
Abstract
Background:
Scalp erosion is not an uncommon complication of deep brain stimulation (DBS) surgery. Although various methods have been proposed to prevent and manage complications, there are still challenges. We introduce a case of recurrent scalp erosion after DBS surgery treated with vacuum-assisted closure.
Case description:
This article reports the case of a patient who underwent DBS for advanced Parkinson’s disease and suffered from recurrent scalp erosion with device extrusion through the skin. Scalp erosion occurred 2 years after DBS and repeated improvement and deterioration despite scalp reconstruction using a skin flap. We opened the wound and performed temporal muscle reconstruction to cover the burr hole site, and we changed the exposed cable and applied vacuum-assisted closure. During the follow-up period, no signs of erosion or infection occurred, and DBS efficacy was preserved.
Conclusion:
To date, the available management strategies for scalp erosion after DBS are revision with debridement and scalp reconstruction using skin flaps or skin grafts. However, if erosion occurs repeatedly despite the above management strategies, vacuum-assisted closure with temporalis muscle reconstruction could be a suitable option. We suggest that if the condition of the scalp is weakened, it is worth considering this approach preferentially.
INTRODUCTION
Deep brain stimulation (DBS) is an effective form of treatment for an increasing number of patients with movement disorders and pain. Even though technological advances have improved the efficacy and safety of this procedure, there may be different hardware-related complications, including lead migration, device malfunction, infection, and skin erosion [1].
Scalp erosion, with the exposure of underlying hardware, can lead to infection and is, in itself, a strong indication for explantation of the neurostimulation system. Erosion of the overlying scalp occurs at points of increased tension between the skin and hardware. The reported incidence of scalp erosion is between 1.4 and 8.3% [2, 3].
A number of methods can be utilized to reconstruct these defects using a variety of alloplastic materials, grafts, and flaps. Despite the many available tools, surgeons are aware that many patients are poor candidates for immediate reconstruction because of the original pathology, the patient’s comorbidities, and the complications associated with each reconstructive technique.
One therapy that has been used over the past decade with increasing frequency in patients with acutely unfavorable soft tissue conditions is vacuum-assisted closure (VAC). The use of VAC for the treatment of tissue defects was first described by Morykwas et al. in 1997 [4]. This therapy has played an expanded role in negative-pressure therapy for complex head and neck wounds. A few case reports have described the successful use of VAC therapy for complex cranial wounds with exposed dura [5, 6].
In the present report, we describe our experience with the use of VAC therapy in a patient with recurrent scalp erosion with device exposure following DBS. To the best of our knowledge, this is the first report of VAC therapy for scalp erosion after DBS.
CASE PRESENTATION
A 74-year-old male with diabetes mellitus (DM) and a 16-year history of Parkinson’s disease underwent bilateral subthalamic nucleus DBS. He experienced relief of dyskinesia symptoms and achieved a drug dose reduction. Two quadripolar electrodes (Medtronic 3389, Minneapolis, MN, USA) were implanted, and a Stimloc™ burr hole cover (Medtronic, Minneapolis, MN, USA) was used to cover the burr hole and secure the electrode.
Two years later, he underwent a DBS cable change due to an increase in the internal pulse generator (IPG) resistance (> 20000), and approximately 2 weeks after the cable change, he scratched the right burr hole site and experienced wound erosion. Because the area of erosion was small (1-2 mm) and there was no sign of infection (culture negative), we managed the erosion conservatively. The erosion repeatedly improved and deteriorated, but eventually, the implant was exposed after 1 year, so he underwent wound revision using a scalp skin flap with a cable change. After 2 weeks, the erosion recurred, and despite conservative management, the implant was exposed again at 6 months after the revision surgery (Fig. 1). Throughout the process, there were no signs of infection, and the patient had a negative opinion about additional surgery for the erosion. Considering that the erosion repeatedly occurred and did not resolve despite revision surgery using a scalp flap, we decided to apply VAC in the next revision surgery.

The preoperative state of the erosion site with the exposed implant (white arrow). There were no signs of infection (discharge, redness, etc.).
SURGICAL APPROACH
Under general anesthesia, a scalp incision was made at the previous incision site. The scalp was observed to be very thin. After dissecting the temporalis muscle fascia and making a muscle flap, we used it to cover the burr hole cover and the proximal portion of the cable (Figs. 2–4). After removing the necrotic tissue, we tried to close the wound, but this required too much tension. Because we judged that the scalp would not stand the tension, we sutured the wound with a slight gap remaining (0.5 cm). After suturing, we applied VAC (Kinetic Concepts, Inc., San Antonio, TX, USA) to the wound (Fig. 5). The pressure on the VAC device was set at – 75 mmHg, and the device was maintained for 5 days. In this period, there were no signs of cerebrospinal fluid leakage. Two weeks after the surgery, the wound had recovered well, and the patient was discharged. Three months after surgery, the wound remained in a good state, and there was no additional erosion (Fig. 6).
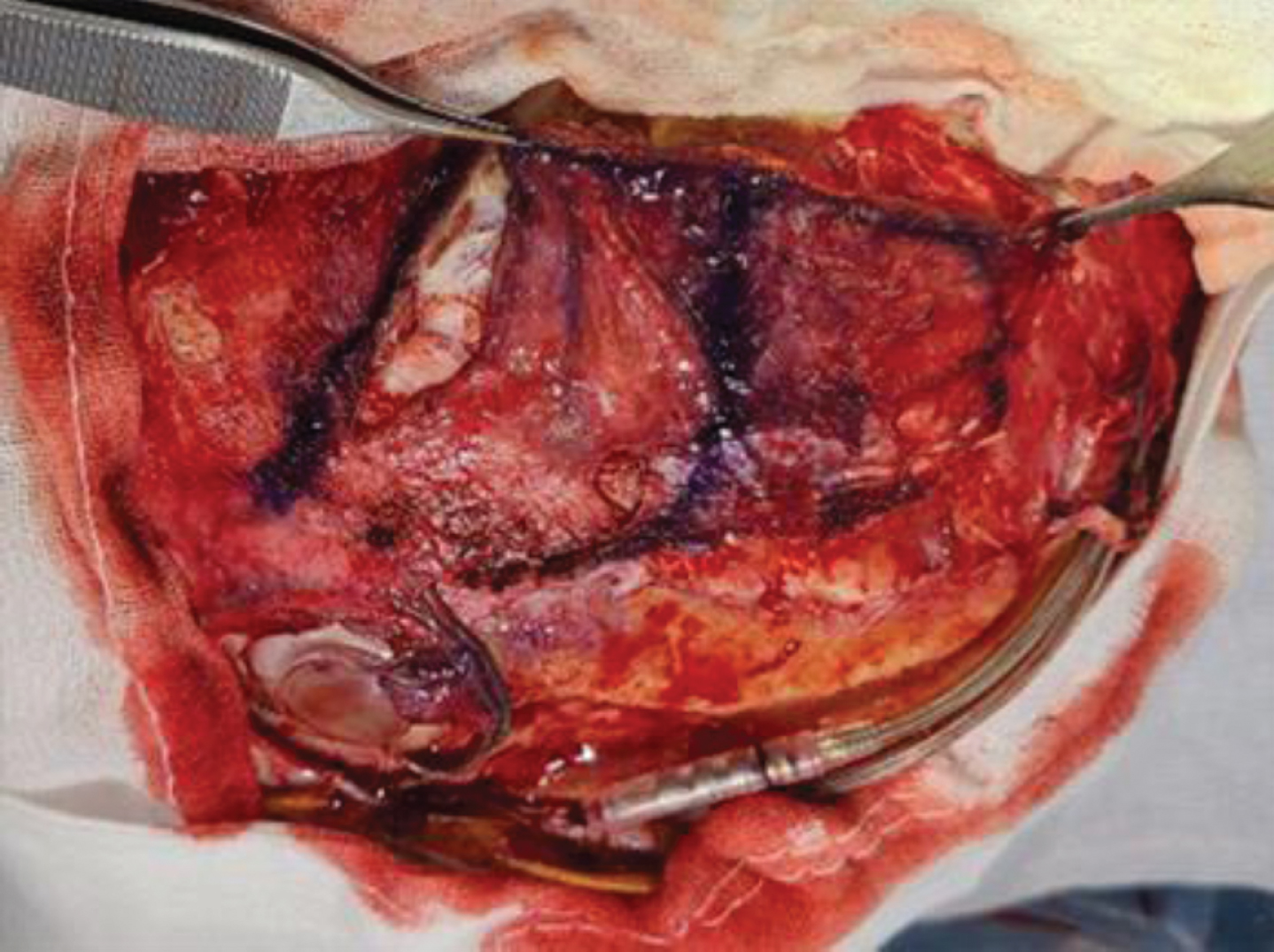
After the scalp was elevated, the burr hole cover and the proximal cable were exposed. A blue marker was used to create the surgical design for dissecting the temporalis fascia from the muscle.
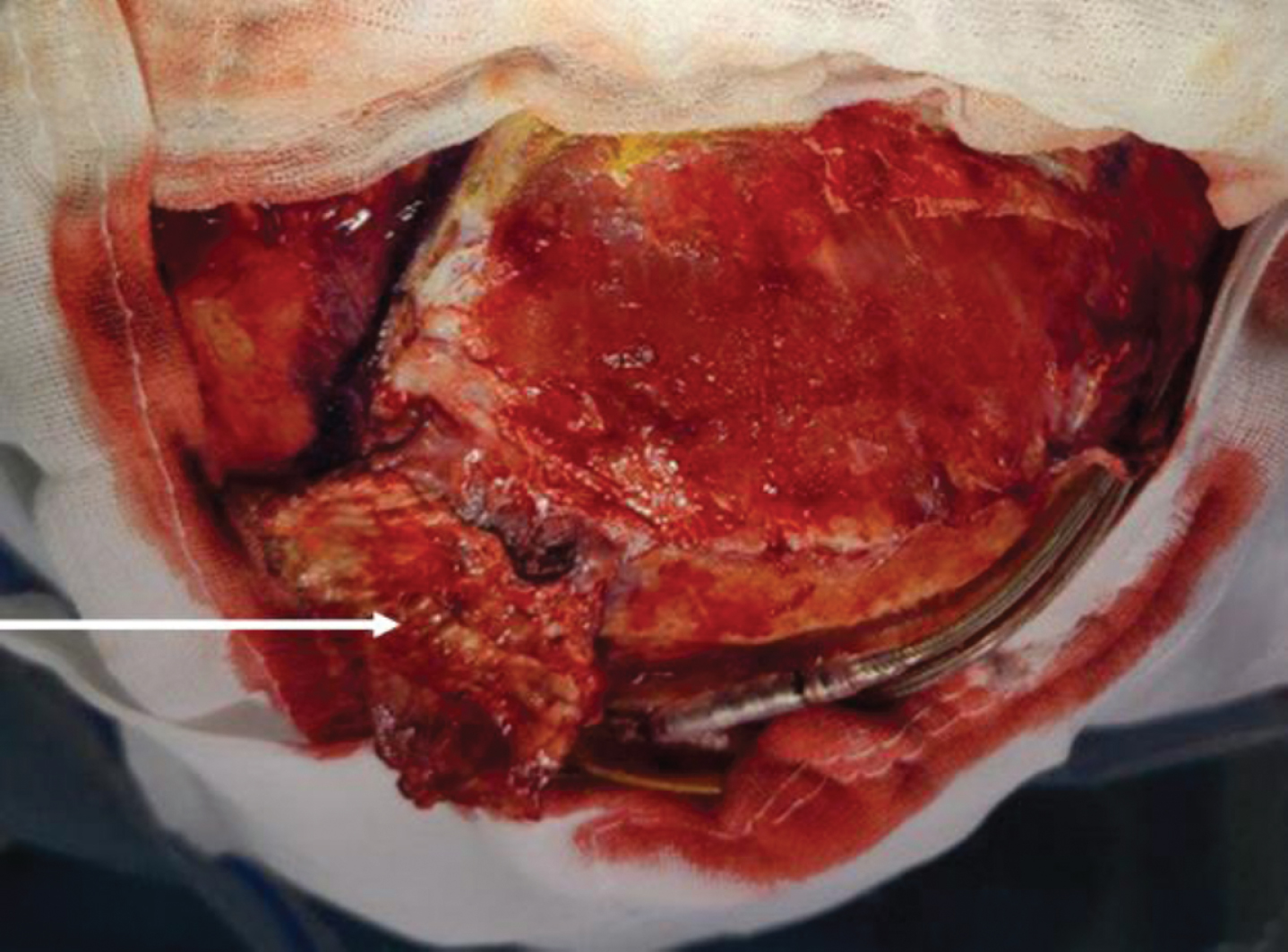
Coverage of the burr hole cover using dissected temporalis fascia (white arrow).
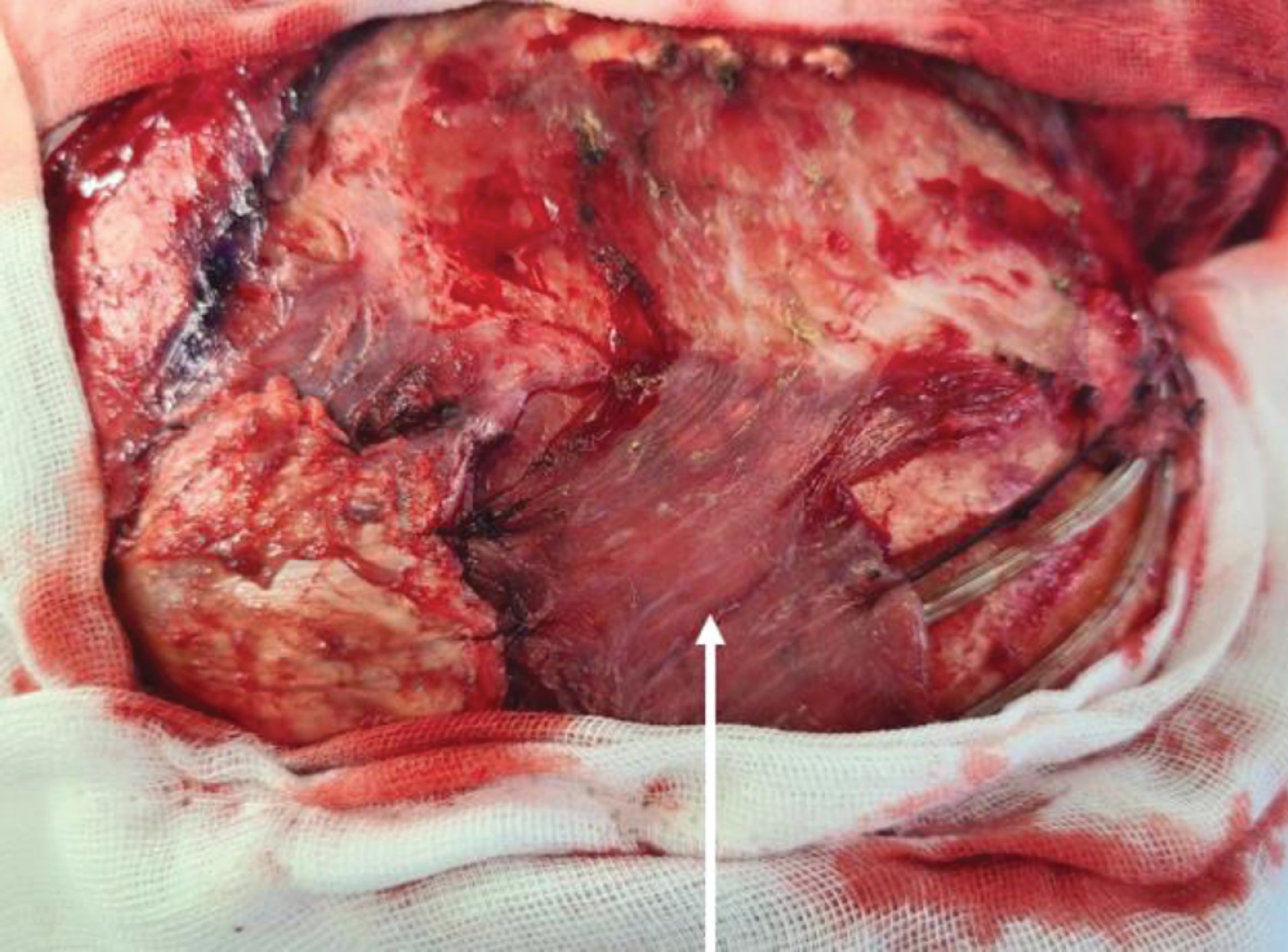
Coverage of the proximal cable using the temporalis muscle flap (white arrow).
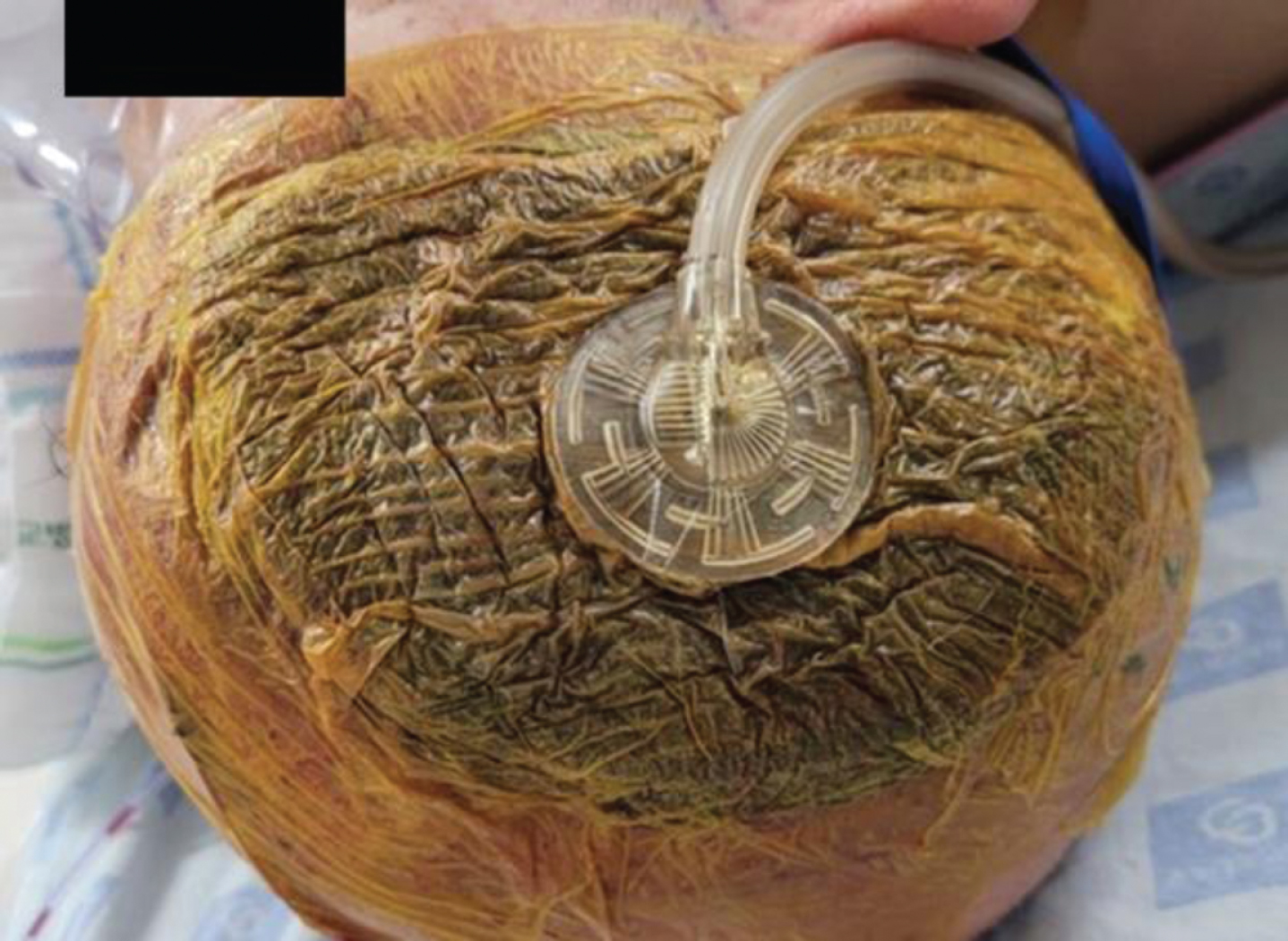
After the surgery, the VAC device was placed with a good seal to maintain negative pressure.

The erosion site (white circle) 3 months after surgery, showing good recovery. There were no additional complications.
DISCUSSION
Scalp erosion is a significant complication that leads to exposure of the underlying hardware and possible infection [7, 8]. A variety of preventative techniques have been described, including modified methods for creating the cranial incision and burr hole [9, 10]. In cases of obvious infection and purulence, debridement and hardware explantation are commonly recommended [11]. However, in cases of nonpurulent erosion, there is no consensus regarding the optimal treatment.
Factors that likely predispose a patient to scalp erosion include scalp thickness and the use of bulky hardware [12]. However, in the case of DBS, because of the burr hole, poor cortical bone vascularity also affects erosion. Most DBS patients are elderly, and if they have complications, such as DM, as in our case, they are more likely to develop erosion.
If scalp wounds are eroded without obvious purulence or infection, there is a possibility of wound revision without hardware removal. Traditionally, this would involve the debridement of friable scalp edges, undermining of the galea and/or pericranium, and an attempt at mobilizing the local tissues for primary closure. However, even small areas of erosion are subject to increased tension with primary closure due to the relative inelasticity of the scalp and underlying layers [13–15]. Furthermore, once erosion has occurred, further tissue loss following debridement should preclude any additional attempts at primary closure, and a flap should be considered in any subsequent reconstruction. However, if the scalp erodes despite the flap, there are few options to consider.
The temporalis muscle flap has a reliable and hearty blood supply, can be tailored for the reconstruction of most craniofacial defects, and arguably presents minimal donor site morbidity if performed correctly. The temporalis muscle flap lies in the same operative field as the defect, potentially reducing the operative duration and motion-induced viability issues during the recovery period. The deep temporal fascia lines the flap and obviates the need for skin grafting [16].
In our case, we used the temporalis fascia and muscle flap to cover the burr hole cover. In this way, we were able to block direct contact between the scalp and the burr hole cover, which would also induce physiological adhesion of the scalp to the muscle flap. In addition, using the flap could prevent the possibility of creating dead space between the scalp and burr hole cover caused by vacuum.
Although the standard pressure in VAC is 125 mmHg [17], in situations where CSF leakage is a possibility, the pressure is lowered to 25– 50 mmHg [6, 18]. In our case, with a burr hole covered with a temporalis muscle flap, we judged that the possibility of CSF leakage was not high. Therefore, we applied 75 mmHg of pressure.
VAC therapy is a novel method of wound healing using topical negative pressure to encourage the healing of deep, chronic wounds. This therapy has documented efficacy in accelerating healing and improving the healing rates of wounds, such as diabetic ulcers, postsurgical abdominal and sternotomy wounds, complex perineal wounds, infective wounds, and pressure ulcers [19].
The mechanism of action of VAC is understood to increase healing rates by enhancing blood flow, reducing edema, increasing granulation tissue formation and wound retraction, aiding the removal of exudate and biochemically reducing the concentration of proteases, which are known to impair healing [20]. In patients with DM, VAC is known to reduce the healing time and may reduce the incidence of infection; furthermore, one trial reported significantly fewer secondary amputations among DM foot ulcer patients who received VAC therapy [21]. This suggests that it can also be effective in the treatment of recurrent scalp erosion accompanied by DM.
Although VAC has been increasingly used to treat wounds in the head and neck region [22–25], its use for scalp erosion after DBS has not been described.
Our patient’s scalp was weakened by previous surgeries, and due to the advanced age of the patient and the presence of diabetes, an additional flap or skin graft was judged to be risky. Therefore, we decided to apply VAC therapy to cover the defect and achieved recovery of the weakened scalp.
Due to the characteristics of patients treated with DBS, patients with erosion tend to be old, and due to the implant, additional surgery is burdensome. In patients with recurrent scalp erosion after DBS, VAC therapy could restore the weakened scalp and be a good option for surgeons to consider instead of additional scalp flaps or skin grafts.
CONCLUSION
The aim of our study was to provide a technical note on VAC in a patient with recurrent scalp erosion after DBS. This is the first report to discuss the use of a temporalis fascia and muscle flap with VAC. Recurrent scalp erosion risks implant exposure, and skin grafts or flaps can be difficult to consider depending on the patient’s comorbidities. Our method will be a good choice for patients with recurrent scalp erosion. If the condition of the scalp is weakened, this method can be considered preferentially.
Footnotes
ACKNOWLEDGMENTS
This research was supported by Chungbuk National University Korea National University Development Project (2020).
STATEMENT OF ETHICS
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. The identity of the patient was protected.
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare.