
Abstract
Background:
Individuals with Parkinson’s disease (PD) may be especially vulnerable to future cognitive decline from anticholinergic medications.
Objective:
To characterize anticholinergic medication burden, determine the co-occurrence of anticholinergic and cholinesterase inhibitors, and to assess the correlations among anticholinergic burden scales in PD outpatients.
Methods:
We studied 670 PD outpatients enrolled in a clinic registry between 2012 and 2020. Anticholinergic burden was measured with the Anticholinergic Cognitive Burden Scale (ACB), Anticholinergic Drug Scale (ADS), Anticholinergic Risk Scale (ARS), and Drug Burden Index-Anticholinergic component (DBI-Ach). Correlations between scales were assessed with weighted kappa coefficients.
Results:
Between 31.5 to 46.3% of PD patients were taking medications with anticholinergic properties. Among the scales applied, the ACB produced the highest prevalence of medications with anticholinergic properties (46.3%). Considering only medications with definite anticholinergic activity (scores of 2 or 3 on ACB, ADS, or ARS), the most common anticholinergic drug classes were antiparkinsonian (8.2%), antipsychotic (6.4%), and urological (3.3%) medications. Cholinesterase inhibitors and medications with anticholinergic properties were co-prescribed to 5.4% of the total cohort. The most highly correlated scales were ACB and ADS (κ= 0.71), ACB and ARS (κ= 0.67), and ADS and ARS (κ= 0.55).
Conclusion:
A high proportion of PD patients (20%) were either taking antiparkinsonian, urological, or antipsychotic anticholinergic medications or were co-prescribed anticholinergic medications and cholinesterase inhibitors. By virtue of its detection of a high prevalence of anticholinergic medication usage and its high correlation with other scales, our data support use of the ACB scale to assess anticholinergic burden in PD patients.
Keywords
INTRODUCTION
Anticholinergic medication usage in mid-life has been associated with an increased risk of future dementia [1–7], falls [8, 9], mortality [10], and frailty [11]. In a smaller number of studies, anticholinergic medication usage has also been found to increase the risk of future dementia in Parkinson’s disease (PD) [12–15]. Individuals with PD may be especially vulnerable to the negative effects of anticholinergics. First, prior studies report an especially high prevalence of anticholinergic medication usage in PD [16–18]. This includes both anticholinergic medications used to treat parkinsonism and tremor and anticholinergic medications prescribed for other indications. Second, because degeneration of the cholinergic basal forebrain is a common characteristic feature of PD [19–22], anticholinergic medications are likely to exacerbate underlying cholinergic deficiency. Prior studies have identified co-prescription of cholinesterase inhibitors and anticholinergic medications, drugs with opposing pharmacological effects, as common in PD [23].
Based on the negative long-term effects of anticholinergic medications, PD patients taking these medications are potential candidates for deprescribing interventions. Thus, it would be valuable to identify a reliable and relatively simple means for clinicians to monitor anticholinergic burden in their PD patients. It is also important to assess outpatient medication anticholinergic burden in PD as most PD care is in the outpatient setting. Prior studies assessing anticholinergic burden in PD have studied inpatient, mixed inpatient and outpatient cohorts, or smaller outpatient cohorts [13, 24–27]. We evaluated anticholinergic medication usage in a large, exclusively outpatient cohort.
Currently, there is no standard measure to characterize anticholinergic burden in PD. Prior studies assessing prevalence of anticholinergic burden in PD have variably applied the Anticholinergic Cognitive Burden Scale (ACB) [16, 27], the Anticholinergic Drug Scale (ADS) [16, 24], and the Anticholinergic Risk Scale (ARS) [16, 26]. Studies showing a relationship between anticholinergic medication use and risk of developing dementia in PD used either the ACB [15], a categorical measure of serum anticholinergic activity [13] or no scale at all [12, 14].
On this background, the objectives of this study were 1) to determine the prevalence and characteristics of anticholinergic medication burden in an outpatient cohort of PD patients, 2) to determine the co-occurrence of anticholinergic and cholinesterase inhibitors, and 3) to assess the correlations among scales commonly used to measure anticholinergic burden in this population. Consistent with the current PD literature and recommendations from the non-PD literature [28], we chose to apply the ACB, ADS, and ARS to assess anticholinergic medication burden. We additionally applied the Drug Burden Index-Anticholinergic component (DBI-Ach), which uniquely accounts for drug dosage [29].
METHODS
Study participants
This study included all PD patients from the clinic registry of the Parkinson’s and Movement Disorders Center at Virginia Commonwealth University (VCU) enrolled between 2012 and August 1, 2020. Patients in the registry were seen by movement disorder specialists and provided consent for their clinical data to be collected and used for the purposes of research. This specific study was approved by the Human Research Protection Program/Institutional Review Board at VCU.
Demographic data were obtained from the clinic registry, including patient’s age at PD diagnosis, age at last outpatient encounter, gender, race/ethnicity, and medication usage data. Based on the available data, duration of PD was assigned as the time between the year of diagnosis and the year of last outpatient visit. For this study, we analyzed the medications that coincided with the last outpatient encounter in the neurology clinic. Medication information included drug names and dosages. The number of scheduled (not p.r.n.), oral medications, including over the counter medications, were summed to determine the total number of medications. In addition to analyzing medications with anticholinergic properties, we also determined whether patients were concurrently prescribed one of the three cholinesterase inhibitors used in PD patients to treat cognitive dysfunction: donepezil, rivastigmine, or galantamine.
Anticholinergic exposure
Total anticholinergic medication burden for each patient was calculated using the ACB, ADS, ARS, and DBI-Ach. These scales use different criteria to determine which medications are included, and further, use different scoring criteria. For each scale, a total score is determined by summing each medication’s individual score. Medications designated as p.r.n. (as needed) were excluded. We also excluded topical, ophthalmic, otologic, sublingual, inhaled, and intramuscular medication preparations.
The ACB, published in 2008, is a widely used scale for estimating anticholinergic burden and its association with cognitive impairment [30]. It was developed in response to a comprehensive literature review of anticholinergic drugs and their association with dementia and cognitive impairment. The ACB scale assigns scores (0 to 3) to medications based on their affinity for muscarinic receptors and their effect on cognition. A score of 1 indicates affinity to muscarinic receptors but no clinically relevant established cognitive effects. Scores of 2 indicate mild and 3 indicate more severe established adverse cognitive effects.
The ADS ranks anticholinergic drugs based on adverse effects and was published in 2006 using serum anticholinergic activity (SAA) [31]. Drugs are assigned scores (0 to 3), with 1 indicating potential anticholinergic activity based on SAA, 2 indicating anticholinergic properties sometimes leading to adverse effects, usually at high doses, and 3 indicating marked anticholinergic activity.
The ARS, published in 2008 [32], ranks a list of commonly prescribed medications with anticholinergic activity. For its development, 500 medications were initially studied and weighted based on in vitro dissociation from cholinergic receptors. Medications are ranked on a scale of 0 to 3 representing anticholinergic potential with 0 indicating limited or none, 1 indicating moderate, 2 indicating strong, and 3 indicating very strong. The ARS was found to reliably estimate the association of use of anticholinergic medications with central adverse effects [32]. Unique to the ARS, carbidopa-levodopa is assigned a score of 1. As carbidopa-levodopa is eventually prescribed to most PD patients and is not listed in the other scales, it was not included in the calculation of anticholinergic burden.
The Drug Burden Index (DBI), published in 2007, incorporates medication dose to calculate burden of medications with anticholinergic and sedative effects [33]. The DBI-Ach is calculated with the following formula in which D is daily dose and δ is the recommended minimum daily dose approved by the US FDA: DBI-ACh =∑ [D/(D +δ)]).
Statistical analysis
For comparing ACB, ADS, and ARS, the scores for anticholinergic medications were summed for each patient and this measure of total anticholinergic burden was divided into 5 categories: 0, 1, 2, 3, and 4 + . For the purpose of comparing ACB, ADS, and ARS to DBI-Ach, total anticholinergic burden was divided into three categories: absent, low, or high. For the ACB, ADS, and ARS, total anticholinergic burden was categorized as follows: 0 indicated absent burden; 1–2 indicated low burden; and ≥3 indicated high burden. For DBI-Ach, total anticholinergic burden was divided into the following categories: 0 indicated no burden; 0–1 indicated low burden; and ≥1 indicated high burden [34]. Correlations among anticholinergic burden scales were estimated using weighted (linear and quadratic) kappa statistics [35], which have both been used by prior studies. Because quadratic weighting penalizes greater deviations more than mild deviations, correlation coefficients from the quadratic weighted kappa were considered as the primary outcome. Because the ACB was the most highly correlated with other scales, Pearson correlation coefficients were calculated to explore the relationships between duration of disease and ACB total score and duration of disease and total number of medications. Statistical significance was set at p < 0.05. Statistical analysis was performed using StataIC14 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP).
RESULTS
Demographic and medication usage characteristics of the cohort are presented in Table 1. Participants were 60.3% men, had a mean age of 71.4 years (SD = 9.2 years), and had a mean disease duration since diagnosis of 7.4 years (SD = 5.3 years). Median number of total scheduled, oral medications (anticholinergic and not anticholinergic) was 7 per participant (I.Q. range = 5–10). Duration of PD was not associated with the total number of medications (r = 0.002, p = 0.97) nor with the total ACB score (r = 0.07, p = 0.09).
Demographic characteristics of study population
IQR, interquartile range; SD, standard deviation.
For the ACB, 53.5% (53/99) of medications listed in the scale were represented in the cohort, and the prevalence of anticholinergic medication usage was 46.3%. For the ADS, 43.1% (50/116) of included medications were represented in this cohort, and the prevalence of anticholinergic medication usage was 44.6%. For the ARS, 53.1% (26/49) of medications listed for this scale were represented, and the prevalence of anticholinergic medication usage was 38.8%. For the DBI-Ach, 40.0% (30/75) of medications listed for this scale were represented, and the prevalence of anticholinergic medication usage was 31.5%. The prevalence of the cohort using an anticholinergic medication with score of 2 or 3 was 20.7% for ACB, 10.6% for ADS, and 18.7% for ARS. The number of anticholinergic medications, total score, and highest single anticholinergic medication score for each scale are reported in Table 2.
Number of anticholinergic medications, total anticholinergic burden scale scores, and highest single anticholinergic scores for ACB, ADS, ARS, and DBI-Ach
AC, anticholinergic; ACB, Anticholinergic Cognitive Burden scale; ADS, Anticholinergic Drug Scale; ARS, Anticholinergic Risk Scale; DBI-Ach, Drug Burden Index- anticholinergic component.
Individual anticholinergic medication usage for ACB, ADS, ARS, and DBI-Ach is provided in Supplementary Table 1. We separately considered only anticholinergic medications that were included in 2 of the 4 scales and were considered a 2 or 3 on the ACB, ADS, or ARS. Among these the most commonly represented drug classes in the entire cohort (n = 670) were antiparkinsonian (8.2%), antipsychotic (6.4%), and urological (3.3%) medications; and the most common individual medications were amantadine (6.1%), quetiapine (5.1%), oxybutynin (2.5%), and trihexyphenidyl (1.8%). Cholinesterase inhibitors were prescribed to 10.2% of the study population, and 5.4% (n = 36) of the cohort were prescribed both cholinesterase inhibitors and any medications with anticholinergic properties. Excluding overlap between the groups, 20% (134/670) of the cohort were either prescribed one of the 3 most commonly prescribed anticholinergic drug classes or were co-prescribed anticholinergic medications and cholinesterase inhibitors.
Figure 1 displays the relationships between the total scores of ACB, ADS, and ARS when categorized as 0, 1, 2, 3, or 4 + . Using five categories for each scale, weighted kappa coefficient values for the correlations among ACB, ADS, and ARS are presented in Table 3. The most highly correlated scales were ACB and ADS (κ= 0.71). Using the three categories of absent burden, low burden, and high burden, weighted kappa coefficient values for correlations among ACB, ADS, ARS, and DBI-Ach are presented in Table 4. Again, the most highly correlated scales were ACB and ADS (κ= 0.65).
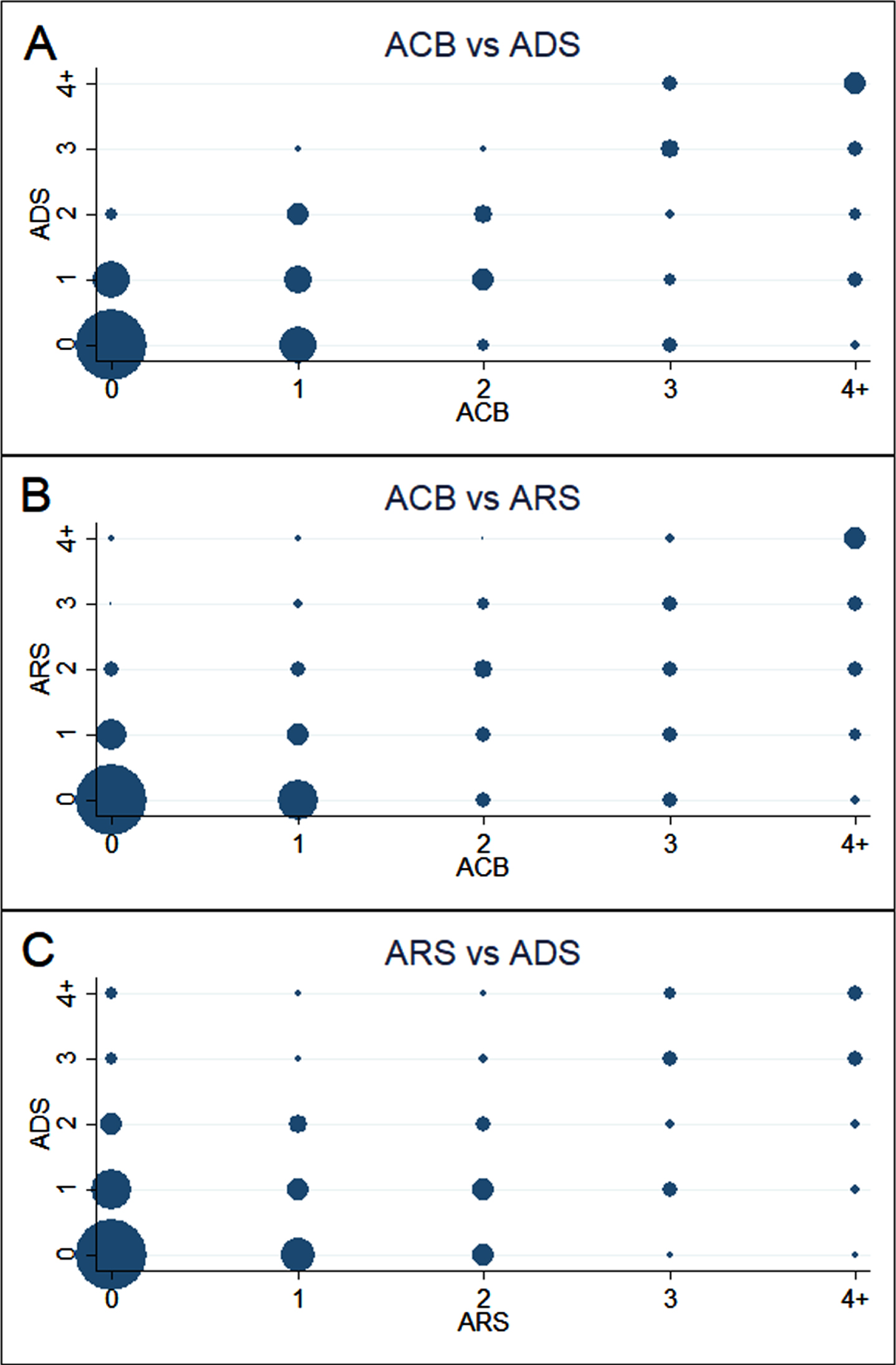
Scatterplots of ACB, ADS, and ARS total scores. These scatterplots display the relationships between the total scores of ACB, ADS, and ARS when categorized as 0, 1, 2, 3, or 4 + . Datapoint size represents the number of study participants for each combination of total scores for the comparison of ACB versus ADS (A), ACB versus ARS (B), and ARS versus ADS (C). ACB, Anticholinergic Cognitive Burden scale; ADS, Anticholinergic Drug Scale; ARS, Anticholinergic Risk Scale.
Weighted Kappa Statistics Comparing total anticholinergic burden (categorized as 0,1,2,3,4+) for ACB, ADS, and ARS
ACB, Anticholinergic Cognitive Burden scale; ADS, Anticholinergic Drug Scale; ARS, Anticholinergic Risk Scale.
Weighted Kappa Statistics Comparing total anticholinergic burden (categorized as absent, low, and high burden) for ACB, ADS, ARS, and DBI-Ach
ACB, Anticholinergic Cognitive Burden scale; ADS, Anticholinergic Drug Scale; ARS, Anticholinergic Risk Scale; DBI-Ach, Drug Burden Index-anticholinergic component.
DISCUSSION
Depending on the anticholinergic burden scale that was applied, we found that 31.5–46.3% of PD outpatients were taking medications with anticholinergic properties. Among the scales we applied, the ACB included the greatest proportion of anticholinergic medications observed in our cohort and provided the highest prevalence of anticholinergic medication usage. Prior studies in non-PD geriatric populations have also found that the ACB produces the highest prevalence of anticholinergic medication usage [8, 35–37]. To evaluate the correlations between scales, we used the weighted kappa statistic with both quadratic [38], and linear [39], weighting as previously applied. Regardless of which weighting is applied, both measures indicate that the ACB and ADS are the most highly correlated, followed by the ACB and ARS. DBI-Ach shows the least correlation with ACB, ADS, and ARS. Prior studies in non-PD populations have also reported that the ACB and ADS are the most highly correlated scales [34, 38]. Considering that the ACB detects the highest prevalence of anticholinergic medication usage and was the most highly correlated with other scales, our data support the ACB scale as an appropriate choice to assess anticholinergic burden in PD patients.
Prior studies in PD reported anticholinergic medication usage rates of 42.6% in 195 patients [24], 43.4% in a prospective cohort of 235 PD patients at baseline [13], 51.4% in an observational research cohort at 5 years [25], and even higher numbers (53.6% [16] and 57% [26]) in PD inpatients. In a cross-sectional database of adverse drug reactions, 58% of PD patients were prescribed medications with anticholinergic properties [18]. One cross-sectional study in PD found a prevalence of 58.4% for individuals with total ACB scores > 3, but this study included carbidopa/levodopa [27]. Potential reasons for the lower prevalence rates in our population include the different compositions of the applied scales, analysis of a lower acuity, outpatient cohort, exclusion of carbidopa/levodopa; and exclusion of all medications that were not orally administered or scheduled.
Disagreement between scales arises from the different medications included in each scale and the score that each medication is assigned. In addition to the ACB, ADS, and ARS, which have been applied in previous PD studies [16, 27], we applied the DBI-Ach in our PD cohort because it incorporates daily dose into its calculation of anticholinergic medication burden. We found that DBI-Ach was the least correlated with the other scales, likely in part because this measure includes a limited number of medications compared to the other scales.
Because anticholinergic medications commonly cause or exacerbate confusion and pose a risk for future dementia and since PD patients may be especially vulnerable, there is a clear need for greater vigilance and deprescribing of anticholinergic medications in PD. This study identifies potential targets for deprescribing. In this cohort, anticholinergic medications used for antiparkinsonian, antipsychotic, and urological indications collectively accounted for 16% of the anticholinergic medications that were prescribed and these classes were prescribed to 17.9% of the total cohort. Amantadine, quetiapine, oxybutynin, and trihexyphenidyl accounted for the majority of this anticholinergic burden. As previously reported in PD [23], our study found a high rate of co-prescribed cholinesterase inhibitors and anticholinergic medications. We found that 10.2% of our cohort were using cholinesterase inhibitors and 53% of those taking cholinesterase inhibitors were also taking anticholinergic medications. The prior study reported cholinesterase use in 23.9%, with 81.3% also using anticholinergic medications. While our prevalence of co-prescribing was lower than the prior study, it still indicates that co-prescribing is common and a potential target for intervention. Using our cohort, a deprescribing intervention targeted at the three most common definite anticholinergic classes and those patients co-prescribed anticholinergic medications and cholinesterase inhibitors would apply to 20% of PD outpatients. However, we recognize that not all anticholinergic medications can be deprescribed as they may be the only reasonable option for certain clinical indications (e.g., amantadine for dyskinesia) for which reasonable alternatives do not exist.
Prior studies have assessed the correlation between anticholinergic burden scales in non-PD populations including older adults and patients with psychiatric illnesses. Our study is the first to assess the correlation among these scales in PD patients. We also present anticholinergic burden in the largest clinical outpatient PD cohort yet reported. A limitation of this study is that it was retrospective and therefore may include errors present in patients’ medical records. Also, our cohort was ascertained from an academic medical center and therefore our findings may not be applicable to all PD patients in the community. Another limitation is that we do not have information about cognitive status or psychotic symptoms which should influence the use of anticholinergic medications in clinical practice. Assessment of cognition and psychotic symptoms should be a priority of any future prospective studies.
As evidence has accumulated about the negative long-term effects of anticholinergic medications, it is important to accurately assess anticholinergic burden and understand contributors to anticholinergic burden in specific patient groups. We provide important information about anticholinergic burden in PD outpatients, the performance of anticholinergic burden scales in PD, and potential targets for anticholinergic deprescribing interventions in an outpatient PD cohort. We found anticholinergic burden to be present in up to half of PD outpatients. Compared to the other scales, ACB identified the greatest number of anticholinergic medications and was the most highly correlated with other scales. Lastly, our study identified potential targets for anticholinergic medication deprescribing, which together, could ultimately influence the care of 1 in 5 PD patients.
Footnotes
ACKNOWLEDGMENTS
This study received support from the C. Kenneth and Dianne Wright Center for Clinical and Translational Research grant (UL1TR002649).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.