
Abstract
Background:
Deterioration of working memory(WM) is a common cognitive deficit in Parkinson’s disease (PD), and severely influences the ability to lead an independent life. Interventions which can delay the impact of WM deficits could positively impact the independence and quality of life of patients.
Objective:
To evaluate effects of computer-based cognitive rehabilitation (CBCR) on WM in patients with PD.
Methods:
Pubmed, Embase, Psycinfo and Cochrane Library were systematically searched. Authors of included studies were contacted to detect unpublished data or articles not found by database-search. Broad selection criteria were applied because literature was expected to be limited. Studies were eligible for inclusion if they investigated the effects of CBCR on WM in a sample consisting of at least 50% PD patients, or in which the results of PD patients could be isolated. Studies were further eligible for inclusion in a planned meta-analysis if the effects of the CBCR intervention could be isolated, the CBCR intervention was compared to active or passive control groups consisting solely of PD patients, and the WM outcome measure could be isolated.
Results:
Only six studies were included despite broad inclusion criteria. Study results were heterogeneous, and the risk of bias in study methodology was either unclear or high. Two studies were eligible for meta-analysis. A meta-analysis was not performed, because these studies used different measures of WM which were not rated as equally valid and reliable.
Conclusion:
Existing literature is sparse and provides insufficient evidence to conclude if CBCR benefits WM in PD patients.
Keywords
INTRODUCTION
Rationale
Parkinson’s disease (PD) is one of the most prevalent neurodegenerative disorders second to only Alzheimer’s disease [1]. All though PD is characterized as a movement disorder, the prevalence and impact of cognitive symptoms has become increasingly recognized in recent years [2–6]. Large cohort studies suggest that 36% of newly diagnosed PD patients have some form of cognitive impairment [6], and in 2012 specific diagnostic criteria for mild cognitive impairment were proposed [7]. Dementia describes an observable cognitive decline with several mental faculties involved and implications for the ability to carry out activities of daily living [8]. PD patients have a sixfold increased risk of developing dementia compared to non-PD controls [9] and 46% of PD patients develop Parkinson dementia within 10 years after diagnosis [4]. Thus, cognitive decline represents a common and devastating symptom of PD.Furthermore, resent research suggests that cognitive symptoms might antecede PD diagnosis in some cases [10].
Deterioration of working memory is acommon cognitive deficit experienced by PD patients, and severely influences the ability to lead an independent life [2, 11]. Finding ways to delay, decelerate and ideally treat cognitive deterioration is crucial for patients’ independency and quality of life.
Earlier systematic reviews supportmoderate positive effects of various cognitive training interventions in cognitively healthy elderly people [12] and PD patients [13–16]. However, these reviews all report that current evidence should be interpreted cautiously because of sparse evidence from small sample studies with varying methodological quality. Existing reviews explore the combined effects of various cognitive interventions within a broad range of cognitive domains and more knowledge is needed regarding the effects of specific interventions on specific cognitive symptoms.
A relatively new approach to cognitive training is Computer-based Cognitive Rehabilitation (CBCR), which consist of cognitive exercises that can be performed on a standard home computer as self-training after instructions from a health professional. CBCR has been met with great expectations regarding rehabilitation of different patient groups, because the method is relatively cheap and has the advantages of flexibility and adaptability of training content [17, 18].
This review was carried out to obtain an overview of the existing literature specifically regarding the effects of CBCR on working memory inPD patients. Because the existing literature was expected to be sparse, relatively broad inclusion criteria were applied.
Objectives
The objectives for this review were designed using the PICOS criteria, and the review was conducted using the PRISMA guidelines [19]. Thisreview explores the effects of CBCR on working memory in PD patients compared to active and passive control conditions in randomized controlled trials using quantitative neuropsychological measures to assess outcome.
METHODS
Protocol and registration
Before initiation of this review, areview-protocol was registered at the International Prospective Register of Systematic Reviews(PROSPERO) with ID number: CRD42018104293.
Eligibility criteria
Studies were included in the systematic review if they met the following PICOS-based [19] inclusion criteria: Studies in which at least 50% of the included patients were diagnosed with PD or studies in which the results of patients with PD could be isolated. Presence or absence of mild cognitive impairment orParkinson-dementia and the timing of the intervention relative to disease duration did not constitute inclusion- or exclusion criteria. Studies using a CBCR method as an intervention to enhance executive functions or specifically working memory. Studies that compared different CBCR interventions were also included. Studies in which CBCR was part of amulti-method rehabilitation intervention were also included. Studies comparing the effects of CBCR to active or passive control groupswere included. Studies with no control groups were also included, if they compared the cognitive development in the patients before and after the treatment. Studies exploring the effects of CBCR in all settings were included Studies using a quantitative working memory measure or studies using an outcome measure which included a quantitativeworking memory measure, but in which the outcome for working memory could not be isolated. All controlled, clinical trials were included regardless of randomization and blinding procedures.
Studies were subsequently included in the meta-analysis if they met all the above outlined inclusion criteria as well as the following criteria: The effects of the CBCR intervention could be isolated. The intervention was compared to active or passive control groups consisting solely of patients with PD. The working memory outcome measure could be isolated.
Studies were excluded from the systematic review based on the following criteria: They did not meet the above outlined PICOS-criteria.
Information sources and search
Four online databases were searched: PubMed/Medline, Embase, PsycINFO and Cochrane Library. The search strategy included terms describing the population (PD patients) the intervention (CBCR) and the targeted cognitive function (working memory). Filters were used to find only clinical trials including humans from 1980 and forward, because the first trials of CBCR are from the early 1980 s [20]. All search-terms along with the full search string are provided in Supplementary Material 1.
Authors of articles included in the review were contacted in an attempt to identify unpublished data and reduce possible effect of publication bias. No further relevant studies were identified from this approach.The full search strategy is available in Supplementary Material 1. All searches were performed on 20 September 2018.
Study selection
Two authors were involved in the entire process of study selection from initial searches and screening for relevant titles to final inclusion in the review. The authors selected studies for each step individually before checking if the chosen studies for each step were identical. When this was not the case, a third author was involved in the discussion about further inclusion. See flow diagram in Fig. 1.
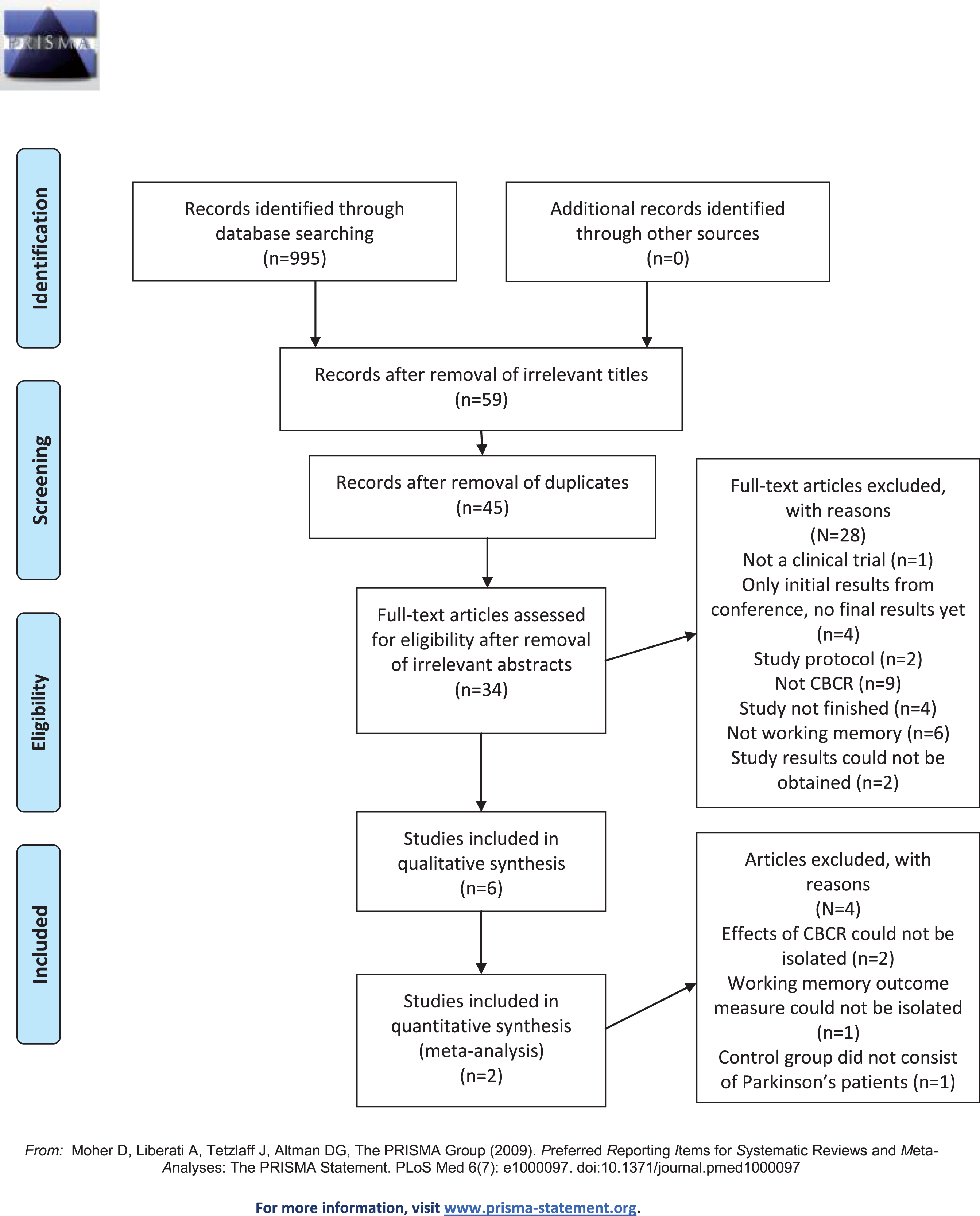
PRISMA 2009 flow diagram.
Data collection process and data items
All data from relevant reports were extracted using pre-designed data-extraction charts with information about relevant data-items. The full list of extracted data-itemscan be found in Supplementary Material 2.
Risk of bias in individual studies and across studies
Risk of bias in individual studies and across studies was assessed using the Cochrane Collaboration’s tool for assessing risk of bias [21]. With this tool, risk of bias is assessed as high, low or unclear for six types of bias: Selection bias (which concerns both random sequence generation and allocation concealment); performance bias; detection bias; attrition bias; reporting bias; and other types of bias. For the present review, performance bias was not assessed as high if personnel were not blinded, because blinding of personnel in a CBCR-intervention study is not realistically possible (Svaerke et al., unpublished data). Thus, if participants were blinded, it was assessed that there was a low risk of performance bias. Risk of bias was assessed by two review authors with regard to outcome measures of working memory only. For the studies that included more than one such outcome measure, risk of bias was assessed across these measures.
Based on the risk of bias within the bias domains in the individual studies, a summary assessment of risk of bias within studies across domains was also carried out, following the Cochrane Collaboration’s specifications. Risk of bias across studies was assessed based on the assessment of risk of bias in the individual studies as proposed by the Cochrane Collaboration [21].
Summary measures and synthesis of results
The primary outcome of interest was the effect of CBCR on working memory in PD patients. A standardized mean difference, Cohen’s d, is used as a summary measure for the effects of CBCR on the working memory measures used in included studies. The measures of working memory used in studies eligible for meta-analysis were ranked regarding their quality and trustworthiness as working memory measures. This ranking was performed to assess the heterogeneity in trustworthiness of the working memory outcome measures. This ranking was based on published estimates of reliability, validity and re-tests effects of the individual working memory measures.Digit Span Backwards and Letter-Number Sequencing were rated as the most trustworthy working memory outcome measures because of high degrees of validity and reliability [22]. The trail making B test was rated as the second most trustworthy measure of working memory because of high degrees of validity, but a susceptibility to visuoperceptual and visuospatial deficits without the use of the Trail Making A test [23]. The Paced Auditory Serial Addition Test (PASAT) was rated as the least trustworthy included working memory outcome measure because it is susceptible to test-retest effects [24].
Additional analysis
One additional analysis was performed in order to cautiously estimate the difference between increases in performance on working memory measures for the control groups and intervention groups. This was done instead of a meta-analysis of effect-sizes due to heterogeneity in working memory measures used in the studies eligible for the meta-analysis. Specifically, the additional analysis consisted of calculations of percentwise increases from pre- to post intervention for all working memory outcome measures for the control and intervention groups in the studies eligible for meta-analysis.
RESULTS
Study characteristics
Six studies were included in this review. A summary ofstudy-characteristics ispresented in Table 1, and a detailed table of study-characteristics is provided in Supplementary Material 3. A brief outline of included studies is presented below.
Characteristics of included studies
Adamski et al. (2016) [25]
This study explored the effects of CBCR on working memoryin a parallel design with three groups in a total of 25 participants: One group with PD patients, and two groups with healthy controls who weresubdivided into an active control condition and a passive control condition. The PD-group trained with the programme‘Brainstim’. The study found no significant differences between baseline and post-intervention or between baseline and three months follow up for the PD-group on any working memory measures.
Cerasa et al. (2014) [26]
This study explored the effects of CBCR on attention and processing speed in 15 PD patients, but outcome measures of working memory were also included. Eight PD patients completed exercises for attention and processing speed with the computer software ‘RehaCom’, andseven PD patients completed a control conditionconsisting of a visuomotor tapping task for the same amount of time as the experimental condition.A comparison between the groups revealed no significant differences on any of the working memory outcome measures.
Lawrence et al. (2018) [27]
This study explored the effects of six different interventions on all cognitive domains and quality of life in 42 PD patients with mild cognitive impairments. Two of the groups completed standard cognitive training and tailored cognitive training with the computer software SmartBrain PRO, and these groups are the only groups in which the isolated effects of CBCR can be analyzed. Because tailored cognitive training is the intended use of the SmartBrain PRO software, the tailored cognitive training intervention is the only group included for further analysis in this review. Statistical analysis between baseline and post-intervention revealed no significant differences on working memory in this group, but a significant increase in quality of life between baseline and post-intervention measured with the Parkinson Disease Questionnaire PDQ-39. The study included a follow-up after six weeks in which the significant improvement on the PDQ-39 for the tailored cognitive training group was sustained.
Paris et al. (2011) [28]
This study explored the effects of combined CBCR and paper-and-pencil exercises on all cognitive domains, quality of life and ADL functions in 28 PD patients. The 16 patients in the experimental condition (EC) used various paper-and-pencil exercises and the software ‘SmartBrain’. The intervention was compared to an active control condition (ACC) of 12 patients who received speech therapy for the same amount of time as the EC received cognitive training. Significant differences from baseline to post-intervention were discovered between the EC and the ACC on one of two working memory outcome measures. No significant differences were found on measures of quality of life or activities of daily living after the intervention between the EC and the CC.
Reuter et al. (2012) [29]
This study was a randomized, controlled, outcome-assessor blinded trial investigating the effects of: i) cognitive training, ii) cognitive training and psychomotor training, iii) cognitive training, psychomotor training and transfer training in a three-group parallel design with three groups consisting of a total of 223 PD patients. All three groups received cognitive training consisting of both computerized and paper and pencil tasks that required executive and memory functions. Testing at baseline, after 4 weeks of training and after 6 months of continued training at home showed that all groups improved on measures of working memory. The group receiving both psychomotor, transfer and cognitive training improved more than the cognitive and transfer training group, and the cognitive training only group. The results thus show a positive effect of cognitive training, but larger effects of cognitive training supplemented with transfer training and psychomotor training.
Zimmermann et al. (2014) [30]
Zimmermann et al. (2014) investigated the effects of computerized cognitive training compared with non-specific training on Nintendo Wii in a parallel controlled, randomized single-blinded study with 39 PD patients. The Experimental condition consisted of computerized cognitive training in CogniPlus-software. Patients in the control condition trained equal amounts of non-specific tasks on Nintendo Wii Sports Resort. Training sessions were supervised by a psychologist or trained psychology student. The study did not find differences in improvement from baseline to post-training evaluation on a working memory parameter measure.
Risk of bias within studies
Risk of bias within studies in the individual domains is presented in a summarized form in Table 2. A green mark represents a low risk of bias, a red mark represents a high risk of bias, and a yellow mark represents an unclear risk of bias. Tables with support for the judgments can be found in Supplementary Material 4.
Risk of bias within studies summary figure
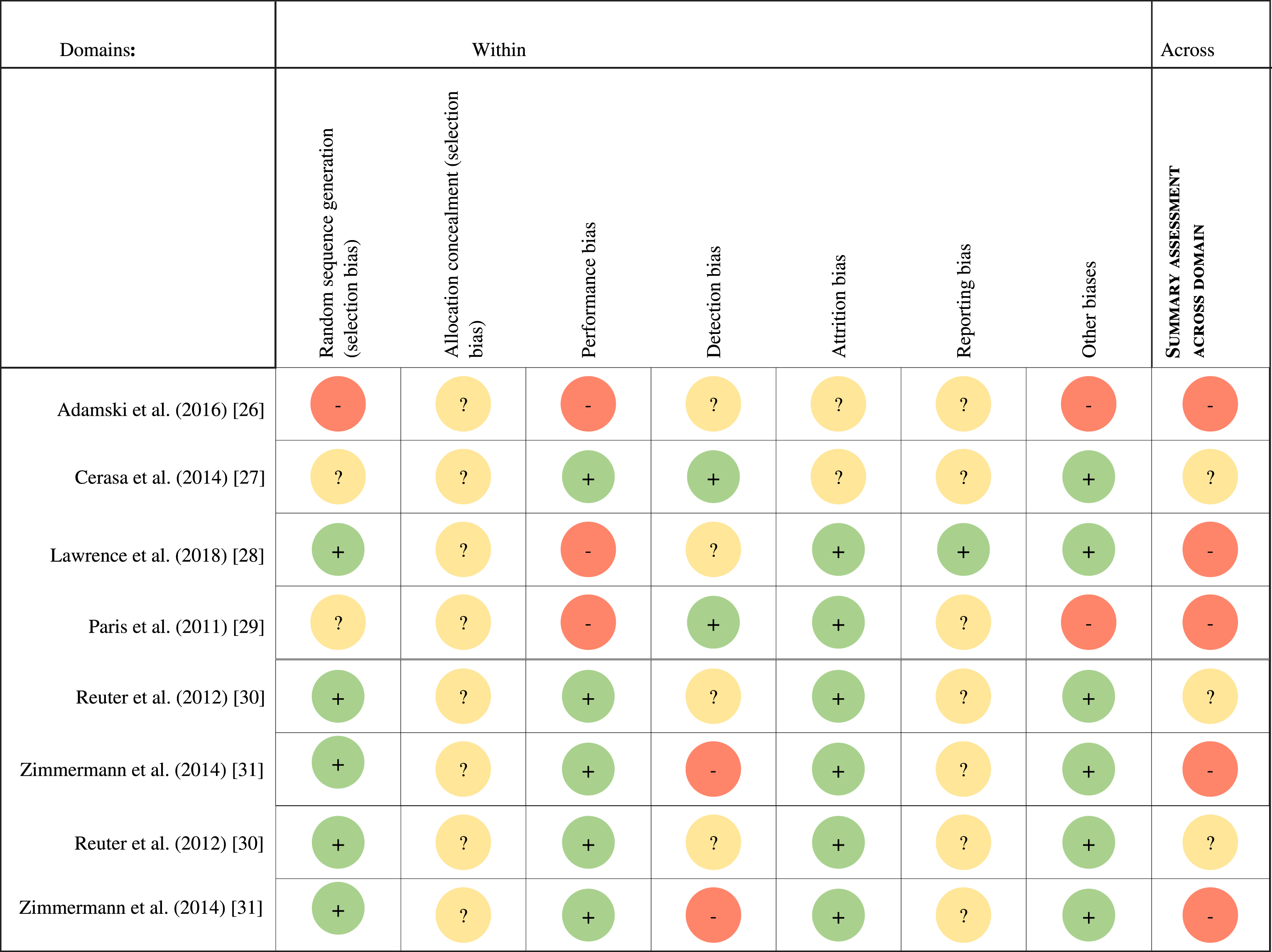
Based on the assessment of risk of bias within studies in the individual domains, Table 2 further presents the summary assessment of risk of bias within studies across bias domains.
Results of individual studies included in systematic review and meta-analysis
Of the six studies included in this systematic review, four studies were not eligible for inclusion in the meta-analysis. Adamski et al. (2016) [25] was not eligible because the control group consisted of cognitively healthy adults without PD, Paris et al. (2011) [28] and Reuter et al. (2012) [29] were not eligible because the effect of CBCR could not be isolated in these studies, and Zimmermann et al. (2014) [30] was not eligible because the primary outcome measure was an overall ‘working memory parameter’ but it was not possible to assess which working memory tests this parameter consisted of. Two studies met all the criteria for inclusion in the meta-analysis: Cerasa et al. 2014 [26] and Lawrence et al. 2018 [27].
The effect-sizes of the working memory outcome measures in the two studies included in the meta-analysis are presented in Table 3. As these were not provided by the authors,the presented data are calculated by the review authors from the data presented by the studies. Working memory outcome measures from the eligible studies were sorted regardingquality and trustworthiness, based on measures of validity, reliability and test-retest effects as outlined in the method-section. Four measures of working memory were used in the two studies included in the meta-analysispresented in Table 3. None of the studies eligible for meta-analysis used the same working memory outcome measures. Because of heterogeneity of working memory measures and heterogeneity of estimated quality of these measures, it was not deemed justifiable to perform a meta-analysis.An overall forest plot to estimate the average effect size is therefore not presented. Instead, a forest-plot is presented for each working memory measure in Illustration 1–4. An alternative method for estimating average effects is presented in the section ‘additional analysis’.
Working memory outcome measures used by included studies. Ranked based on assessment of trustworthiness
Risk of bias across studies
Based on assessment of risk of bias (Table 2), the overall risk of bias was assessed across studies. The overall risk of bias across studies was assessed to be high, meaning that the proportion of information from studies is at high risk of bias is sufficient to affect the interpretation of results.While risk of bias across studies is usually used to assess the quality of evidence, such an assessment has not been made in this review. Methodological quality was assessed by means of the within-study risk of bias, but the other areas of consideration for quality assessment, i.e. directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias, were not addressed directly. This is because the limited amount of studies with certain risks of bias means that no definite conclusions can be drawn, and that an elaborated assessment of the quality of evidence was deemed not to have made any meaningful contributions in this respect.
Additional analysis
An additional analysis was performedto estimate the difference between the percentwise increase on working memory during the intervention period between the control conditions and the intervention conditions across all working memory measures in both studies included in the meta-analysis.This analysis is presented in Table 4. The analysis revealed no meaningful differences in the average increase on working memory measures between control and CBCR conditions: On average, the CBCR interventions led to 12.1% increase in working memory performance, while an increase of 12.4% was the average forthe control conditions.
*CG, Control group; ACG, Active Control Group; PCG, Passive Control Group.
DISCUSSION
Summary of evidence
All six studies included in this review were estimated to have a high risk of bias or an unclear risk of bias, highlighting the current methodological shortcomings within this field of research.
Of the four working memory outcome measures from the two studies included in the meta-analysis, none showed significant effects of CBCR compared to an active [26] or passive control condition [27]. The additional analysis of the average percentage increase across working memory measures from the studies eligible for the meta-analysis revealed no meaningful differences between the experimental conditions and the control conditions. This additional analysis, however, should be interpreted with care because of the outlined methodological limitations of studies, the heterogeneity of outcome measures and the possible risk of bias across studies. Furthermore, the analysis does not take the variability of sample-sizes in individual studies into account. It is important to highlight that this does not necessarily reflect that CBCR is not an efficacious intervention for cognitive rehabilitation of patients withPD. It only reflects that the current literature is too sparse and methodologically limited to estimate the effects of CBCR in this context with reasonable certainty. Furthermore, the study by Reuter et al. (2012) [29] suggests, that the effects of CBCR might be increased when combined with other types of rehabilitation training, and no studies reported severe adverse effects or infeasibility of CBCR training for PD patients.
Limitations of the current literature
The studies included for both the systematic review and meta-analysis use different CBCR-programmes, which is a possible methodological limitation of the existing literature. It is still unclear exactly which variables constitute an effective CBCR-programme and therefore the question arises whether it is reasonable to evaluate the different CBCRprogrammes as one overall method, and the effects of CBCR programmes as stemming from it, or if the different programmes should be evaluated individually until greater consensus is reached about what constitutes an effective CBCR-programme.
Furthermore, because of the scarcity and heterogeneity of existing literature, it is not possible to conclude on the isolated effects of CBCR on working memory in PD. From this and other broader reviews it cannot be concluded that CBCR does not have an effect, it can only be concluded that the existing literature is insufficient to estimate effects.
Limitations of this review
The literature used in this review was derived from systematic searches in four online databases and additional contact with authors of relevant identified papers. However, the search-process was not exhaustive, as it did not include systematic screening of relevant journals in the field or attempts to contact relevant authors of papers not included in the review as proposed by Cooper (2017) [31]. As such, it cannot be ruled out that this review has failed to include existing relevant literature.
Conclusions
A total of six studies were included. Of these, two were also eligible for inclusion in a meta-analysis. Due to heterogeneity of working memory outcome measures, a meta-analysis was not deemed justifiable, and was not performed. An additional analysis of the average effects ofCBCR on working memory performance across studies included in the meta-analysis revealed no meaningful differences between intervention conditions and control conditions. However, this analysis should be interpreted with care as it does not take the heterogeneity of working memory outcome measures and the differences in sample sizes across studies into account. The overall risk of bias across studies was assessed to be high because of various methodological limitations. Overall, existing literature is sparse and provides insufficient evidence to conclude if CBCR benefits working memoryPD patients. It is important to highlight that this does not necessarily reflect that CBCR is not an efficacious intervention for cognitive rehabilitation of PD patients. It only reflects that current literature is too sparse and methodologically limited to estimate the effects of CBCR in this content with reasonable certainty.However, no studies reported severe adverse effects or infeasibility of CBCR for PD patients, suggesting it is a relatively risk-free intervention. Cognitive rehabilitation of PDis essential to maintain independency in activities of daily living and quality of life, andfuture studies with strong methodological designs are needed to further explore the effects of CBCR on working memory in PD.
CONFLICTS OF INTEREST
There are no conflicts of interest to declare regarding the conduction of this review.