
Abstract
Background:
Positive personality resources have demonstrated the ability to positively impact health outcomes.
Objective:
To examine the psychometric properties of the original Psychological Capital Questionnaire (PCQ-24) in patients with Parkinson’s disease (PD).
Methods:
A sample of 114 individuals with PD completed the PCQ-24, and via a latent factor modeling framework exploratory and confirmatory factor analyses were conducted to evaluate the psychometric properties in people with PD.
Results:
Exploratory factor analysis (EFA) revealed that both the efficacy and hope scales were reliable (Cronbach’s alpha = 0.87 and 0.86, respectively) and had statistically acceptable validity with strong factor loadings all above the practical threshold of 0.60. The resilience and optimism scales were also reliable (Cronbach’s alpha = 0.78 and 0.73, respectively) but had only moderately acceptable validity in part due to three reverse-scored items (i.e., No. 13, 20, & 23) with weak factor loadings of 0.26, 0.46, and 0.50, respectively. After excluding these at-risk items, the overall factor loadings for resilience and optimism were significantly improved at the acceptable above 0.60. The CFA results confirm a statistically acceptable model fit for the modified version (only 21-items) of the PCQ in the PD sample.
Conclusion:
Both EFA and CFA analyses provide statistical evidence supporting the modified PCQ version and demonstrate better test validity and reliability for the PD population. The refined PCQ form is both effectively shorter and psychometrically superior to the original and has promise in investigating health outcomes in people with PD.
Keywords
INTRODUCTION
Despite the historical focus on the motor features of PD, an increased focus on the myriad non-motor features (e.g., depression, urogenital dysfunction, constipation, rapid eye movement sleep behavior disorder) has led to an understanding of the significant contributing role they play in individual functioning and health-related quality of life [1–3]. Although a surfeit of literature exists examining the relationships between disease-related variables and outcomes among people with PD, research assessing the salubrious effects of psychological resources e.g., hope, optimism, resilience, and self-efficacy, on a number of important health outcomes is accumulating [4] and may hold promise for individuals with PD.
Social psychologists have long emphasized the role of individual psychological resources in influencing positive health outcomes [5, 6]. Psychological resources may be understood as individual factors of positive psychological functioning that contribute to health outcomes and how individuals deal with challenging life events [7]. A robust corpus of literature supports the association between psychological resources and mental and physical health outcomes [8–15]. A number of health behaviors, e.g., exercise, sleep, medication adherence, and spirituality, are critical to positive outcomes for people with PD, and evidence supports the role of positive psychological resources in supporting these health-promoting behaviors [15, 16].
Positive psychological capital (PsyCap) is a framework for understanding the psychological resources that individuals use to deal with hardships in their lives and to even thrive despite them. In an attempt to directly identify and ultimately quantify specific positive psychological resources, the hierarchical construct of PsyCap was introduced to represent individuals’ positive psychological state of development [17]. PsyCap is the amalgamation of four psychological resources that were known to positively affect outcomes and determined to be both state-like and malleable, i.e., hope, (self-)efficacy, resilience, and optimism [18, 19] and can be defined as
. . . an individual’s positive psychological state of development and is characterized by: (1) having confidence (self-efficacy) to take on and put in the necessary effort to succeed at challenging tasks; (2) making a positive attribution (optimism) about succeeding now and in the future; (3) persevering toward goals and, when necessary, redirecting paths to goals (hope); and (4) when beset by problems and adversity, sustaining and bouncing back and even beyond (resilience) to attain success [17].
PsyCap emphasizes capitalizing on one’s strengths and virtues rather than negative dispositional and behavioral tendencies and developing those strengths to achieve desired behaviors and emotions [19]. The four components of PsyCap have been demonstrated to be conceptually and psychometrically distinct; however, they share evidence of convergent validity and, when combined, give rise to a psychological resource that is synergistically greater than any of the individual components alone [20]. The concept of synergy, a higher-order factor being more than the sum of its distinct components, is not novel; it can be found, for instance, in the idea of “resource caravans” [21] where similar psychological characteristics exist not in isolation but, rather, aggregate and interact synergistically. Empirical evidence exists supporting the higher order status of PsyCap [22–25], and confirmatory factor analytic validation suggests high correlations (0.6 to 0.7) among the individual components demonstrating convergent validity and support for PsyCap as a higher-order latent factor [25].
Evidence regarding the reliable and valid measurement of PsyCap when altered to fit subjects with chronic illnesses and disabilities is critical in determining whether it is a feasible construct of interest. Although positivity has been demonstrated to result in favorable outcomes, PsyCap requires evidence-based answers on the specific outcomes among clearly defined populations. To date, PsyCap research has largely focused on job performance, satisfaction with work and life, relationship quality, with nascent efforts to assess its role in physical health [23, 26–29]. The common thread running through PsyCap is “one’s positive appraisal of circumstances and probability for success based on motivated effort and perseverance” [17]. The evidence for PsyCap is consistent with the preponderance of support for the effects of positive psychological resources on multiple life domains, which is contrary to the conventional belief that success and favorable outcomes precede positivity [30].
Individuals with PD likely require additional supports to function optimally and fully participate in life, and one of the most useful ways to provide this support is a strengths-based approach that focuses on promoting positive traits [31]. This approach is consistent with the paradigm shift that occurred moving the field of rehabilitation from a deficit-based model to a strengths-based approach (i.e., positive psychology). Accordingly, researchers and clinicians have increased the focus on positive psychological resources and the role they play in desirable outcomes, and the core constructs of PsyCap, in particular, are frequently touted as protective factors in a strengths-based approach [32]. In light of the potential utility of using PsyCap to predict favorable outcomes for people with chronic illnesses, we sought to validate the PCQ-24 in a sample of individuals with PD.
METHODS
Participants and procedures
Participants for this study were a purposive sample of 114 adults with a self-reported diagnosis of PD recruited through peer-lead PD support groups in a mid-western state between January 2018 and March 2018. Paper surveys were made available at weekly group meetings for all interested participants, and completed surveys were gathered by a group member (to maintain anonymity) and returned to the lead investigator. Participants were informed that survey completion counted as consent for de-identified and aggregated data to be used in analysis and reporting. This study protocol (#44405) was approved on 4/17/2018 by the University of Kentucky, Office of Research Integrity Institutional Review Board. Following institutional IRB approval, the lead investigator attended support groups to deliver hard copies of surveys. There were 175 potential participants; of these, 114 completed the survey resulting in a response rate of 65.1%. The response rate could be indicative of the increased risk of cognitive deficits among people with PD who may have been unable to complete the survey. The inclusion criteria were: (a) age > 18 years old and (b) have a self-reported diagnosis of PD.
The sample (n = 114) was 67.5%male and disproportionately Caucasian (96.5%). The mean age of participants was 68.8 years old (SD = 8.3). Most of the sample reported being married (80.7%) and having attended some level of post-secondary education (77.2%), and the median household income was about $62,500. Sample characteristics are described in Table 1.
Participant Demographics
The average age is 68.8 (SD = 8.3); the average age at first signs PD is 61.2 (SD = 9.1); and the average age at diagnosis of PD is 63.3 (SD = 8.7).
The PCQ for individuals with PD was examined and improved in two stages. At the first stage, psychometric evaluation of reliability (Cronbach’s alpha) and validity (EFA) were performed, to determine whether the PCQ instrument might be acceptable for use with people with PD. Next, the selected PCQ items were re-assessed through CFA to ensure that the modified PCQ is working appropriately for the PD population. For the standards of psychometric evaluation, Cronbach’s alpha provides an index of the internal consistency reliability of items in a scale, and the general assumption is that higher coefficients (i.e., > 0.7) indicate better consistency (or good reliability) of a measure. Further, all 24 items of the PCQ scale are evaluated through EFA and CFA. With a latent factor modeling framework, EFA is to examine the appropriateness of each item by testing whether the factor loading is met as the satisfactory level (i.e., item factor loading ≥0.6), plus whether any tested factor is equipped with an eigenvalue of ≥1.0 (i.e., statistical importance); and CFA is to test the overall goodness fit of the modified PCQ through a latent factor modeling procedure for statistical model validation.
Measures
The Psychological Capital Questionnaire (PCQ-24) [17] is a 24-item, self-report instrument designed to measure each of the individual first-order factors of PsyCap as well as the higher-order PsyCap construct. The basis for the development of the PCQ-24 is: (a) hope [33]; (b) resilience [34]; (c) optimism [11]; and (d) self-efficacy [35]. Although the PCQ has undergone extensive validity analysis [25], it is specific to a work domain and, therefore, the specific wording had to be adapted to a health domain. Care was taken to keep the original questions as unaltered as possible. This 24-item, self-report questionnaire consists of a 6-point Likert scale (1 = strongly disagree to 6 = strongly agree) and has 6-item subscales designed to measure each of the four psychological constructs of PsyCap (i.e., hope, efficacy, optimism, and resilience). Representative items include the following: “I feel confident setting targets/goals for my health” (efficacy); “I can think of many ways to reach my current health goals” (hope); “When I have a health setback, I have trouble recovering from it and moving on” (resilience); and “I approach my health as if ‘every cloud has a silver lining”’ (optimism).
Data analysis
Statistical analyses were conducted via IBM SPSS Version 26 (2019) for data preparation and management as well as basic psychometric assessment of reliability (Cronbach’s alphas) and validity (factor models with principal component analysis) [36] and Mplus Version 8.1 [37] for latent factor modeling on EFA (by a four-dimensional latent structure for all 24 items) and CFA (via the proposed latent factors with selected and retained items). All statistical tests for parameter estimates were performed at a 0.05 level of significance. The cutoff criteria for CFA were based on the following rules of thumb [37–39]: (a) Lower Bound of 90 Percent Root Mean Square Error of Approximation (RMSEA) ≤0.05; (b) Standard Root Mean-Square Residual (SRMR) < 0.08; (c) Comparative Fit Index (CFI) > 0.90; (d) Tucker-Lewis Index (TLI) > 0.90; and (e) Hoelter’s Critical N (CN) < Studied Sample Size.
RESULTS
Exploratory factor analysis
Theoretically, PsyCap was multidimensionally measured using four validated constructs of HERO [17]. In this study, all of the 24 items used for mapping on the overall PsyCap were re-assessed with the studied PD sample. A sequential analysis for the reliability (Cronbach’s coefficient alpha) and validity (item factor extraction by projected principal components via EFA) assessments was completed as follows (also refer to Table 2).
Exploratory factor analysis for all 24 items of the Within HERO scales
*represents a reverse worded item.
First, adequate internal consistency for the Efficacy scale (items 1–6) was established (Cronbach’s α= 0.86), and the validity was statistically acceptable (eigenvalue = 3.96) as item factor loadings lay within a range from 0.60 to 0.89 (above the practical threshold of 0.6). Second, the Hope scale (items 7–12) was also found to have adequate internal consistency (Cronbach’s α= 0.87), and the validity was also statistically acceptable (eigenvalue = 3.72) since item factor loadings were within a range from 0.61 to 0.82. Third, the Resilience scale (items 13–18) had acceptable internal consistency (Cronbach’s α= 0.78) and moderately acceptable validity (eigenvalue = 2.71) because, except for the reversed item (item 13; factor loading = 0.26), all other item factor loadings were within a range from 0.66 to 0.79. Fourth, for the Optimism scale (items 19–24), was also found to have acceptable internal consistency (Cronbach’s α= 0.73), and the validity was also moderately acceptable (eigenvalue = 3.06) because, except for the reversed items (for items 20 & 23, the factor loadings were 0.46 and 0.50, respectively), all the rest of item factor loadings lay within a range from 0.71 to 0.88.
The factor loadings for all the three reverse-scored items were below the established acceptable threshold (i.e., 0.6), suggesting that these items may not contribute sufficient statistical information to the designated factor (or latent construct principal component) in the present PD sample. The three reversed items were therefore excluded to improve the model fits (latent measurements on Resilience and Optimism) as well as the interpretability (factor loading effect sizes) of the relationship between observed responses and latent scores in exploratory latent factor models [40].
After omitting the three reversed items (item 13 on the Resilience scale and items 20 & 23 on the Optimism scale), the results of the EFA for the modified Resilience and Optimism were as follow (see also Table 3)
Exploratory factor analysis for the modified Resilience and Optimism scales
*represents a reverse worded item.
For the five items remaining in the modified Resi-lience scale, the Cronbach’s α= 0.77 and the validity was still acceptable (eigenvalue = 2.62), with the item factor loadings ranging from 0.68 to 0.79. For the four items remaining in the modified Optimism scale, the Cronbach’s α= 0.85, and the validity was acceptable (eigenvalue = 2.81) with the adjusted factor loadings ranging from 0.70 to 0.91.
After excluding the three reversed items with low loadings, the modified EFA for both Resilience and Optimism were found to be more appropriate measurements (better overall loadings) for the PD sample. The modified EFA also suggests that, due to the high frequency of cognitive impairment among those with PD, items with reversed-scored wording may create potential risks and threats to internal validity and reliability due to item ineffectiveness and acquiescence response bias or agreement [41, 42].
Confirmatory factor analysis
To study the proposed latent modeling structure of HERO (modification to exclude the three reversed items) of the PCQ for the vulnerable PD population, CFA with latent variable modeling framework was conducted to examine the modified latent constructs. Note that in the modified latent factor model, the reversed items were omitted and not linked with the original four HERO constructs as well as the collective PsyCap factor (see Fig. 1 as an illustration of the proposed CFA model with modifications). The CFA results show a statistically acceptable model fit for the modified version of the PCQ on the PD sample. The statistical summary includes: (a) Lower Bound of 90%RMSEA = [0.05,0.08]≤0.05; (b) SRMR = 0.07 < 0.08; (c) CFI = 0.95 > 0.90; (d) TLI = 0.93 > 0.90; and (e) CN = 90 < 114 (i.e., sample size of the study). The final CFA model suggests that the modified PCQ would be able to provide a better model fit than the original version of the PCQ (including all 24 items), and that the reversed-score items should be omitted when the PCQ is administrated to a vulnerable population with cognitive challenges such as people PD so that the psychometric properties of test validity and reliability on the PCQ items as well as HERO constructs would remain intact. Both EFA and CFA analyses provide evidence supporting the modified PCQ version and demonstrate better test validity and reliability in the PD population. The refined PCQ form, excluding three reverse worded items) is both effectively shorter and psychometrically superior to the original.
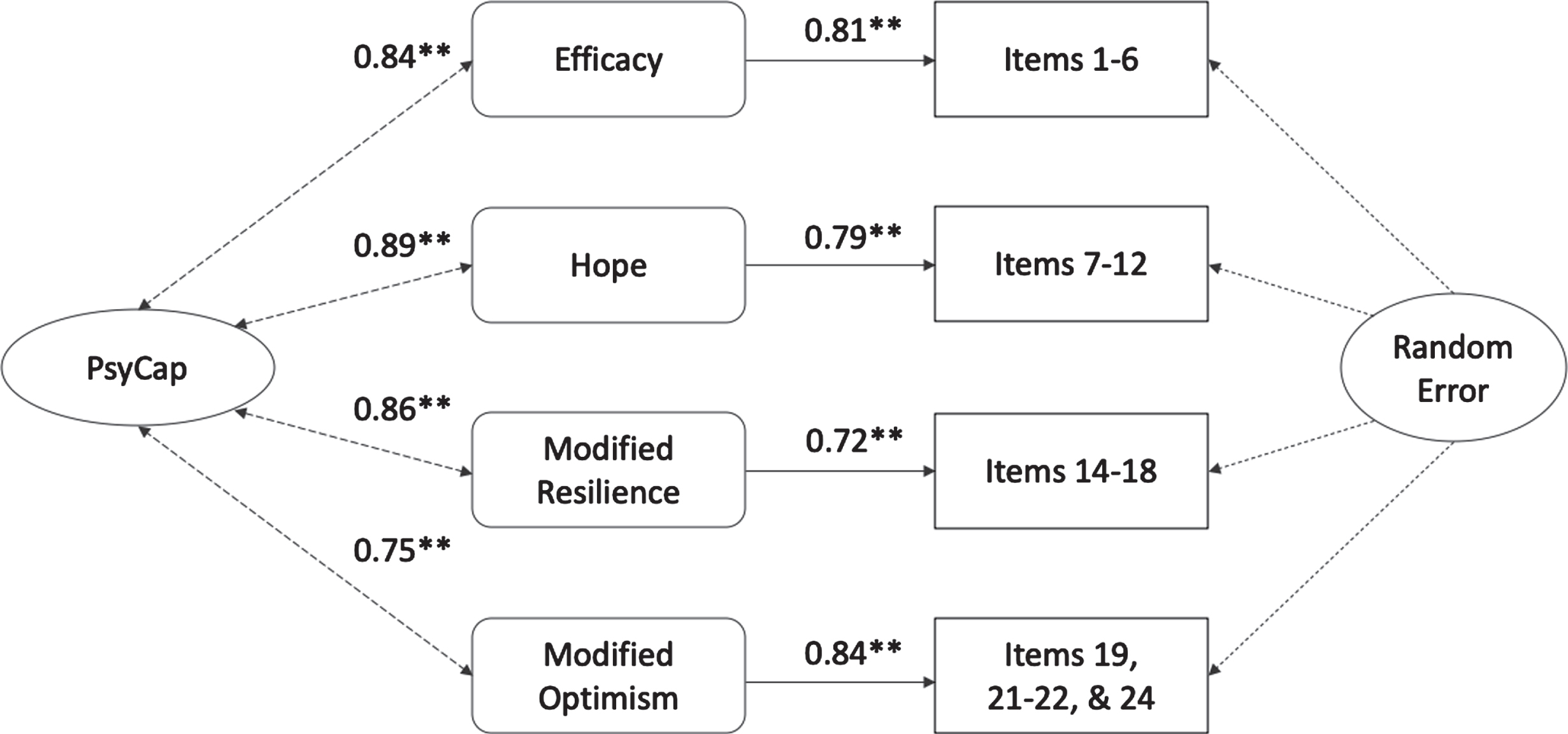
Path Diagram for the Proposed CFA Model **p ≤0.05.
DISCUSSION
To date, a number of studies have suggested that work-related PsyCap is positively correlated with health and well-being [26, 43–45]; however, providing support for validation of measures in people with chronic illnesses is needed. This is the first study to evaluate the psychometric properties of the PCQ-24 in a sample of adults with PD and provides support for the construct and its potential usefulness in this population. As hypothesized, we observed strong support for Luthans et al.’s [17] PCQ-24 general population model in which the four latent factors of HERO load on the higher-order PsyCap factor resulting in a good overall fit. Following the elimination of the problematic, reverse-scored items with low loadings, however, the data demonstrates superior validity and reliability of the modified instrument compared to the original.
Each of the individual scales for HERO demonstrated acceptable internal consistency based on the Cronbach’s alphas (0.87, 0.86, 0,78, and 0.73, respectively) and statistical validity derived from the individual eigenvalues (3.72, 3.96, 2.71, and 3.06, respectively). Additionally, with the exception of the reverse scored items (i.e., No. 13, 20, & 23), the factor loadings for each of the items in the individual HERO measures support the overall validity of the PsyCap factor. The original psychometric information for the PCQ-24 is demonstrated in Table 4 for comparison.
Original psychometric information for all 24 items of the Within HERO scales
The statistical information (n = 404) is retrieved from Luthans et al. (2007).
Due to the high likelihood of having cognitive decline associated with PD, the reverse-scored items were eliminated resulting in acceptable psychometric properties. Utilizing both positively and negatively worded items in surveys has been used for decades in an attempt to prevent or reduce response bias (e.g., acquiescence bias) [41]. However, experts have also long advised against using reverse-scored items because such questions appear to negatively affect the dimensionality of the scale [46]. Moreover, positively and negatively valanced items should not be combined in instruments because reliability can be flawed, and the dimensionality of the scale may be compromised by secondary sources of variance [47]. More specifically, due to the decrease in cognitive flexibility and perseveration among people with PD, including reverse-scored items is likely to be problematic for appropriate interpretation [48].
Many studies have demonstrated the benefits of PsyCap on well-being in different contexts of life and work. Specifically, PsyCap appears to be a robust predictor of satisfaction with the domains of work, relationships, and health [27] and correlates positively with increased commitment and well-being [43, 49] and negatively with stress and anxiety [50].
For decades, rehabilitation professionals have encouraged people with chronic illnesses and disabi-lities to focus on the positively valanced character strengths to facilitate positive outcomes [51]. Re-search examining the role of hope, optimism, resilience, and efficacy in psychosocial adaptation and favorable health abounds [52–58]. Having a psychometrically sound instrument to not only evaluate the presence of each of these state-like psychological resources but to also provide a synergistic, higher-order construct holds practical promise for identifying its role in positive health outcomes for people with PD.
Limitations
The sample for this investigation was not representative of the U.S. population, with a limited number of racial and ethnic minorities. Most participants were Caucasian and well-educated, which may preclude generalizing to disparate populations. Second, a cross-sectional purposive sample was used in this study, and participants were recruited from a PD support group, which may have led to bias because those who attend support groups may already have the resources needed to manage their PD. Although this potential confounder is reasonable, there is also the possibility that those who choose to attend a support are lacking necessary psychological resources and are actively pursuing solutions. Third, the study relied exclusively on self-report measures obtained through surveys, which have been criticized for being potentially biased; however, recent literature indicates that, specifically among patients with PD, the accuracy of information provided correlates highly with clinician diagnosis [59, 60]. Despite a plethora of literature validating instruments with relatively small samples, this study was fairly small and further evaluation of the PCQ in a larger, more diverse sample would be advised.
Despite these limitations, the current study contributes to the understanding of the adequate psycho-metric performance of the PCQ instrument in people with PD. It provides support for the psychometric properties of a novel measure to evaluate individuals’ positive psychological resources and may be the impetus for future research assessing the role in positive health outcomes in people with PD. Future research should evaluate the extent to which these findings generalize to a more representative population and explore practical utility among people with PD.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.