
Abstract
Background:
People with Parkinson’s disease (PwPD) are less active than their age-matched peers. Non-motor symptoms, specifically, deficient motivation, may influence decision-making for exercise due to the impaired mesolimbic dopaminergic pathway.
Objective:
The purpose of this study was to determine if effort-based decision-making for physical effort was different in PwPD compared to healthy controls. We sought to determine the relationship between effort-based decision making for exercise and a discrete motor task as well as the impact of components of motivation on decision-making for physical effort in PwPD.
Methods:
An effort-based decision-making paradigm using a discrete motor task (button pressing) and a continuous exercise task (cycling) was implemented in 32 PwPD and 23 healthy controls. Components of motivation were measured using the Apathy Scale and the Temporal Experience of Pleasure Scale- Anticipatory Pleasure scale.
Results:
The presence of Parkinson’s disease (PD) did not moderate decisions for either physical effort task. There was a moderate correlation between decisions for both tasks, within each group. The anticipation of pleasure and apathy were predictors of decisions for both physical effort tasks in PwPD, but not in healthy controls.
Conclusion:
PwPD responded similarly to effort and reward valuations compared to those without PD. Individuals were consistent in their decisions, regardless of the physical effort task. The anticipation of pleasure and apathy were significant predictors of decisions for exercise in PwPD only. Increased anticipation of pleasure, reduction of apathy, and the use of rewards may enhance engagement in high effort exercise among PwPD.
INTRODUCTION
The evidence revealing the effectiveness of exercise in the management of Parkinson’s disease (PD) is mounting [1, 2]. Exercise reduces motor symptoms, improves functional outcomes, and enhances quality of life in people with PD (PwPD) [3–8]. High-intensity exercise, requiring much effort, may be particularly important given the potential disease modifying effects [8–10]. Despite the known benefits of exercise, PwPD remain significantly less active compared with healthy older adults [11–16].
Although older age and worsening motor symptoms are known to contribute to lower engagement in exercise in PD [11–13, 18], non-motor symptoms, such as reduced motivation (i.e., apathy), may also impact decisions to engage in effortful behaviors like exercise [19–21]. Motivation is a complex construct that includes, among other things, the anticipation of pleasure, effort expenditure, and organized, goal-directed behavior. The anticipation of pleasure is an affective state connected to future activities and is required for many goal-directed behaviors [22]. It includes the expectation for a future event as well as the related reward associated with the experience [23]. Expenditure of effort is the behavioral output of motivation. When motivation for goal-directed behavior is reduced, it is labeled as the behavioral syndrome of apathy. Anticipatory pleasure and the behavioral aspect of motivation (expenditure of effort) are reduced when mesolimbic dopamine is depleted, as in PD [24, 25].
High effort exercise combined with less anticipation of a pleasurable reward may lead to rejection of physical effort and subsequent sedentary behavior. Anticipatory pleasure supports the preparation for goal directed behavior, moving one towards a desired outcome (i.e., approach motivation) [26]. Dopamine predominately regulates approach motivation and a decrease in this neurotransmitter, as seen in PD, may contribute to rejecting physical effort [25].
Effort-based decision-making paradigms serve to quantify levels of approach motivation [24, 25]. Effort-based decision-making is a cost-benefit valuation of weighing the effort involved (cost) versus the potential reward (benefit) for a certain course of action [27]. Within animal studies, effort (e.g., climbing over a barrier) is perceived as a “cost” and animals consistently attempt to minimize how much effort must be expended for a given reward (e.g., food) [27]. Humans with PD have been shown to expend lower levels of effort (e.g., slower movement) for rewards compared to aversive stimuli [28]. This indicates that despite having the ability to move faster, they are not responding similarly to rewards. Additionally, PwPD compared to healthy controls, were less responsive to rewarding stimuli [29]. In studies using discrete motor tasks (e.g., hand-held dynamometry, upper extremity reaching, keyboard button pressing), PwPD are less willing to exert physical effort for low rewards (e.g., monetary, points) compared to healthy controls, despite force production being similar [30, 31]. Conversely, effort-based decision-making in PwPD approximates that of controls under conditions of high rewards. However, these studies are limited to discrete motor tasks requiring low energy expenditure [30–32]. Exercise, unlike a discrete motor task, is a continuous, gross motor task with high energy expenditure.
Beyond the energy requirements for the task, the underlying neurological processes related to decision-making for physical effort may be the same despite differences in the physical task under consideration. This consistency may indicate that decisions, whether to engage in keyboard button pressing or cycling on a bike, are highly correlated. However, there are obvious differences between these two tasks that may create different effort and reward valuations and weaken the correlation.
In this study, we used an effort-based decision-making paradigm using a discrete motor task (button pressing) and a continuous exercise task (cycling) in 32 PwPD and 23 healthy controls to quantify approach motivation. Additional components of motivation were measured using the Apathy Scale and the Temporal Experience of Pleasure Scale- Anticipatory Pleasure scale. The aims of this study were three-fold: 1) to determine if effort-based decision-making related to exercise was different in PwPD compared to healthy age-matched controls; 2) to determine if components of motivation (apathy and the anticipation of pleasure) predict decision-making for physical effort in PwPD, controlling for the physical measures of age, walking capacity, and motor disease severity; 3) to identify if effort-based decision-making for a discrete motor task was correlated to effort-based decision-making for exercise in PwPD. We hypothesized that PwPD would have a higher likelihood of rejecting effortful exercise compared to healthy controls in a full-body exercise task and that anticipatory pleasure and apathy would be significant moderators of decisions for physical effort in PwPD. Finally, we hypothesized that effort-based decision-making for a discrete motor task would be moderately correlated with effort-based decision-making for exercise.
METHODS
Participants
In this cross-sectional study, a convenience sample of 32 people with idiopathic PD and 23 age and education-matched healthy controls (HC) participated. This study was approved by the Institutional Review Board at Boston University. Potential participants underwent a phone and in-person screening to determine eligibility. Those that met the criteria participated in one study session that included all testing procedures. Inclusion Criteria were 1) diagnosis of idiopathic PD according to the UK Brain Bank Criteria, 2) Hoehn &Yahr stages 1–3, 3) stable PD medications for at least 2 weeks prior to study entry. Exclusion Criteria were 1) significant cognitive impairment (Telephone Interview for Cognition Scale score of ≤30) [33, 34], 2) cardiac conditions that interfered with the ability to safely engage in exercise, 3) orthopedic conditions that limited the ability to cycle.
Study procedures
All participants provided written informed consent. Basic demographic information, resting vital signs (heart rate, blood pressure, oxygen saturation levels and Borg Rating of Perceived Exertion), and PD medications were collected. The Geriatric Depression Scale [35, 36] and the Physical Activity Scale for the Elderly [37, 38] were administered to characterize the sample. In persons with PD, all study procedures were implemented during the “on” medication state.
Effort-based decision-making tests
Participants completed two computer-based decision-making tests requiring a cost-benefit analysis for both a discrete fine motor task (keyboard button pressing) and for full-body exercise (stationary cycling). There was a rest period between these two tests. Each test ranged from approximately 5–10 min. The standard computer-based, binary choice paradigm of experimental decision-making, using the keyboard button pressing task (fine motor task), was used in this study [39]. This test is a modification of the Effort Expenditure for Reward Task (EEfRT) [40]. In addition, this paradigm was modified to use stationary cycling (full-body exercise). Stimulus presentation and response acquisition were performed using MATLAB R2013b (MathWorks) [41] with the Psychophysics Toolbox [42]. This effort-based decision-making paradigm required participants to weigh the cost (varying levels of effort required for keyboard button pressing or for stationary cycling) versus the benefit (varying levels of monetary reward) over a series of trials (Fig. 1). The stimulus prompted participants to choose between the effortful option for the presented reward, or the no effort option that always paid $1.00. Participants were specifically instructed to choose between these two effort and reward combinations based on their determination of whether the effort was worth the reward. The 36 reward presentations ranged from $1.00 to $5.73. There were six rewards of $1.00 and six rewards within each of the following ranges: $1.26–$1.71, $2.29–$2.73, $3.33–$3.74, $4.27–$4.65, $5.41–5.73. Each of these monetary values were combined with varying levels of effort required (low, medium, or high), for a total of 36 combinations. Participants had 3 s to select their decision before the next stimulus was presented.
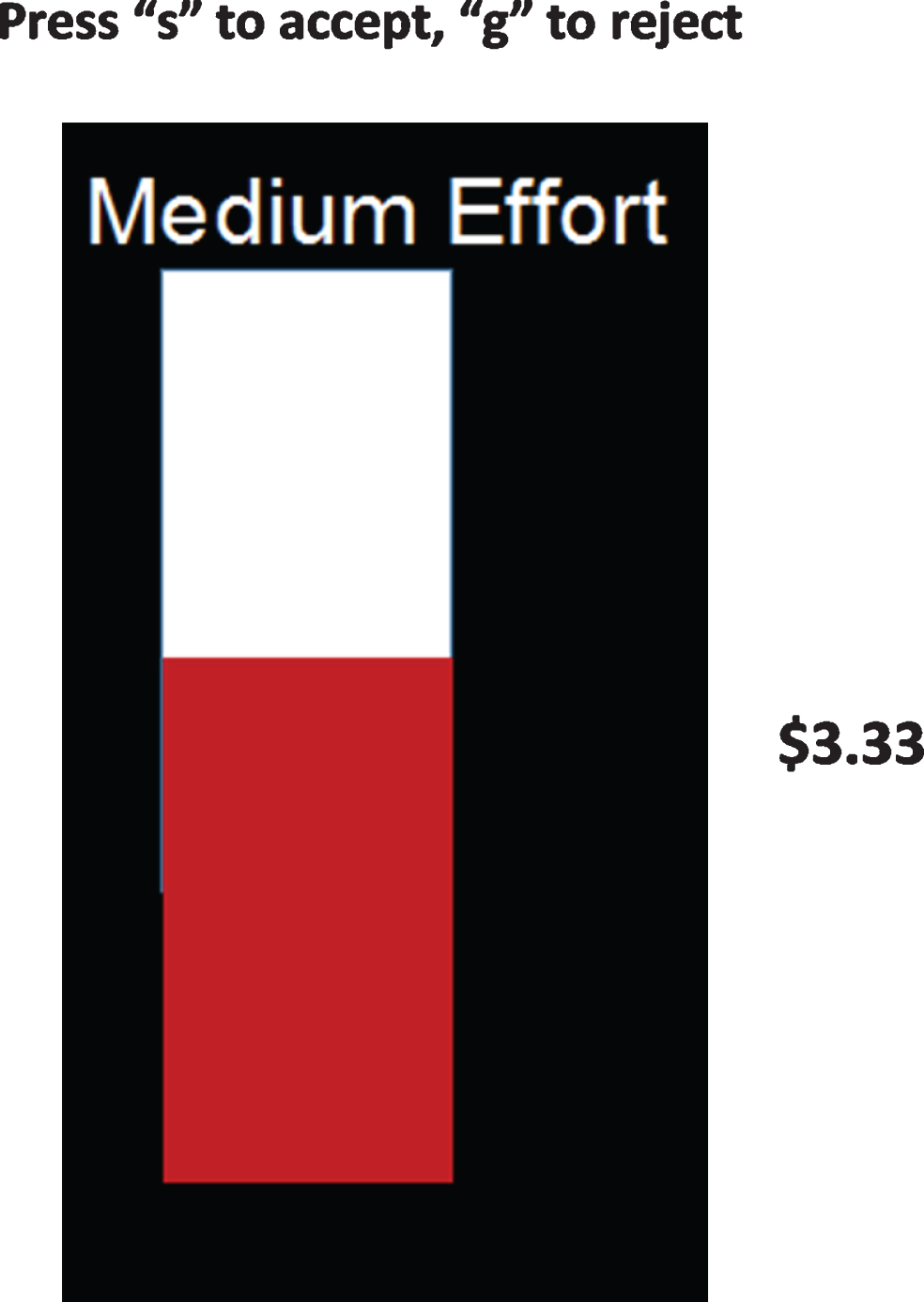
Computer screen image of one of the 36 decisions that participants consider in the effort-based decision-making test. Participants viewed the image of either low, medium or high effort on the computer screen simultaneously with a monetary reward amount. The image of effort was a display of a vertical bar that was partially filled (red area) and corresponded with the level of effort relative to maximum effort. Participants had 3 seconds to select by either pressing the “s” to accept the effortful option for the stated reward or “g” to reject the effortful option and receive $1.00.
Effort-based decision-making for a discrete motor task: keyboard button pressing
Participants engaged in a decision-making task involving pressing a keyboard button with their non-dominant fifth finger (Fig. 2). They were asked to decide if they were willing to press the keyboard button for up to 20 s at low, medium, or high effort for varying amounts of monetary reward.
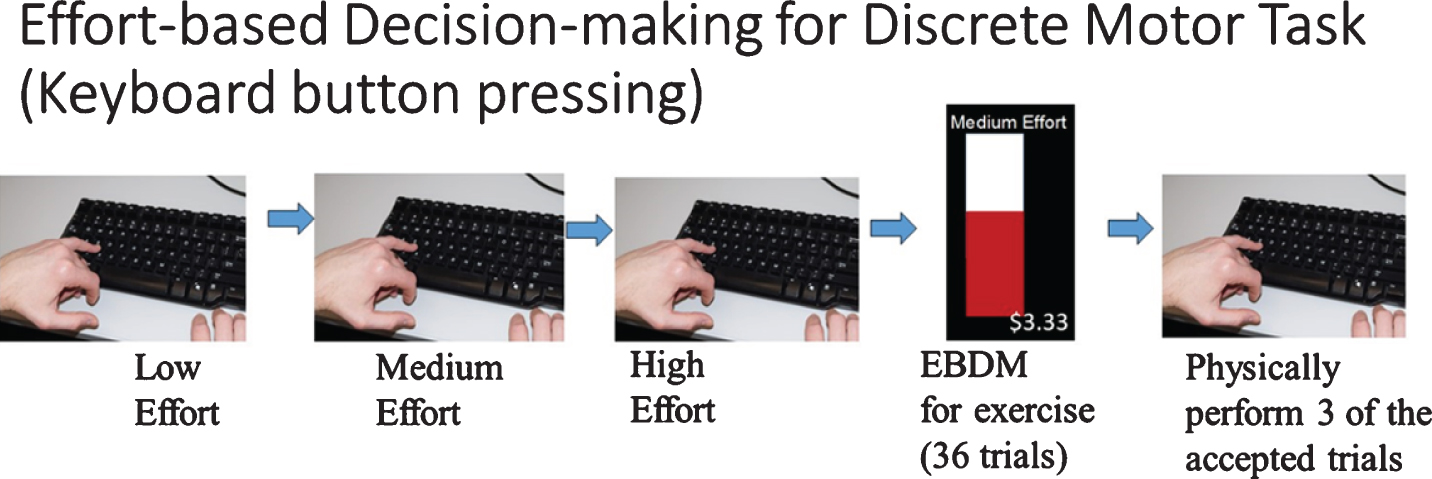
Effort-based decision-making for a discrete motor task. Button pressing capacity was established. Participants then practiced button pressing at low (20%), medium (60%) and high (100%) effort with 2 practice trail at each effort level. This practice familiarized participants with each effort level before engaging in decisions. Participants were then presented with 36 effort and reward combinations for them to decide “accept” or “reject”. Three of the selected trials were randomly selected for participants to physically complete to earn the associated monetary reward.
The low, medium, and high effort levels during the button pressing task were individualized to each participant’s ability. To determine individual effort levels, each participant was instructed to press a keyboard button with their non-dominant fifth finger as fast as possible for twenty seconds, three times. Baseline button pressing capacity was calculated by averaging these three trials. Low effort was achieving 20%of the average of the baseline trials in 20 s; medium effort was 60%, and high effort was 100%of their baseline capacity in 20 s. Participants experienced low, medium, and high effort button-pressing before engaging in decision-making. There were 36 trials of effort and reward combinations, each requiring a cost-benefit analysis and a decision (e.g. Would you be willing to press the “s” button with your non-dominant fifth finger at high effort for $1.26?). The reward and effort combinations were the same in both the button pressing test and the stationary cycling test.
Effort-based decision-making for exercise (full-body exercise): stationary cycling
Before making decisions about their willingness to engage in cycling for rewards, participants experienced 5 min of cycling at each effort level (Fig. 3) to calibrate between low, medium, and high effort. Participant’s cycling heart rate range was determined by using their age-predicted maximum heart rate (APMHR) [43] to calculate the targeted percentages to achieve each effort level. Borg’s Rating of Perceived Exertion (RPE) scale was assessed at rest and while cycling [44]. Individuals were instructed to cycle on a stationary bicycle for a duration of 5 min each at low effort (<50%of APMHR and less than 12 on the RPE), medium effort (50–60%of APMHR and/or 12-13 on the RPE scale), and high effort (65–75%of APMHR and/or between 14-15 on the RPE scale). When lower bounds of the target heart rate zone and/or the rating of perceived exertion were reached by each participant, they were instructed that they had reached the target effort zone. Then participants were given scripted verbal directions to maintain their effort at each level.
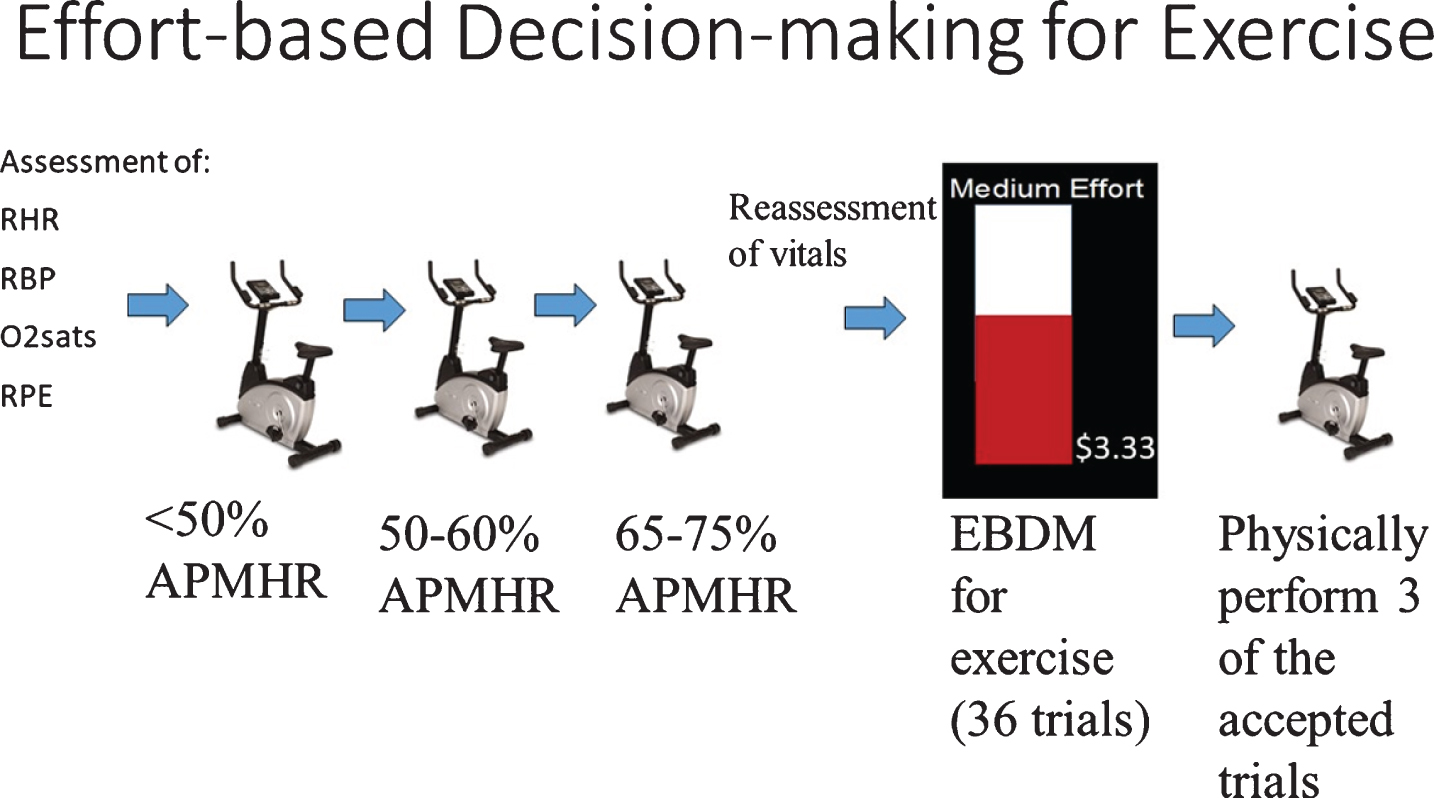
Effort-based decision-making for exercise. Assessment of resting heart rate (RHR), resting blood pressure (RBP), resting oxygen saturation levels (O2sats) and resting rating of perceived exertion (RPE) was completed. Age-predicted maximum heart rate (MHR) was calculated. Participants cycled for 5 min at low (<50%MHR), medium (50–60%MHR), and high (65–75%MHR) effort with rest periods between each 5 min of cycling to become familiarized with each effort level before engaging in decisions. Participants were then presented with 36 effort and reward combinations for them to decide “accept” or “reject”. Three of the accepted trials were randomly selected for the participant to physically complete to earn the associated monetary rewards.
While cycling, heart rates were continually assessed using Polar H10 heart sensors. RPE was assessed at baseline, after 2.5 min of cycling, and during recovery. Individuals’ effort levels were maintained at the target heart rate range and effort level by adjusting the resistance and/or revolutions per minute. Scripted verbal directions (e.g., after 2 min of cycling: “This is 2 minutes at medium effort”; after 4 min: “You have 1-minute left at the medium effort level”) were provided by the researcher to assist the participant in maintaining the effort level for 5 continuous minutes.
Participants first made 36 decisions (accept or reject) about their willingness to engage in the cycling task and then made 36 decisions about their willingness to engage in the button pressing task. The decision-making for cycling test was ordered first and was consistent among all participants. Participants were informed, prior to their decision-making, that three of their “accept” decisions for cycling and three of their “accept” decisions for button pressing would be randomly selected for them to complete. This was to ensure that participants understood that their decisions would be followed by completing some of the physical effort tasks that they agreed to. They were informed that they had the opportunity to win the monetary rewards associated with “accept” decision if they successfully completed the physical effort. In actuality, all participants earned a $35.00 gift card for their participation and were debriefed at the conclusion of all testing.
Covariates
The Movement Disorder Society-Unified Parkinson’s Disease Rating Scale, Part III, (MDS-UPDRS-III) is the gold-standard measure of Parkinson disease motor symptoms and was used to capture motor disease severity. It is a valid and reliable 18-item assessment of rigidity, tremor, posture, balance, and gait with higher scores indicating worse motor symptoms [45].
The fast Six Minute Walk Test (6MWT) is a measure of walking capacity. Individuals walked over-ground as fast as possible for 6 min and the distance walked was recorded [46]. Six minute walk distance is significantly correlated with parkinsonism characteristics, mobility, and balance in those with PD [47].
Predictor variables
The Apathy Scale (AS) is a valid, reliable, 14-item self-report questionnaire that measures generalized apathy, or decreased goal-directed behavior during daily activities [48, 49]. The score ranges from 0–42 with higher scores indicating higher levels of apathy or impaired motivation.
The Temporal Experience of Pleasure Scale-Anticipatory Pleasure (TEPS-ANT) is a valid and reliable 10-item self-report scale that measures trait tendencies for the anticipatory experience of pleasure [50]. Raters indicate levels of agreement with items such as, “When I think of something tasty, like a chocolate chip cookie, I have to have one.” This score ranges from 10–60 with low scores indicating anticipatory anhedonia, a lowered tendency to experience pleasure in anticipating events or experiences.
Data analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 24.0 [51] and Hierarchical Linear and Nonlinear Modeling (HLM) version 7.03 [52]. Descriptive statistics were calculated to characterize the sample and examine normality of distributions. Independent samples t-tests and chi-square tests were conducted to compare the groups on demographic variables and clinical assessment scales (PD vs. HC). Likelihood ratio testing was conducted to determine the justification for multilevel modeling. First, we analyzed group differences in decisions. Choices to exert physical effort, for both cycling exercise and button pressing, across 36 trials for varying amounts of monetary reward (accept or reject) was specified as the dichotomous outcome in a logistic multilevel model across groups. This model included effort required, reward amount, and trial number as random effects in Level 1 and group status (PD vs. healthy control) as a fixed effect at Level 2. Exploratory analyses were conducted to examine within-group predictors of decision-making in those with PD and HC. We examined the contribution of motivation after controlling for demographic and physical attributes (age, walking capacity (6MWT)), and motor signs (MDS-UPDRS III). Clinical measures of motivation, generalized apathy (AS) and the anticipation of pleasure (TEPS-ANT), were independently tested in models that explained decisions for physical effort. AS or TEPS-ANT were level 2, fixed effect predictors of overall choices. Unit-specific models with robust standard errors were used to estimate the effects in these analyses. The unit-specific model provides odds ratios that are a function of each unit’s individual cluster probability which provides information at the individual level [53]. Significance was set at p is less than or equal to 0.05.
RESULTS
PD and HC participants were middle-aged to older adults who were not clinically apathetic or depressed, had normal age-related walking capacity, and were moderately physically active. Individuals with PD were in Hoehn & Yahr (H&Y) stages 2 and 3 (Table 1). There were no significant differences in age, education, gender, anticipation of pleasure (TEPS-ANT), or walking capacity (6MWT) between the two groups.
Participant Demographics & Clinical Assessments
Mean (SD) except where noted as frequency; ↑+, Higher scores are positive; ↑-, Higher scores are negative; 6MWT, Six-minute Walk Test; AS, Apathy Scale; GDS-S, Geriatric Depression Scale-Short form; HC, healthy controls; H&Y, Hoehn & Yahr; LED, Levodopa Equivalent Dose; PASE, Physical Activity Scale for the Elderly; PD, Parkinson’s disease; TEPS-ANT, Temporal Experience of Pleasure Scale-anticipatory pleasure scale; MDS-UPDRSIII, Movement Disorder Society- Unified Parkinson’s Disease Rating Scale-Part III.
Group differences in decisions for physical effort
Group status (PD vs. HC) was not a significant predictor of choices to exert physical effort (group status on cycling response: β= 0.15, p = 0.74; group status on button pressing response: β=–0.62, p = 0.33)). Group also did not moderate the impact of reward amount, effort required, or trial number on choices. The mean acceptance of effort was not significantly different between groups for cycling or button pressing (cycling, PD = 65.97%, HC = 64.37%, p = 0.76; button pressing, PD = 59.08%, HC = 60.60%, p = 0.78).
Impact of apathy on decisions for button pressing
The fixed effects of age, UPDRS, AS, and 6MWT were entered into the model (Supplementary Table 1). Age, reward, effort, and trial (one singular experience within the 36 items of the decision-making test) were significant predictors of decisions for button pressing for PwPD. Increased age, effort, and trial decreased the likelihood of accepting effort (for every one-year increase in age, the odds of deciding “accept” to button pressing was decreased by 16.1%; for every one level increase in effort, the odds of deciding “accept” to button pressing decreased by 99.9%; for every one level increase in trial (e.g., trial 2 to trial 3) the odds of deciding “accept” to button pressing decreased by 2.5%, holding all other factors constant). Increased reward increased the likelihood of accepting effort (for every increased level of reward, the odds of deciding “accept” to button pressing was increased by 361.4%, holding all other factors constant). The coefficient suggested that the impact of AS on decisions was in the expected direction, though not statistically significant. MDS-UPDRS III and 6MWT did not significantly predict decisions. In healthy controls, age, reward, effort, and trial were significant predictors of decisions for button pressing; however, AS and 6MWT did not significantly predict decisions in those without PD (Supplementary Table 1).
Impact of anticipatory pleasure on decisions for button pressing
In a multilevel hierarchical logistic regression model to analyze decisions for a discrete motor task (button pressing) in PwPD, the fixed effects of age, MDS-UPDRS-III, TEPS-ANT, and 6MWT were entered into the model at level 2 (Supplementary Table 2). Age, TEPS-ANT, reward, effort, and trial were significant predictors of decisions for button pressing. Increased age, effort, and trial decreased the odds of agreeing to expend effort for button pressing (for every 1 year increase in age, the odds of deciding “accept” to button pressing decreased by 15.3%; for every one level increase in effort, the odds of deciding “accept” to button pressing decreased by 99.9%; for every one level increase in trial (e.g., moving from trial 2 to trial 3), the odds of deciding “accept” to button pressing decreased by 2.5%, holding all other factors constant). Increased anticipation of pleasure and rewards increased the odds of agreeing to effort (for every 1-point increase in TEPS-ANT, the odds of deciding “accept” to button pressing was increased by 21.6%; for every increased level of reward, the odds of deciding “accept” to button pressing was increased by 365.1%, holding all other factors constant). The 6MWT and MDS-UPDRS III did not significantly explain decisions. In healthy controls, age, reward, effort, and trial were significant predictors of decisions for button pressing; however, TEPS-ANT and 6MWT did not significantly predict decisions in those without PD (Supplementary Table 2).
Impact of apathy on decisions to exercise
In a multilevel hierarchical logistic regression model, engagement in exercise among those with PD was significantly influenced by reward and effort. Reward, effort, and trial were significant predictors of effort choices for cycling (Table 2). As reward values increased, the odds of agreeing to exercise increased; as effort amount and trial number increased, the odds of agreeing to exercise decreased (for every increased level of reward, the odds of deciding “accept” to cycling was increased by 188.1%; for every one level increase in effort, the odds of deciding “accept” to cycling decreased by 97.1%; for every one level increase in trial number, the odds of deciding “accept” to cycling decreased by 2.9%).
Hierarchical Logistic Regression model explaining choices for cycling exercise in people with PD and healthy controls: generalized apathy
*significant at p≤0.05, **significant at p < 0.001; ↑+, Higher scores are positive; ↑-, Higher scores are negative; 6MWT, Six Minute Walk Test; AS, Apathy Scale, MDS-UPDRS III, Unified Parkinson’s Disease Rating Scale, part III.
Age and AS were significant fixed effects predictors of effort choices. As age and apathy scores increased, there was a decreased likelihood of accepting exercise (for every 1-year increase in age, the odds of deciding “accept” to cycling decreased by 7.5%; for every 1-point increase on the AS, the odds of deciding “accept” to cycling decreased by 13.3%). The 6MWT and MDS-UPDRS III did not significantly explain choices for exercise. In healthy controls, age, AS, or 6MWT did not explain effort choices; reward, effort, and trial, however, did explain choices (Table 2).
Impact of anticipatory pleasure on decisions to exercise
The anticipation of pleasure was a significant predictor of decisions in PwPD (Table 3) (for every 1-point increase in TEPS-ANT, the odds of deciding “accept” to cycling was increased by 17.2%). Additionally, age, reward, effort, and trial were significant predictors of decisions for cycling in this population, while holding all other factors constant. Scores on the 6MWT and MDS-UPDRS III were unrelated to decisions to exercise. In healthy controls, age, TEPS-ANT, or 6MWT did not explain choices; reward, effort, and trial, however, did explain choices (Table 3).
Hierarchical Logistic Regression model explaining choices for cycling exercise in people with PD and healthy controls: anticipatory pleasure
*significant at p≤0.05, ** significant at p < 0.001; ↑+, Higher scores are positive; ↑-, Higher scores are negative; 6MWT, Six Minute Walk Test; TEPS-ANT, Temporal Experience of Pleasure Scale-anticipatory pleasure scale, MDS-UPDRS III, Unified Parkinson’s Disease Rating Scale, part III.
Correlations of decisions across tasks
In PwPD, decisions that were made for button pressing and cycling were significantly correlated (Spearman’s rho = 0.562, p < 0.001). In healthy controls, decisions for both tasks were also significantly correlated (Spearman’s rho = 0.603, p < 0.001).
DISCUSSION
We examined decisions related to engaging in physical effort for both a discrete motor task (button pressing) and in a continuous exercise task (cycling), in PwPD and healthy controls. We found that overall choices to exert effort for exercise were similar between PwPD (on dopamine replacement therapy) and controls. However, there was significant within-group variation (between-person variance) in individual responses in PwPD. Specifically, we found that two separate components of motivation—apathy and anticipatory pleasure—predicted decisions to engage in exercise in PwPD, but not in healthy controls. Importantly, these associations held after adjusting for the contributions of age, walking capacity, and motor disease severity.
There is a paucity of studies in PD examining the contribution of motivation on engaging in exercise despite the high prevalence of motivational deficits [20, 55]. Our findings are consistent with prior work showing an association between apathy and self-reported physical activity in PwPD [55]. We also found a significant relationship between decisions for physical effort and the anticipation of pleasure (TEPS-ANT), suggesting that higher levels of anticipation of pleasure were related to a greater tendency to choose effortful exercise. This effort-based decision-making task provides quantitative information related to the general assessment of apathy as well as the anticipation of pleasure providing a more comprehensive assessment of motivation than either self-report measure alone.
Dopamine deficiency in PD, especially in the mesolimbic pathway, may decrease approach motivation. Our sample consisted of PwPD with varying disease durations and varying dopamine replacement doses leading to variability in components of approach motivation as measured by the apathy and anticipation of pleasure scales. This may explain why we saw greater variability in scores related to the anticipation of pleasure in PwPD than in controls. Apathy and the anticipation of pleasure were not predictors of decisions in healthy controls. Individuals with PD who are experiencing high apathy and/or low anticipation of pleasure may be less likely to engage in exercise. However, as rewards increased, there was an increased likelihood of choosing exercise, suggesting a potential treatment strategy to increase engagement in exercise in those with PD. This suggests that clinicians may consider the use of computer applications that track exercise and provide rewards with points, social approval (e.g., thumbs up, happy face, etc.) or reinforcing positive graphics (e.g., closing a circle or fireworks when a goal is achieved) to increase engagement.
Our hypothesis that there would be group differences in effort-based decision making for effort choices for exercise was not supported [30, 31]. The composition of our convenience sample, which included relatively active PwPD in the early to moderate disease stage, may partially explain the lack of group differences. Our sample of PwPD had a mean PASE score that exceeded reports of average scores for community dwelling adults without PD, revealing a physically active cohort that may be more likely to exert effort for exercise [38]. More than half of our sample was in the early stages of the disease, with presumably less dopamine deficiency, which could minimize differences in decision-making between the two groups. Prevalence of depressive symptoms (PD = 19%, HC = 9%in our sample) were not statistically different between the groups, despite estimated rates of 35%in PwPD [56] and 9%in healthy older adults in the population [57]. In addition, our sample had low scores on the Apathy Scale, potentially underestimating the effects of apathy and willingness to exert effort for exercise. Another potential reason for the lack of group differences is that benefits of exercise may be perceived as an additional reward (i.e., general health benefits, disease management), thereby elevating the overall reward for the task. Prior research has shown that when rewards are high, PwPD, who are on dopaminergic replacement therapy, have similar or increased acceptance of effort compared to controls [30].
Consistent with our hypothesis, effort-based decision-making for exercise was correlated with effort-based decision making for a discrete motor task in both PwPD and healthy controls. This indicates that there is a significant relationship between both decision-making processes despite differences in energy expenditure between the discrete and continuous physical effort tasks. Therefore, effort-based decision-making tasks, using a discrete motor task, may be generalizable beyond the task at hand. A simple button-pressing task may be able to relay information about decisions for exercise.
There are several study limitations. The difference in the cardiovascular demands between the physical effort tasks limited our ability to precisely match effort across the tasks. It is unclear if these effort levels are equivalent across the two different tasks. Additionally, it is possible that more vigorous aerobic exercise (80–85%of APMHR), which is beyond what was tested in this study, may influence the results, and should be examined in future studies. Furthermore, we considered a limited number of covariates given our small sample size. It is plausible that other non-motor signs, including depression, have important relationships with engagement in exercise. The order of EBDM tests was consistent; therefore, we are unable to determine if the order of the tests had an influence on the results. Finally, our sample encompassed persons with mild to moderate PD. These results may not generalize to those with greater disease severity with more significant dopamine deficiency.
CONCLUSIONS
In conclusion, we found that PwPD with relatively low levels of apathy and depression have similar effort-based decision-making for exercise and fine-motor tasks when on dopamine-replacement medications compared to healthy peers.
Correlations were present between effort-based decision-making for both types of physical effort in both PwPD and healthy controls. Apathy, the anticipation of pleasure, and age had a significant influence on decisions to engage in exercise in PwPD but not healthy controls. Rewards increased the likelihood of accepting exercise and greater effort levels decreased the likelihood of choosing exercise in those with and without PD. Due to the known benefits of high effort exercise [8, 59] future studies should examine the use of high rewards to sustain engagement with high intensity exercise. Future research should also examine the relationship between effort-based decision-making and objectively measured exercise and physical activity outside of the lab environment.
CONFLICT OF INTEREST
The authors declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
ACKNOWLEDGMENTS
The authors wish to extend sincere gratitude to all of the participants in this study. Thank you to physical therapists, Maggie Delaney and Taylor Cole, and research assistant, Skylar Shumate, for their assistance with recruitment and data collection. Thank you to Maria Iennaco and Marriah Warren for their assistance with MATLAB coding.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dudley Allen Sargent Research Fund [grant number 9250001170].