]. Tai Chi has been found to increase mobility, balance, and reduce falls [105, 196]. Aquatic exercise programs also may improve mobility, gait and balance, ADL, and quality of life [78, 198]. With increasing use of these complementary modalities, knowledge of PD symptoms, stages, and safety issues are critical for those professionals involved.
In recent years, the use of technology in PD and rehabilitation has grown including assistive technology (e.g., adaptive technology and devices), wearable sensors, home monitoring, and virtual or augmented reality techniques [199]. Objective assessment and monitoring of motor symptoms across large PD populations and in home or other environments are feasible [200]. Adaptive technology and mobile applications in PD demonstrate promising ways to improve speech, communication, and motor functionality [201]. Assessments with assistive technology in standardized settings are well validated, but studies often had small sizes with significant variability in outcomes and results reported, [202] and controlled trials of adaptive technology and devices are limited to date. Virtual reality techniques have been employed in PD as exergames, immersive environments, and other strategies for promoting physical activity, improving balance and motor function, reducing freezing of gait, and enhancing manual dexterity. Systematic reviews of virtual reality techniques, however, suggest variable methodological quality of studies, thereby limiting conclusions regarding effectiveness and safety for PD rehabilitation at present. While promising, rigorous and robust randomized controlled trials with larger sample sizes are needed [203, 204]. Given the emerging and broad nature of these therapies and interventions, the Task Force does not offer guidance for these interventions at the present time.
DISCUSSION
Robust literature supports the benefits of rehabilitative interventions in PD for motor and non-motor symptoms, functional abilities, and quality of life. However, to date, many healthcare professionals and people with PD remain unaware of the potential impact of rehabilitative services and evidence-based approaches to rehabilitation interventions in PD [23, 26], thereby limiting their use and availability in the PD community. Studies reveal that up to 57% of people with PD are never referred to PT in their lifetime [205], with similar rates regarding referrals to SLP [206]. Furthermore, utilization of rehabilitation services is more likely to occur in later stages of PD despite mounting evidence of benefits from earlier engagement in therapies [24], even at the time of diagnosis, and regarding proactive strategies that impact symptoms and quality of life [26, 208]. Unless contraindicated, physical activity and exercise also should be encouraged given their beneficial effects [89]. In many cases, rehabilitative services are only offered once in the course of the disease. However, given the progressive nature of PD and the subsequent changes in individual’s goals and needs across these different PD stages, rehabilitative care should be offered regularly throughout the disease course with repeat assessments and interventions adapted to changes in a person’s condition or needs [24]. As such, this international consensus statement begins to address these gaps and serves as a first step in raising global awareness of the role of comprehensive rehabilitation programs in PD.
The field of rehabilitation is inherently multidisciplinary, uses a coordinated and integrated team approach, and focuses on goal-oriented, person-centered, and individualized approaches to improve function and quality of life. These elements are essential for PD care, especially due to its complexity, heterogeneity, and chronicity [28, 209]. Indeed, giving patients greater control over their situation through patient-provider collaboration and shared-decision making has recognized benefits in PD [38, 211]. Person-centered, goal-directed interventions have been shown to be more effective than usual care across the continuum of PD [69, 94]. The Task Force consensus statements reflect these key elements of rehabilitative care and services in PD.
Regarding the multidisciplinary rehabilitation team, the Task Force emphasizes the importance of including healthcare professionals who demonstrate appropriate knowledge and expertise in PD and rehabilitation. Education and training in these areas, along with teamwork and coordination of care, are areas for continued growth opportunities. Considerable debate remains as to the optimal organization and management of rehabilitation care models and their effects in PD. For example, questions remain regarding the optimal combination(s) of rehabilitation professionals, outcome measures, and practice settings, among other aspects. In addition, the timing and regularity of assessments and interventions, as well as their “dose” or intensity, are not fully elucidated. In one model, called the secondary prevention or “dental” model in PT as proposed by Ellis and colleagues, a person with PD consults with a PT with PD-related expertise at the point of diagnosis but since the mode and intensity of exercise and PT requires adaptation to the individual’s needs as PD symptoms change over time, patients are recommended to have regular visits with the PT every 6 months or annually, much like dental care [207]. These topics represent areas for future research and consensus statements.
The Task Force consensus statements on optimal rehabilitation assessments and interventions for OT, PT, SLP, and psychology/neuropsychology complement a recent 2022 World Health Organization (WHO) report of workable avenues for action regarding the global burden of PD [212]. Specifically, the WHO report highlighted the need for inclusive rehabilitative treatments tailored to the individual and unique needs of the person with PD, for increased advocacy and awareness for all health care workers involved in PD care including neurologists, non-neurologist physicians, and allied health team members, and for greater physical activity throughout the course of PD along with the importance of the caregiver role. This further supports the need to accelerate multi-disciplinary research, in line with the key recommendations of the Task Force consensus statement.
Strengths of the Task Force consensus statement include the large international, multidisciplinary group of experts in PD and rehabilitation, use of systematized methodology, and active engagement of individuals with first-hand personal experience as integral Task Force members. In addition, the proposed discipline-specific assessments and interventions may be used in combination with previously developed mono-disciplinary guidelines, thereby expanding rehabilitative care opportunities in PD [11, 96]. Limitations include that due to our scope of work, the Task Force did not focus on other elements of rehabilitative care, e.g., its theoretical basis, temporal applicability, dosing schedules, and intervention combinations, though future research may address. We emphasized rehabilitation therapies (i.e., OT, PT, SLP, and psychology/neuropsychology) that are most commonly utilized, recommended, or available, even though these remain under-utilized in PD treatment; however, future recommendations could incorporate additional disciplines working in rehabilitation, such as case managers, dieticians, nurses, orthotists, social workers, physiatrists, among others. To date, available guidelines on rehabilitation in PD do not include many rehabilitation team members beyond OT, PT and SLP or reflect a variety of comprehensive care settings. While the task force composition represented 7 countries and different healthcare systems, future work may incorporate additional countries and regions to enhance knowledge sharing and greater generalization. Our inclusion of people with lived experience of PD as equal stakeholders in the Task Force represents an important advance towards person-centered care [60, 61], but we acknowledge that including even greater numbers of voices and perspectives from people with PD and care partners would be informative. Future studies are needed to address optimal ways to deliver rehabilitative care and measure its effects of clinical symptoms, disease progression, and underlying neurobiological aspects of PD. Lastly, our overall approach was based on a systematic and iterative process involving a collaborative process with group participation and feedback. As such, the group members’ identities were known to each other, and the statements were crafted with group contributions, iterative feedback, and refinement in our discussions. We employed safeguards, however, to minimize bias, groupthink, and unbalanced group dynamics with the oversight of the Steering committee and third-party healthcare consultants. Moreover, given the vast background and experience of the Task Force in the field of rehabilitation which emphasizes multidisciplinary collaboration and teamwork, this type of group and teamwork flowed naturally to allow all members to participate openly. We acknowledge that the lack of a formal Delphi process may be a methodological limitation, though also recognize that literature supports various adaptations and reporting of Delphi methods [35, 213–215].
In conclusion, rehabilitative interventions are critical in the complete treatment of PD, along with medical, surgical, and other PD-related interventions. It is hoped this consensus statement will raise awareness of the importance of multidisciplinary rehabilitation in PD and motivate professionals to include evidence-based rehabilitation interventions in their multidisciplinary care of persons with PD.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the Avalere Health team (Michelle Bruno, Starr Webb, and Mallory Yung) for their helpful guidance and facilitation of the Task Force consensus procedures and their assistance editing the manuscript. The authors also thank the following external manuscript reviewers for their valuable input and contributions: Stanley Fahn, MD (USA), Genko Oyama, MD (Japan), Meg Morris, PT (Australia), Ingrid Sturkenboom, OT (Netherlands), Lindsey Heidrick, SLP (USA), Rob Skelly, MD (United Kingdom), Lisa Cone, Parkinson’s advocate (USA).
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
All Task Force members received honorarium from the Parkinson’s Foundation for their participation in the Task Force initiative unless noted.
Dr. Goldman has received grant/research support from Acadia Pharmaceuticals, American Parkinson’s Disease Foundation, Lewy Body Dementia Association, Michael J. Fox Foundation, and Parkinson’s Foundation; she has received honoraria from the International Parkinson and Movement Disorder Society and Parkinson’s Foundation.
Dr. Ellis receives funding paid to Boston University from NIH and NSF to support research. She also receives funding paid to Boston University from Parkinson’s Foundation and the American Parkinson Disease Association to support education and outreach activities. Dr. Ellis participates on various committees for the Parkinson’s Foundation, American Parkinson Disease Association, and the Michael J. Fox Foundation, and the Movement Disorder Society; all roles are unpaid.
Dr. Hirsch receives grant and other funding paid to Wake Forest School of Medicine including from: Wake Forest Clinical and Translational Science Institute, Dutch Brain Foundation, and Dutch Parkinson Patient Association. He is a board member on the Scientific Program Planning Board of the International Association of Parkinsonism and Related Disorders, and on the Editorial Board of the Journal of Parkinsonism and Related Disorders. He is also a member of the advisory board of the Parkinson Association of the Carolinas; this role is unpaid. Dr. Hirsch declined honorarium for the Task Force initiative.
Ms. Johnson received honoraria from the Parkinson’s Foundation.
Dr. Biundo has received honoraria from Bial Pharmaceuticals. She is supported by the Ministry of Health under grant number GR-2016-02361986.
Ms. St. Clair received honoraria from the Parkinson’s Foundation.
Dr. York serves on the Michael J. Fox Foundation steering committee Registry for the Advancement of Deep Brain Stimulation in Parkinson’s Disease.
Todaro, Yarab, and Wallock – Parkinson’s Foundation, NY
All other authors have no conflict of interest to report.
DATA AVAILABILITY
Data supporting this study are available from the corresponding author upon reasonable request.