
Abstract
Background:
Scans without evidence of dopaminergic deficit (SWEDDS) on 123I-FP-CIT SPECT (DAT) can occur in patients with clinical evidence of Parkinsonism. In this patient population, autonomic function testing may elucidate the underlying clinical disorder.
Objective:
To evaluate SWEDD patients undergoing autonomic testing and determine the severity and pattern of autonomic dysfunction.
Methods:
All patients with a diagnosis of SWEDD and formal autonomic function testing at Mayo Clinic, MN were retrospectively reviewed. Autonomic failure was quantified using composite autonomic severity score (CASS). The Modified Hoehn and Yahr score (HYS) determined Parkinsonism severity.
Results:
Of 1,874 patients with DAT imaging at Mayo Clinic, 13 met diagnostic criteria of SWEDD. The median age of symptom onset was 56.0 (IQR 40.5–75.5). Autonomic dysfunction was present in 12/13 on ARS and/or TST. The median CASS was 2.50 (IQR 1.00–3.00). Distal anhidrosis was most common (7/13) while 3/13 had widespread anhidrosis on TST and/or QSART testing. Patients with a distal pattern of anhidrosis had a median score of 3.0 (IQR 2.38–4.25) on the HYS versus 2.0 (IQR 1.00–2.00) for those with a diffuse pattern (p = 0.048). Patients with more advanced Parkinsonism were more likely to respond to L-Dopa, with higher HYS in the dopa-responsive versus non-Dopa-responsive (p = 0.026). No correlation existed between severity of Parkinsonism, and CASS (p = 0.39).
Conclusion:
Autonomic function testing may detect autonomic dysfunction in most patients with SWEDD. The pattern of dysfunction is suggestive of the degree of clinical Parkinsonism, and autonomic testing may predict whether patients with SWEDD respond to L-Dopa.
Keywords
INTRODUCTION
Scans without evidence of dopaminergic deficit (SWEDD) refer to 123I-FP-CIT SPECT (DAT) imaging without evidence of dopaminergic deficit in patients with clinical Parkinsonism. The pathogenesis and underlying disease mechanisms for this phenomenon has yet to be fully elucidated. To date, it has been hypothesized that patients with SWEDD have underlying early idiopathic Parkinson’s disease that have not yet shown presynaptic dopaminergic deficit in the striatum; however, this hypothesis has been challenged in a longitudinal observational study [1]. Conversely, it has been hypothesized that the SWEDD are seen in patients with Dopa-responsive dystonia that mimic features of Parkinsonism [2].
Regardless of the diagnostic nomenclature, patients with SWEDD may present with autonomic dysfunction. To date, cardiac sympathetic denervation and abnormalities in 24-hour ambulatory blood pressure monitoring have been described [3, 4] supporting the hypothesis that patients with SWEDD may have concomitant autonomic dysfunction. However, there has been no description of autonomic function testing in patients with SWEDD. Autonomic Reflex Screen (ARS) includes postganglionic sympathetic sudomotor, cardiovagal and adrenergic testing including a head-up tilt. Thermoregulatory sweat test (TST) assesses the entire thermoregulatory pathway. These tests can provide localization of autonomic dysfunction with certain patterns indicative of various disease states such as a pattern of distal small fiber involvement in patients with Parkinson’s disease [5].
MATERIALS AND METHODS
Study design
This study was approved by the Mayo Clinic Institutional Review Board. Patients in this study or their authorized representatives gave permission for their medical records to be reviewed for research purposes. We reviewed all patients that presented at Mayo Clinic, MN with clinical Parkinsonism, but negative DaTscan imaging, who also underwent formal autonomic function testing. We reviewed the electronic medical records using Advanced Cohort Explorer (ACE) tool using terms “DAT negative,” “Parkinsonism,” and “autonomic reflex screen” from 2008 to 2018.
We identified thirteen eligible patients (13/1874) based on the following criteria: 1) patients greater than 18 years of age or older; 2) documented evidence of Parkinsonism on exam by a Mayo Clinic Rochester neurologist; 3) patients must have undergone DAT with formal radiographic interpretation negative for evidence of pre-synaptic dopaminergic deficit; and 4) completion of formal autonomic testing including an autonomic reflex screen (ARS) or a thermoregulatory sweat test (TST) at the Mayo Clinic. The referral reasons for autonomic testing included urinary symptoms in 2 patients, orthostatic symptoms or falls in 5 patients, and baseline screening in 6 patients. The exclusion criteria included patients with a cause of their Parkinsonism other than SWEDD, including but not limited to drug-induced Parkinsonism, functional movement disorder, or normal pressure hydrocephalus (see Fig. 1 for details). All eligible patients were reviewed for other causes of autonomic failure. 1/13 patients had the diagnosis of diabetes but were not on any medications for treatment, hemoglobin A1c<7 at most recent evaluation, and no evidence of peripheral neuropathy on recent examinations, thus this was not considered a significant factor in their autonomic testing. L-Dopa responsiveness was assessed via review of clinical documentation regarding the patient’s symptom improvement after L-Dopa initiation.
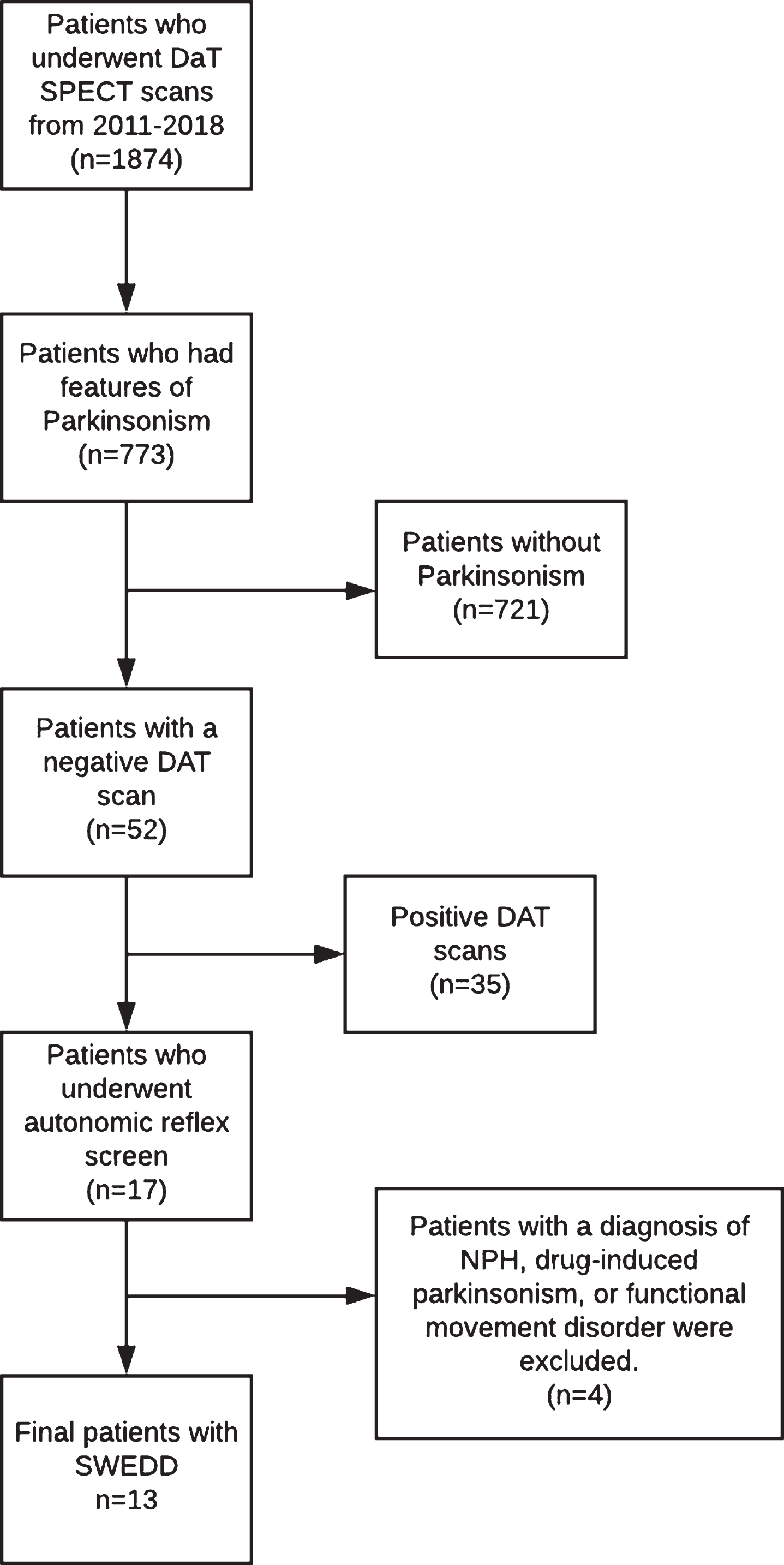
Patient Selection Flow Diagram. Patients reviewed using the Advanced Cohort Explorer (ACE) tool which reviews all patients who underwent DaTScan at Mayo Clinic from 2011-2018. If there was no documentation of parkinsonism then the patients were excluded. NPH, normal pressure hydrocephalus; SWEDD, Scans without evidence of dopaminergic deficit.
The ARS includes testing of postganglionic sympathetic sudomotor function with quantitative sudomotor axon reflex test (QSART), heart rate to deep breathing, heart rate response to Valsalva maneuver, blood pressure response to Valsalva maneuver, and head-up tilt. All patients who undergo autonomic reflex screening at Mayo Clinic are instructed to hold any potentially confounding medications such as antidepressants or antihypertensives for testing. We used the composite autonomic severity score (CASS) for quantification of autonomic failure. This scale assigns values based on testing with maximum scores for each category listed: sudomotor (3), cardiovagal (3), adrenergic (4) with a maximum score of 10 indicating severe autonomic failure. Scores of less than 3 indicate mild impairment with scores from 7 to 10 indicating severe autonomic failure [5].
Statistical analysis
Descriptive summaries were reported as median and interquartile range (IQR) for continuous variables and frequencies and percentages for categorical variables. Categorical and continuous data were analyzed using Wilcoxon signed rank test and Spearman’s rank order correlation. All tests were two-sided and p values less than 0.05 were considered statistically significant. All statistical analyses were performed using JMP 13.0.0 (SAS Institute Inc).
RESULTS
Of 1,874 patients who underwent DAT imaging at Mayo Clinic from 2008 to 2018, 773 patients had features of Parkinsonism documented on physical exam. Out of these patients, 52 patients were determined to have a DAT negative for any evidence of dopaminergic deficit (SWEDD). Of those patients, 13 underwent autonomic function testing with either an autonomic reflex screen (12) and/or thermoregulatory sweat test (6) and were not diagnosed with other diseases (including but not limited to NPH, drug-induced Parkinsonism, or functional movement disorders). The median time of symptom onset to time of DAT and diagnosis was 3.0 years (IQR 2.0–15.0).
Of the 13 patients with autonomic function testing, 12 had autonomic dysfunction on either ARS and/or TST. Demographic information is reported in Table 1.
Demographics
Categorical variables represented as frequency (percentages). Continuous variables represented as median (interquartile range). CASS, composite autonomic severity scale; TST, thermoregulatory sweat test.
The pattern of anhidrosis was associated with a different severity of Parkinsonism as noted on the Hoehn-Yahr scale (HYS). Patients with a distal pattern of anhidrosis had a median HYS of 3.0 (IQR 2.38–4.25) versus 2.0 (IQR 1.00–2.00) for those with a diffuse pattern (p = 0.048). Patients with more severe and advanced Parkinsonism as evidenced by higher HYS were more likely to be responsive to L-Dopa (p = 0.026). CASS was not significantly related to the degree of Parkinsonism the patients exhibited on exam (2.0, IQR 1.0–3.0, p = 0.39). Time from symptom onset to diagnosis and DAT was not significantly related to severity of Parkinsonism (p = 0.48), or autonomic failure (p = 0.66).
DISCUSSION
In our retrospective review of all patients who were diagnosed with SWEDD and underwent autonomic function testing, we observed that autonomic dysfunction is present in most patients with clinical Parkinsonism and SWEDD. Furthermore, the pattern of sudomotor dysfunction on autonomic testing was associated with greater severity of Parkinsonism: patients with distal anhidrosis had higher HYS than those with global anhidrosis (see Fig. 2). Distal anhidrosis or a normal TST are the most commonly observed sweating patterns in idiopathic Parkinson’s disease [6]. Autonomic tests have also been reported to be helpful to support the diagnosis of an atypical Parkinsonism with greater degree of autonomic dysfunction seen in patients with multiple system atrophy [6] while patients with PSP typically have minimal degree of autonomic dysfunction [7]. Additionally, patients with MSA tend to have high degrees of anhidrosis and may exhibit a pattern of acral preservation “purple hands” on TST [1, 7]. The use of QSART and TST can be useful to determine the site of the lesion as either central or peripheral in patients with synucleinopathies. Similar to idiopathic Parkinson’s disease, both Lewy body disease and pure autonomic failure classically involve peripheral autonomic neurons; whereas central patterns of anhidrosis are more typical in MSA [8, 9].
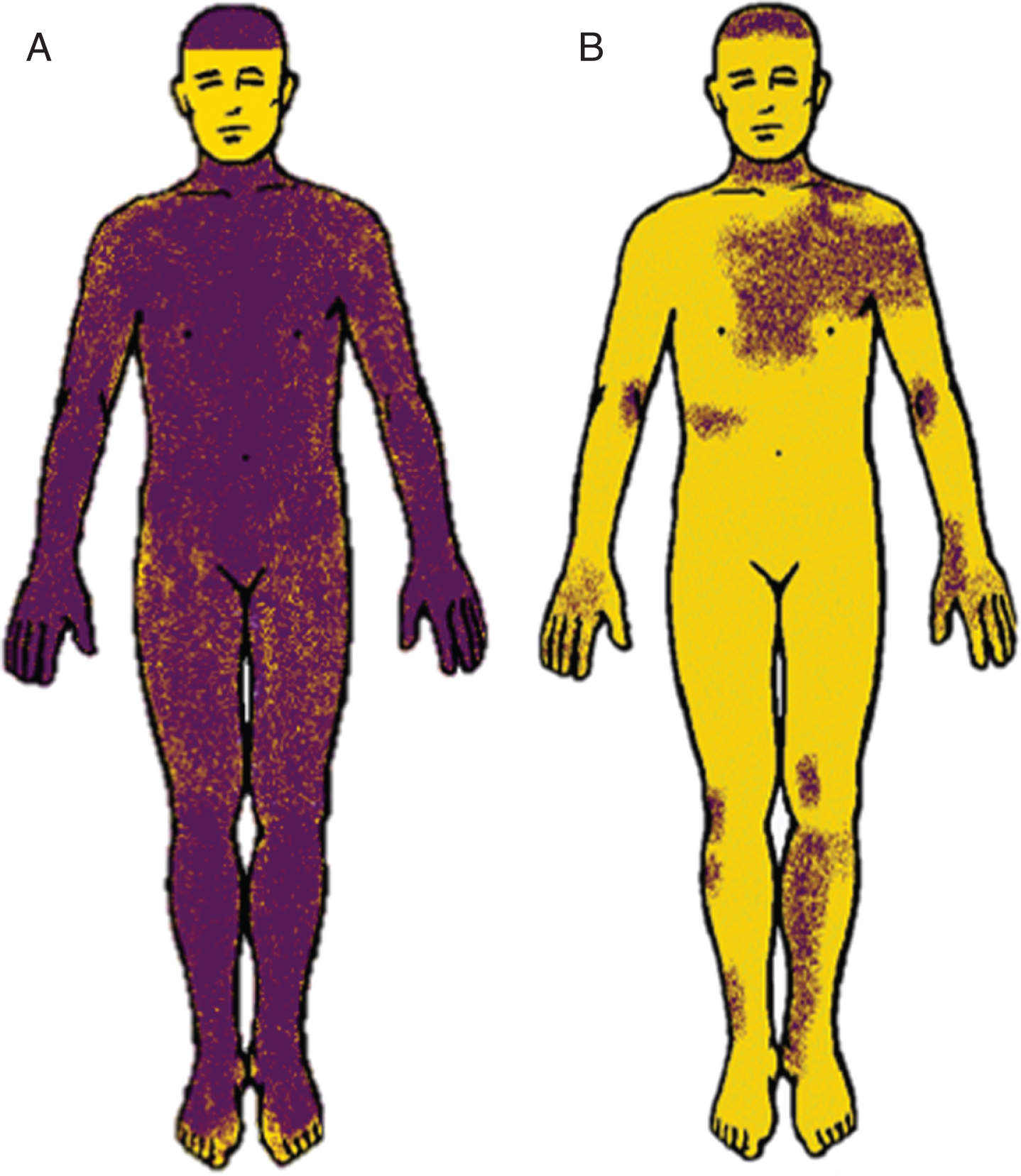
Thermoregulatory sweat tests. A) Patient with distal anhidrosis and B) patient with widespread or global (see above) anhidrosis. Purple indicates sweating while yellow indicates anhidrosis (the face is not powdered).
Importantly, we observed that some patients with SWEDD exhibit a pattern of distal anhidrosis, and the patients that responded to L-Dopa treatment may have more severe Parkinsonism. Thus, even in the absence of dopaminergic deficit on DAT imaging, patients may still benefit from a trial of L-Dopa.
Strengths of our study include the large number of patients referred to a tertiary referral center, the high number of DAT scans available for analysis, as well as subspecialty evaluation of all patients. Our study has limitations given that this is a retrospective design. As patients with autonomic testing were included, it was unclear whether some patients had additional features suggestive of autonomic failure that may have impacted the likelihood of obtaining autonomic testing in this patient population. In addition, a distal pattern of anhidrosis may be associated with lesions that are central, in additional to peripheral.
In summary, our findings suggest that autonomic dysfunction is present in the great majority of patients with clinical Parkinsonism with SWEDD, although the degree of autonomic failure is typically minor, such as that seen in idiopathic Parkinson’s disease. Additionally, the pattern of dysfunction on autonomic testing may be associated with the severity of Parkinsonism. Distal anhidrosis (as typically seen in idiopathic Parkinson’s disease) is associated with L-Dopa responsiveness in patients with SWEDD. Future prospective studies are needed to expand the role of autonomic testing in SWEDD.
FUNDING SOURCE
No extramural funding supported this work.
CONFLICT OF INTEREST
Rodolfo Savica receives research support from the National Institute on Aging, the National Institute of Neurological Disorders and Stroke, and the Mayo Clinic Small Grants Program National Center for Advancing Translational Sciences (NCATS) and unrestricted research grants from Acadia Pharmaceutical, Inc. The other authors have no conflicts of interest to report.