
Abstract
Background:
Parkinson’s disease (PD) is an age dependent neurodegenerative disorder with increasing prevalence. Digital technologies like computers and smartphones offer mobile telecommunication, diagnostic and monitoring and may connect the patient continuously with his healthcare team, providing disease related information, and support healthcare. Since the use of these technologies in western civilization is age dependent, possession and usage cannot be regarded as given in PD. In contrast to increasing efforts to implement digital technology into PD patient care, little is known about the use of computers, smartphones, and internet-affinity in PD patients.
Objective:
To evaluate the use of digital technologies in different age groups of PD patients.
Methods:
We developed a questionnaire adapted to the annual German microcensus on “use of digital communication technologies”, allowing a comparison to the general population in Germany.
Results:
190 PD patients completed the questionnaire. About 75% of PD patients access disease related information on the internet. Patients across all age groups used computers and the internet as frequent or more frequently compared to the German population. Use of computers, smartphones, and the internet in PD was age dependent. Advanced PD patients with higher motor impairment used smartphones less often, while mobile phone usage was not reduced.
Conclusion:
The adoption of a digital lifestyle is present in the PD population, apart from smartphone usage, which is impaired by motor symptoms. Thus, future healthcare technologies are not hampered by the inability of PD patients to use the necessary tools, however, fine motor-skill requirements have to be acknowledged.
INTRODUCTION
Parkinson’s disease (PD) is the most prevalent movement disorder, affecting 0.25– 0.57% of the world’s population [1]. Males are slightly more affected, and age is the major risk factor to develop PD since the prevalence of the disease is age dependent, ranging from 0.04% in the population from 40– 49 to 1.9% in the population older than 80 [1], also in Europe and Germany [2, 3]. Importantly, in continuously aging societies around the globe, the prevalence will increase [4]. In fact, recent data already indicate an increased prevalence of about 0.5% of the German population, which is a two to three fold increase compared to data reported previously [5, 6]. During the next 30 years, the cost burden of PD for European healthcare systems will likely double [7]. In PD, change in medication is frequently required as disease progresses, and a satisfying control of symptoms is frequently not achieved [8]. The PD specific disease course results in increased consultation of the treating physician and frequent change of treatment regimens, resulting in side effects of dopaminergic treatment leading to hospitalization. In the US, most of the medical costs in outpatient care are due to physician’s office visits [9]. In this context, health technologies may offer unbiased monitoring options that may be as efficacious as usual in-person care [10], and thus change healthcare industry, also due to their cost saving potential [11]. Patients and physicians may profit from the use of computers and smartphones by enabling and simplifying the connection of the patient to his healthcare team. Currently a variety of trials are designed that aim to assess the feasibility and benefit of these technologies (i.e., [12–14]). Beneficial effects may range from engaging physical activity and participation [15] to a continuous and objective monitoring of motor and non-motor symptoms [16–18]. Recently, the MDS Technology Task Force and the MDS Rating Scales Program Electronic Development Ad-Hoc Committee summarised characteristics and developmental steps for a technology-enhanced e-Diary, usable in both clinical practice and treatment trials [19].
Smartphones with their advanced set of sensors and connectivity can either directly be used as monitoring [19] and treatment tools [20] or alternatively serve as a hub to store or transmit data derived from wearable sensors [15]. However, with the iPhone© being introduced in 2007, this technology is less than a decade old. Yet, information on the mobile data of PD patients using the iPhone© has been published [21]. Computers on the other hand are more stationary and most frequently used at home. Their high storage capacity may be particularly useful for home monitoring concepts that use storage intensive assessments like video monitoring.
Since the use of these technologies in Western civilization is age dependent [22], possession and frequent use of these technologies in PD patients cannot be regarded as given. However, a recent study revealed that currently about 25% of Germans older than 60 years possess a smartphone, whereas only 4% did so in 2012 [23]. Thus, smartphones increasingly become a communicative tool for the elderly and will be an important prerequisite for active engagement of patients and caregivers. In contrast to the increasing effort to implement digital technology into patient care in PD [24], little is known about the use of computers and smartphones and internet affinity in PD patients. In general, the applicability of these technologies in chronic disease such as PD depends on the affinity of the target population as well as the capability to use these tools. Several motor and non-motor symptoms in PD may hinder proper handling of i.e. smartphones [25], or computers. Moreover, impaired cognitive function may impede improvident use of these technologies and navigating the internet.
Therefore, we have developed a questionnaire evaluating the use of computers, internet, and smartphones in German PD patients. Part of the questions were adapted to the annual microcensus on the “use of information and communication technologies in Germany” by the German statistical federal office (Statistisches Bundesamt; Destatis; [26]), enabling comparison to the general population in Germany.
METHODS
This study was granted by the local ethics committee (No 344_14Bc).
Questionnaire
We have generated a questionnaire consisting of 29 questions in total, 8 demographical questions and 21 questions to obtain information on the use of digital technology and media in PD. The 29 questions consist of 8 multiple choice questions, 4 yes/no questions, 7 questions allowing multiple answers, 7 questions containing multiple y/n answers and 3 open question allowing a text-based answer. Questions 10 and 11, 12– 14, 15– 18, and 19– 23 are hierarchically structured. Therefore i.e. question 11 could only be answered if the answer in question 10 was “no”. In general, completion of the questionnaire was satisfying. Across the dataset, 23.68% of the variables were incomplete, 7.9% of participants did not completely fill out the questionnaire. This leads to a percentage of only 0.312% of nonhierarchical data that were missing. Missing values for hierarchically structured questions were below 0.9% (question 23_1). For more details on missing data see Supplementary Figure 1. Six questions (questions 12– 18) were adapted to the 2015 microcensus on the use of information and communication technologies in Germany. Data on five age dependent groups (< 45 years, 45– 54 years, 55– 64 years, 65– 75 years,>75 years) was kindly provided by the Statistische Bundesamt Germany [26]. A detailed summary of the questionnaire is provided in Table 1. The English version of the German questionnaire is provided in the Supplementary Material.
Summary of the questionnaire and the category of questions asked
Statistical analysis
All data were analyzed using IBM’s SPSS software (Version 21.0). A significance level of p < 0.05 was set to be statistically significant; significance levels are indicated as follows: ***p < 0.001; **p < 0.01; *p < 0.05. Data are given as mean±standard deviation (SD) if not indicated otherwise. Patients were grouped into 5 age dependent groups matching the groups of the microcensus. Of the 190 patients, only 3.6% (n = 7) were aged < 45. In this age group, the expected frequencies when analyzing categorical multiple-choice questions were below 5. Therefore, this group was not included into statistical analysis of categorical data. For the remaining four groups, the overall effect of age group on categorical variables was analyzed using Pearson’s χ2. Z-test (with Bonferroni correction) was used to detect differences between groups in case a significant effect was observed. Differences in the motor score of the Unified Parkinson’s Disease Rating Scale (UPDRS III) were analyzed using one-way analysis of variance (ANOVA) with Bonferroni post-hoc testing for group comparison. Comparison to the German population was performed in a qualitative way without statistical testing.
RESULTS
Study population
PD patients were recruited from 2014 to 2016 in two movement disorders outpatient units in Germany (Department of Molecular Neurology, University Hospital Erlangen and Movement Disorders Clinic, Beelitz-Heilstaetten). Diagnosis of PD was made according to the guidelines of the German Society of Neurology, which are similar to the UK PD Society Brain Bank criteria for diagnosis of PD [27].
In Erlangen, questionnaires were sent to a total of 202 PD patients. Patients were asked to fill out the questionnaire and send it back. In total 131 questionnaires were returned and completely filled. For the completion of this questionnaire, the participants were not informed that they could use assistance, even though this was not forbidden per se. The 71 patients who did not return the questionnaire did not differ in age, disease duration or Hoehn and Yahr (H + Y) disease stage, however motor impairment was significantly higher (24.64±12.69 vs. 19.28±11.5, ANOVA: F(1,194) = 9.633, p < 0.05, Fig. 1). In Beelitz, 59 questionnaires were handed out to PD patients during their regular visit at the outpatient center. Patients were asked to fill out the questionnaire and anonymously return it after completion. Here, all questionnaires were returned.
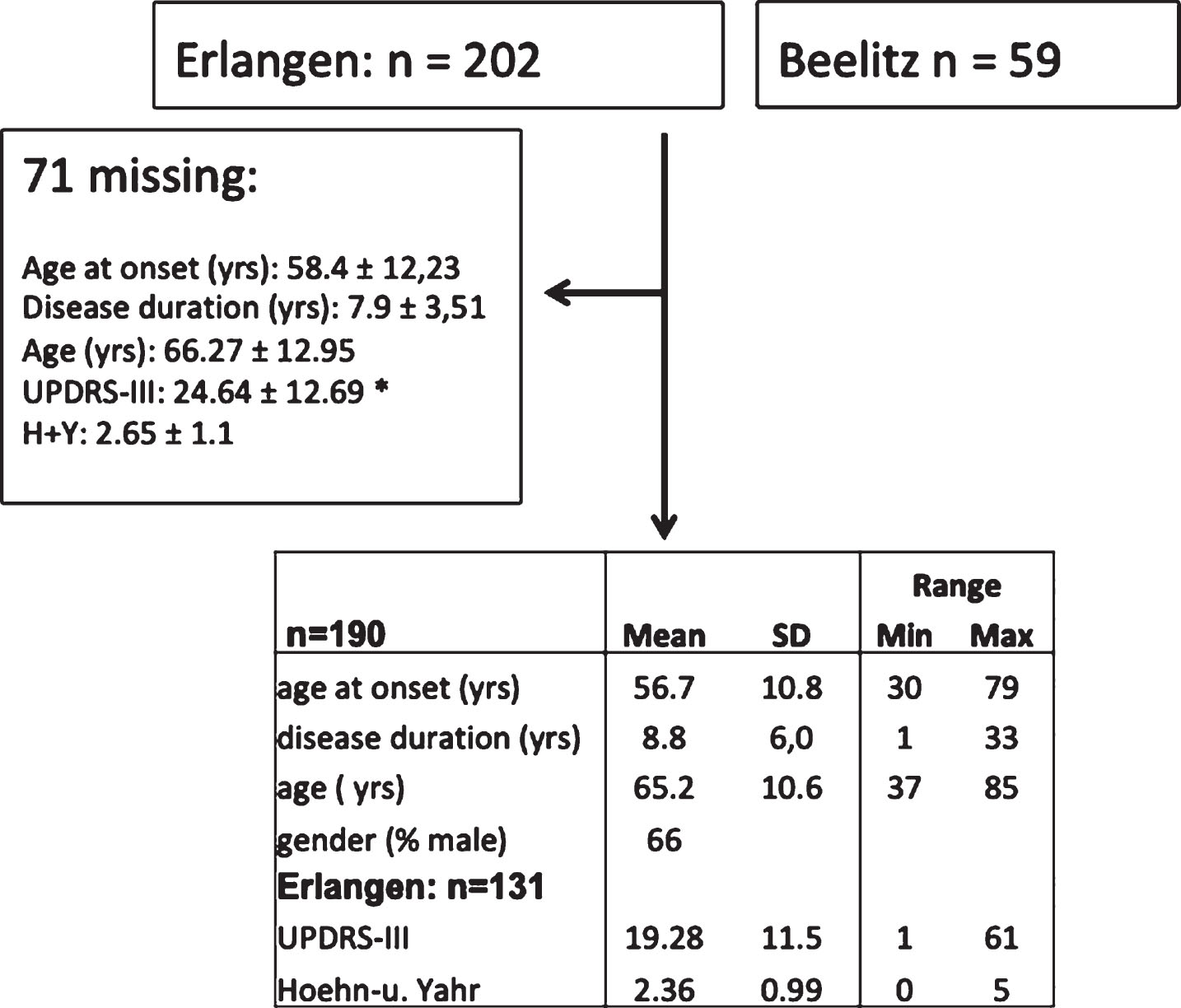
Study population. In Erlangen, 202 questionnaires were handed out, 131 were returned. 71 questionnaires remained unreturned (65% return rate). Participants that did not return the questionnaire differed in UPDRS III ratings, only. UPDRS and H + Y were available for the Erlangen cohort, only. In Beelitz, 59 questionnaires were handed out and returned. Data are presented as mean±SD. *indicates significant differences of p < 0.05 compared to the study population.
Clinical information on disease duration, disease stage (H + Y [28]), motor impairment in the on state (UPDRS III [29] were available for all PD patients recruited in Erlangen. The age at disease onset (defined as the year in which first symptoms of motor impairment were reported by the patient or relatives), gender and disease duration were extracted from the questionnaire (questions 26– 28).
Demographical characteristics
In total, 190 PD patients (66% male) with a mean age of 65.2±10.6 years and mean disease duration of 8.8±6.0 years completed the questionnaire (Erlangen n = 131; Beelitz n = 59, Fig. 1). For the Erlangen cohort, the mean H&Y was 2.36±0.99 with a mean UPDRS III of 19.28±11.5. There was no effect of age group on disease duration (F = 2.348; p = 0.076), UPDRS III (F = 2.380; p = 0.073) and H&Y stage (χ2 = 5.23; p = 0.156; for details, see Supplementary Figure 2). Age had no influence on the housing situation, but had a significant impact on the care level received (χ2 = 32.441, p < 0.001). Significantly less PD patients older than 75 received no care level (p < 0.05; Table 2). Overall, age did not influence educational background as measured by the training received (χ2 = 20.2 p = 0.063). However, in the age group between 55 and 64 less people had a university degree but received vocational training compared to the other groups (p < 0.05; Table 2). Compared to the general population in Germany (with about 16% having a university degree, [30]), 45.3% of the participating PD cohort had a university degree.
Demographic characteristics. Characteristics are presented in percent, *indicates significant differences of p < 0.05 compared to the other groups (Bonferroni post hoc analysis)
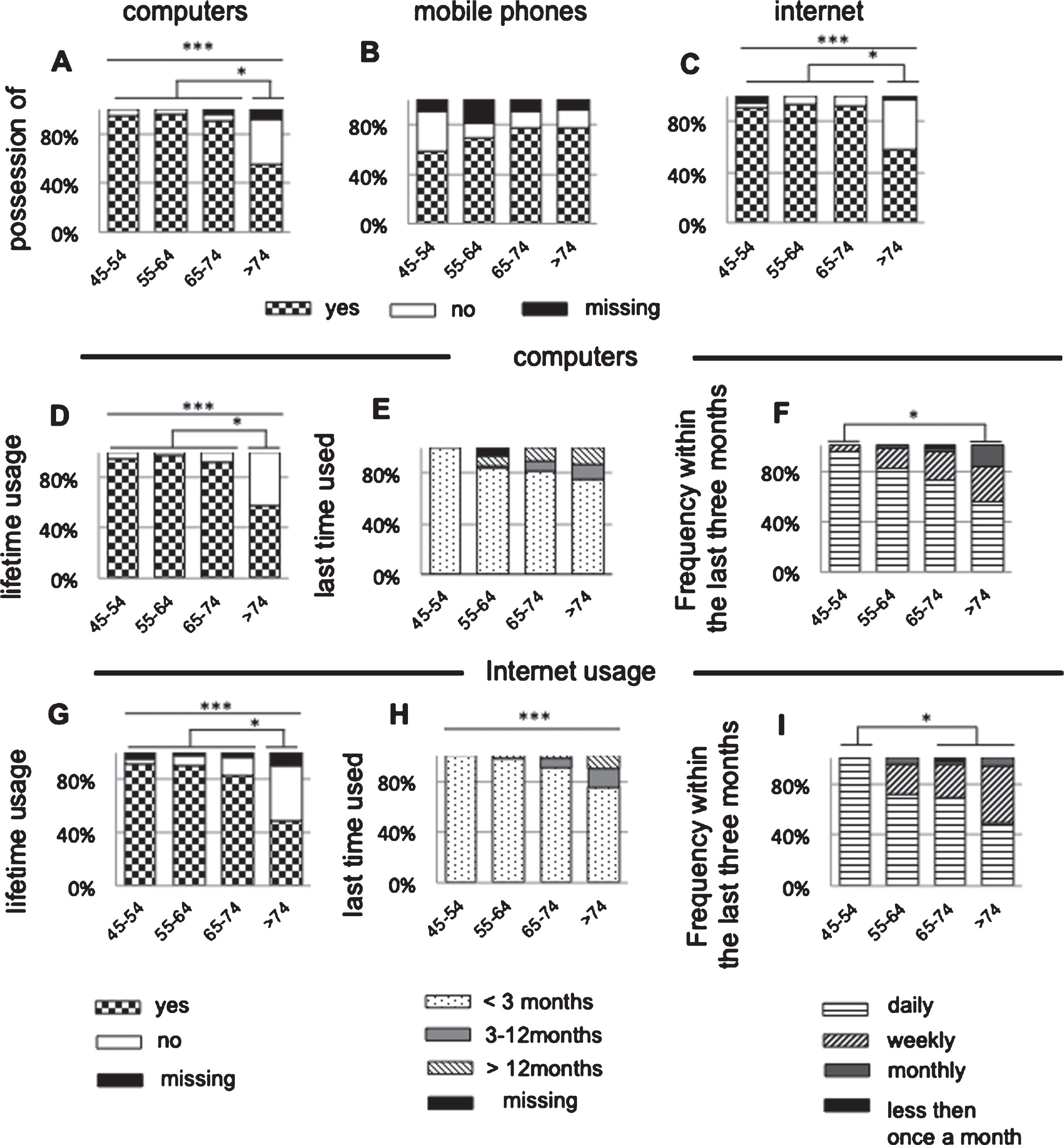
Possession and lifetime usage of computers, mobile phones and the internet in PD. Possession of digital technologies (A-C), usage of computers (D-F) or the Internet (G-I) in 4 age groups. *indicates p < 0.05, **indicates p < 0.01, ***indicates p < 0.001.
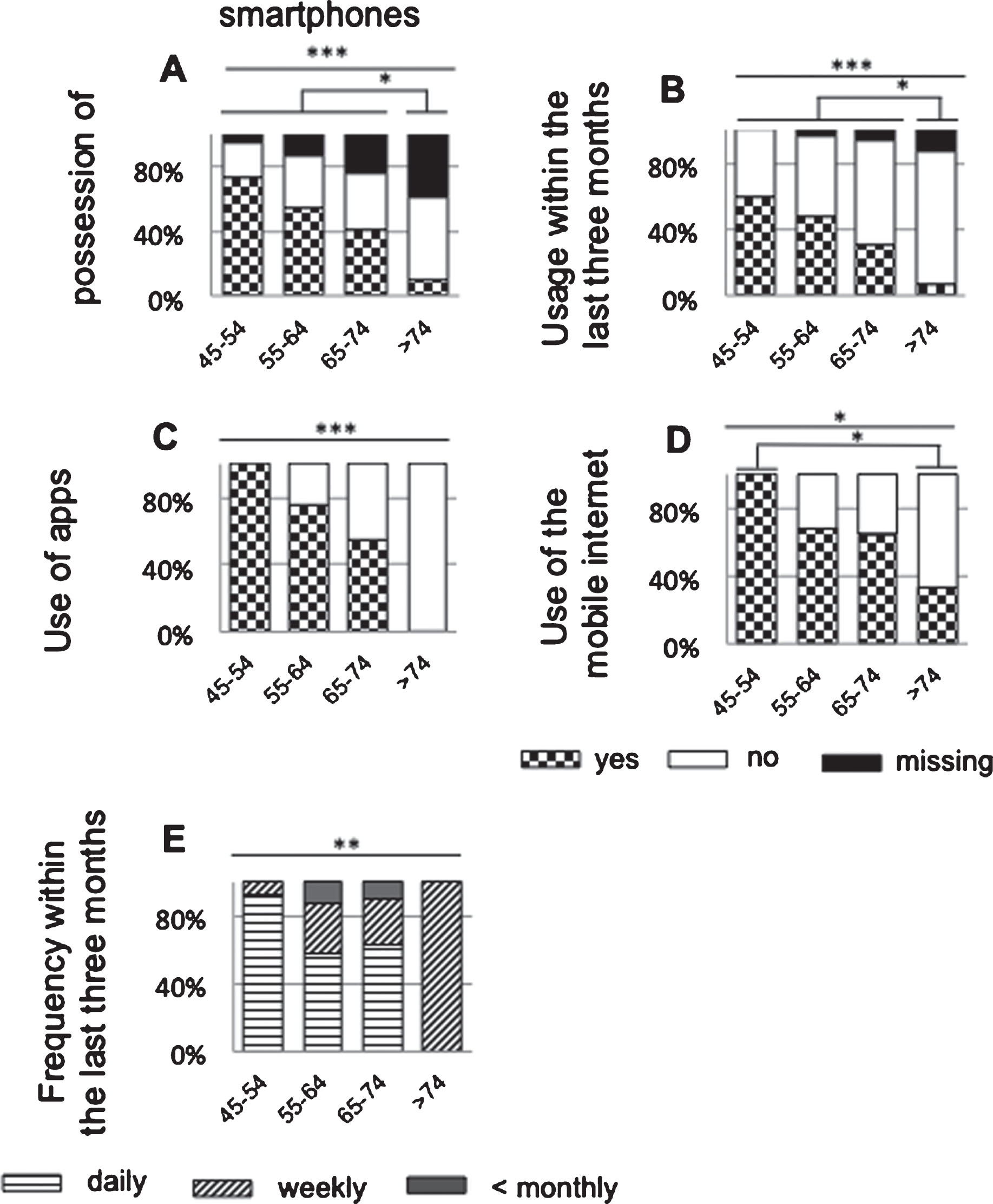
Possession and usage of smartphones in PD. Possession of smartphones and usage within the last three months (A-B). Use of Apps or the mobile internet (C-D). Frequency of smartphone usage within the last three months (E). *indicates p < 0.05, **indicates p < 0.01, ***indicates p < 0.001.
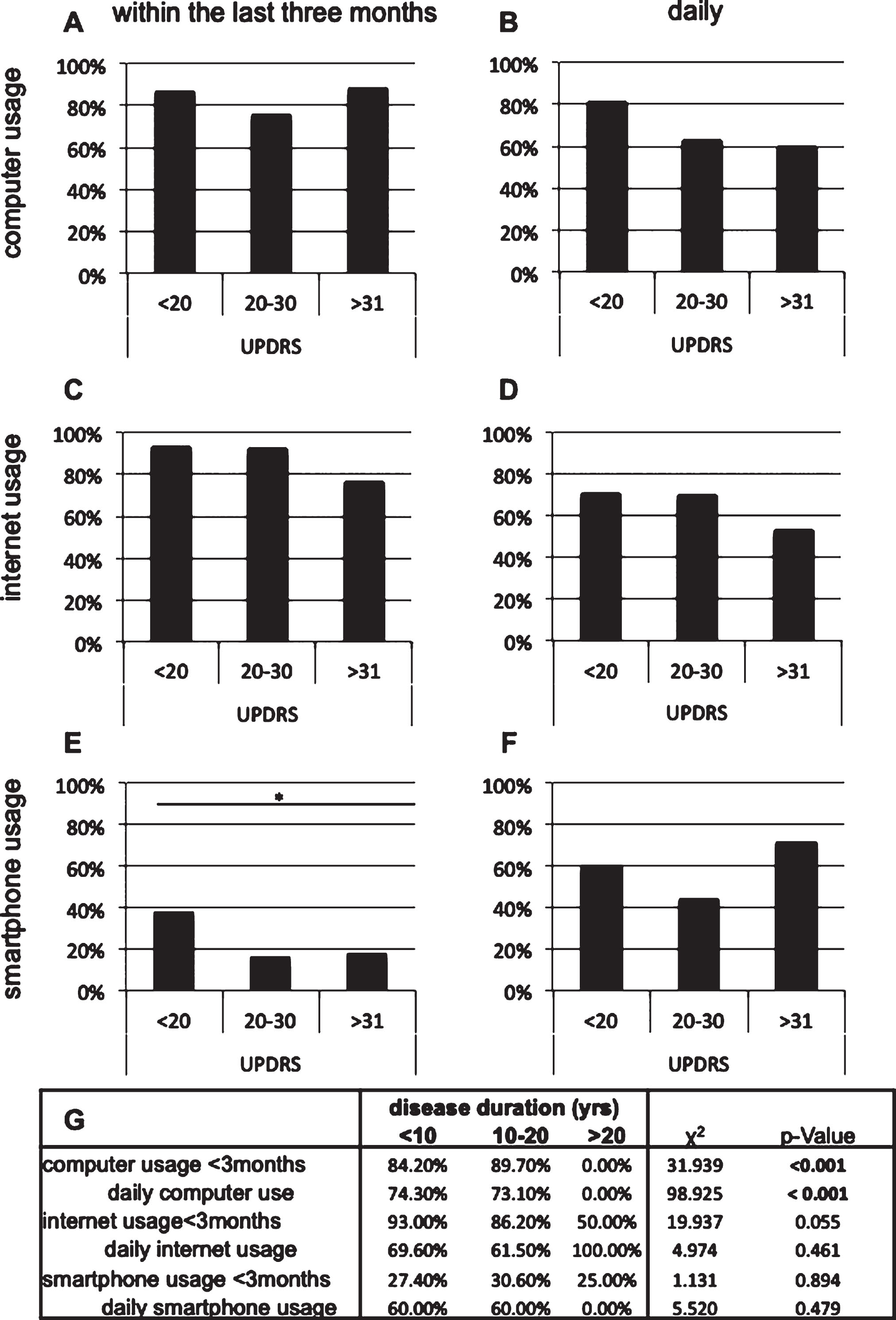
The influence of motor impairment and disease duration on the use of digital technology. Use of computers (A-B), the internet (C-D), and smartphones (E-F) within the last three months (A, C, E) or daily (B, D, F) with respect to the level of motor impairment as measured by the UPRS-III (A-F) and disease duration (G). *indicates p < 0.05.
Possession and usage of computers and mobile phones
Influence of age
Age had a significant influence on the possession of a computer in PD patients (χ2 = 36.4; p < 0.001). In particular, less patients older than 75 owned a computer compared to all other age groups (Fig. 2A). In contrast, age did not influence the possession of a mobile phone (χ2 = 9.354 p = 0.155; Fig. 2B). Use of computers was age dependent (χ2 = 37.244 p < 0.001). In our cohort, only 5% in the age group of 45– 54-year-old patients have never used a computer, whereas 41.5% in the age group of > 75 year olds have not used a computer so far (Fig. 2D). The last time a computer was used did not differ between age groups (χ2 = 14.338; p = 0.11; Fig. 2E), and on average 84% of all participants, that have used a computer once in their lifetime, have used it within the last three months. Overall, age did not have a significant influence on the last time a computer was used and the frequency of computer usage within the last three months (χ2 = 16.477 p = 0.058; Fig. 2E, F). Yet, while 95% of PD patients in the age group of 45– 54 use a computer daily, only 55.6% of those aged > 75 do so (p < 0.05, Fig. 2F).
Influence of motor impairment
Motor impairment as measured by UPDRS III ratings in the Erlangen subpopulation did not impede computer usage. The majority of PD patients with lower motor impairment (UPDRS < 20) used a computer and the internet within the last three months (Fig. 4A, C) mostly on a daily basis (Fig. 4B, D) which was not statistically different from PD patients with intermediate (UPDRS 20– 30) or severe motor impairment (UPDRS > 30).
Use of the internet
Possession of an internet account was age dependent (χ2 = 33.006 p < 0.001; Fig. 2C). In particular, fewer patients aged 75 years or older did not own an internet account. Everybody in the age group of 45– 54-year-old patients has used the internet at least once in their lives, whereas only 58.5% in the age group of > 75 year olds have used the internet so far. Thus, lifetime usage of the internet was age dependent (χ2 = 29.120 p < 0.001; Fig. 3G), so was the last time the internet was used (χ2 = 13.554; p < 0.05; Fig. 3H). The frequency in which the internet was used within the last three months did not differ across groups (χ2 = 14.241; p < 0.114). Post hoc analysis revealed a significant difference between daily internet usage between patients aged 45– 55 and those older than 65 (Fig. 3I). Information on the purpose for which the internet was used is provided with the Supplementary Figures 3 and 4.
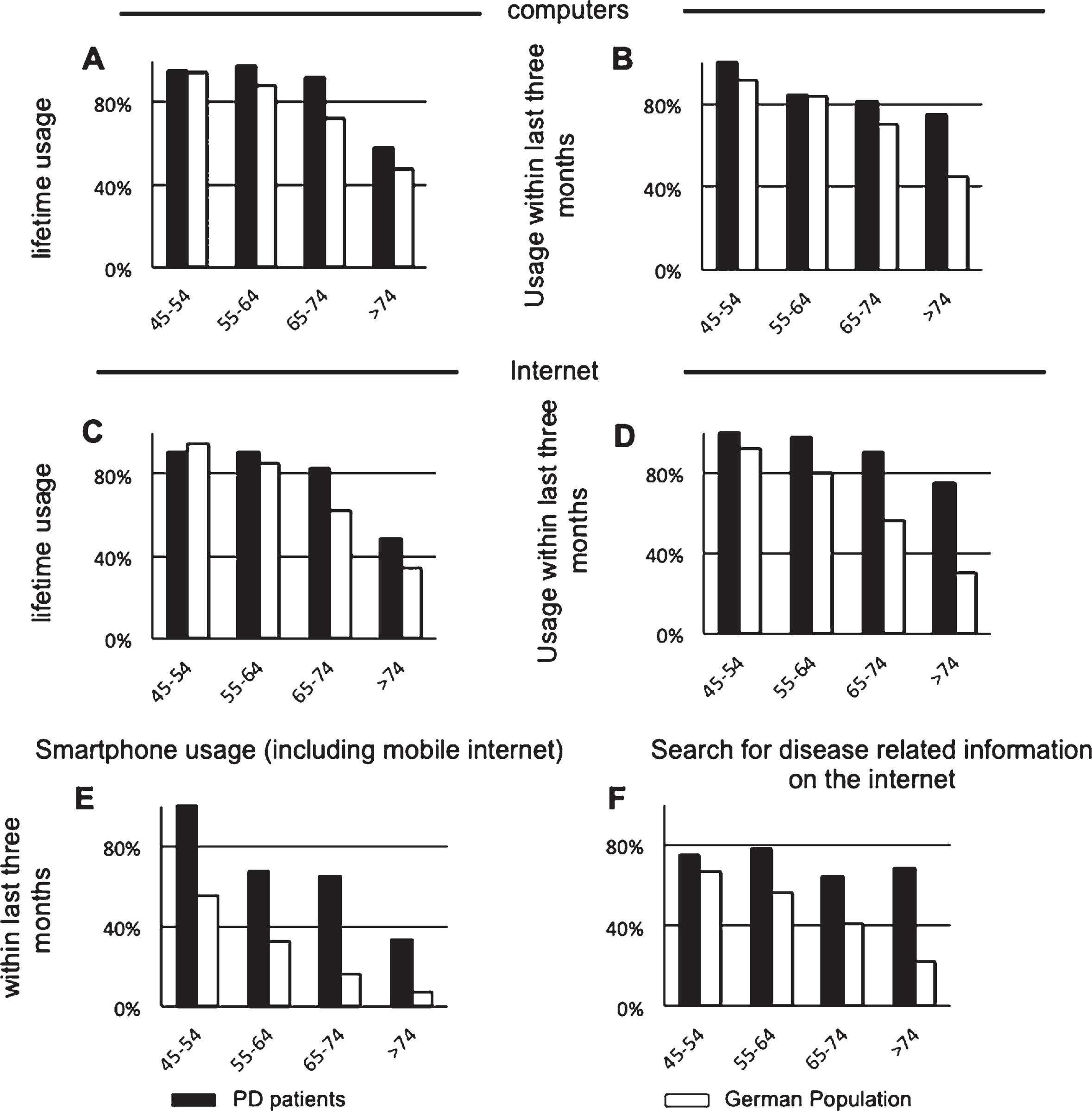
Usage of digital technology in PD is not reduced compared to the German population. Compared to the German population (white bars) lifetime usage (A, C) and Use within the last three months (B, D) of Computers (A, B) and the Internet (C, D) was comparable or higher in PD patients (black bars). Smartphone usage within the last three months and search for disease related information on the internet was even more frequent in PD than within the overall German population.
Use of smartphones and the mobile internet in PD patients
Influence of age
The possession (χ2 = 31.666; p < 0.001; Fig. 3A), and usage of a smartphone within the last three months was age dependent (χ2 = 25.188 p < 0.001; Fig. 3B). In particular, patients aged > 75 used a smartphone significantly less often within the last three months compared to the other groups. Patients that used a smartphone within the last three months were asked to provide information about the use cases. While making calls, text messaging, taking pictures and playing games did not differ between age groups (data not shown), the use of apps (χ2 = 15.281; p < 0.001; Fig. 3C) and the mobile internet (χ2 = 7.987 p < 0.05; Fig. 3D) decreased significantly with age. Also, the frequency of using the mobile internet within the last three months was age dependent (χ2 = 25.236; p < 0.01; Fig. 3E).
Influence of motor impairment and disease duration
Moreover, motor impairment significantly influenced the percentage of PD patients that used a smartphone within the last three months (Fig. 4E). However, patients who used a smartphone within the last three months did not differ in the frequency of smartphone usage (Fig. 4F), independent of motor impairment.
Influence of disease duration
Disease duration did not have an influence on the percentage of PD patients that used a smartphone within the last three months or on the frequency of smartphone usage within those three months (Figs. 4 and 6). Reasons for using the mobile internet are provided in Supplementary Figure 4.
Comparison to the general population in Germany
In comparison to the general population in Germany, a similar (age groups 45– 54 and 55– 64) or higher (age groups 65– 74 and > 74) proportion of PD patients have at least once in their lifetime used a computer (Fig. 5A). While computer usage within the last three months appears to be similar until the age of 64 it may be higher in older PD patients, in particular in PD patients older than 74 (Fig. 5B). Lifetime internet usage, as well as usage within the last three months may be higher in PD patients, especially in the age groups 65– 74 and > 74 (Fig. 5C, D). Also, a higher percentage of PD patients may use a smartphone across all age groups compared to the general population in Germany (Fig. 5E). Finally, a higher percentage of PD patients seem to search health/disease related topics on the internet compared to the German population (Fig. 5F).
DISCUSSION
In this explorative, questionnaire-based, cross-sectional study, performed at two movement disorders centers in Germany, we addressed the use of digital technologies, namely, computers and mobile-/smartphones, and the disease-related utilization of the internet in PD patients. Whereas the overall use of computers was not influenced by age in PD compared to age-matched controls, smartphone usage was. The frequency of computer usage however decreases upon aging in both cohorts. Yet, PD patients across all age groups have used computers and the internet as frequent or more frequently compared to the general German population. While smartphone use was influenced by motor impairment, the general usage of mobile phones was not altered, indicating difficulties in using a smartphone with increasing motor impairment. Independent of age, a higher percentage of PD patients gathered disease related information on the internet compared to the general German population. However, the high amount of participants with higher education level is a relevant confounder when interpreting these results.
Adoption of a digital lifestyle is not reducedin PD
These observational data suggest that the adoption of a digital lifestyle is in general not reduced in PD. Participants were capable of using a computer for gathering disease related information on the internet. Since computers were accessible to most PD patients, they are available as data transfer systems for telemonitoring concepts in most households [15]. Also, internet-platform based communication with the patient is possible via this technology. Yet, in higher age-groups (>75) communication via computers was less frequent, and therefore the usability of smartphones has to be improved and the patients may have to be specifically trained in their application.
Smartphone adoption and usage in PD patients
Recently, the Parkinson @home study revealed the feasibility to collect objective data using smartphones and sensors [14]. Yet, possession of a smartphone was an inclusion criterion. Here, we provide evidence that the distribution of smartphones currently decreased stronger with age than computer possession, but the distribution will increase rapidly within the next years [23]. Therefore, more and more PD patients will gain access to smartphone-integrated technology and software, overcoming the low use of the mobile internet and apps present in this study. Since apps are not used by the majority of older PD patients, these age-groups may currently be underrepresented in studies using apps to obtain information about PD patients. Also, when using apps as monitoring options in clinical studies, a proper teaching of older participants may be necessary. Since motor impairment influenced smartphone usage, apps should be designed to be usable even by patients in an advanced disease stage. This may be of particular importance in trials that aim to assess the acceptability of digital health platforms in PD [12].
Limitations
With regards to geographic transferability of the data presented in this study, demographic and economic factors of the German population differ from other countries. Also economic differences may influence the accessibility to the digital media analyzed in this study. Yet, while the German gross domestic product is the 4th largest worldwide, data provided in the Global Information Technology Report 2016, reveal that Germany ranks place 16 in Internet users, place 11 in households with a personal computer, place 15 in households with Internet access, and place 39 in mobile broadband Internet subscriptions. Therefore, while the German population has a rather good access to personal computers and the internet compared to other countries, the German population ranks only average in terms of mobile digital technology [31].
Thus, gross domestic product does not appear to directly translate into accessibility to digital media. The general conclusion of the manuscript that, in an increasingly ageing society, age as the most important risk factor for PD must be considered when speaking about the implementation of digital media is likely transferable to other countries. Especially, the fact that motor impairment, which is influenced by disease duration negatively impacts the use of smartphones, can be deducted to impact PD patients independent of their country of origin.
In addition to motor-impairment, cognitive impairment, which occurs in PD in up to 40% in the course of the disease [32] may additionally influence the use of digital technologies. Since we designed the questionnaire to be comparable to the annual microcensus in Germany, which assesses the aspects of digital media use in age cohorts, data on cognitive impairment were not assessed in this dataset. However, the proportional role of motor impairment and/or cognitive impairment in the inability to use digital media is a yet unexplored research question and subject of future studies, that should not only assess motor impairment, but also non-motor symptom burden and cognitive status to provide this crucial piece of information to the scientific community.
The biggest shortcoming of this study is the fact that our PD cohort had a significantly higher educational level than the general population in Germany [30], most likely due to an institutional bias. Therefore, the observed differences in the use of computers, internet and smartphones may be influenced by the educational level. Thus, the data presented here must be interpreted with caution when making general assumptions about adoption of digital technologies in, i.e., the total PD population in Germany. Here larger, and epidemiologically more robust data, reflecting demographics of a population more closely are necessary to provide evidence for the adoption of digital technologies in PD without educational bias. A loglinear regression model that could correct for this confounding variable and provide more authoritative statistical information on the interaction of age and motor impairment would have needed a significantly larger amount of participants to reach the statistical power necessary to calculate this model. Moreover, a significant amount of missing data was evident when patients were asked about the possession of smartphones with an age dependent increase in missing answers. This indicates, that the term “smartphone” may not be familiar to older participants. Therefore, future questionnaires addressing this topic should provide a definition or example of a smartphone to increase comprehension. Hence, the data presented here remain descriptive in nature. Furthermore, it is unclear how many patients participated in digital interventions, while our questionnaire-based assessment was conducted. Yet, since no such trials were ongoing at the two academic research centers involved in this study, we believe that this is a negligible amount.
Conclusion
Nevertheless, these data support the notion, that future healthcare technologies are not hampered by the inability of PD patients to use the tools necessary, with the limitation of smartphone usage in older cohorts with high levels of motor impairment. The data presented here imply, that in 10 years from now, more than 2/3 of PD patients aged 65 or older possess smartphones.
In general, our data provide evidence that the PD population is accessible by digital media already now. Considering the overall high percentage of smartphone usage compared to the general German population across all age groups, and the high percentage of using the internet to gather disease related information in the PD cohort, future digital health technologies meet a well prepared and digitally educated cohort. Since motor impairment influenced smartphone usage, apps should be designed to be usable even by patients in an advanced disease stages. This may be of particular importance in trials that aim to assess the acceptability of digital health platforms in PD [12]. Future studies should address the influence of education on adoption of digital technologies as well as regional differences across Europe to provide a more complete picture about the accessibility of the PD population via digital technologies.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.