
Abstract
Background:
People with Parkinson’s disease suffer from a range of various symptoms. Altered movement patterns frequently represent the prevailing symptom experience and influence the everyday life of the affected persons.
Objective:
This qualitative study explores how persons with Parkinson‘s disease experience everyday life with a complex symptom profile and how they manage the consequential challenges in their daily life, as well as the motivation and consequences of these coping behaviours.
Methods:
Thirty-four patients with Parkinson’s disease were interviewed as an integrated part of the method Video-based Narrative. The interviews were analysed by means of qualitative content analysis according to Graneheim & Lundman.
Results:
The analysis identified six predominant coping types with different behavioural traits: The convincing behaviour, The economizing behaviour, The encapsulating behaviour, The evasive behaviour, The adaptable behaviour, and The dynamic behaviour. The strategies embedded in each of the six types are diverse, but all participants seek to maintain their integrity in different ways leading to the main motivation “To stay the same person”.
Conclusion:
Healthcare professionals should be aware of the patients‘ various coping behaviour in order to offer a person-centred approach. Psychoeducational interventions to promote coping skills may be essential in incorporating disease-related changes in the conduct of everyday life with Parkinson’s disease to maintain integrity.
Keywords
INTRODUCTION
In 2018, Parkinson’s disease (PD) was rated as the most frequent neurodegenerative movement disorder with an age-specific increase [1]. PD patients can experience a range of symptoms such as the classical triad of motor symptoms (tremor, bradykinesia, and rigidity) and non-motor symptoms (autonomic, affective, and neuropsychiatric disturbances). After some years of treatment, the “honeymoon” phase, which refers to the stage when motor symptoms are largely reduced by dopaminergic treatment, usually ends [2]. The decreasing effect of medication leads to fluctuations in symptom severity, loss of physical capacity and subsequently loss of control [3, 4]. How these consequences influence life with PD and how PD patients cope with these aspects has not been fully examined, but it may be a multi-factor interplay between personality traits, physical condition, psycho-social factors, symptom profile and other mediators embedded in everyday life with PD [5, 6].
As the disease progresses and an increase in symptoms and fluctuations occurs, the ability to perform activities of daily living (ADLs) become more and more affected [6]. The decline in ability to perform ADLs also limits the patients’ ability to maintain a “normal life” [7, 8]. Qualitative literature shows that PD patients in medium and advanced stages experience symptoms that affect aspects of everyday life such as social life, sense of control, and independency [3, 9]. However, most PD patients strive to live as normal a life as possible, and they use a variety of coping strategies to manage the symptoms of PD and their impact on everyday life [10, 11]. Reduced mobility, pain, postural instability, fatigue, anxiety, depression, and giving up previously enjoyed activities are some of the most resilient challenges [8]. Specific coping strategies seem to be associated with bodily discomfort, decrease in quality of life (QoL), depression and risk of mortality [5, 11]. This emphasizes that coping is an essential factor in the improvement of both the affective and psychosocial adjustment to PD [12–14]
Coping may be defined as changing cognitive and behavioural responses to dealing with specific external and/or internal demands that are conside-red to exceed the resources the individual possesses during handling the challenges [15]. Traditionally, the assessment of an individual’s coping behaviour is based on psychological components, but little is known about if and how these psychological compon-ents shape particular types of coping when managing PD. It may involve a range of components as described by Navarta-Sánchez et al., who recommend multidisciplinary psychoeducational interventions with the aim to strengthen and improve coping skills [16]. A scientific approach with involvement of multi-dimensional components such as physiological, affective, and psycho-social factors seems to be relevant in both the evaluation and identification of coping strategies. Furthermore, a scientific approach in the analyses of developmental pathways of coping may be based on integration of individual differences, degree of acceptance and self-efficacy [12, 17]
The literature within coping in PD shows that two main strategies dominate: Emotion-focused coping is associated with less constructive coping as it only changes the emotional perception of the situation. Problem-focused coping is based on plan-full problem solving and studies have demonstrated that problem-focused coping is associated with a higher QoL, although patients with PD use features of both types of coping strategies to manage daily life [5, 11]. It remains unclear if an identification of coping types in patients with PD can serve as a predictor of the impact on psychosocial and affective factors in daily life with PD.
Knowledge about PD patients’ coping behaviour provides insight into the complex life with PD and how coping behaviour may be influenced by both motor symptoms as well as non-motor symptoms such as cognitive consequences of the pathology. Clinically, it would be of interest whether an identification and differentiation of predominant coping types may enable health professionals to tailor the support and/or treatment of patients with PD. Hence, a better understanding of coping strategies could lead to an individualization of opportunities and rehabilitation services, and an improvement in psychosocial adjustment to PD.
Consequently, the aim of this study was to ex-plore how persons cope with living with PD in their everyday life and to identify predominant coping types.
MATERIALS AND METHODS
Design
This qualitative study is the second sub-study of a convergent mixed methods study. Prior to this study, we made a quantification of the ADL-level based on accelerometer-measurements [18]. In the final and third sub-study, we will identify clinical markers on each pre-dominant coping type identified in this present study. The sample in all three sub-studies consists of the same individuals.
Participants
Thirty-four patients with PD were included in the study and recruitment was executed by a two-way gate; consecutively from the neurological outpatient clinic for Movement Disorders at Zealand University Hospital, Denmark, and from the Danish Parkinson Association (Fig. 1). The goal was to recruit a cohort of 30–35 patients. As there were no previous studies that allowed for more detailed power calculation, the sample size was based on previous experience in similar studies [19, 20].
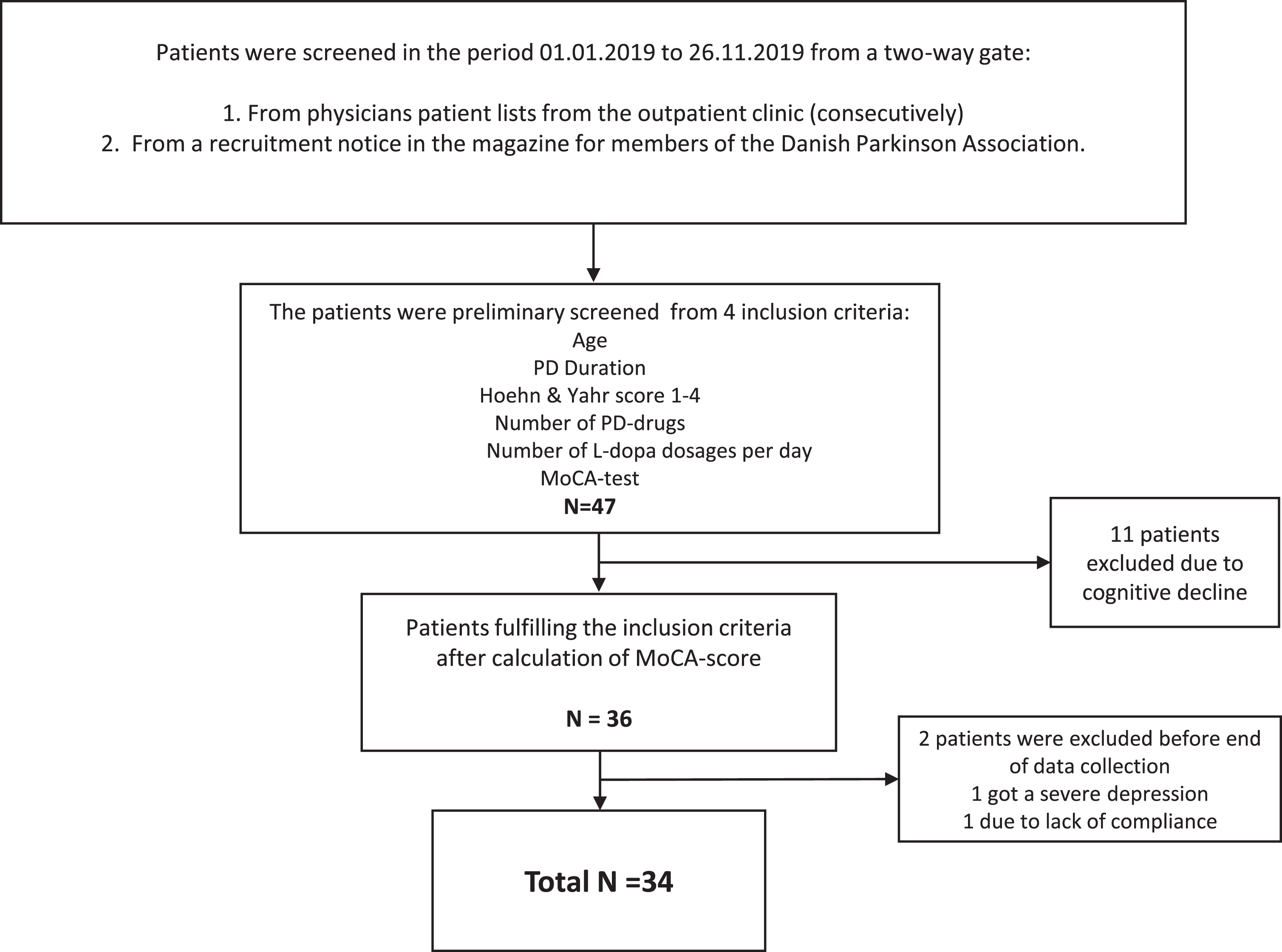
Flowchart of the recruitment and inclusion of participants.
All eligible patients with PD were screened based on following criteria: fulfilling the Movement Disorder Society diagnostic criteria [22], age of 50–75 years (mean age of PD diagnosis time), and PD duration of 3–7 years to capture the behaviour of patients in a possibly therapeutic balance within the “honeymoon” phase [4]. Further, the inclusion criteria were mild to moderate PD (Hoehn and Yahr scale 1–4), and non-dementia based on a cut off score >26 in The Montreal Cognitive Assessment (MoCA) to avoid severe cognitive declines [22]. A limitation of numbers of PD drugs (minimum of 1 and a maximum of 3) and number of daily doses (max of 4) was set. Exclusion criteria were patients with advanced treatments, dementia, and severity in co-morbidity (cut off <5, assessed in the Charlsson Co-morbidity Index). All potential participants accepted to participate in the study. Characteristics of the participants are presented in Table 1.
Baseline demographics and characteristics for the participants
Data collection
The study draws on qualitative research carried out from February 2018 to April 2019. Data were collected on all 34 participants in an identical sample [23]. In the first sub-study the participants were monitored with an accelerometer (Parkinson Kineti Graph™ (PKG) [24] providing measurements of the severity of the motor symptoms (tremor, bradykinesia, dyskinesia) and fluctuations [24]. These mea-surements also allowed the investigator to identify at which time period during the day the participants were less capable to perform ADLs and to which cause. The participant then identified the most bothersome ADLs in these periods and selected two ADLs to be video recorded.
Video-based narratives (VN)
VN was chosen as method to stimulate the patient’s ability to narrate based on a concrete situation and with the feelings associated during the ADLs. PD patients may have different perceptions of their appearance and physiological capacity than the surroundings, and therefore VN can be useful within this patient group [25]. Each participant in the study agreed to two home visits by the investigator (first author). Within the first visit the patients were video recorded during two ADLs. These ranged from gardening, cooking, cleaning, showering, dressing, texting on a smartphone, handling cutlery, walking, changing sheets and writing. The recordings lasted on average 3–8 minutes.
In the second visit, semi-structured interviews were performed with each participant describing the-ir experiences with challenges in everyday life after having seen themselves perform the selected ADLs on video reflecting the method of VN [25]. In order to secure privacy and to give participants the possibility to speak freely, spouses or caregivers were asked to leave the room/house when the interviews were conducted. An interview guide, with the involvement of both physiological, psycho-social, affective, cognitive and autonomic components to uncover aspects of daily life with PD, was used (Supplementary Table 1). The guide was tested and adjusted after feedback from three PD patients prior to the data collection. The interviews lasted approximately 45–55 minutes. They were saved as audio files and transcribed verbatim.
Ethical considerations
All participants received both oral and written information regarding the study’s aim, confidentiality issues and their rights to withdraw from the study without consequences of their further treatment. This was done in strict compliance with the ethical guidelines of the Declaration of Helsinki [26]. All participants signed a form of informed consent to participate in the project and also to the video-recording of two ADLs being performed by the participant. The Danish Data Protection Agency (REG-110-2017) and the Regional Committee on Health Research Ethics (IRB 58638) approved the project.
The essence of VN lies in the element of self-observation, which might be overwhelming and un-pleasant for the participants, especially in terms of violating the patients’ integrity [25, 27]. Most of the patients in this study were very surprised when seeing themselves on video, and different reactions appeared. Subsequently, a debriefing with the patients was accomplished to avoid psychological distress and take the participants vulnerability into account [25]. The participants were also offered a follow-up conversation with a neuropsychologist involved in the study, but none of the participants had the need for it.
Data analysis
The software program NVivo12 was used to structure the components in the analysis and created a visual overview of data.
Qualitative content analysis (QCA)
Data was analysed using QCA. The iterative process and the structure embedded were inspired by Graneheim & Lundman due to their step-by-step method of analysis [28, 29].
After each interview was conducted, an initial coding in a “data-tree” in NVIVO12 of emerging co-des was performed to get an overview [28]. After 31 interviews were conducted, new codes no longer appeared. The last three interviews were still performed to ensure variance [29]. When all the interviews were completed and transcribed the analysis was conducted in triangulation between three of the authors. The text was re-read and the audio files were re-listened several times with the aim of getting a sense of the underlying meaning. The preliminary impressions and findings were written down in a mind-map in NVivo.
Deductive forming of data
The QCA was built around different phases with both an inductive and deductive approach, and was synthesized in an abductive approach [28]. Four domains of coping identified in patients‘ narratives using VN by Jørgensen et al [27] were used as a lens to frame our analysis in a preliminary deductive phase grouping the codes into:
Inductive coding
The analysis consisted of examining the meaning units for patterns, similarities and differences, and the codes labelled each meaning unit in line with an inductive approach [29]. To get a sense of the underlying meaning in the text, the context of the interviews (noticing silence, sighs, laughter, posture etc. and the home environment in general) was also included.
The development of main categories
Guided by the codes, the text was further structured into sub-categories based on their commonalities. In NVivo12, different queries were made to identify the similarities and variations regarding content and coding-categories within the sub-categories. The sub-categories were compared and sorted into broader categories that were related to each other through their content or context but describing different aspects. Consequently, a pattern of different categories began to emerge.
The main categories were extracted from the categories expressing commonalities and similarities within the categories. Mind maps and other features from NVivo12 were used in this process. Six main categories were finally revealed by letting the data shape the categories into narrow, itemized typologies. These main categories constituted the base for the development of predominant coping types. Table 2 illustrates an example of the analysis process extracting one of the main categories. A more in-depth overview of the analysis process is presented in Supplementary Table 5.
Text matrix illustrating the process in extracting the main category “To stay under the blanket”
Numbers in parentheses refer to the participant.
RESULTS
The analysis of the data revealed six predomi-nant coping types. These are described on the basis of behavioural traits, where the main-categories (described in the parentheses) reflects the characteristic perspective on life: The convincing behaviour (To be your own project), The economizing behaviour (Always be a step ahead), The encapsulating behaviour (To stay under the blanket), The evasive be-haviour (To live in “free spaces”), The adaptable behaviour (Enjoying life no matter what), and The dynamic behaviour (To look PD in the eyes).
The classification of the 34 participants into the predominant coping types was based on their specific behaviour and motivation. Descriptive and clinical data were also included in the characterization of the groups (Table 3). Additionally, by going through the video recordings after the classification of the behaviour into typologies, it seemed that the choice of ADLs differed between the pre-dominant coping types.
Characterization of the classified six pre-dominant types
To stay the same person
It was not intended that an overall theme should be identified, but throughout the analysis a recurring theme labelled “To stay the same person” was dominant.
The protection of integrity was the underlying motivation behind the differences in behavioural strategies. Different aspects were reflected in the protection, and both physical, existential and psychosocial dimensions were revealed and captured in statements such as:
“Because I want to be who I was, the old me, I do not want to be the one they take into account, or the one who changes completely or something like that. For as long as possible, I will remain who I am ... ” (C4).
“Well you feel like a stranger in yourself, you know, you come to the feeling of not “being home”, you are home, but yet, I am a stranger. It is the same with the disease and myself ... in some way you have to re-build yourself” (C12).
Description of the six predominant coping types
The extraction of the predominant coping types are illustrated in Fig. 2 presenting core features within each step of the analysis process.
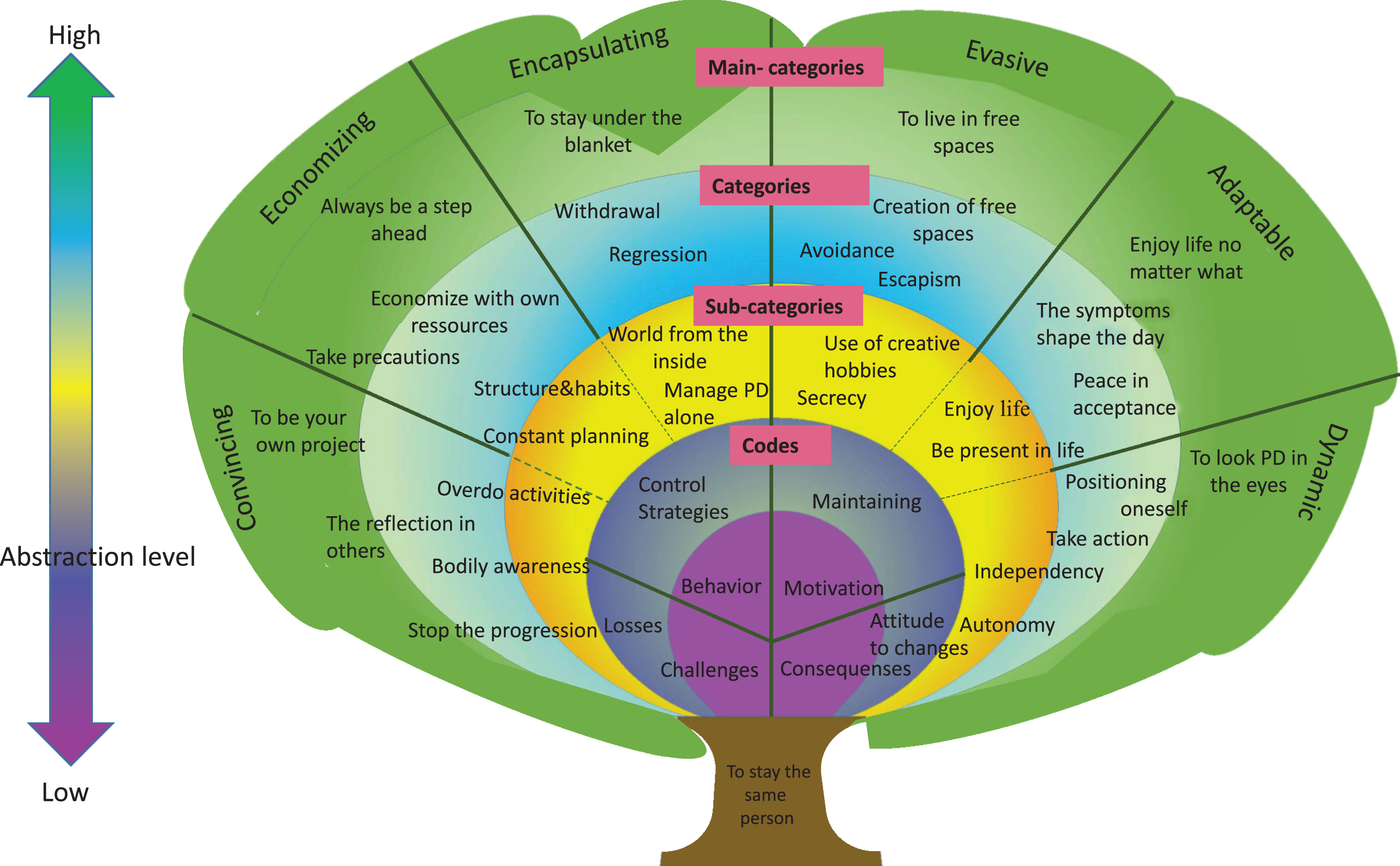
Overview of the analysis process with different abstraction levels starting with the four domains: Challenges, Behaviour, Motivation and Consequences.
Although there were intermittent references to other strategies and similarities between the predominant coping types within the sub-categories (yellow zone), an emerging specification began by letting the data drive the compiling of sub-categories into categories (blue zone) and further on into main categories (green zone). The use of colours illustrates the movement from the generic to the specific, from coding to the extraction of pre-dominant types in line with an inductive approach and with changing abstraction-level.
In general, it seems that the greatest challenge in daily life with PD is the variety of losses, such as loss of abilities, loss of control, loss of freedom, loss of identity, loss of intimacy, etc. that occur. It was difficult to extract generic features regarding the behaviour as it seems to be extremely dependent on the individual participant and reflects the variety in both symptom profile and strategies to overcome life with PD. However, the behaviour to manage the challenges seems to be dominated by an underlying need for staying in control. The motivation behind these control strategies focuses on maintaining life as it was, e.g., role in family, status, independence, and autonomy. Regardless of coping type and the behaviour embedded, every individual strived to stay the same person, but at the same time, they had to face constant changes. Different attitudes to these changes reflect the consequences of the behaviour.
The convincing behaviour
The main category “To be my own project” re-flected different perceptions regarding coping with PD that were interpreted as a convincing type. Data show that the individuals in this group have a high degree of bodily awareness and experiences a constant threat against identity and self-image. They need social interactions to reflect themselves to feel normal. As a result, they push their physical capability to maintain a level of daily activities as a healthy person and to maintain the same person. An underlying urge of convincing others (and oneself) of being able to perform as always is very important to them, and a key element of obsession/duty is reflected in this type as stated by C27: “I have high demands to myself ... it affects me every day. ... I want to be able to do things I could before, as much as possible”. The motivation behind this behaviour is to stop the progression of PD and maintain bodily functions. Consequently, every day is a fight against the progression of PD, where daily training schedules are made, and it becomes a project to manage PD.
The economizing behaviour
The economizing behaviour is expressed in the main category “Always be a step ahead”. Data show that for individuals in this group, everyday life is built around the physical disabilities. Within the economizing behaviour it is very important to preserve regular habits and routines, which is related to an underlying fear of standing out and losing control. In terms of social activities, travels, and daily activities the economizer predicts what might happen in any case as illustrated in this quote: “You have to be prepared of what might happen if you do not want to get in uncomfortable situations” (C18). The key words are pragmatism and alignment of challenges, and therefore every activity is adjusted after the circumstances and with an economizing of resources. The overall motivation is to maintain control of the situation. Consequently, everything in daily life must be planned, which influences psychosocial factors due to unspontaneous behaviour and the need to take precautions.
The encapsulating behaviour
The main category “To stay under the blanket” reflects the encapsulating type. Data show that this tends to be a regression strategy into a self-made world. Individuals with the encapsulating behaviour focus on creating his/her own world, thereby making it smaller. An underestimation of physical capability is common within this type, and there seems to be a component of dependency on spouse. In addition, anxiety was identified as an affective component. The encapsulating behaviour is characterized by key words such as withdrawal and retreatment, primarily in social relations, but also from the world in general as expressed in this quote: “People simply don‘t interest me anymore, I cannot find my former engagement in the world around me, and I just want to be alone ... ” (C19). The motivation behind the behaviour is the need to gather strength in solitude to protect the “core” of the individual’s integrity. As a possible consequence, individuals with the encapsulating behaviour often describe their personalities as changed and the feeling of being a stranger to oneself.
The evasive behaviour
The main category “To live in free spaces” is embedded in the evasive behaviour. Data show that individuals with evasive behaviour use avoidance-strategies, such as keeping PD a secret, immersion into creativity, and attending social/cultural activities, which serve as mental “free spaces”. The individuals are very cautious not to involve family/relatives in their illness, but instead delve into new hobbies and activities as a mental “free space”. They often curb feelings and thoughts, and only show emotions when being alone. Key words are escapism and avoidance; these concepts are manifested in a dependence on the possibility of creating “free spaces” as stated by C16: “I immerse myself in creative things that can make it all disappear ... it is actually the best way, it is better than training too, yes ... in a way it is a form of escape, into another world”. Use of alternative treatment, alcoholism and cannabis also constitute “free spaces”. The motivation behind the creation of “free spaces” can be encompassed in “forgetting” PD and to maintain life as it was before PD, and not being discarded as sick. The consequences of this behaviour can be attributed to the feeling of stress due to the constant struggle of forgetting PD.
The adaptable behaviour
Based on the main category “To enjoy life no matter what”, the individuals with adaptable behaviour focus on the balance between their limitations and the appreciation of life. Data show that this behaviour is characterized by individuals letting their symptoms shape their day and the activities they perform. In fact, the individuals do not register the limitations and ignore thoughts about the future and this serves as a strategy to manage daily life. There seems to be a degree of hedonism in all activities carried out by the individuals in this group. The adaptable behaviour causes an openness about PD and an involvement of the family. The key elements are finding peace in the situation, enjoying life, and a day-to-day adjustment of physical limitations. Participant C21 states “So my aim is to experience the things I think have been fun in life, and achieve it now, while you can, and then enjoy life”. The motivation behind the behaviour is to live in the present, and to gain as much from life as possible. Consequently, a change in attitude towards life is present in the individuals.
The dynamic behaviour
The main-category “To look PD in the eyes” encompasses the dynamic type, as this is the one most action-oriented type, even to extreme degrees such as making suicidal plans. Data show that the individuals in this group hide the symptoms to maintain the position in the community. It can be difficult to distinguish between the convincing and the dynamic behaviour traits, but one significant difference is that the dynamic behaviour does not possess the convincer-element. The key elements within the dynamic behaviour are maintaining autonomy and the ability to make decisions on their own as stated in this quote “I need to decide ... and be respected for it ... it is something about dignity” (C14). To stay independent and position themselves as the “usual” person to protect integrity is the most important motivation within this group. Participant C2 expresses “I WILL be able to do things. I do NOT want to be dependent on others, and feel their pity ... that would be the worst ever”. Consequently, these individuals strive to achieve self-set goals, and are willing to make radical, life-altering changes to accomplish these goals.
The findings seem to stress the need of different approaches depending on pre-dominant coping type. In the discussion section the importance of identifying coping strategies as mediators in the adjustment to everyday life with PD and the approaches in clinical practise will be further discussed. Figure 3 shows this dynamic process.
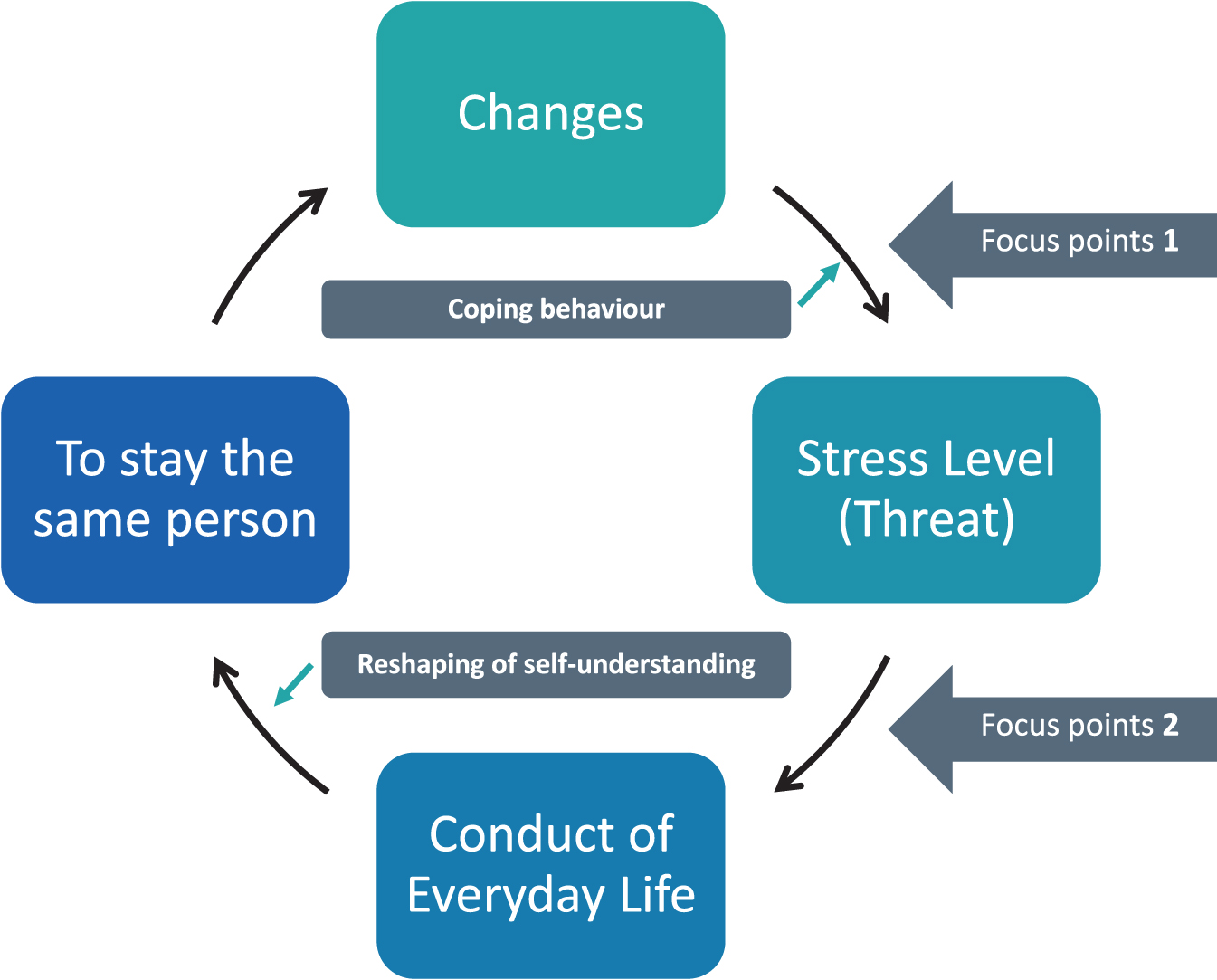
The transition process of coping with changes in everyday life with PD including the mediators.
DISCUSSION
This study reveals a paradox between the main motivation “To stay the same person” and the fact that PD patients must constantly relate and cope with changes in daily life and thus reshape their self-understanding. This aspect seems to be important in a clinical perspective, and therefore the discussion is built around these components.
In this study we identified six pre-dominant coping types, which each has specific behavioural traits, but with the same existential motivation “To stay the same person”. To our knowledge no studies have identified similar or even other coping types within PD. Traditionally, when working with and identifying different coping strategies, questionnaires such as The Way of Coping Questionnaire (WCQ) [30] and The Coping Inventory for Stressful Situations are used [31]. Corti et al. examined the factor structure of the WCQ in a mild to moderately affected PD cohort, and found that only six factors could be reproduced: Escape avoidance, Faith, Confrontive, Seeking Social Support, Planful Problem Solving, and Distancing [32]. These factors can, to a large extent, be compared to some of the predominant types identified in this study, primarily the Escape Avoidance (The Evasive behaviour), Distancing (The Encapsulating behaviour), and the Confrontive (The Convincing and Dynmaic behaviour).
However, Corti et al. suggest that a better understanding of the use of coping strategies will be gained if the participants were directed to think of a PD-specific situation [32]. This is in line with this study‘s use of VN in confronting the individuals with PD-specific limitations in daily life. This dynamism cannot be captured in traditional coping instruments which yield a single measurement at a single moment and highlights a view that coping behaviour is static [33, 34]. Therefore, qualitative methods may be more capable of encompassing complex, interrelated factors when identifying predominant coping types. However, future comparative studies are needed.
Furthermore, the six predominant coping types within PD identified in this study can be compared with traits from main coping styles within chronic illness [35]. The evasive behaviour may belong to the group of avoidance-orientated coping, as it is characterized of seeking distraction in so-called “free spaces”. In addition, those exhibiting evasive behaviour are prone to be socially active with the purpose to “forget PD” and feel like the same person as before PD. Some of these features are also encompassed in the convincing behaviour, where the individuals overdo activities and take on themselves as projects with the feeling of duty. These individuals need social interactions as a reflection, which is in line with the social diversion nature described in the avoidance-orientated coping style [33, 34]. The encapsulating behaviour seems to be contained in the group of emotion-oriented coping styles, where the strategies focus on pushing negative feelings away, and withdrawal from confrontations [35]. Pro-blem-orientated coping alters the environment to reduce stress and is generally employed when the situation is perceived as controllable [34]. These features were identified within the economizing and dynamic coping behaviour. Within the adaptable behaviour the individuals focus on joy in life as a strategy and let the symptoms shape the day, and thereby alter the environment but the individuals also tend to avoid confrontations. Therefore, this behaviour seems to be encompassed in both the emotion-orientated and task-orientated coping styles.
The main theme identified in this study was “To stay the same person”, which reflects the importance of preserving integrity as the underlying motivation across the six coping types. This finding is consistent with existing coping studies illuminating that living with a chronic disease is a constant struggle to maintain integrity [36, 37]. The consequences of the coping behaviour differed in each coping type. Some of the consequences of the coping behaviour across types were feeling stressed, isolation, new attitude to life, and change in personality. For example, the individuals with economizing behaviour are dependent on usual habits and structures, and experience stress and anxiety when not being able to maintain the structure, which causes a high stress-level when meeting changes. This may also be due to the high average number of years with PD compared to the other groups. Regardless of predominant coping type, all patients face changes in everyday life, which is in line with other studies investigating adaptation to life with chronic illness and PD [38, 39]. The degree to which these changes are perceived as a threat to staying the same person is related to the coping type, as the consequences behind each coping behaviour seem to predict the PD patients’ attitude towards changes.
Some of the participants across the six predominant coping types labelled the changes “stepping into next phase” or “a new evaluation” (C13, C30). Studies have investigated the concept of transition, which is the people’s response during a passage of change. Reconstruction of self-identity is essential when making a transition to living well with chronic illness [40, 41]. The PD patients in this study are forced to deal with biological and social dys-appearance, which may influence their self-identity and integrity. Additionally, they constantly have to adapt to new circumstances in order to incorporate these changes into their lives. The coping types seem to function as mediators in the transition process. Therefore, different approaches depending on coping type may be relevant. For example, the individuals with convincing and dynamic behaviour need to maintain autonomy and be involved in decision-making. The approach towards these individuals should be motivated by employing agency, and thus a self-monitoring of their symptoms.
The concept of Conduct of Everyday Life is defined as actions involved in people‘s creation and organization of the fabric of everyday life, and highlights routines as a necessary part of life [42, 43] and is connected to transition. Together they articulate the subjective experience of change and the impact on self-understanding. When people’s health changes, their conduct of everyday life also changes. The changes may be particularly profound if caused by an illness, as the conduction of cyclic routines have to be re-established [43]. The need for usual routines and habits was dominant in individuals with economizing and encapsulating behaviour. On that basis, the routinization may serve as a relief and prevent overload of challenges and stress in daily life. Consequently, life “as it was” before entering the transition-process has to be maintained as much as possible for the individuals within these types. Self-understanding is related to the individual’s reasons for changing the conduct of everyday life, and is partly determined by the social context [42]. For example, individuals with convincing behaviour need social interactions to be reflected in to preserve and to protect integrity.
Relevance to clinical practice
The identification of the six predominant coping types can support healthcare professionals (HCPs) to tailor treatment to each individual with PD based on their coping type and different needs for guidance, empowerment and motivation. Thus, targeting individual coping behaviour may be effective in improving psychosocial adjustment to PD.
Figure 3 illustrates the transition process when coping with disease-related changes. It is suggested that possible focus points (1 + 2) indicate the time and need of actions from HCPs. It would be helpful for HCPs to identify what constitutes a “usual” life for each PD patient, and identify their position in the transition process to support them in developing a positive mind-set and accepting new challenges by drawing on the differences in coping types (focus point 1). The theory behind Conduct of Everyday life is often used in patient education courses with a person-centred approach [43, 44]. This may enable PD patients to learn to manage illness-related roles in everyday life, and, in turn, positively impact the psychosocial adjustment to PD (focus point 2). The coping types function as mediators, and partly determine whether the change increases the stress level to a definite threat. A reshaping of the self-understanding is essential when establishing a new conduct of everyday life to maintain integrity [43]. Thus, this is another mediator in the transition-process.
Instead of focusing on acceptance of PD, HCPs may have to alter the focus to the patients‘ readiness to change and position in the transition-process. This requires a person-centred care approach, which can assist people with a chronic condition in living well by supporting their self-efficacy and empowerment in addressing changes [44].
Method discussion
Figure 2, Table 2, and Supplementary Tables 4 and 5 illustrate the analysis to ensure transparency, which strengthens the credibility [45]. Dependability is sought through describing methods as well as analytic strategies. To ensure confirmability we repeatedly read the interview material to stay close to the participants’ own statements. As a part of this process, triangulation between three of the authors was intensively performed to challenge any pre-assumptions and misinterpretation and ensure trustworthiness [29]. The study is based on data from 34 participants reflecting the experiences with living with moderate PD. Thus, we consider the findings to be transferable to other PD patients in a similar context even though this cohort is relatively moderately affected compared to other studies.
The data collection was based on the participants’ physical limitations, which may have been experienced as confronting and vulnerable to the participants. Therefore, to build up a trust, the participants had two meetings with the investigator in the outpatient clinic before the home visits. The recording of the ADLs took place in the participants’ private homes, which secured a safe environment for the participants, which they also expressed during the data collection.
This qualitative study is the second study of a mixed methods study. It may be considered as being a rigid approach both in the data collection and analysis to use the same patient sample for each sub-study. It may have been more valid to extract a subset of a larger quantitative sample to participate in this qualitative strand of the study [23]. For pragmatic reasons, however, we chose not to.
Further, it would be of interest and utmost clinical relevance to conduct a follow-up in the same cohort after 5 years to clarify if the predominant coping behaviour changes along with the progression of the disease. Moreover, descriptive and clinical data will be further analysed and used in the final phase of this mixed methods study, and may narrow the number of the six pre-dominant typologies, if identical clinical markers are identified within the groups. Evidence supporting the potential applications of findings for psychosocial interventions must also be further investigated.
Conclusion
Six pre-dominant coping types were derived from the data. The convincing behaviour, the economizing behaviour, the encapsulating behaviour, the evasive behaviour, the adaptable behaviour, and the dyna-mic behaviour. The coping behaviour in each type are diverse, but the overall, underlying motivation was the same: to stay the same person as before PD. The results should not be evaluated as a rigid “one size fits all” model, but as an opportunity to guide HCPs working with PD patients and to gain an understanding of the challenges, motivation and consequences of the different behaviour underlying the predominant coping types. We suggest a new approach to PD patients where each individual is met based on their different needs and coping type highlighting a focus on the individuals‘ position in the transition-process. Thus, a more person-centred treatment based on psychosocial and affective components that influence on coping with PD can be incorporated in PD patients’ conduct of everyday life, depending on the readiness to change. These components can be revealed by using qualitative methods instead of or in combination with traditional coping questionnaires.
CONFLICT OF INTEREST
Troels Wesenberg Kjær: Consultant for UNEEG medical
The other authors declare that there is no conflict of interest regarding the publication of this article.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Neurological Department, Zealand University Hospital, and from grants from the Danish Parkinson Association, and Aase & Ejnar Danielsens Foundation.
The authors also thank all the patients for volunteering for the study.