
Abstract
Background:
Dyskinesia, wearing off (WO) and freezing of gait (FOG) are troublesome complications degrading quality of life in the course of Parkinson’s disease (PD).
Objective:
This study evaluated the gross chronological trend of 4 motor complications - peak dose dyskinesia (PDSK), diphasic dyskinesia (DDSK), WO and FOG in a large PD population with stratification by age at disease onset according to the PD duration.
Methods:
The motor complications of 1212 Korean PD patients were analyzed using Kaplan-Meier curves and Cox proportional hazards models.
Results:
PDSK and WO appeared first as motor complications and showed accelerated development around the 5 year-PD-duration, while DDSK showed a rather constant development over time and FOG developed around the 10 year-disease duration at an accelerated rate (p < 0.001). A younger age at PD onset predicted an earlier appearance of PDSK, DDSK and WO (p < 0.001), while an older age at onset (≥60 years) was a predictor for FOG (p = 0.014).
Conclusion:
Motor complications developed with a distinguishing inclination over the PD duration. This study provides insight into the chronological trend of motor complications in PD at a glance.
INTRODUCTION
Dopaminergic treatment in the early stage of Parkinson’s disease (PD) provides good relief of some motor symptoms for several years considered the honeymoon period. However, as Parkinson’s disease progresses, the benefit wanes with patients experiencing distressful motor complications such as peak dose dyskinesia (PDSK), diphasic dyskinesia (DDSK), wearing-off (WO) or freezing of gait (FOG), which are often difficult to treat with any drugs [1, 2]. These motor complications, especially dyskinesia and WO are associated with several clinical features such as age at PD onset, disease severity, gender and dopaminergic drug use [3–6]. Among them, age at PD onset is the most potent predictive factor for WO and dyskinesia [3]. There are few studies that have evaluated the prevalence and risk of FOG; however, a longer disease duration and severity of disease are relatively consensual risk factors of FOG, while dopaminergic drug use is partially associated with FOG [7, 8]. Based on different evaluation methods and populations, the prevalence of motor complications has been reported to vary from 30 to 80% in the incidence of dyskinesia [1, 10]. Although there are much previous epidemiological data on each motor complication, an observation of the whole trend of these motor complications all together in a same population with the disease duration will be very practical in helping to predict the prognosis of patients.
Thus, the aim of this study was to evaluate the chronological trend of the 4 most common motor complications, PDSK, DDSK, WO and FOG, in a Korean PD population simultaneously. In addition, the cumulative prevalence of each motor complication was stratified by age at PD onset which will enable clinicians to estimate the prognosis of a patient regarding motor complications at a glance during the first PD diagnosis.
METHODS
Subjects and data collection
This was a single center and retrospective review study which was done at Seoul National University Hospital (SNUH). We recruited consecutively 1,212 patients with PD and collected all the demographic and clinical information of all participants who visited the outpatient clinic from Jan 2011 to Feb 2013. They were all native Koreans. Their diagnosis of PD was done by the UK Parkinson Disease Brain Bank Criteria.
All the authors, who are movement disorder specialists, evaluated motor complications by neurological exam and history taking every visit as a routine clinical practice. Our standardized medical record for follow-up of the patients with PD included items regarding the existence and onset time of 4 motor complications. The authors evaluated the motor complications according to the following definition of terms and registered the existence and the onset of them in the medical record. The medical records were thoroughly reviewed until the study period (data collection period from Jan 2011 to Feb 2013). This study was approved by the Institutional Review Board at SNUH.
Definition of terms
This study included 4 representative motor complications including peak dose dyskinesia (PDSK), diphasic dyskinesia (DDSK), wearing-off (WO) and freezing of gait (FOG). The motor complications were based on their classic definition. PDSK is the most common type of dyskinesia with stereotypic and choreic movements involving the head, trunk, and limbs which is characterized by the sequence of parkinsonism-improvement-dyskinesia-improvement-parkinsonism. On the other hand, DDSK usually appears at the beginning and at the end of the levodopa effect [11]. WO means the re-emergence of parkinsonian symptoms towards the end of a levodopa dose [12]. FOG is a sudden, transient inability to move. It typically causes a start hesitation when initiating walking and a sudden inability to move feet when turning or walking through narrow passages [13].
Age of disease onset was defined as the year in which a cardinal sign of PD was first noted by the patient, family members, or a physician. L-dopa onset was the date a patient first started Levodopa. Levodopa equivalent daily dose (LEDD) was calculated and obtained from the last clinical follow up [14]. LEDD was divided into four groups (≤450; 450.1–750; 750.1–1012.5; 1012.5<) according to the dose formed from the quartiles of the patient number to determine the hazard ratio. The onset of motor complication was defined as the visit date in which a motor complication of any severity was noted by the patient or family members or observed by a neurologist.
The patient distribution according to the age at PD onset is shown in Supplemental Figure 1. Subgroups by the age at PD onset were divided to reflect clinically meaningful groups to determine the different prevalence of the motor complications and to provide an adequate number: ≤49; 50–59; 60–69; 70≤ [6, 15].

Kaplan-Meier curve showing that the risk of PDSK, DDSK, WO and FOG increased with the duration of PD, paired comparison of PDSK, DDSK, WO and FOG showed log rank test P < 0.001, except the comparison between DDSK and FOG P < 0.05 and the comparison between PDSK and WO showed P = 0.031. Abbreviations: PDSK, peak dose dyskinesia; DDSK, diphasic dyskinesia; WO, wearing off; FOG, freezing of gait; Censored, observation period is shorter than whole period or follow up loss.
Outcome and statistics
Time-to-event methods, including Kaplan-Meier curves and proportional hazards (Cox) models to determine the survival rate and hazard ratio of the 4 motor complications with time, were used.
Chi-square test was used to compare the prevalence of the motor complications according to several variables, and ANOVA was used for continuous variables. A p value <0.05 was considered significant. These statistical evaluations were done by the IBM SPSS statistics software, ver 19.0.
RESULTS
Of the total 1,212 patients, 46.9% were males. Mean age at onset of PD was 56.53±10.00 years, and the mean disease duration was 7.44±4.71 years. The prevalence of the 4 motor complications, PDSK, DDSK, WO and FOG, among the total 1,212 patients were 37.4%, 6.4%, 41% and 10%, respectively.
A comparison of the demographic characteristics and clinical features by the age at PD onset is listed in Table 1. The gross prevalence of PDSK, DDSK and WO was observed to be significantly higher (p < .001) at an earlier age in the onset group than at an older age in the onset group although this was not conclusive regarding FOG (p = 0.051) (Table 1).
Clinical and demographic features of 1212 Parkinson’s disease patients according to the age at onset
P value were measured by ANOVA or Pearson’s chi-square test. Abbreviations: LEDD, levodopa equivalent daily dose; PDSK, peak dose dyskinesia; DDSK, diphasic dyskinesia; WO, wearing off; FOG, Freezing of gait.
Figure 1 shows the Kaplan-Meier curve which depicts the risk of motor complications according to the disease duration. The cumulative survival of PDSK was in line with that of WO (p = 0.208). The others showed a distinguishing trend, respectively. The prevalence of PDSK and WO showed a precipitous rise around the 5-year PD-duration. FOG showed a steep increment at 10 years after PD onset whereas the prevalence of DDSK revealed a steady and slow increase over time.
The exact occurrence of PDSK was 16.5% at the 5-year, 53.1% at the 10-year and 75.2% at the 15-year PD duration. WO was 19.2% at the 5-year, 58.0% at the 10-year and 81.3% at the 15-year PD duration. FOG showed an incidence of 1.5% at the 5-year, 10.3% at the 10-year and 23.7% at the 15-year PD duration. DDSK was 2.5% at the 5-year, 9.5% at the 10-year and 18.6% at the 15-year PD duration (Fig. 1).
Patients with an earlier age at onset experienced PDSK, DDSK and WO earlier than patients with an older age at onset, even when it was adjusted for gender, final LEDD, levodopa delay time (years) and levodopa treatment duration (Fig. 2 and Table 2). Meanwhile FOG showed a reverse trend for which the older onset PD group showed a higher occurrence than that of the younger onset PD group (Fig. 2 and Table 2). Patients with an age of onset ≥60 years developed FOG more than the PD patients with an age of onset <60 years (Hazard ratio = 1.833; 95% CI = 1.128–2.977; p = 0.014).
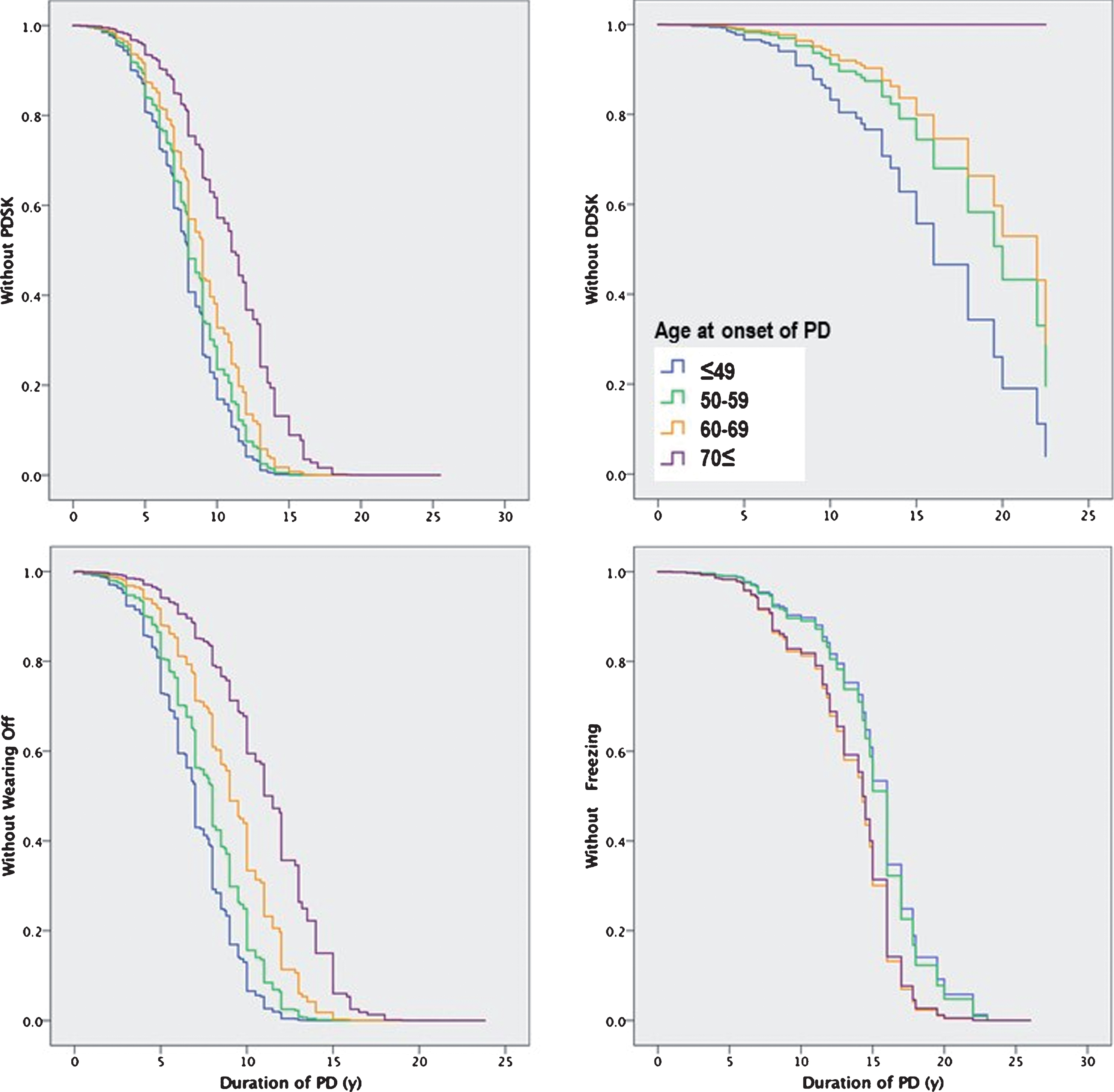
Survival curve by cox regression analysis showing the effect of age at onset of PD on the occurrence of PDSK, DDSK, WO and FOG. Patients with younger age at onset experienced PDSK, DDSK, WO earlier than older patients adjusted by Gender, LEDD, levodopa delay (years), and L-dopa treatment duration. (log-rank P < 0.001) However the FOG showed that older age at onset was associated with earlier FOG development in reverse.
Risk parameters by Cox proportional hazards model regarding the development of motor complications
CI, confidence Interval, other abbreviations are same as Table 1.
DISCUSSION
This study showed that the 4 motor complications have a distinguishing chronological inclination during the course of PD. The age at onset of PD is a strong predictor for the onset of these motor complications, but it affected freezing of gait and the other motor complications oppositely.
It is well known that disease duration is an important risk factor in developing motor complications [3–6]. Nevertheless, there is no previous report comparing the development of various major motor complications, which included special types of dyskinesias, using the survival time trend in one population. This study showed the occurrence of the 4 representative motor complications with a contextual order with the disease duration. This will help predict the motor complications of patients in a clinic according to the disease duration or age at onset. The prevalence of motor complications has been reported with varying ranges due to the different evaluation methods [1, 10]. In addition, there was limited evidences on the epidemiological data regarding some motor complications (DDSK and FOG). Therefore, this all-inclusive and refined evaluation of 4 motor complications in the same population will be informative for clinicians and patients.
In this study, the occurrence of WO showed a very similar trend with PDSK according to the disease duration, that was an earlier accelerated occurrence around the 5-year PD-duration while DDSK did not. This result could suggest that PDSK may share a mechanism with WO but not with DDSK. The WO phenomenon reflects the decrement of the dopamine storage capacity by the loss of the dopaminergic nerve terminal resulting in fluctuations of the plasma levodopa concentration which may reflect the disease severity related to the disease duration [16]. At this time, LEDD is increased usually to overcome WO. Therefore, this conventional dose strategy provides an intermittent delivery of levodopa to the nigrostriatal system resulting in a pulsatile stimulation of the striatal postsynaptic receptor and increasing the levodopa stimulation may provoke peak dose dyskinesia proceeding after the WO [12]. This post synaptic pulsatile stimulation and change in the downstream cascade in genes and proteins were suggested to be the mechanism of dyskinesia [12, 17]. However, distinguishing the epidemiologic prevalence of PDSK and DDSK may suggest different pathophysiological and genetic implications regarding genetic susceptibility [16].
Previous evidence delineated the effect of the age at onset on the clinical features of PD showing that a younger age at onset increased the risk of dyskinesia [6, 18]. The interest in most previous studies was confined to PDSK. Meanwhile, our study showed the features of four motor complications including DDSK according to the age at onset. This study showed that a younger age at onset was associated with an earlier occurrence of DDSK as well as PDSK and WO. Compared to an age at onset ≤49 years, the prevalence of DDSK in patients with an age at onset over 50 years decreased steeply (Table 2). Although there is a relative lack of studies on DDSK, it is postulated that a different mechanism such as genetic susceptibility may be involved with the development of DDSK more so than in other motor complications.
FOG showed a distinguishing trend compared with the other motor complications in the survival model. It developed at a later time during the PD course, and an older age at PD onset increased the risk of FOG in contrast to the other 3 motor complications in this study. FOG has been reported to often show a poor response to dopaminergic medication or sometimes refractory to any kind of medication [19]. It is assumed that the mechanism of FOG is different from the other motor complications, that is, other anatomical areas such as the cortical basal ganglia connection or pedunculopontine nucleus rather than the nigrostriatal pathway itself and emotional problems or an impaired cognitive resource rather than genetic factors may be involved [2, 20–24].
Female gender was a constant risk factor for PDSK, DDSK and WO except for FOG. Low body weight has been suggested as a cause for the female predominance related to levodopa fluctuation [1]. FOG is commonly unrelated or refractory to dopaminergic medication which reflects why FOG is not related to the female gender.
This study did not use the duration of levodopa use but disease duration as a time factor to show the occurrence of 4 motor complications, this study intended to show whole trend of 4 motor complications over disease duration. Thereby the prevalence of 4 motor complications seems like lower prevalence than previous reports using duration of levodopa use. This study was conducted in a tertiary referral hospital and thereby the age at PD onset is younger than the usual PD population. In addition, even though the onset of motor complications was carefully observed, the interval between the clinical follow-ups was rather long usually 3 to 4 months, and the follow-up interval was not the same for all participants. Because the onset of a motor complication was assumed as the time it was observed or noticed by a patient in the outpatient clinic, recall bias could be included as a limitation. In addition, unrecognized motor complications by clinicians or caregivers could be reported at a later time rather than at the exact onset. However, this study included a large PD population to overcome this limitation. Because SNUH is one of the largest hospitals in Korea as well as a tertiary referral center, it is possible that patients with disabling motor complications tend to visit this center more often. It could exaggerate the incidence of motor complications in this study group compared to the general PD population; however, the temporal trend in the occurrence of motor complications is less affected by this time related statistical evaluation. Nevertheless, this study only included Korean patients and presents the first epidemiologic data that include a Korean population only with a longitudinal evaluation.
This study presents a chronological view of the 4 big motor complications. The results of this study could serve as valuable clinical information to monitor the disabling motor symptoms of PD patients.
CONFLICTS OF INTEREST
The authors have no conflict of interest to report.