
Abstract
The authors report of a patient with Parkinson’s disease in whom imaging revealed a complete agenesis of the corpus callosum. Although this co-occurrence is probably coincidental, this finding suggests that the bilateral degenerative changes in Parkinson’s disease may occur independent of the interhemispheric connections.
INTRODUCTION
While imaging of the brain may support or exclude the diagnosis of Parkinson’s disease (PD), the diagnosis of PD rests on expert clinical examination [1]. Here we present a patient diagnosed with PD in whom MR imaging revealed a complete agenesis of the corpus callosum.
HISTORY
This 60-year-old ambidexter patient with an otherwise normal medical and developmental history presented with a progressive rest tremor in the right hand. Clinical examination showed normal cranial nerve function, normal sensibility, coordination, and tendon reflexes. Motor examination indicated a rest tremor in the right arm with a frequency of about 4–6 Hz, suppressed by initiation of movement. Upon levodopa challenge test patient scored 38 on the motor evaluation of the Unified Parkinson Disease Rating Scale Part III (UPDRS-III) in “off” stage and 19 in the “on” stage. Patient remained stable in Hoehn and Yahr stage 2 since the diagnosis (>7 years). The clinical diagnosis of PD was confirmed by three neurologists in three different expert centers. An MRI scan revealed a complete agenesis of the corpus callous with no other gross structural abnormalities (Fig. 1) A presynaptic dopamine transporter single photon emission computerized tomography (DAT SPECT with 123I-FP-CIT) showed decreased values of dopamine transporter activity in the bilateral striatum with most impact on both putamina.
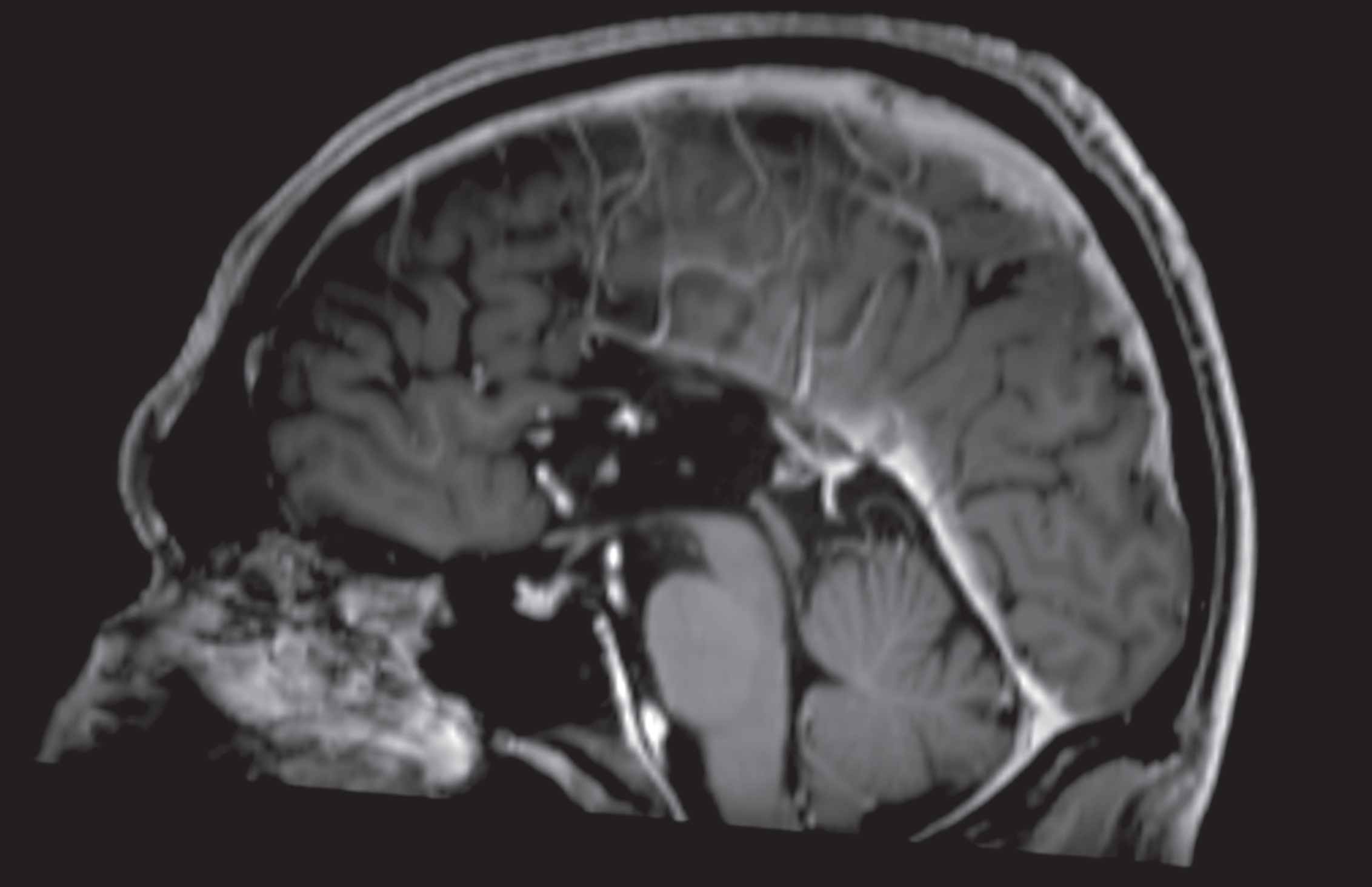
Structural T1-weighted, gadolinium enhanced MRI of the patient’s brain, midsaggital slice. Note the complete absence of the corpus callosum.
DISCUSSION
Two centuries after James Parkinson’s essay on the Shaking Palsy (1817), the diagnosis of PD is still based on clinical signs and symptoms. To our knowledge, there have been no previous reports of PD patients with a complete agenesis of the corpus callosum (AgCC), nor have there been descriptions of AgCC patients with parkinsonian symptomatology (or “parkinsonism”). Whereas the prevalence of PD increases with age up to 4% in individuals over 60 years [2], the prevalence of AgCC is a factor 200 less and estimated between 0.018–0.025 in live births [3, 4]. The prevalence of AgCC in asymptomatic individuals is not known.
AgCC stems from a failure to develop the large bundle of fibers that connect the cerebral hemispheres and probably results from a disruption in the early callosal developmental stage. Genetic causes have been identified, but environmental factors such as fetal alcohol syndrome are also associated. The neuroanatomy and fiber tracts of individuals with AgCC was thoroughly described by Probst in 1901, rendering his name to the so called “Probst bundles”, association fibers that instead of passing contralateral grow caudally along the medial surface of the ipsilateral cerebral hemisphere [5]. Individuals with AgCC present with a large variability in cognitive and behavioral symptomatology [3]. Subtle deficits in bimanual motor coordination have been reported in AgCC patients [6], but rest tremor or other parkinsonian motor symptoms have not yet described in the literature. Based on the prevalence of PD and AgCC, and the possible causes of both entities, we currently consider AgCC and PD to be unrelated and its co-occurrence as coincidental. The absence of the corpus callosum in this PD patient suggests that the bilateral neurodegenerative changes in PD are independent of the corpus callosum.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.