
Abstract
Background:
There is a need for identifying risk factors for hospitalization in Parkinson’s disease (PD) and also interventions to reduce acute hospital admission.
Objective:
To analyze the frequency, causes, and predictors of acute hospitalization (AH) in PD patients from a Spanish cohort.
Methods:
PD patients recruited from 35 centers of Spain from the COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015) cohort from January 2016 to November 2017, were included in the study. In order to identify predictors of AH, Kaplan-Meier estimates of factors considered as potential predictors were obtained and Cox regression performed on time to hospital encounter 1-year after the baseline visit.
Results:
Thirty-five out of 605 (5.8%) PD patients (62.5±8.9 years old; 59.8% males) presented an AH during the 1-year follow-up after the baseline visit. Traumatic falls represented the most frequent cause of admission, being 23.7% of all acute hospitalizations. To suffer from motor fluctuations (HR [hazard ratio] 2.461; 95% CI, 1.065–5.678; p = 0.035), a very severe non-motor symptoms burden (HR [hazard ratio] 2.828; 95% CI, 1.319–6.063; p = 0.008), falls (HR 3.966; 95% CI 1.757–8.470; p = 0.001), and dysphagia (HR 2.356; 95% CI 1.124–4.941; p = 0.023) was associated with AH after adjustment to age, gender, disease duration, levodopa equivalent daily dose, total number of non-antiparkinsonian drugs, and UPDRS-IIIOFF. Of the previous variables, only falls (HR 2.998; 95% CI 1.080–8.322; p = 0.035) was an independent predictor of AH.
Conclusion:
Falls is an independent predictor of AH in PD patients.
INTRODUCTION
Motor and non-motor symptoms (NMS) in Parkinson’s disease (PD) progress as the disease advances, which leads to complications such as falls, fractures, or infections. As a consequence, PD patients are reported to have 1.44 times more hospital admissions when compared to age and sex-matched peers [1, 2]. These admissions are associated with prolonged length-of-stay and increased morbidity and mortality [3–5]. Once PD patients are admitted to hospital, they have prolonged inpatient stays [6], poor motor outcomes, infections, prescription errors, and increased postoperative mortality [7–10]. Moreover, following a first hospital encounter, the rate of a second encounter increased to approximately 50% when patients were followed into a second year [11]. Previous studies reported a significant economic burden from PD hospitalization as well [12, 13]. There is a need for identifying risk factors for hospitalization in PD and also interventions to reduce acute PD hospital admission [14].
The aim of the present study was (1) to analyze the frequency and causes of acute hospitalization in PD patients from a Spanish cohort followed for 1-year and (2) to identify predictors of acute hospitalization.
MATERIAL AND METHODS
PD patients recruited from 35 centers of Spain from the COPPADIS cohort [15], from January 2016 to November 2017, were included in the study. Methodology about COPPADIS-2015 study can be consulted in https://bmcneurol.biomedcentral.com/articles/10.1186/s12883-016-0548-9. This is a multi-center, observational, longitudinal-prospective, 5-year follow-up study designed to analyze disease progression in a Spanish population of PD patients. All patients included were diagnosed according to UK PD Brain Bank criteria. Exclusion criteria were: atypical parkinsonism, dementia (Mini-Mental State Examination [MMSE] < 26), age < 18 or > 75 years, inability to read or understand the questionnaires, to be receiving any advanced therapy (continuous infusion of levodopa or apomorphine, and/or with deep brain stimulation at baseline), and the presence of comorbidity, sequelae, or any disorder that could interfere with the assessment.
The data for the present study was obtained from the baseline evaluation [15]. Patient baseline evaluation included staging of severity of disease (modified Hoehn &Yah [H&Y] scale), motor assessment (Unified Parkinson’s Disease Rating Scale [UPDRS] part III and part IV, Freezing of Gait Questionnaire [FOG-Q]), non-motor symptoms (Non-Motor Symptoms Scale [NMSS], Parkinson’s Disease Sleep Scale [PDSS], Visual Analog Scale-Pain [VAS-Pain], Visual Analog Fatigue Scale [VAFS]), cognition (MMSE, Parkinson’s Disease Cognitive Rating Scale [PD-CRS], completing a simple 16-piece puzzle), mood and neuropsychiatric symptoms (Beck Depression Inventory-II [BDI-II], Neuropsychiatric Inventory [NPI], Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale [QUIP-RS]), disability (Schwab &England Activities of Daily Living Scale [S&E]), health related quality of life (QoL) (the 39-item Parkinson’s disease Questionnaire [PDQ-39SI]), and global QoL (PQ-10, EUROHIS-QOL 8-item index [EUROHIS-QOL8]) [16]. Interviews were conducted to determine the presence of falls according to the definition for falls proposed by the Kellogg International Work Group on the prevention of falls by the elderly [17]: a fall is an unintentional or unexpected event, results in the person coming to rest on the ground or another lower level and is not the result of a major intrinsic event (such as a loss of consciousness) or an overwhelming external force. The event was considered when it was not something that happened for a specific reason some time ago but was a repeated abnormal phenomenon. A time frame was not defined but it was specifically asked about the presence and number of falls in the last month. Moreover, falls diary, calendar, or postcard were not used. In patients with motor fluctuations, the motor assessment was conducted during the OFF state (without medication in the last 12 hours) and during the ON state. However, in patients without motor fluctuations, the assessment was only performed without medication (first hour in the morning without taking medication in the previous 12 hours).
The patients were followed for 1-year after the baseline visit and information about hospital admission was collected. Specifically, the following hospitalization-related data were recorded: number of hospitalizations, hospital stay days, and reasons for hospital admission. Those patients with at least one acute hospitalization during the follow-up were defined as Patients with acute hospitalization, whereas those with non-acute hospitalization during the follow-up was defined as Patients without acute hospitalization. Therefore, those patients with one or more programmed admission but without any acute hospitalization were considered as Patients without acute hospitalization. Rehospitalization was not considered for the analysis. The reasons for hospital admissions were divides in three groups [18]: 1) Direct PD-related morbidity: motor complications, psychiatric symptoms, autonomic dysfunction, sensory symptoms, sleep disorders, and side effects of anti-parkinsonian drugs; 2) Indirect PD-related morbidity: traumas, pneumonia, and intestinal obstruction / gastroparesis; 3) Non-PD related causes.
Data analysis
Data were processed using SPSS 20.0 for Windows. For comparisons between patients with and without an acute hospitalization, the Student’s t-test, Mann-Whitney-Wilcoxon test, Chi-square test, or Fisher test, as appropriate, were used (distribution for variables was verified by one-sample Kolmogorov-Smirnov test). Kaplan-Meier estimates were obtained to determine the risk of acute hospitalization with regards to the presence of different PD symptoms and/or complications: motor fluctuations; dyskinesia; very severe NMS (NMSS total score > 70) [19]; major depression [16]; cognitive impairment [20]; freezing of gait (FOG); falls; dysphagia. Self-reported FOG was defined regarding the FOG-Q as presenting with a FOG-Q item-3 score > 0. Functional dependency was defined as a S&E score less than 80% (80% = completely independent; 70% = not completely independent) [21]. Patients with a NMSS item-19 score > 0 were considered as suffering from dysphagia. Cox proportional hazards models were applied to identify independent predictors of acute hospitalization during the 1-year follow-up. Factors included as potential predictors were motor severity, motor complications, axial symptoms and related complications (FOG; falls; dysphagia), NMS burden, mood, cognition, neuropsychiatric symptoms, and disability for activities of daily living (Supplementary Table 1). Age, gender, disease duration, LEDD (levodopa equivalent daily dose [22]), and total number of non-antiparkinsonian drugs (as a marker of comorbidity [23]) were included as covariates (Supplementary Table 1). Values of p < 0.05 were considered significant.
Standard protocol approvals, registrations, and patient consents
For this study, we received approval from the Comité de Ética de la Investigación Clínica de Galicia from Spain (2014/534; 02/DEC/2014). Written informed consents from all participants in this study were obtained before the start of the study. COPPADIS-2015 was classified by the AEMPS (Agencia Española del Medicamento y Productos Sanitarios) as a Post-authorization Prospective Follow-up study with the code COH-PAK-2014-01.
Data availability
The protocol and the statistical analysis plan are available on request. De-identified participant data are not available for legal and ethical reasons.
RESULTS
A total of 605 (62.5±8.9 years old; 59.8% males) from the 694 patients diagnosed with PD at baseline from the COPPADIS cohort were included in the analysis (87.2%). Figure 1 shows the reasons for the lack of follow-up of 89 patients. In 64 cases (9.2%) no data was recorded. The mean disease duration (N = 605) at baseline was 5.5±4.4 years. Forty-one out of 605 PD patients (6.8%) presented at least one hospitalization during the 1-year follow-up after the baseline visit, being 35 of them (85.4%) with at least one acute hospitalization. From the initial PD cohort (N = 693; 1 case excluded due to change in diagnosis), 5% of the patients presented an acute hospitalization (Fig. 2A). In 35 out of 41 patients (85.4%) hospital admission was reported once, twice in 4 patients (9.8%), and three times in 2 patients (4.8%). The mean hospital stay days was 8.4±8.3 (range 1–39). A total of 49 admissions were reported, being 38 acute and 11 programmed hospitalizations (Table 1). With regards to the acute admissions, 3 patients out of 35 (8.6%) were hospitalized due to a direct PD-related morbidity, 15 (42.9%) due to an indirect PD-related morbidity, and 14 (40%) due to non-PD related causes (Fig. 2B). Traumatic falls (9 events) represented the most frequent cause of admission, being 56.3% of all indirect PD-related morbidity causes, 23.7% all acute hospitilizations (38 events), and 18.4% of all hospitalizations (49 events) (Table 1 and Fig. 2C). No deaths were reported, neither in patients who presented a hospitalization nor in those who did not.
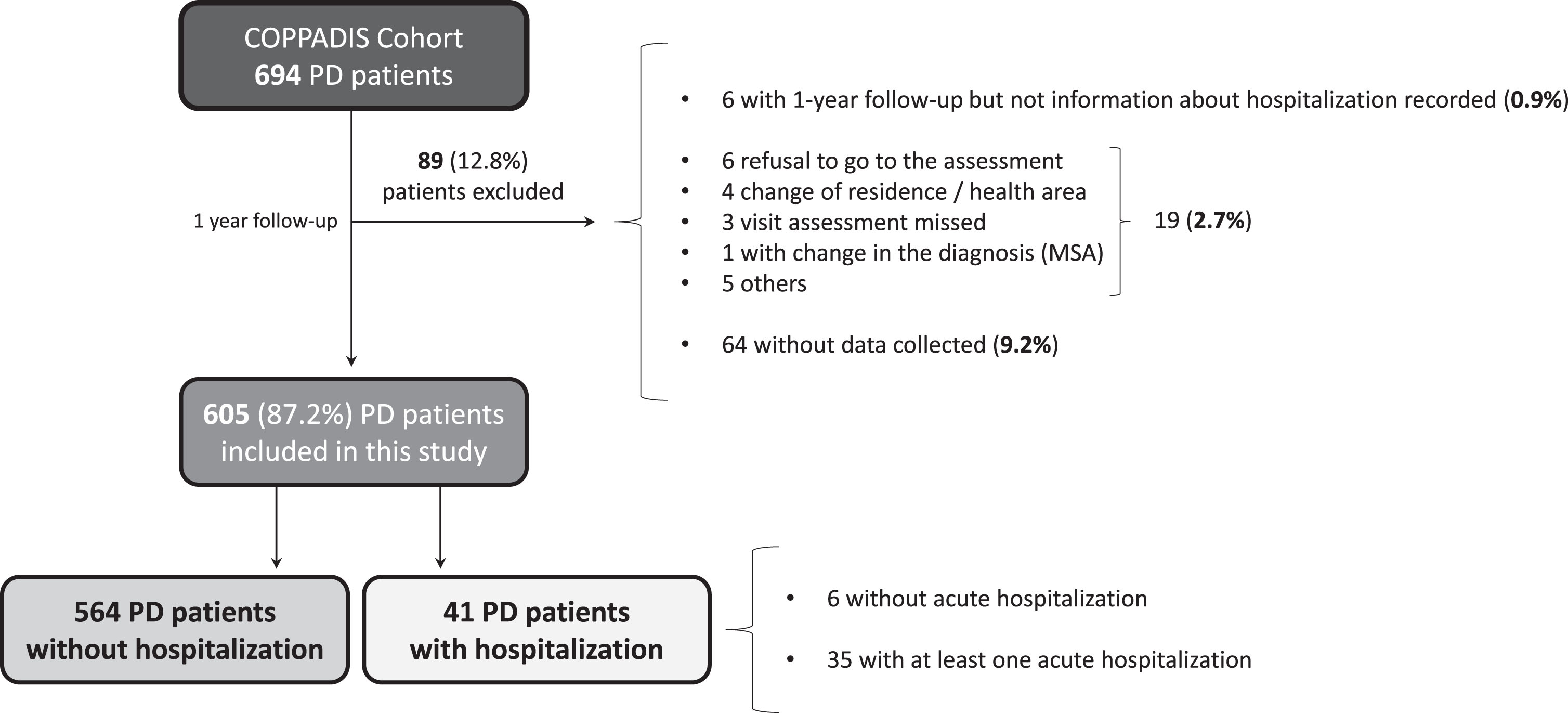
Flowchart about PD patients from the COPPADIS cohort participating in the present study. Of 594 patients, 1 patient was excluded due to change in the diagnosis (from PD to MSA) and 88 for other reasons. Of 605 patients included in the analysis, 41 (6.8%) presented at least one hospitalization (35 acute and 6 planned hospitalization). MSA, multiple system atrophy; PD, Parkinson’s disease.
Causes of hospitalization during the 1 year follow-up after the baseline visit: 49events in 41 PD patients
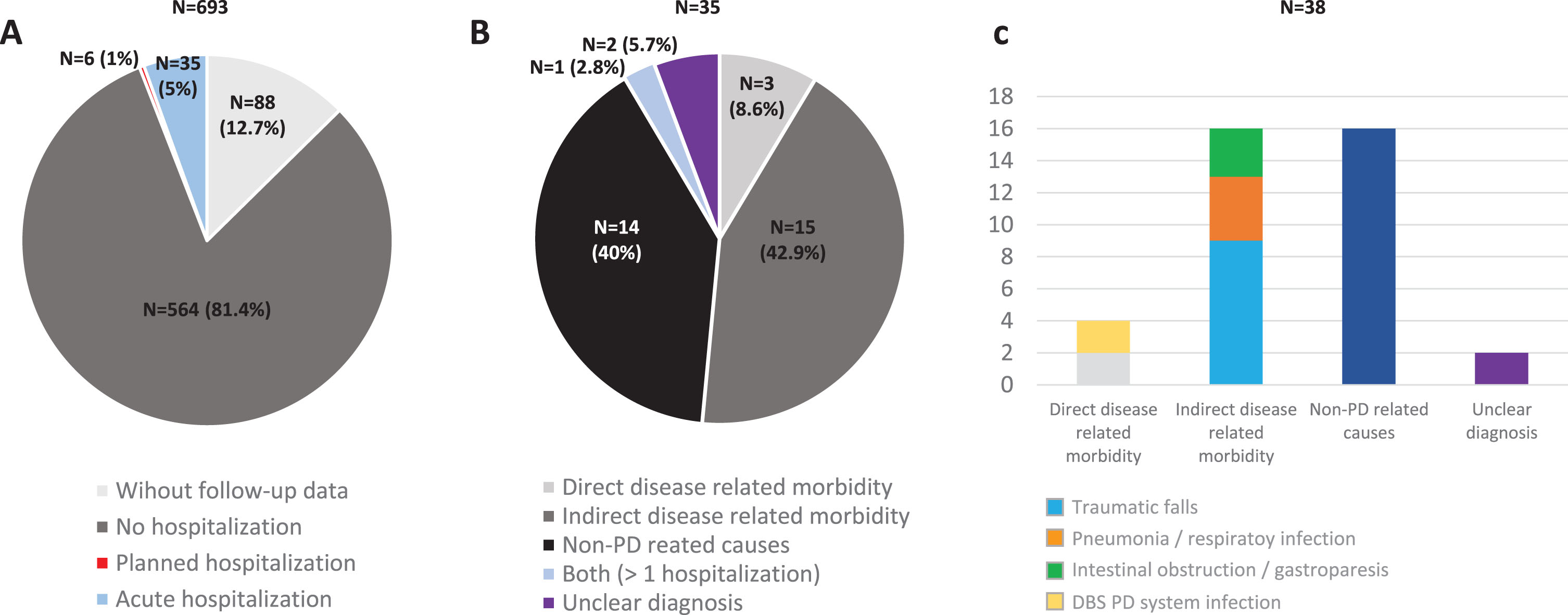
A) Percentage of PD patients from the COPPADIS cohort (N = 693; 1 excluded due to change in the diagnosis) without follow-up data (N = 88; 12.7%), without hospitalization (N = 564; 81.4%), with planned hospitalization (N = 6; 1%), and with acute hospitalization (N = 35; 5%) during the 1-year follow-up after the baseline visit. B) Percentage of patients with at least one acute hospitalization (N = 35) regarding the reason of admission: Direct PD-related morbidity (N = 3; 8.6%); Indirect PD-related morbidity (N = 15; 42.9%); Non-PD related causes (N = 40; 40%); More than 1 hospitalization with both reasons (N = 1; 2.8%); Unclear diagnosis (N = 2; 5.7%). C) Reasons for hospital admissions (38 events) in the subgroup of patients with acute hospitalization: 1) Direct PD-related morbidity (4 events; 10.5%); 2) Indirect PD-related morbidity: traumas, pneumonia, and intestinal obstruction / gastroparesis (16 events; 42.1%); 3. Non-PD related causes (16 events; 42.1%). PD, Parkinson’s disease.
There were no differences between patients who presented an acute hospitalization compared to those who did not in terms of age, gender, disease duration, motor phenotype, and H&Y motor stage (Table 2). However, patients who suffered from an acute hospitalization presented a worse motor (UPDRS-III-OFF and UPDRS-IV) and non-motor status (PD-CRS, NMSS, BDI-II, NPI, and PDSS) at baseline (Table 2). Motor fluctuations, dyskinesia, falls, dysphagia, a severe and/or very severe NMS burden, and pain were more frequent in patients who presented an acute hospitalization compared to those who did not (Table 2). Specifically, the NMSS total score (66.1±42.8 vs 41.9±35; p < 0.0001) and the score on domains 2 (sleep/fatigue), 3 (mood/apathy), 4 (perceptual problems/hallucinations), 5 (attention/memory), 6 (gastrointestinal symptoms), and 7 (urinary symptoms) of the NMSS indicating a greater severe burden were higher in patients with acute hospitalization (Fig. 3A and Supplementary Table 2). Moreover, QoL and disability were worse in this group of patients with acute hospitalization, presenting a higher score at baseline on the PDQ-39SI (26.6±16 vs 15.9±13.3; p < 0.0001) and a lower score on the EUROHIS-QOL8 (3.6±0.6 vs 3.8±0.5; p = 0.038) and S&E score (83.4±11.4 vs 87.9±10.7; p = 0.048) when compared with patients without acute hospitalization (Table 2). With regards to the domains of the PDQ-39SI, patients with acute hospitalizations presented significantly higher scores in all domains indicating a worse QoL except on domains 4 (stigma), 5 (social support), and 8 (pain/discomfort) (Fig. 3B and Supplementary Table 2).
Disease related characteristics, motor and non-motor symptoms, autonomy for activities of daily living and quality of life in PD patients with and without acute hospitalization during the year after the baseline visit (n = 605)
The results represent percentages, mean±SD or median [p25, p75].Chi-squared and Mann-Whitney-Wilcoxon test were applied for comparisons between Non acute hospitalization (N = 570) and Acute unplanned hospitalization (N = 35) patients. Data about H&Y and UPDRS-III are during the OFF state (first thing in the morning without taking medication in the previous 12 hours). ADLS, Schwab and England Activities of daily living Scale); BDI, Beck Depression Inventory-II; NMSS, Non-Motor Symptoms Scale; NPI, Neuropsychiatric Inventory; PD, Parkinson’s disease; PD-CRS, Parkinson’s Disease Cognitive Rating Scale; PDSS, Parkinson’s Disease Sleep Scale; PIGD, Postural Inestability Gait Difficulty; QUIP-RS, Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale; UPDRS, Unified Parkinson’s Disease Rating Scale; VAFS, Visual Analog Fatigue Scale; VAS-Pain, Visual Analog Scale-Pain.
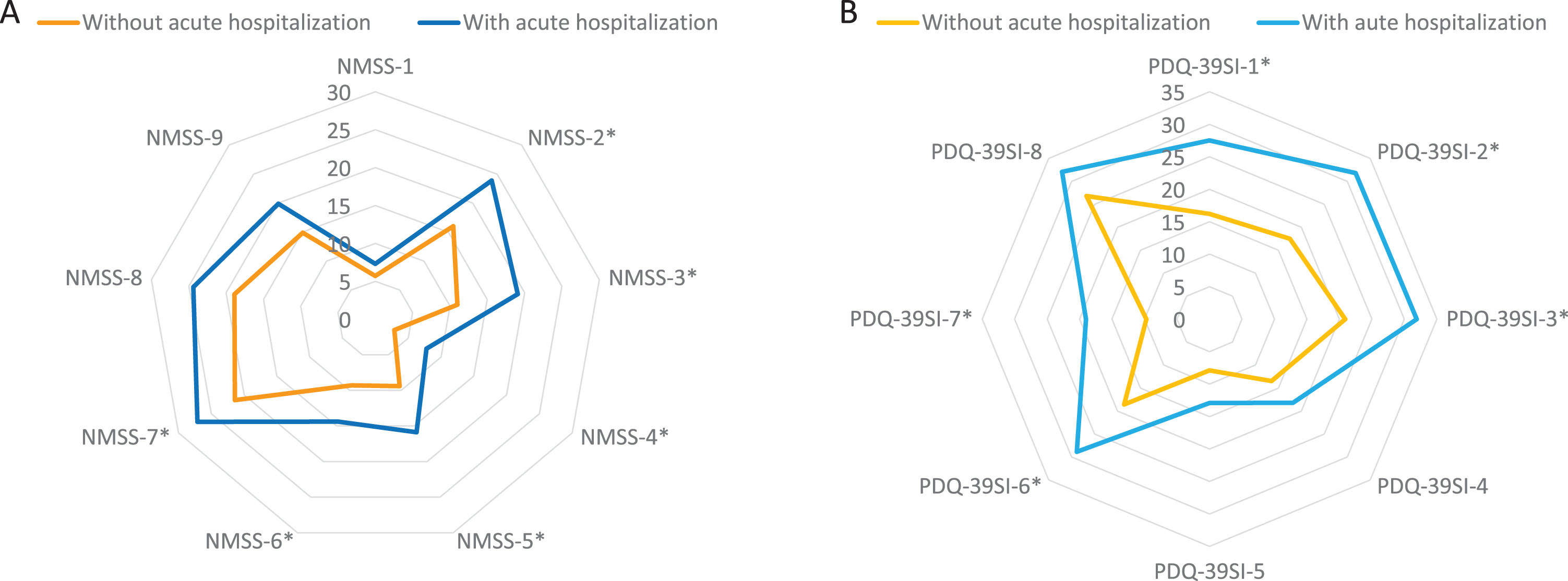
A) Comparison in PD patients with vs without acute hospitalization of mean NMSS score on each domain of the scale at baseline; NMSS-1, Cardiovascular (p = 0.892); 2) NMSS-2, Sleep/fatigue (p = 0.003); NMSS-3, Depression/apathy (p = 0.003); NMSS-4, Perceptual problems/hallucinations (p = 0.001); NMSS-5, Attention/memory (p = 0.001); NMSS-6, Gastrointestinal tract (p = 0.041); NMSS-7, Urinary symptoms (p = 0.040); NMSS-8, Sexual dysfunction (p = 0.152); NMSS-9, Miscellaneous (p = 0.106). B) Comparison in PD patients with vs without acute hospitalization of mean PDQ-39SI score on each domain of the scale: PDQ-39SI-1, Mobility (p = 0.001); PDQ-39SI-2, Activities of daily living (p = 0.002); PDQ-39SI-3, Emotional well-being (p = 0.002); PDQ-39SI-4, Stigma (p = 0.153); PDQ-39S-5, Social support (p = 0.259); PDQ-39SI-6, Cognition (p = 0.001); PDQ-39SI-7, Communication (p < 0.0001); PDQ-39SI-8, Pain and discomfort (p = 0.133). NMS, Non-motor symptoms; PD, Parkinson’s disease.
In Kaplan-Meier analysis, the presence at baseline of motor fluctuations (p = 0.004), dyskinesia (p = 0.003), very severe NMS burden (p = 0.001), major depression (p = 0.037), falls (p = 0.001), and dysphagia (p = 0.001) was related to a higher risk of acute hospitalization (Fig. 4). Specifically, to suffer from motor fluctuations (HR [hazard ratio] 2.461; 95% CI, 1.065–5.678; p = 0.035), a very severe NMS burden (HR [hazard ratio] 2.828; 95% CI, 1.319–6.063; p = 0.008), falls (HR 3.966; 95% CI 1.757–8.470; p = 0.001), and dysphagia (HR 2.356; 95% CI 1.124–4.941; p = 0.023) was associated with acute hospitalization after adjustment to age, gender, disease duration, LEDD, total number of non-antiparkinsonian drugs, and UPDRS-III-OFF (Table 3). Patients who presented a score on the UPDRS-III-OFF > 20 at baseline had a significantly higher risk of acute hospitalization after adjustment to the same covariates as well (HR 3.644; 95% CI 1.430–9.284; p = 0.007). Although unadjusted HR associated with dyskinesia (HR 2.792; 95% CI 1.365–5.711; p = 0.005) and major depression (HR 2.159; 95% CI 1.033–4.515; p = 0.041) were significant (Table 3), the effect was not after adjustment to the previous commented covariates. Of the previous variables, only falls (HR 2.998; 95% CI 1.080–8.322; p = 0.035) was an independent predictor of acute hospitalization when different covariates as potential predictors of hospitalization were included in an “a priori” well-planned model (Table 4). In the model, having falls triples the probability of acute hospital admission regardless of other variables, and the frequency of falls at baseline was double in those patients who were admitted during the 1-year follow-up compared to those who did not (31.4% vs 15.5%; p = 0.020). Specifically, having falls during the previous month to the baseline visit was associated with acute admission during the 1-year follow-up (Supplementary Figure 1).
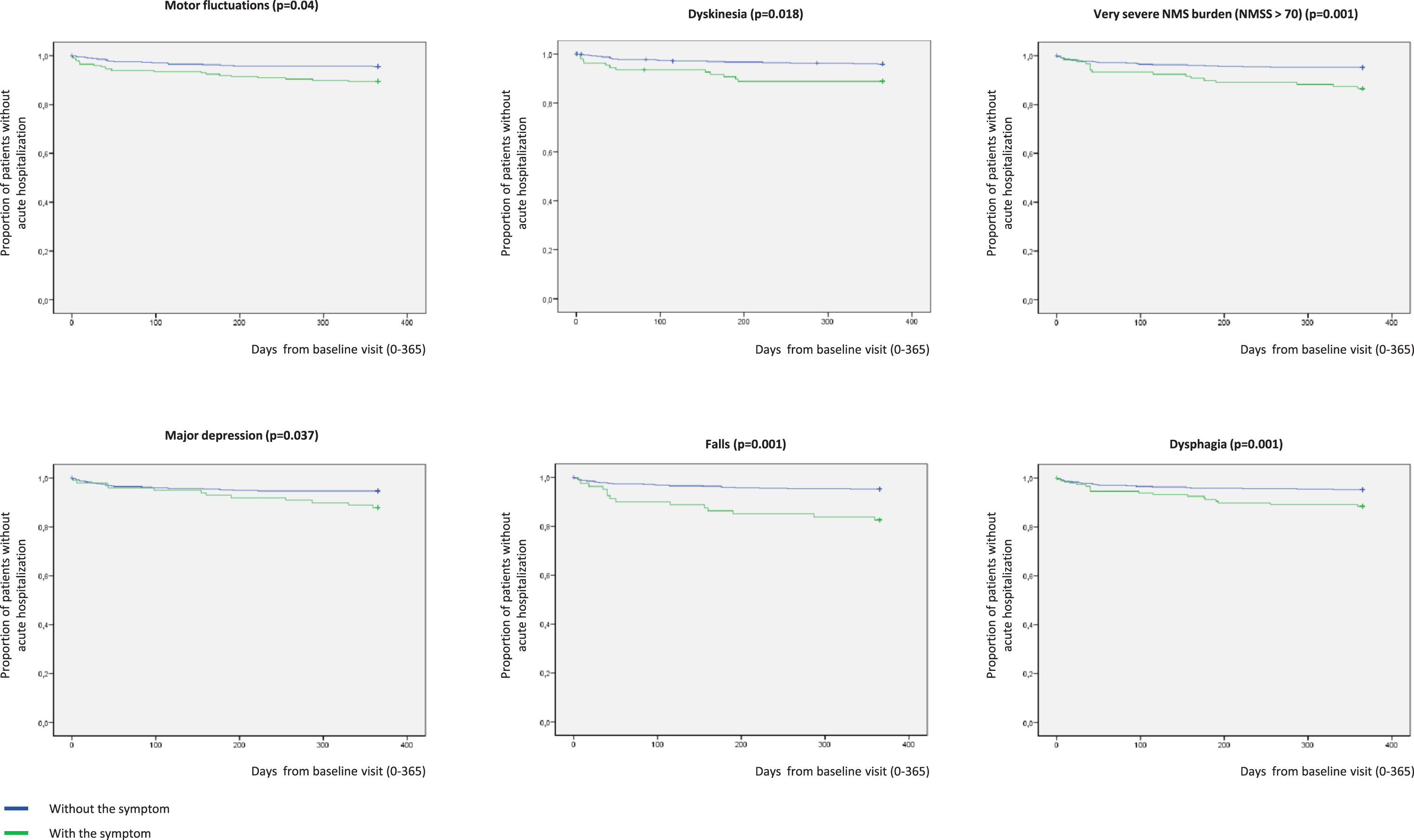
Proportion of patients without acute hospitalization with regards to suffering (in blue) or not (in green) from motor fluctuations (p = 0.004), dyskinesia (p = 0.003), very severe NMS burden (p = 0.001), major depression (p = 0.037), falls (p = 0.001), and dysphagia (p = 0.001). Y, survival; X, days of follow-up. NMS, Non-motor symptoms.
Analysis about the risk of acute hospitalization after 1 year of follow-up with regards to having or not different complications (N = 605)
Age, gender, disease duration, LEDD (levodopa equivalent daily dose), total number of non-anti parkinsonian drugs (as a marker of comorbidity) and UPDRS-III-OFF were included in the model as covariates. *For this analysis the UPDRS-III-OFF was not included in the model. FOG, freezing of gait; HR, Hazard ratio; NMSB, non-motor symptoms burden; NMSS, Non-Motor Symptoms Scale; PD-CRS, Parkinson’s Disease Cognitive Rating Scale; UPDRS, Unified Parkinson’s Disease Rating Scale.
Cox-regression model about predictors of acute hospitalization in PD patients after 1 year of follow-up (N = 605)
Hazard ratio; LEED, Levodopa equivalent daily dose; NMSS, Non-Motor Symptoms Scale; NPI, Neuropsychiatric Inventory; PD-CRS, Parkinson’s Disease Cognitive Rating Scale; UPDRS, Unified Parkinson’s Disease Rating Scale. The omnibus test indicated an overall significant model χ2 = 34,149 (p = 0.001).
DISCUSSION
In the present study, we observed different important findings: 1) the probability of presenting an acute hospitalization is not infrequent in patients with PD; 2) the QoL and autonomy for activities of daily living is worse and the NMS burden is greater in those PD patients who will have an acute hospitalization; 3) there are certain symptoms associated with a greater risk of acute hospitalization such as motor fluctuations, dyskinesias, severe NMS burden, major depression, falls, and dysphagia; 4) falls is an independent predictor of acute hospitalization that increases the risk by three times.
About 5% of the patients from the COPPADIS cohort [15, 16] presented an acute hospitalization after 1-year of follow-up. This percentage is low compared to other studies, ranging from 7 to 28% per year [17]. The results between studies vary in part to differences in methodology [1, 24–27]. Moreover, many studies are prospective [6, 28] or, more frequently, retrospective [29–34] analysis conducted only in PD patients admitted with the aim to analyze problems during hospitalization. Moreover, several studies were conducted in small samples and/or without control group: 76 patients [28]; 108 patients [26]; 130 patients [25]; 132 patients [6]; 143 patients [33]; 144 patients [24]; 173 patients [30]; 367 patients [3]. A recent study conducted in a large population from North America, the Netherlands, and Israel showed that of 4,680 PD patients followed during an average of 2 years (median 1.85, maximum 4.85 years), 2,264 patients (48.4%) had a hospital encounter after the baseline visit [35]. Compared with many other studies [6, 37], the mean age of the patients from the COPPADIS cohort is lower, and, as previously reported [23, 38], our sample is not fully representative of the PD population due to inclusion and exclusion criteria at baseline (i.e., age limit, no dementia, no severe comorbidities, no second line therapies, etc.) which subsequently entails a bias toward early PD. This aspect may explain the lower frequency of admissions in our analysis after 1-year of follow-up. On the other hand, with regards to the causes of hospitalization, our findings are in line with two recent review studies [26, 39], in which infections, worsening motor features, falls/fractures, cardiovascular co-morbidities, neuropsychiatric, and gastrointestinal complications were the main reasons for hospitalization among people with PD. Specifically, in our study, falls was the most frequent cause despite more than 90% of the patients had a stage 2 of the H&Y. By the contrary, admissions related to a direct PD-related event were infrequent since ambulatory PD symptoms management is often preferred.
A worse QoL and a greater disability and NMS burden at baseline was observed in PD patients who presented an acute hospitalization in our study. We observe this finding because, unlike most other studies, the assessment at baseline was exhaustive using different validated scales. Differences were observed between patients who were admitted during the follow-up and those who did not as those who were admitted had a worse motor and non-motor status and worse autonomy for activities of daily living and QoL. In other words, PD patients more affected by their disease may be more vulnerable and have a higher risk of acute hospitalization. Symptoms such as pain, dysphagia, falls, motor fluctuations, dyskinesia, a worse QoL, and a greater motor disability were more frequent in patients who presented an acute hospitalization, but no differences were observed in fatigue and motor phenotype. Falls, fractures, infections, cognitive, and motor decline have been identified as risk factors for acute hospital admissions in patients with PD [11, 14]. More specifically, longer timed up and go test, higher number of comorbidities, number of medications, the presence of motor fluctuations, having deep brain stimulation, and the degree of caregiver burden have been associated with hospitalization and/or rehospitalization in PD [35]. A higher PDQ-39 total score was observed to be associated with a higher risk of rehospitalization as well [35]. In our study, the factors associated with acute hospitalization are not surprising. However, the only independent predictor of hospitalization was falls. In this context, in a pooled data of 7 studies selected [27], the main causes of general ward admission were falls (30%) and PD-related causes (16%), whereas the main causes of neurological ward were motor (42.3%) and psychiatric complications (21.2%). In any case, our finding of falls as a predictor of acute hospitalization in PD should be interpreted with caution because the rates of admission due to fall (N = 9) were very low. Ideally, these findings should be reproduced over a longer period to capture more admission and arguably with patients with a broader range of severity.
A very important point is that some of these symptoms can be treated with the aim of reducing acute PD hospital admission [14]. For example, in our cohort, motor fluctuations were associated with a doubled probability of acute hospitalization, so reducing OFF time could reduce the risk. Many factors are correlated. Falls were associated with motor fluctuations (falls were present in 22.4% of patients with motor fluctuations compared to 8.5% of patients without them; p < 0.0001). One strategy for reducing them could be to increase the ON time in PD patients. However, falls can have different etiology. Optimizing motor symptom control and managing medication side effects may prevent falls and hence hospital admissions [14]. Furthermore, physiotherapy is thought to improve PD motor symptoms, mobility, and balance [39], which also may reduce the risk of falls. However, there is a lack of evidence about interventions or negative results in the few trials performed [14]. In a randomized clinical trial comparing the incidence of pneumonia among 515 patients with dementia and PD who were randomized to either chin-down posture technique or two types of thickened fluids (nectar- and honey-thick consistencies) over a 3 month follow up period, at least one hospital admission was observed in 20% of each intervention arms [40]. Considering the complexity of managing PD, it is likely that a multimodal approach which addresses motor and non-motor complications, as well as palliatives aspects in end-stage disease, may be more effective compared to a single intervention approach [14, 42]. The risk of acute hospitalization seems to be more related with PD symptoms, proper care, medication adherence, and comorbidity than age, gender or disease duration [4, 42]. Both patients who were admitted and those who were not had a similar mean disease duration. However, in the model and after adjustment to covariates related to disease progression, longer disease duration was associated with a lower risk of hospitalization. Lower risk of falls in more advanced patients because they have limited walking or prioritized care towards those with a more recent diagnosis could explain these findings.
The most important limitation of this study is the fact that information about admission in 88 of 693 PD patients was not recorded (12.7%). However, this is a limitation observed in other prospective studies. Of 7,507 PD patients, follow-up data was available only for 4,680 participants (62.3%) [35]. Although hospital admissions or mortality cannot be ruled out in this group from our study (N = 88), there were no significant differences between this group and the rest of patients from the cohort with regards to age, disease duration, LEDD, and all the covariates included in the model (data not shown). A very important second limitation is that PD patients older than 75 years old were excluded from participation by COPPADIS study protocol [16], which is a major weakness because older patients with PD are more likely to have complex disease (cognitive impairment, high comorbidity, etc.) and falls. Other limitations are the bias toward early PD in this cohort, as we previously commented, and the lack of a control group. Moreover, falls diary, calendar, or postcard were not used [43] and a patient was considered to suffer from falls based on the interview conducted. On the contrary, the strengths of our study include the large sample size, the prospective longitudinal follow-up design, the fact that this analysis was “a priori” planned as one objective of the multicenter COPPADIS project [16], and the extensive clinical and demographic information recorded.
In conclusion, this study observes that acute hospital admission is not infrequent in PD patients, that the risk is higher in patients with different complication (such as dysphagia, motor fluctuations, dyskinesia, and greater motor disability and NMS burden), and that falls is an independent predictor of acute hospitalization in PD patients. Future prospective studies are required to identify other predictors of acute hospitalization in PD and, more interestingly, to evaluate the effectiveness of proposed interventions over them.
CONFLICT OF INTEREST
Santos García D. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Lundbeck, KRKA, Zambon, Bial, Italfarmaco, and Teva.
de Deus Fonticoba T: None.
Cores C. has received honoraria for educational presentations and advice service by Lundbeck and UCB Pharma.
Suárez Castro E: None.
Hernández Vara J. has received honoraria for advice service from Britannia, travel bursaries and educational grants from Abbvie, and has received honoraria for educational presentations from Abbvie, Teva, Bial, Zambon, Italfarmaco, and Sanofi-Genzyme.
Jesús S. has received honoraria from AbbVie, Bial, Merz, UCB, and Zambon and holds the competitive contract “Juan Rodés” supported by the Instituto de Salud Carlos III. She has received grants from the Spanish Ministry of Economy and Competitiveness (PI18/01898) and the Consejería de Salud de la Junta de Andalucía (PI-0459-2018).
Mir P. has received honoraria from AbbVie, Abbott, Allergan, Bial, Merz, UCB, and Zambon. He has received grants from the Spanish Ministry of Economy and Competitiveness [PI16/01575] co-founded by ISCIII (Subdirección General de Evaluación y Fomento de la Investigación) and by Fondo Europeo de Desarrollo Regional (FEDER), the Consejería de Economía, Innovación, Ciencia y Empleo de la Junta de Andalucía [CVI-02526, CTS-7685], the Consejería de Salud y Bienestar Social de la Junta de Andalucía [PI-0437-2012, PI-0471-2013], the Sociedad Andaluza de Neu-rología, the Jacques and Gloria Gossweiler Foundation, the Fundación Alicia Koplowitz, and the Funda-ción Mutua Madrileña.
Cosgaya M: None.
Martí MJ. received honoraria for advice and lecture from Abbvie, Bial, and Merzt Pharma and grants from Michael J. Fox Foundation for Parkinson Disease (MJFF): MJF_PPMI_10_001, PI044024; Fondo de Investigacuiones Sanitarias of Spain (FIS PI17/00096) and from Generalitat de Catalunya (AGAUR Exp 2017 SGR 1502).
Pastor P: None.
Cabo I. has received honoraria for educational presentations and advice service by Abbvie, Zambon, and Bial.
Seijo M. has received honoraria for educational services from KRKA, UCB, Zambon, and Bial; travel grants from Daiichi and Roche.
Legarda I. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Zambon, Bial, and Teva.
Vives B: None.
Caballol N. has received honoraria from Bial, Italfármaco, Qualigen, Zambon, UCB, Teva, and KRKA and sponsorship from Zambon, TEVA, and Abbvie for attending medical conferences.
Rúiz Martínez J. has received honoraria for educational presentations, attending medical conferences, and advice service by Abbvie, UCB Pharma, Zambon, Italfarmaco, Bial, and Teva.
Croitoru I: None.
Cubo E: Travel grants: Abbvie, Allergan, Boston; Lecturing honoraria: Abbvie, International Parkinson’s disease Movement Disorder Society.
Miranda J: None.
Alonso Losada MG. has received honoraria for educational presentations and advice service by Zambon and Bial.
Labandeira C. has received honoraria for educational presentations and advice service by Abbvie, Italfarmaco, Zambon, and Bial.
López Ariztegui N. has received honoraria for educational presentations and advice service by Abbvie, Italfarmaco, Zambon, and Bial.
Morales-Casado M. has received honoraria for educational presentations and advice service by Bial, Zambon, UCB, Ferrer and Fressenius-kabi.
González Aramburu I: None.
Infante J. has received travel bursaries and honoraria for educational presentations from Abbvie and Zambon.
Escalante S. has received honoraria for educational presentations and advice service by Abbvie, Zambon, and Bial.
Bernardo N: None.
Blázquez Estrada M. has received honoraria for educational presentations and advice service by Abbvie, Abbott, UCB Pharma, Allergan, Zambon, Bial, and Qualigen.
Menéndez M. has received honoraria for educational presentations by KRKA and Zambon.
Seijo M. has received honoraria for educational services from KRKA, UCB, Zambon, and Bial; travel grants from Daiichi and Roche.
García Caldentey J. has received honoraria for educational presentations and advice service by Qualigen, Nutricia, Abbvie, Italfarmaco, UCB Pharma, Lundbeck, Zambon, Bial, and Teva.
Borrué C: None.
Vela L. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Lundbeck, KRKA, Zambon, Bial, and Teva.
Catalán MJ: None.
Gómez-Mayordomo V: None.
Kurtis M. has received honoraria from Bial, the Spanish Neurology Society and the International and Movement Disorders Society.
Prieto C: None.
Ordás C: None.
Nogueira V: None.
López Manzanares L: Compensated advisory services, consulting, research grant support, or speaker honoraria: AbbVie, Acorda, Bial, Intec Pharma, Italfarmaco, Pfizer, Roche, Teva, UCB, and Zambon.
Ávila Rivera MA. has received honoraria from Zambon, UCB Pharma, Qualigen, Bial, and Teva, and sponsorship from Zambon and Teva for attending conferences.
Puente V. has served as consultant for Abbvie and Zambon; has received grant/research from Abbvie.
García Moreno JM. has received honoraria for educational presentations and advice service by Abbvie, Ital-Pharma, Lundbeck, Merz, KRKA, UCB, Pharma, Zambon, Bial and Teva.
Solano Vila B. has received honoraria for educational presentations and advice service by UCB, Zambon, Teva, Abbvie, and Bial.
Álvarez Sauco M. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Zambon, Bial, and Teva.
Carrillo Padilla F. has received honoraria from Zambon (SEN Congress assistance).
Martínez Castrillo JC. has received research support from Lundbeck, Italfarmaco, Allergan, Zambon, Merz, and Abbvie. He has also received speaking honoraria from AbbVie, Bial, Italfarmaco, Lundbeck, Krka, TEVA, UCB, Zambon, Allergan, Ipsen, and Merz.
Sánchez Alonso P. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Lundbeck, KRKA, Zambon, Bial, and Teva.
Gastón I. has received research support from Abbvie and Zambon and has served as a consultant for Abbvie, Exelts, and Zambon.
Kulisevsky J: (1) Consulting fees: Roche, Zambon; (2) Stock / allotment: No; (3) Patent royalties / licensing fees: No; (4) Honoraria (e.g., lecture fees): Zambon, Teva, Bial, UCB; (5) Fees for promotional materials: No; (6) Research funding: Roche, Zambon, Ciberned; Instituto de SaludCarlos III; FundacióLa Maratóde TV3; (7) Scholarship from corporation: No; (8) Corporate laboratory funding: No; (9) Others (e.g., trips, travel, or gifts): No.
Valero C. has received honoraria for educational services from Zambon, Abbvie and UCB.
de Fábregues O. has received honoraria for educational presentations and advice service by Bial, Zambon, Abbvie, KRKA, and Teva.
González Ardura J. has recieved honoraria for speking from italofarma, Krka, Genzyme, UCB, Esteve, Psyma iberica marketing research SL and Ferrer, course grant from Teva and travel grant from Merck.
López Díaz L. has received honoraria from UCB, Lundbeck and KRKA.
Martinez-Martin P. has received honoraria from Editorial Viguera and Takeda Pharmaceuticals for lecturing in courses; from Britannia for writing an article in their Parkinson’s Disease Medical Journal-Kinetic; and from the International Parkinson and Movement Disorder Society (MDS) for management of the Program on Rating Scales. Grants from the MDS for development and validation of the MDS-NMS.
Footnotes
APPENDIX 1. COPPADIS STUDY GROUP
Adarmes AD, Almeria M, Alonso Losada MG, Alonso Cánovas A, Alonso Frech F, Alonso Redondo R, Álvarez I, Álvarez Sauco M, Aneiros Díaz A, Arnáiz S, Arribas S, Ascunce Vidondo A, Aguilar M, Ávila Rivera MA, Bernardo Lambrich N, Bejr-Kasem H, Blázquez Estrada M, Botí M, Borrue C, Buongiorno MT, Cabello González C, Cabo López I, Caballol N, Cámara Lorenzo A, Carrillo F, Carrillo Padilla FJ, Casas E, Catalán MJ, Clavero P, Cortina Fernández A, Cosgaya M, Cots Foraster A, Crespo Cuevas A, Cubo E, de Deus Fonticoba T, de Fábregues O, Díez-Fairen M, Erro E, Escalante S, Estelrich Peyret E, Fernández Guillán N, Gámez P, Gallego M, García Caldentey J, García Campos C, García Moreno JM, Gastón I, Guillén Fopiani D, Gómez Garre MP, Gómez Mayordomo V, González Aloy J, González-Aramburu I, González Ardura J, González García B, González Palmás MJ, González Toledo GR, Golpe Díaz A, Grau Solá M, Guardia G, Hernández Vara J, Horta-Barba A, Idoate Calderón D, Infante J, Jesús S, Kulisevsky J, Kurtis M, Labandeira C, Labrador MA, Lacruz F, Lage Castro M, Legarda I, López Ariztegui N, López Díaz LM, López Manzanares L, López Seoane B, Lucas del Pozo S, Macías Y, Mata M, Martí Andres G, Martí MJ, Martínez Castrillo JC, Martinez-Martin P, McAfee D, Meitín MT, Menéndez González M, Méndez del Barrio C, Mir P, Miranda Santiago J, Morales Casado MI, Moreno Diéguez A, Nogueira V, Novo Amado A, Novo Ponte S, Ordás C, Pagonabarraga J, Pareés I, Pascual-Sedano B, Pastor P, Pérez Fuertes A, Pérez Noguera R, Planas-Ballvé A, Planellas LL, Prats MA, Prieto Jurczynska C, Puente V, Pueyo Morlans M, Redondo Rafales N, Rodríguez Méndez L, Rodríguez Pérez AB, Roldán F, Ruíz De Arcos M, Ruíz Martínez J, Sánchez Alonso P, Sánchez-Carpintero M, Sánchez Díez G, Sánchez Rodríguez A, Santacruz P, Santos García D, Segundo Rodríguez JC, Seijo M, Sierra Peña M, Solano Vila B, Suárez Castro E, Tartari JP, Valero C, Vargas L, Vela L, Villanueva C, Vives B, Villar MD
ACKNOWLEDGMENTS
We would like to thank all patients and their caregivers who collaborated in this study. Many thanks also to Fundación Española de Ayuda a la Investigación en Parkinson y otras Enfermedades Neurodegenerativas (Curemos el Parkinson; www.curemoselparkinson.org), Alpha Bioresearch (![]() ), and other institutions helping us.
), and other institutions helping us.