
Abstract
Background/Objective:
Easily applicable, quantitative assessment of movement is widely needed in various clinical settings, especially in the evaluation of Parkinson’s disease (PD).
Methods:
We developed a highly repeatable tablet computer-based finger movement assessment system (FMAS) to record finger movement profile in a visual-motor task both in PD (n = 217) and healthy participants (n = 221).
Results:
We found age-related declines in finger movement performance among the healthy participants but not in PD patients with the FMAS. Significant differences in movement time (MT) and latency/MT ratio but not in latency were observed in PD patients as compared with healthy subjects (P < 0.000). Meanwhile, we identified the latency/MT ratio as the optimal parameter to differentiate PD from age-matched healthy subjects in an age-independent manner (cut-off 1.08 with corresponding AUC = 0.861). In addition, a significant correlation was found between finger movement parameters and the Hoehn and Yahr scale (H-Y scale), UPDRS III score and the duration of the disease in PD patients (P < 0.01).
Conclusion:
It was suggested that the tablet computer-based evaluation of finger movement provided an easily applicable quantitative method to assess the conditions of PD patients.
Keywords
INTRODUCTION
Parkinson’s disease (PD) is one of the commonest neurodegenerative diseases among elderly people, and is clinically characterized by bradykinesia, resting tremor, rigidity, and postural instability. The slowness of movement in speed and amplitude, known as bradykinesia, is the cardinal symptom which is fundamental to the assessment and diagnosis of PD. However, bradykinesia is a symptomatic description that is generally obtained by subjective judgement, where accurate assessment is needed. Therefore, quantitative movement assessment would potentially enhance the diagnosis and management of PD.
The composition of voluntary movement could be generally divided into two segments, premovement phase, also called latency, which refers to the time for movement preparation and planning, and movement [1]. Voluntary finger movement is one of the fine motor skills employed in most daily tasks and requires a wide scope of neuro-motor integrity, including visual-motor coordination and neuromotor control. Most movement disorders including PD affect the movement latency and speed, leading to voluntary task disturbance. Slowness of finger movement in PD patients has been described by some investigations [2, 3], and alteration of finger movement is a predictive factor for levodopa response [4]. Although several approaches [5–12] have been used to measure movement in various clinical settings, there is still a lack of a simple and easy approach to quantitatively measure both movement latency and speed in the visual-motor tasks.
In this study, we designed an easily-applicable, tablet computer-based system (finger movement assessment system, FMAS) to simultaneously assess both finger movement latency and finger flight speed in a visual-motor task, and evaluate its power in assessing hypokinesia in PD patients.
MATERIALS AND METHODS
Participants and clinical measurement
Two hundred and seventeen PD patients (109 men and 108 women) and 221 healthy participants (100 men and 121 women) were included in this study (Table 1). The diagnosis of PD was based on the UK Parkinson’s Disease Society Brain Bank Clinical Diagnostic Criteria [13] and PD patients were registered consecutively from the Clinical Research Centre for Movement Disorders of Shaanxi Provincial People’s Hospital from August 2013 to September 2016. Healthy participants were from age-matched spouses, caregivers, relatives of the patients and volunteers without known diseases that might affect finger movement. All participants were right-handed by self-report and there were no ambidextrous persons. Exclusion criteria for all participants included: (1) the subjects who had reported obvious visual, joint, skeletal motor problems and other illnesses and medications that might influence the performance of the task; (2) a Mini-Mental State Examination (MMSE) score <24; (3) Parkinsonism that were caused by diseases other than idiopathic PD, such as multiple system atrophy, progressive supranuclear palsy, and side effects of medications. The above-mentioned conditions were ruled out through careful medical history reading, neurologic examination, and neuroimaging. The PD patients were assessed with UPDRS III and Hoehn-Yahr score during their “off” period immediately prior to the assessment by an experienced neurologist. Frequencies of anti-Parkinsonian medications among PD patients (n = 217) were as follows: Levodopa 38.7% at a mean L-dopa equivalent dose (LEDD) of 316 mg (range 0–1200 mg), dopamine agonists 24.4%, antidepressants 16.1%, monoamine oxidase B inhibitors 7.8%, amantadine 5.1% and COMT inhibitors 4.6%. Among the PD patients, 158 (72.8%) had purely unilateral symptoms at the time of testing. The protocol of this study was carried out in accordance with the recommendations of the Ethics Committee of Shaanxi Provincial People’s Hospital, the Third Affiliated Hospital of Xi’an Jiaotong University School of Medicine, and written informed consent was provided by all the participants before enrollment into the study.
Characteristics of PD and control participants
Data are presented as mean±SD. PD, Parkinson’s disease; MT, movement time; Ratio, Latency/MT. #P > 0.05, as compared with left.
The design of finger movement assessment system (FMAS)
Finger movement in a visual signal-stimulated task was divided into two domains. The first was latency, defined as the time elapsed from visual signal appearance to the initiation of finger movement. The second phase was movement time, defined as the time for finger flight from the start point to the destination. To fulfill the purpose of obtaining the two key parameters, with the consideration for clinical convenience and availability, we developed the system for finger movement assessment based on a visual-motor task and utilized a tablet computer (Samsung Galaxy Tab A 10.1), which had a multi-point capacitive touch screen with a 10.1-inch rectangular surface. Five virtual stimulus buttons of 8 mm in diameter were located on a circle arc 22.5° apart with each stimulus button, 150 mm away from the central start button (Fig. 1). The visual motor task was initiated by touching the central start button with the participant’s index finger. One of the five stimulus buttons then lit up in a random manner (to avoid the habitual formation that might affect the finger movement). The participant was then required to touch the stimulus button as quickly as possible by moving the same finger from the central start button. Latency was defined as the time elapsed between the point when the stimulus button turned on and the release of the central start button. Movement time (MT) was defined as the time between the release of the central start button and hitting the stimulus button. Latency and MT were measured with millisecond (ms). The resolution of the timer embedded in the touch pad reached in ∼5 ms as was indicated by the manufacturer. The accuracy of the FMAS was verified by a pressure sensor implemented under the touch-pad, and a high-speed video camera embedded on the desk, showing that movement time recorded by FMAS was in good consistency with the two methods. All these procedures and the interface were driven by dedicated software named FMAS Version 3.0 developed by Dr. Yutao Yang from Xidian University in China. The software has been tested in a variety of other touch pad devices with Android operation system (including Xiaomi Mi Pad 4 Plus, Lenovo TAB4 TB-X304N, and HUAWEI Tablet M6).
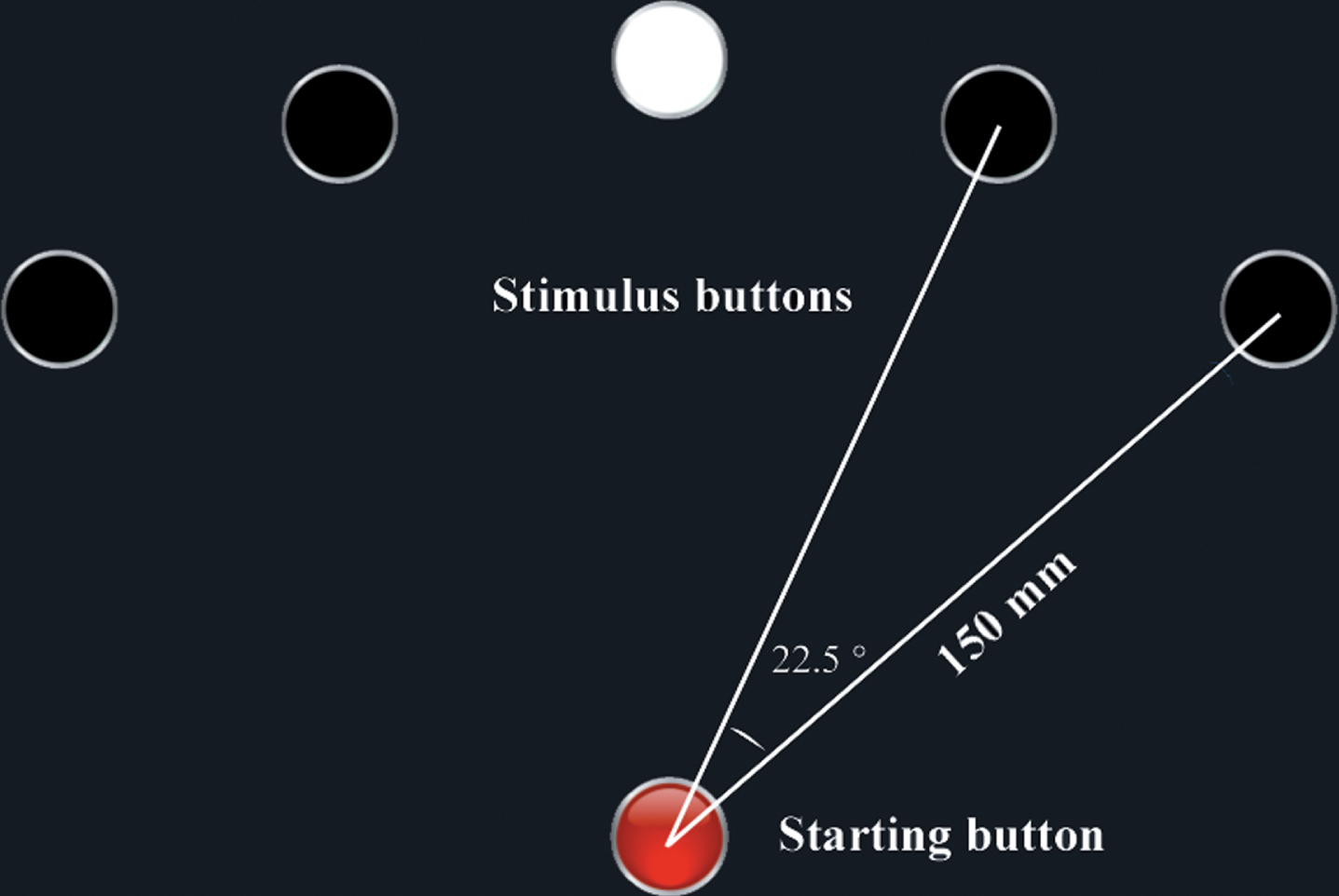
The interface of tablet computer for assessing finger movement in a visual-motor task. The tablet computer has a multi-point capacitive touch screen. Five virtual stimuli buttons (white circles), with equal 150 mm distance from the central start button (red) located on the lower part of the screen, were in the upper screen. Each test started with the subject touched the central start button with their index finger. On the demand of the start button, one of the five stimulus buttons would turn on in a random manner. The pariticipant was then required to touch the stimulus button as quickly as possible by moving their index finger from the central start button. Latency was defined as the interval between when the stimulus button light turned on and the release of the central start button, while movement time (MT) was defined as the interval time between the finger departure from the central button to the touch of the stimulus button. The subjects performed repetitive 30 times. The inner computer timer automatically calculated the first quartile Q1 of 30 repetitive latency and MT.
A test consisted of 30 repeated tasks and the whole procedure took less than 3 min. Each participant was instructed to understand the task by a medical staff member or a demonstration video clip prior to the test. Due to the fact that most of the record data of 30 repetitive tasks did not meet the distribution of normality in the pilot study, and the mean value of these records might be greatly affected by a few aberrant ones, we used the first quartile Q1 value of latencies and movement time of 30 repetitive task performances as the final score, which were more stable than means (data not shown). The task was undertaken on a tablet computer horizontally placed on a table (70 cm above the floor). The participant sat in a height-adjustable chair with their upper body straight, with a forearm’s distance between their eyes and the screen. To minimize the potential influence of anti-parkinsonian medications on the movement performance, the test was conducted at an “off” period, before the first drug administration of a day.
Validation and repeatability of FMAS
Since the distance between the start button and the five-stimulus button was equal (150 mm), the finger flight speed from the start button to the stimulus button could be determined by the time elapsed in the task. Although the response time of touch screen varied ranging from 55 ms to 150 ms on different devices, depending on the manufacture parameter, the finger flight time and latency were not affected by response time because the start time and the end time recorded by the computer equally included screen response time, resulting in an absolute interval time.
To verify the repeatability of the system, we conducted a series of tasks to study if repeated tests affected the participant’s performance. Twelve healthy control participants were assigned the task, with each participant duplicating the task at baseline, and 24 h apart. The performances in the tasks were recorded and compared to determine the repeatability of the system (Table 2).
Repeat measurement for finger movement (n = 12)
Data are expressed as mean±SD. MT, movement time; Ratio, Latency/MT.
Statistical analysis
Descriptive statistics were used to examine the central tendency and variability of all measured variables, and the distribution of all data was checked for normality. Student’s t-test was performed to analyze the differences between the two groups in continuous variables such as age, latency and MT. Chi-square tests were carried out to examine the gender differences between the two groups. Pearson’s correlation coefficient was applied to test all correlations between the clinical data in PD patients and healthy participants (except H-Y scale, in which Spearman correlation coefficient was used). Statistical analyses were performed using SPSS version 19.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Repeatability of FMAS
Highly consistent results of finger movement parameters obtained by the FMAS at the baseline and at 24 h apart were observed in the repeated tests. A 24 h-later repeated assessment did not affect latency, movement time and their ratio on both sides, indicating a high repeatability of FMAS (Table 2).
Age-related declines of finger movement profile in healthy participants
Age-related declines in the task performances were observed in healthy participants but not in PD patients, as shown in Fig. 3. The increase of latency and movement on both sides of the finger was correlated with age (Pearson correlation 0.315–0.462, P < 0.01). Consequently, the latency/MT ratio exhibited a negative correlation with age (Pearson Correlation –0.265 for left side and –0.283 for right side respectively, P < 0.01). In PD patients, however, the age-dependent decline trend was disrupted, only slightly positive correlation with age in latency being observed (Pearson Correlation 0.204 for left side and 0.197 for right side, P < 0.05).
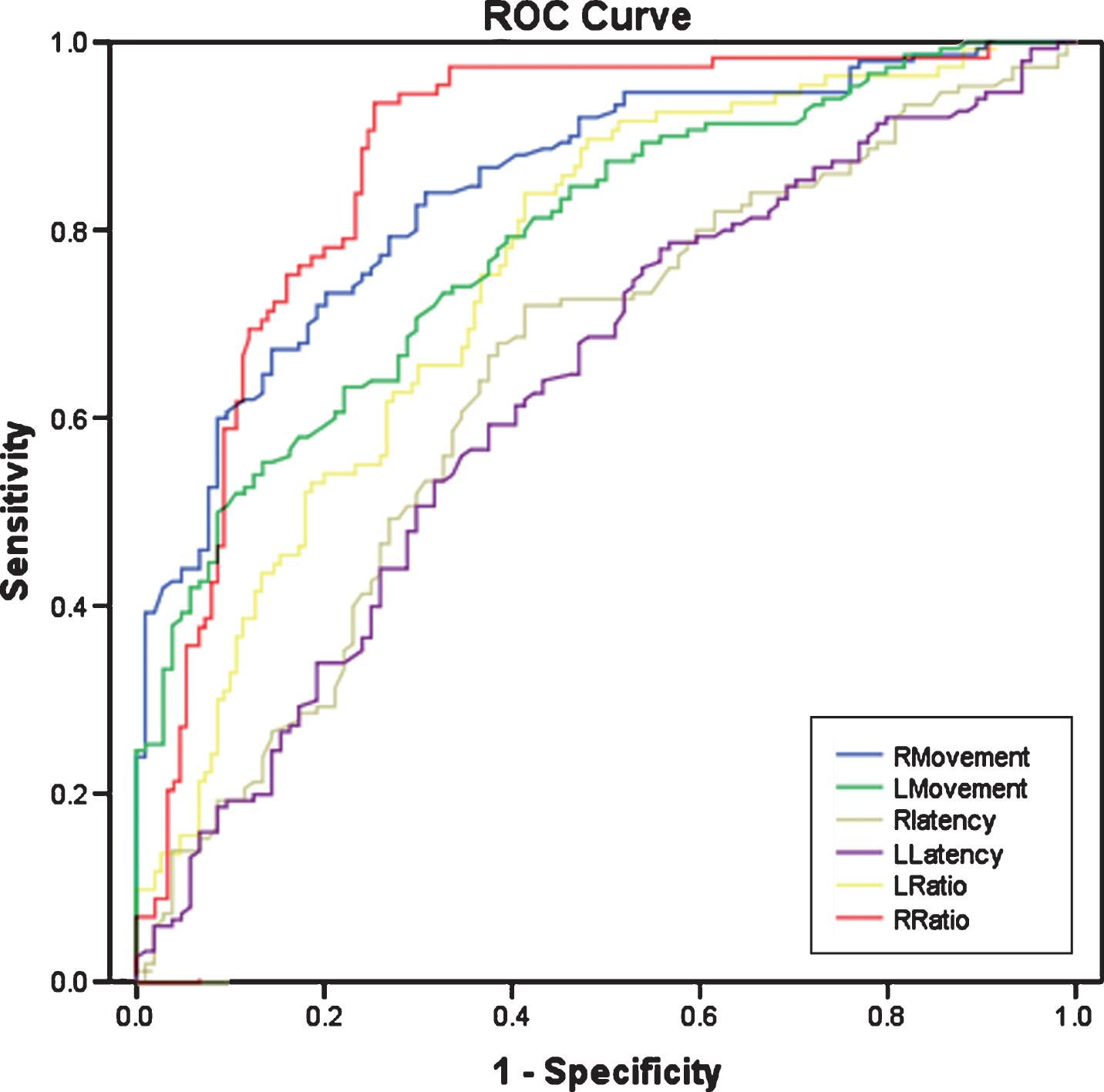
Receiver operating characteristic (ROC) analysis of finger movement parameters in the visual-motor tasks. Among latency, MT and the latency/MT ratio, the ratio (1.08) on the right side (RRatio) possessed the most powerful value to distinguish PD from normal subjects, where the area under the curve (AUC) was 0.87, followed by right MT which AUC was 0.84.
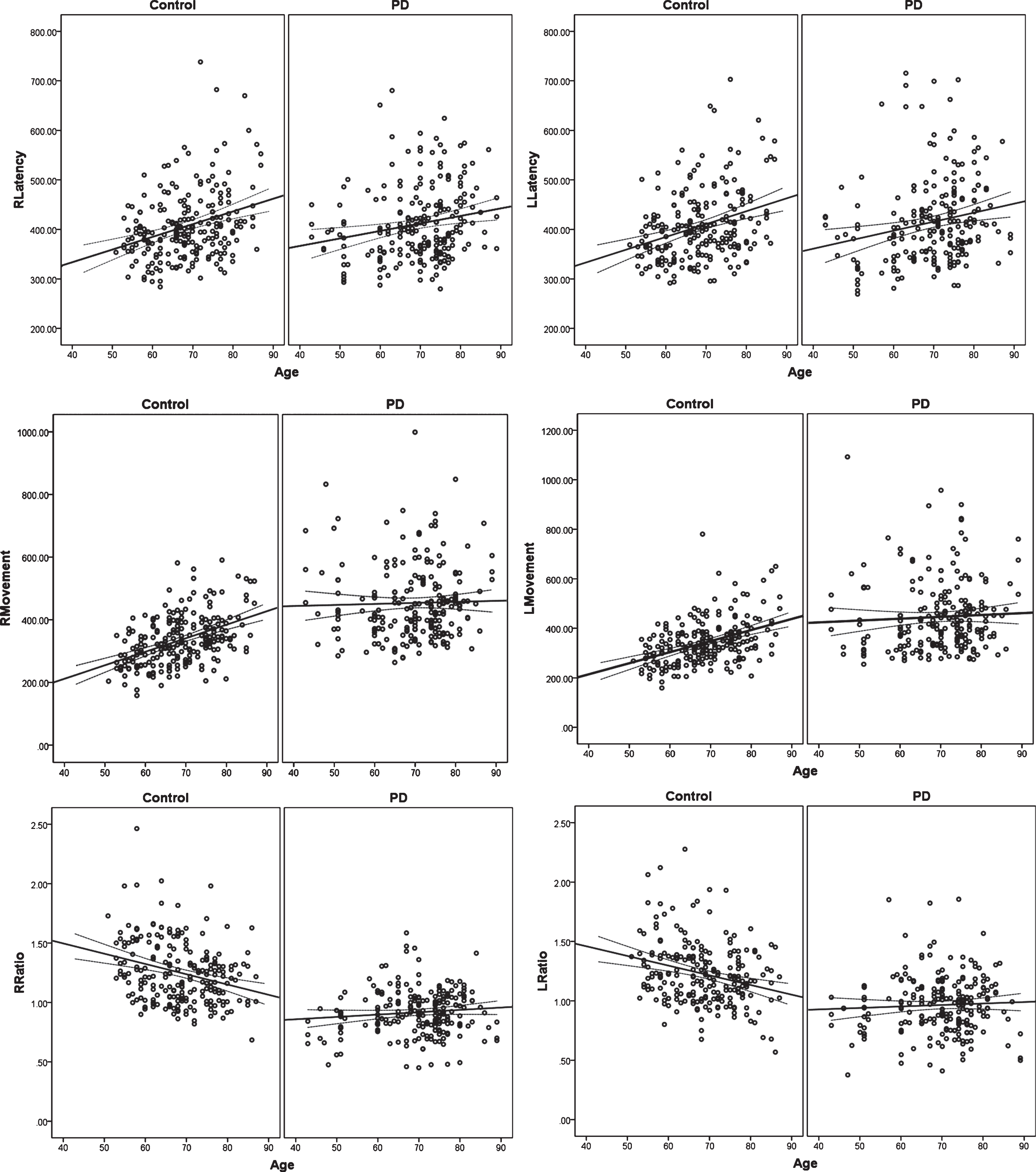
Age-related declines of finger movement performance in FMAS. PD (n = 217) and control participants (n = 221) were assessed their finger movement in the visual-motor tasks. The correlations between age and finger movement performances were analyzed. Latency, movement time and their ratio on both sides in control subjects were statistically correlated with age. However, among these parameters, only latency in PD patients showed slight correlation with age. RLatency, latency of right-side finger; LLatency, latency of left-side finger; RMovement, movement time of right-side finger; LMovement, movement time of left-side finger; RRatio, latency/movement time of right side; LRatio, latency/movement time of left side.
Different profiles of finger movement in PD patients
The characteristics of PD and control participants were shown in Table 1. Both groups were comparable for age, gender and the MMSE scores. MT but not latency on both sides in PD patients were significantly delayed as compared with the control (P < 0.000). Consequently, the latency/MT ratio remarkably decreased in PD as compared with the control (P < 0.000). Moreover, no significant difference between the right and left sides was observed for MT, latency and ratio of latency/MT in PD and normal controls (P > 0.05).
The latency/MT ratio reflected the weight of movement planning in the whole visual-motor task. The ratio in right side was 0.92 in PD patients (95% confidence interval [CI] = 0.89 to 0.94) while the ratio was 1.25 (95% CI = 1.23 to 1.30) in the control group, indicating the disproportionate delay of movement time in PD patients over normal subjects.
To assess the power of these movement parameters to differentiate PD from normal subjects, a receiver operating characteristic (ROC) was analyzed. Among latency, MT and the latency/MT ratio, the ratio on the right side (RRatio) was the most powerful parameter to distinguish PD from normal subjects. The cut-off value for RRatio was 1.08, where the area under the curve (AUC) was 0.87, followed by right MT whose corresponding AUC was 0.84 (Fig. 2).
The correlation between finger movement parameters and clinical assessment of PD
We further investigated the correlation between the finger movement parameters and clinical characteristics of PD. The results revealed that the MT, latency and the ratio were all correlated with Hoehn and Yahr scale (H-Y scale), UPDRS III score and duration of disease in PD patients (P < 0.01). The strongest correlation among them occurred between the ratio of the right side and UPDRS III score, where the r value reached 0.651 (Table 3).
Correlations between clinical characteristics and measurement parameters (*for Pearson’s correlation coefficient and #for spearman correlation coefficient) in PD patients
H-Y scale, Hoehn and Yahr scale; UPDRS, Unified Parkinson’s Disease Rating Scale; MT, movement time; Ratio, Latency/MT; r, correlation coefficient.
DISCUSSION
In this study, a touch pad-based, simple and time-saving bedside system, FMAS, was developed and applied to capture the finger movement in a visual-motor task. The merit of this system was that it could actualize the highly-repeatable joint detection of finger movement time and latency in the visual-motor task in a general touch pad in less than 3 min, collecting multiple domains of parameters related to the performance. We further assessed the performance profile of PD patients by applying the FMAS to evaluate its power in the differentiating PD patients from normal control subjects, finding that both MT and latency/MT was significantly compromised in the PD patients, and the latency/MT ratio could be served as an optimal index for potential differential diagnosis of PD.
Quantitative assessment of voluntary movement slowness is important to the diagnosis and management of PD. Finger movement is among the most widely-used fine motor ability in daily life, which is substantially compromised in PD [14]. Unfortunately, identification of bradykinesia is often challenging because there is a lack of reliable and quantitative assessment even if the wearable technology was employed, due to the low specificity and sensitivity in the detection and algorithm of movement [15, 16]. Devices such as ultrasound detector, accelerometer, high-speed video camera and muscle electrophysiology were mobilized to track or measure the certain type of movements such as finger tapping, gait and spiral drawing [17–22]. However, specific devices and equipment required in those approaches often limited their application in bedside clinical settings. Touch screen-based assessment such as smartphone and iPad were also used to detect tremor, movement and task-performance [23]. However, those methods were not task-specific, instrument-specific or only captured single-domain parameter involving voluntary movement, thus limiting their availability and application. Recently, timing information on a computer keyboard was under investigation and resulted in a highly sensitive and specific discrimination between early-PD and normal controls [24]. This report suggested that it was greatly possible to achieve highly accurate diagnostic power through identifying specific movement module. However, the study was not task-specific in daily life and the results of which might be affected by one’s typing habit (for example in those who were accustomed to typing with only one finger) and typing training, which might greatly affect the latency and flight time of the typing finger [25]. Therefore, our design focused on finger movement in the visual-motor task (similar to seeing and reaching) which might be typical in day-to-day situation [26]. Besides, it was a portable, bedside assessment tool, which could be potentially used in various settings. For example, the assessment could be undertaken in a remote touch-pad, and assessment data could be transferred back via the internet for analysis, thus improving the management of PD patients.
PD compromised multiple domains of movement include dynamics, gait, handwriting, grip force and speech, among which finger movement is the prevailing part involving daily activities [27]. Some studies reported that finger or hand movement of PD patients could be quantitatively assessed with wearable movement sensors incorporated with video camera [7], finger tapping [28] and spiral drawing analysis [29]. Given the prevailing role of finger movement in daily activity [30], we chose finger movement in a visual-motor task as the target for measurement. Our data revealed that the quantitative finger movement parameter was able to detect the age-related change of finger movement in healthy participants, and the correlation with UPDRS part III score in PD patients. In UPDRS rating, which is semi-objective classification, investigator rates item 4 and 5 in part III through the judgment of the hand movement [31] which also resembles daily life tasks [32]. As a result, the FMAS may provide a useful objective parameter in the movement assessment.
Age-related deterioration of finger movement performance among the healthy adults and elderly observed in our study was in accord with previous literature [33–39]. This trend, however, was disrupted in the PD patients, probably due to the significant slowness in finger movement. In particular, the finger MT in PD patients was markedly prolonged by at least 25% (>100 ms) over the age-matched healthy controls, indicating that the slowness of finger movement in visual-motor task was significantly compromised in PD patients. Another parameter, finger movement latency in PD group, did not proportionally change over control subjects, suggesting that the movement preparation and planning was not as markedly impaired in PD as with finger MT. It is probably because the movement preparation and planning in visual-motor task was associated with brain structures such as the parietal cortex, the premotor cortex, the medial frontal cortex, and the insular cortex [40], which was relatively spared in PD, particularly in the early stage of the disease [41].
We introduced the latency/MT ratio as an optimal parameter in FMAS firstly because it moderately improved the specificity and sensitivity in distinguishing the PD from normal control subjects. As has been shown, MT alone possessed the diagnostic power (AUC) of 0.84, while the latency/MT ratio improved the AUC up to 0.87. Secondly, considering that the MT in healthy controls but not in PD patients exhibited in an age-dependent manner, the establishing of reference values for MT and latency required a large sample size due to the clustering of PD cohort by age intervals (approximately 886 PD patients needed) [42]. We thus introduced latency/MT ratio as a joint parameter, which has the relatively higher sensitivity and specificity without the requirement for such a large sample size.
The study has some limitations. Firstly, the FMAS recorded only finger movement in a visual-motor task. Considering the diversity of PD in movement profile, finger movement assessment is a limited parameter. Secondly, a host of factors such as age, occupation, attention, cognitive function, vision, lateralization of handedness, nutrient status, physical exercise may potentially affect the performance in the visual-motor task, which remains to be precisely investigated.
Conclusion
Our study indicated that the assessment of finger movement in a visual-motor task based on a tablet-computer system may serve as a method to quantitatively measure finger movement, thus improving the assessment of hypokinesia. The portable, bedside and timesaving method provided the possibility of easy applicability and remote monitoring for PD patients, which may play an important role in PD diagnosis and management. Further large-scale studies should be conducted to test its early diagnostic value and differentiating abilities of Parkinsonism and related disorders.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interests regarding the publication of this paper.
Footnotes
ACKNOWLEDGMENTS
We thank the participants and their relatives for their contribution to this study.
This study was funded by the Shaanxi Innovative Research Team of Key Science and Technology (2012KCT-17) and Shaanxi Province Health Scientific Research Fund Projects (2018D023 and 2018D024).