
Abstract
Neuropsychiatric symptoms are common in Parkinson’s disease (PD). We investigated the relationship between neuropsychiatric symptoms and current and future diagnosis of PD dementia (PDD). Individuals with PD who had a study partner were enrolled (n = 696). Study partners were administered the Neuropsychiatric Inventory or Neuropsychiatric Inventory Questionnaire at baseline. Participants were assigned a cognitive diagnosis at baseline and follow up visits. Hallucinations were significantly associated with a diagnosis of PDD cross-sectionally (p < 0.001) and with shortened time to dementia longitudinally among initially nondemented participants (n = 444; p = 0.005). Screening for hallucinations may be useful for assessing risk of dementia in participants with PD.
INTRODUCTION
Parkinson’s disease dementia (PDD) strongly contributes to reduced quality of life, caregiver distress, higher rate of institutionalization, and mortality [1, 2]. Reported point prevalence of PDD ranges from 25–40% [3, 4]; approximately 80% of patients with PD will progress to dementia over the course of their disease [5, 6]. Identifying individuals who are at a higher risk of developing PDD may lessen the disease burden by planning appropriate interventions with regard to medication management and safety issues, as well as permitting patients and caregivers to make arrangements for the future. Consequently, an effort has been made to detect factors that contribute to or predict the development of PDD [2]. Patients with PDD may demonstrate a variety of psychiatric symptoms, such as hallucinations, delusions, depression, and anxiety. Some of these symptoms might precede the development of, and thus serve as a potential marker for, dementia. In our study we aimed to detect the association between neuropsychiatric variables and current and future diagnosis of dementia in patients with PD.
MATERIALS AND METHODS
Subjects
Participants (n = 696) were enrolled in the Pacific Udall Center (University of Washington/Veterans Affairs Puget Sound Health Care System, Oregon Health and Science University/Veterans Affairs Portland Health Care System, or Stanford University) or the Udall Center at the University of Pennsylvania, had a study partner, and met United Kingdom PD Society Brain Bank clinical diagnostic criteria for PD. Two participants were excluded due to an “unknown” cognitive diagnosis at baseline. Participants completing at least one follow up visit were included in the longitudinal analyses (n = 444). Participants were evaluated on average every 1.5 years (range 0.9–4.7 years). The institutional review boards at each site provided formal approval for the study procedures. All participants (or legally authorized representative) and study partners provided written informed consent.
Assessments
Study partners completed a baseline Neuropsychiatric Inventory (NPI) [7] or Neuropsychiatric Inventory Questionnaire (NPI-Q) [8], providing yes/no responses to regarding the presence of delusions, hallucinations, agitation, depression, anxiety, elation, apathy, disinhibition, irritability, nighttime behaviors, and eating abnormalities. Participants were administered the Movement Disorder Society revision of the Unified PD Rating Scale (MDS-UPDRS), part III [9], Modified Hoehn and Yahr [10], 15-item Geriatric Depression Scale (GDS-15) [11], Montreal Cognitive Assessment (MoCA) [12], and a full neuropsychological battery (Supplementary Table 1) [13, 14]. Participants were genotyped for the APOEɛ4 allele and underwent full sequencing of the GBA coding region (combining mutations and E326K into a single group) as previously described [15, 16]. Motor and cognitive diagnoses were assigned at a clinical consensus conference; cognitive diagnoses were made using published diagnostic criteria for PDD and PD with mild cognitive impairment (PD-MCI) as previously described [13].
Statistical analysis
Logistic regression models tested whether each NPI/NPI-Q variable predicted baseline cognitive status (nondemented vs. PDD). Next, all NPI/NPI-Q variables were entered into a single logistic regression to determine if any variables were associated with PDD over and above the other variables. Logistic regression analyses were then conducted on the initially nondemented sample to determine whether baseline NPI/NPI-Q variables predicted conversion to PDD. Cox regression analyses were conducted to determine whether NPI/NPI-Q variables at baseline predicted time to PDD. Kaplan-Meier estimates were calculated, and log-rank tests were performed to determine whether there was a significant difference between the curves. To determine whether longitudinal associations were impacted by a higher rate of baseline PD-MCI in the PDD conversion group, analyses were run separately controlling for baseline cognitive diagnosis (no cognitive impairment, PD-MCI). Covariates included age, education, sex, PD motor symptom duration, total levodopa equivalent daily dose [17], MDS-UPDRS part III, GDS-15, and study site. Longitudinal analyses additionally controlled for length of follow up and number of study visits. Secondary analyses were conducted that included genetic status (APOEɛ4 or GBA variant) and MoCA (to account for the full range of cognitive performance in the nondemented group). The Bonferroni adjustment was used to control the family wise type I error set a priori at 0.05; since there were 10 NPI variables, a significance level of 0.05/10 = 0.005 was used. All analyses were performed in Stata 15.1.
RESULTS
Baseline associations between cognitive diagnosis and NPI variables
Baseline participant characteristics are provided in the Supplementary Material (Supplementary Table 2). There was a significant association between a diagnosis of PDD and the presence of delusions, hallucinations, anxiety, apathy, and disinhibition (Table 1). When genetic status (APOE or GBA) was included, the results did not significantly change. When the MoCA was included, the relationship between PDD and apathy was no longer statistically significant, suggesting that apathy was more associated with global cognition than with PDD diagnosis per se.
Associations between NPI variables and cognitive diagnosis
†Significant after correcting for multiple comparisons (p < 0.005). CI, confidence interval; NPI, Neuropsychiatric Inventory; OR, odds ratio; PDD, Parkinson’s disease dementia.
When all NPI variables were entered into a single logistic regression, only hallucinations were associated with a PDD diagnosis over and above all other variables (odds ratio = 5.4 95% confidence interval (CI) 2.7–10.8, p < 0.001). This did not change when MoCA, GBA status, or APOEɛ4 genotype were entered.
Associations between conversion to PDD and NPI variables
Of the participants who were non-demented at baseline, 444 (76%) completed at least one follow up visit. Mean length of follow up was 4.5 (SD = 2.6) years; PDD converters did not significantly differ from nonconverters in length of follow up. Baseline characteristics for PDD converters and non-converters are provided in the Supplementary Material (Supplementary Table 3).
Comparison of baseline NPI/NPI-Q variables between converters and nonconverters yielded no significant differences. However, time to convert to dementia was significantly shorter for those participants whose study partners reported hallucinations at baseline (hazard ratio [HR] = 2.4 95% CI 1.3 –4.3, p = 0.005; Fig. 1). The log rank test indicated the difference in Kaplan-Meier survival curves was statistically significant (χ2 = 11.84, p = 0.0006). When baseline cognitive status was included as a covariate, the HR was 2.2, 95% CI 1.2–4.0, p = 0.013. These results did not change significantly when genetic variables were entered. When the analyses were performed only on those participants with a MoCA available (n = 298), the results were nonsignificant whether or not the MoCA was included, suggesting that smaller sample size may have precluded detection of statistically significant differences.
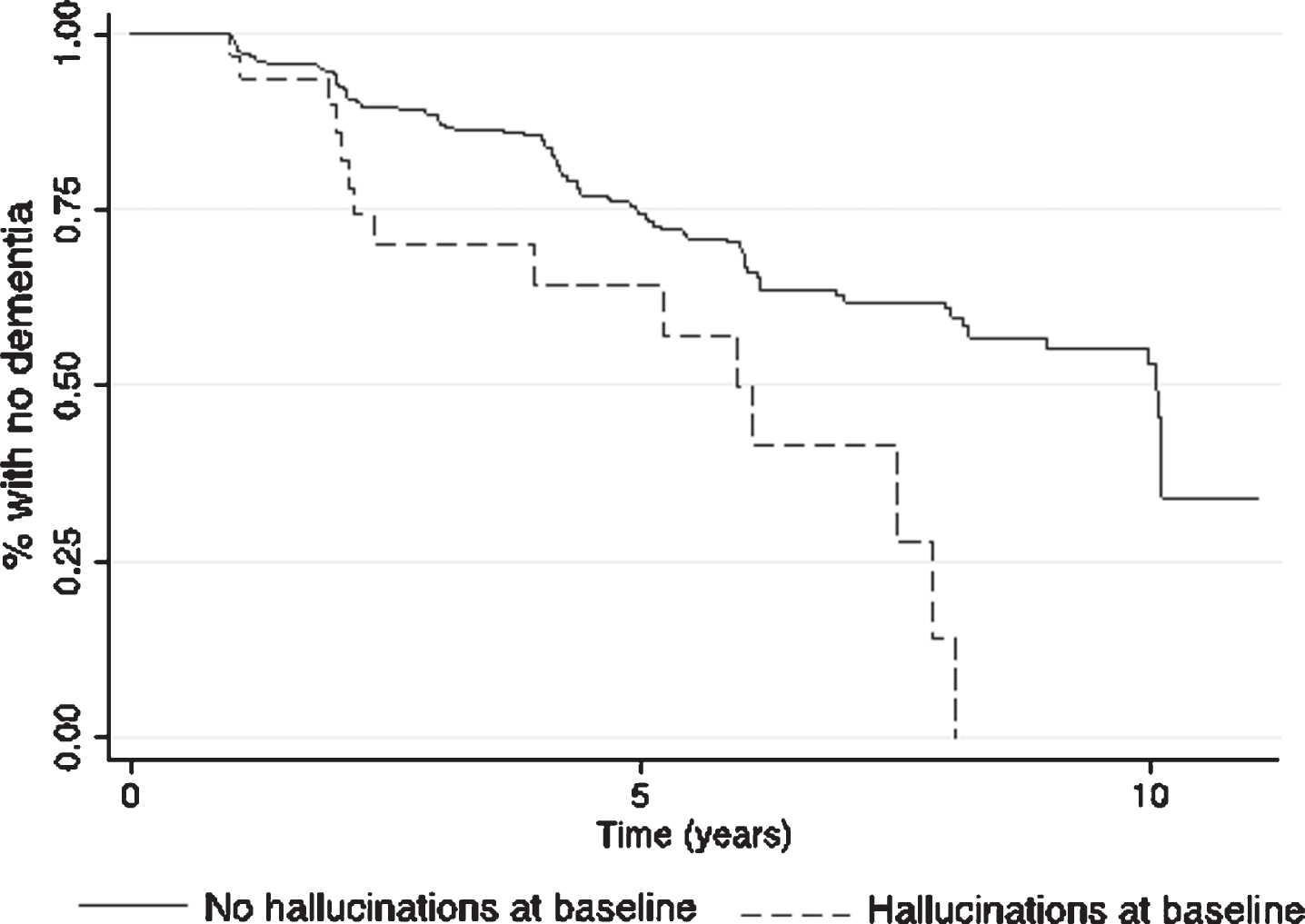
Kaplan-Meier survival estimates of time to dementia for initially non-demented participants with and without study partner reported hallucinations at baseline.
DISCUSSION
This study examined the relationship between study partner reported psychiatric symptoms and dementia in participants with PD. Baseline analyses demonstrated that, while PDD was associated with many neuropsychiatric features, the presence of hallucinations had the strongest association over and above other psychiatric variables. Hallucinations were also the only symptom associated with a shortened time to PDD in initially non-demented participants. Although past studies showed strong cross-sectional associations between hallucinations and dementia of PD [1, 18–24] as well as associations with global cognitive decline in PD [25], ours is the first to explicitly demonstrate decreased time to dementia diagnosis in initially non-demented PD individuals with hallucinations.
It is well-recognized that individuals with PDD may experience pronounced hallucinations as part of the disease process amongst other neuropsychiatric problems [26–28]. Our analyses corroborated this finding by showing that although multiple neuropsychiatric variables were associated with a baseline diagnosis of PDD (delusions, hallucinations, anxiety, apathy, and disinhibition), only hallucinations were associated with PDD when correcting for other variables. The current literature suggests that the underlying process responsible for development of hallucinations is interconnected with a mechanism of cognitive deterioration in PD patients, albeit the pathophysiology is not yet fully understood [18, 27].
Our research demonstrates that time to convert to dementia was significantly shorter for the non-demented participants whose study partners reported hallucinations at baseline. Thus, the presence of hallucinations in PD may foreshadow more insidious disease progression. Management of dementia and its accompanying symptoms necessitates multidisciplinary and multilayered approaches which take more time, effort, and resources [29]. Therefore, it is important to anticipate and recognize these symptoms early, for example with screening tools such as NPI, in order set up a care plan that is best fitted for the affected patient.
Unfortunately based on the NPI/NPI-Q, we were unable to differentiate between types of hallucinations, which might be important, as there are studies that link certain cognitive domain deficits with visual hallucinations specifically as opposed to other forms of hallucinations [19, 22]. Additionally, the NPI/NPI-Q are completed by the study partner rather than patient, leading to possible inability to detect earlier onset and subtler forms of hallucinations. Finally, MoCA scores were not available for a substantial proportion of participants, making it difficult to distinguish whether hallucinations were a primary factor influencing the rate of decline to PDD or developed in conjunction with worsening cognitive impairment. However, when baseline cognitive diagnosis was controlled for in the larger sample, faster time to dementia was still seen among those with hallucinations at baseline.
Our research demonstrates a significant association between multiple neuropsychiatric symptoms and PDD, and hallucinations in non-demented participants predicted a shorter time to PDD. Our study substantiates the link between psychiatric symptoms, especially hallucinations, and dementia in PD. Psychiatric screening batteries such as the NPI/NPI-Q may provide useful information to clinicians by alerting them to non-motor symptoms that may herald impending dementia. Additional work to determine factors that underlie the association between hallucinations and cognitive decline are important future steps.
CONFLICT OF INTEREST
The authors have no conflicts of interest relevant to this article to declare.
Footnotes
ACKNOWLEDGMENTS
This work was supported by grants from the National Institutes of Neurological Disorders and Stroke (P50 NS062684) and Department of Veterans Affairs (101 CX001702). Data contributed by the current project Center On Alpha-Synuclein Strains in Alzheimer’s Disease & Related Dementias at the Perelman School of Medicine at the University of Pennsylvania (U19 AG062418, Trojanowski JQ – PI; Weintraub D; Chen-Plotkin A; Dahodwala N; Morley JF; Duda JE) and former Morris K. Udall Center at the Perelman School of Medicine at the University of Pennsylvania (P50 NS053488, Trojanowski JQ – PI). Dr. Gryc and Dr. Roberts were supported by the Veterans Affairs Advanced Fellowship Program in Parkinson’s Disease. We sincerely thank all of the individuals who participated in this study.