
Abstract
Background:
Domperidone is a proposed treatment of orthostatic hypotension (OH) in Parkinson’s disease (PD). However, domperidone use in PD is tempered by concerns regarding QT prolongation and ventricular tachyarrhythmia and sudden cardiac death (VT/SCD).
Objective:
The aim is to identify peer-reviewed studies in which either (1) the effect of domperidone on blood pressure in patients with PD, or (2) the adverse effects associated with domperidone use in PD patients has been reported.
Methods:
PubMed, EMBASE, Medline and Scopus were searched using the terms Parkinson’s disease and domperidone.
Results:
Twenty-two articles fulfilled the inclusion criteria. One study was a randomized placebo-controlled trial with domperidone administration independent of the commencement of dopaminergic medications. This study identified a non-statistically significant trend that domperidone may be beneficial for OH in PD. Several studies identified statistically significant differences in BP with domperidone in the setting of initiating dopaminergic medication. There is currently the most evidence to support domperidone use with apomorphine commencement. Studies reporting domperidone adverse effects in PD patients were largely retrospective or cross-sectional. The identified studies demonstrated that domperidone may cause QT prolongation and is associated with increased risk of VT/SCD in PD patients with preexisting cardiac disease.
Conclusions:
Domperidone may help to ameliorate OH associated with dopaminergic medications in PD, namely when used in conjunction with apomorphine. When considering whether to use domperidone in PD, factors that should be taken into account include pre-existing heart disease and drug interactions, as well as the impact of OH on mobility, cognition and quality of life.
INTRODUCTION
Parkinson’s disease (PD) is a neurodegenerative condition that involves both motor and non-motor symptoms. One of the non-motor manifestations of PD is autonomic dysfunction, which may include orthostatic hypotension (OH). OH has been estimated to be present in approximately 30% of PD patients, of whom up to 33% may be symptomatic [1, 2]. OH in PD patients may contribute to an already elevated risk of falls, which result in poor patient outcomes [3]. Hypotension is a particular problem when commencing new dopaminergic medications [4]. OH has been described as a predictor of dementia in PD [5]. Although this may be because it marks a disease subtype, there have been recent suggestions that it can directly cause cognitive impairment, presumably via reduced perfusion of the central nervous system [6]. Further to this, patients presenting with idiopathic neurogenic OH (pure autonomic failure) have a high risk of phenoconverting to dementia with Lewy bodies [7].
There are several treatment avenues for OH in PD including both non-pharmacological and pharmacological measures. Non-pharmacological strategies include increasing dietary salt intake, maintaining adequate hydration, compression stockings, standing slowly and avoiding hot weather. These measures may be beneficial; however, the majority of patients also require pharmacological management [8, 9]. Pharmacological treatment strategies include mineralocorticoids (such as fludrocortisone), midodrine, pyridostigmine and droxidopa [10, 11]. However, even with a combination of these strategies PD patients may have refractory orthostatic symptoms.
One of the proposed treatments for OH is the peripheral dopamine-2 receptor inhibitor domperidone [12]. Domperidone acts on peripheral dopamine receptors; since it does not cross the blood-brain barrier it can be given in PD without worsening motor symptoms. It is also often used as an anti-emetic and has also been investigated as a prokinetic agent. Given that peripheral stimulation of dopamine-2 receptors results in vasodilation (as may occur with some PD medications), it has been hypothesized that domperidone may aid in treating orthostatic hypotension in patients with PD [13, 14].
However, concerns have been raised regarding the use of domperidone for this indication because it may prolong the QT interval and has accordingly been associated with ventricular tachyarrhythmia and sudden cardiac death (VT/SCD) [15]. There are many medications that may cause QT prolongation including antidepressants, antipsychotics and antiemetics [16]. Accordingly, there is debate regarding the use of domperidone for orthostatic hypotension in PD, particularly in regards to its effect on a patient’s risk of sudden cardiac death.
The aim of this paper is to identify peer-reviewed studies in which: the effect of domperidone on blood pressure was assessed in patients with PD, or the adverse effects associated with domperidone use in PD patients were reported.
MATERIALS AND METHODS
This review was conducted in accordance with the PRISMA-P guidelines [17]. The databases PubMed, Medline, EMBASE and Scopus were searched on 19 February 2017. The searches used the Medical Subject Headings domperidone and Parkinson’s disease. Search results were limited to those papers published in English.
Titles and abstracts of these publications were then viewed to determine if the papers met the inclusion criteria. To be included in this project a study must: (1) be a primary clinical (involving human patients) research publication (not including published abstracts); (2) involve patients with PD given domperidone, (3) be available in full-text and either (4a) report the effect of domperidone on blood pressure in patients with PD (either with or without concomitant medications) as measured objectively by a BP assessment (subjective scores were not considered to fulfill this criteria), or (4b) report the frequency or nature of adverse effects occurring due to domperidone use in patients with PD (which could not be ascribed to the concurrent commencement of another medication). Therefore, studies in which domperidone was commenced concurrently with another medication and adverse effects were reported, were not included for assessment of side effects (since the observed adverse effects may be due to the second medication). In addition, studies presenting information solely on the efficacy of domperidone for nausea/vomiting and gastric motility disorders in the absence of PD were considered as beyond the scope of this review.
Articles that appeared likely to fit inclusion criteria based on title and/or abstract were viewed in full-text. In cases where it could not be determined if an article met the inclusion criteria the articles were also viewed in full-text. Reference lists of included articles were then searched for further studies that may be included in the project. Eligibility determination and data extraction were performed independently in duplicate by SB and IC using a standardized form. PK was involved in the location of, and data extraction from, full-text articles. Inconsistencies were resolved with PK. Risk of bias was assessed in trial-based papers using adapted criteria from the Cochrane Collaboration’s tool for assessing risk of bias. In observational studies risk of bias was assessed using questions adapted from the Newcastle-Ottawa Quality Assessment Scale.
RESULTS
The initial search of the four databases yielded a total of 1,935 publications. Removal of non-English publications left 1,503 publications. The titles and abstracts of these papers were reviewed. 193 articles were subsequently retrieved in full-text. It was then determined that 22 articles fulfilled the inclusion criteria (see Fig. 1).
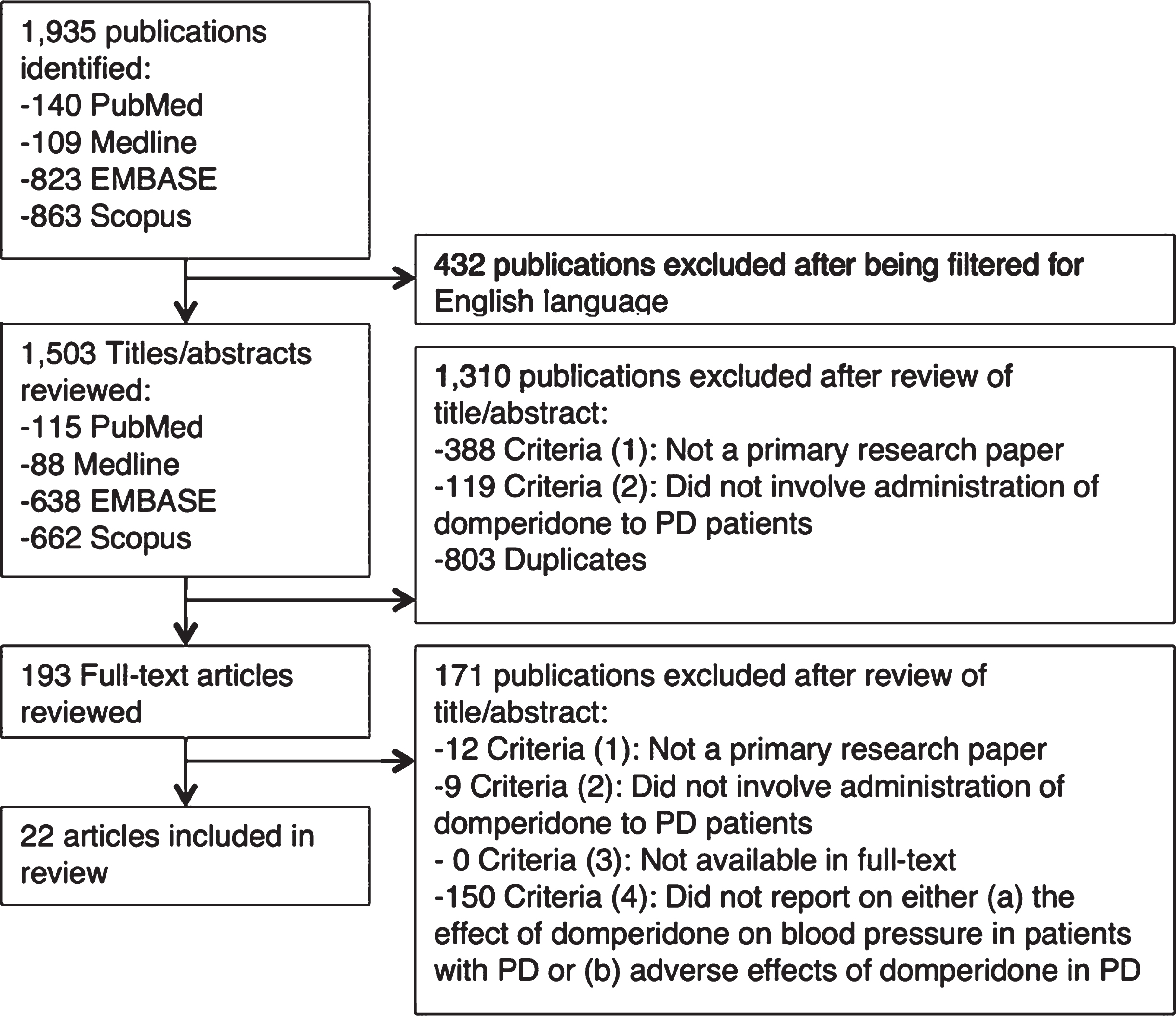
Flowchart detailing results from the search strategy and application of inclusion and exclusion criteria for a review of articles reporting on the efficacy of domperidone for postural hypotension in PD and adverse effects of domperidone in PD patients.
The 22 articles that fulfilled the inclusion criteria included 13 studies that assessed the effect of domperidone on BP in PD and 9 reporting on the adverse effects of domperidone in PD (see below). The most commonly reported dosing regimens were 10 mg TID, 20 mg TID and 50 mg TID.
The main limitations of the studies assessing the effect of domperidone on blood pressure were that the effect on blood pressure was typically only assessed in the setting of a newly commenced dopaminergic agent, commonly in an apparently open-label fashion and often with small sample size (see Table 1). Several studies assessing adverse outcomes had large sample sizes. These studies were predominantly retrospective or cross-sectional in nature (see Table 2). Most studies did not provide a description of how cases of PD were defined (for example, specific diagnostic criteria or assessment by movement disorders specialist). This lack of diagnostic criteria raises the possibility that other diagnoses, particularly multiple system atrophy, may have been included in study groups.
Studies reporting effect of domperidone on blood pressure in patients with Parkinson’s Disease
UK PDS BBC, United Kingdom Parkinson’s Disease Society Brain Bank criteria.
Studies that reported on adverse effects of domperidone in patients with Parkinson’s disease
UK PDS BBC, United Kingdom Parkinson’s Disease Society Brain Bank criteria.
The data presented in Corsini et al. (1980) was considered likely to represent the same data as Corsini et al. (1979) and therefore will not have its results presented separately [18, 19]. The same was considered to be the case for Quinn et al. (1981a) and Quinn et al. (1981b) [20, 21].
Domperidone effect on blood pressure in PD
14 studies reported on blood pressure changes attributable to domperidone (see Table 1). Most studies were in the setting of the initiation of a dopaminergic agent, either with domperidone or with placebo. Dopaminergic medications that were administered with domperidone included apomorphine, bromocriptine, levodopa and CQA 206-291. Only one study was located that specifically examined the efficacy of domperidone for the treatment of OH independent of the initiation of dopaminergic medication [22].
Schoffer et al. (2007) utilized a double-blind RCT crossover methodology to trial both domperidone and fludrocortisone for the treatment of orthostatic hypotension in PD [22]. This study also had a phase during which non-pharmacological measures were assessed. However, blinding of the non-pharmacological stage of the trial was not performed (for feasibility reasons). 17 PD patients were randomized (via a computer-generated number) to determine which pharmacological treatment they would receive first. Unfortunately, four patients withdrew during the study (three from the initial domperidone group and one from the fludrocortisone group) and further analysis was conducted as per protocol. The results indicated that with domperidone, 10 mg TID, there was a trend to decreased drop in BP on tilt table with domperidone use. Some effect was also seen for fludrocortisone, but there was a trend for better effectiveness of domperidone than fludrocortisone. While not an objective assessment of BP, there was statistically significant improvement on the questionnaire relating to orthostatic hypotension (COMPASS-OD) and general clinical impression (CGI) of OH severity with domperidone use (p = 0.04).
Three studies assessed the effect of domperidone in the setting of bromocriptine use [20, 24]. In two out of three studies, domperidone appeared to have no effect, or even a negative effect, on rates of hypotension with bromocriptine administration [20, 23]. Agid et al. (1979) found that 4/8 patients who received domperidone had orthostatic hypotension compared to 0/9 who received placebo [23]. Quinn et al. (1981) found rates of orthostatic hypotension to be similar between the domperidone and placebo arms of their trial (n = 20) [20]. However, Montastruc et al. (1985) identified that domperidone, when given with bromocriptine, resulted in a higher blood pressure in already hypertensive PD patients (n = 5) [24].
Conversely, the five studies that assessed the effect of domperidone on BP when given with apomorphine found that the medication consistently resulted in better avoidance of hypotension [18, 25–28]. For example, Merello et al. (1992) found that when domperidone was provided at the time of apomorphine use, there was no drop in BP, but without domperidone there was a significant drop in systolic and diastolic BP (p = 0.05 and p = 0.004, respectively) (n = 18) [25]. Similarly Corsini et al. (1979) found that when given domperidone with apomorphine 0/4 PD patients had orthostatic hypotension, but when given the saline control 2 out of 4 experienced orthostatic hypotension (n = 4) [18]. Arnold et al. (1997) found that patients treated with domperidone had a significantly smaller decrease in BP than those treated with ondansetron (p = 0.0072) (n = 16) [26]. Sigurdardottir et al. found that domperidone increased both supine and lying blood pressure and heart rates in PD patients commenced on apomorphine (n = 10) [27]. Pollak et al. found a similar result with domperidone again attenuating the hypotensive effect of apomorphine on standing BP in PD patients (n = 16) [28].
Other drugs which have been studied in conjunction with domperidone included levodopa and CQA 206-291 [29, 30]. In the levodopa study pretreatment with domperidone did not alter rates of dizziness or hypotension [29]. With CQA 206-291 two out of six patients experienced hypotension, which then resolved with domperidone [30].
Domperidone adverse effects in PD
The majority of the studies that reported on adverse effects of domperidone use in patients with PD were focused upon potential cardiovascular abnormalities [31–34]. Some studies assessed rates of neurological adverse effects and several reported on non-specific adverse effects (see Table 2).
By far the largest of the four studies that reported on cardiovascular adverse effects was a retrospective case-control study including 214,962 individuals with PD. This study by Renoux et al. (2016) determined that the incidence of sudden cardiac death or ventricular tachyarrhythmia in the entire PD population was 3.28 per 1,000 person-years [31]. Current use of domperidone showed a trend towards increased risk of sudden cardiac death or ventricular tachyarrhythmia (22%) but was not statistically significant (RR 1.22, 95% CI 0.99–1.5). Theoretically, an increased relative risk of 22% on an incidence of 3.28 per 1,000 person years would provide an incidence of VT/SCD of 4 events per 1,000 person-years. This would equate to an absolute risk increase of 0.72 per 1,000 person-years with domperidone use, or a number-needed to harm of 1,395. There was a statistically significant increased risk of VT/SCD associated with domperidone use in the PD group with preexisting heart disease (RR 1.38, 95% CI 1.07–1.78). In those without pre-existing heart disease, the relative risk was RR 1.21; 95% CI 0.81–1.81, a non-statistically-significant change. No relationship between duration of domperidone use or dose and the risk of VT/SCD was identified [31]. There was no clear dose relationship seen, with a trend towards a higher risk for patients on≤30 mg daily (RR 1.3, 95% CI 0.99–1.71) than for those patients on a dose of >30 mg daily (RR 1.17, 95% CI 0.87–1.59).
Heranval et al. (2016) also conducted a retrospective study, including 501 patients with PD, 126 of whom used domperidone [33]. Out of the patient records assessed only one patient had an adverse cardiac event while on domperidone. This was an episode of atrial flutter and a cause-effect relationship with domperidone was unable to be established. However, this study did not provide an assessment of the duration of domperidone therapy. The patient who had the event was on 30 mg domperidone daily.
Cunnington et al. (2013) conducted a cross-sectional medication and ECG review including 192 PD patients of whom 112 had ECG [32]. In this cross-sectional analysis, they found that 9/24 PD patients on domperidone had normal QTc, 11/24 had prolonged QTc (defined as 450–500 ms for men and 460–500 ms for women) and 4/24 had significantly prolonged QTc (>500 ms). Those with normal QTc had a slightly lower mean domperidone dose than those with prolonged QTc (normal QTc - mean 47 mg, range 30–60 mg, compared to prolonged QTc - mean 49 mg, range 30–60 mg). It is unclear if ECGs were assessed blindly. Accordingly, there is the possibility of bias in that the outcome assessors’ expectations regarding patients on medications that are known to prolong the QT interval may have influenced the interpretation of the ECGs.
Quinn et al. (1985) was the only prospective study that reported on cardiac outcomes. However, with a sample size of 3, the findings that with domperidone PD patients had lower rates of aberrant beats and ventricular ectopics is difficult to generalize [34].
Van Dalem et al. (2016) used a retrospective case-control methodology (n = 5,114) to assess the association between domperidone use and all cause mortality in PD patients [35]. Due to the brief nature of the report details regarding aspects of the analysis, including control of confounders and sample size of PD patients taking domperidone, conclusions that may be drawn are limited. However, when comparing PD patients with PD patients on domperidone the study indicates that the use of domperidone is associated with increased risk of mortality (HR = 2, 95% CI 1.64–2.45). It was reported that the mortality risk was highest in the group with a 15–30 mg dose (average daily dose) (HR = 2.16, 95% CI 1.55–3.01). However, such analysis is difficult to interpret due to possible confounders beyond the use of domperidone itself. For example, OH has been strongly linked to a ‘diffuse-malignant’ subtype of PD, which may have higher mortality [35, 36].
One novel potential adverse effect that may be associated with domperidone use in PD is that of restless legs syndrome (RLS) [37]. In a sample of 184 PD patients Rios-Romenets et al. (2013) found a statistically significant relationship between domperidone use and RLS. In the domperidone group 13/27 (48%) had RSL compared to 33/157 (21%) in the non-domperidone group (p = 0.010) [37]. The mechanism of this effect was unclear, and confounding by indication cannot be ruled out. Other adverse effects that were reported with domperidone in PD patients included nipple tenderness, hyperprolactinemia, weight loss, tiredness and loss of appetite [38–40].
DISCUSSION
OH is a common manifestation of autonomic dysfunction in PD and may be exacerbated by dopaminergic medications used to treat PD motor symptoms. In this paper we have reviewed the evidence supporting the use of domperidone for the management of blood pressure and studies assessing its possible adverse effects. Only one RCT has been conducted assessing the efficacy of domperidone for treating OH independent of the concurrent commencement of dopaminergic medications. This study had methodological issues with multiple patients beginning on domperidone withdrawing from the study contributing to a small sample size. The study did identify that domperidone provided a trend to improvement in management of BP, with a trend to having a greater effect on BP than fludrocortisone; however, neither of these observations reached statistical significance. Studies assessing the effect of domperidone on BP in the setting of the initiation of a dopaminergic medication have found mixed results. There is currently the most evidence to support concurrent domperidone use with apomorphine to prevent hypotension, with several studies identifying statistically significant results which indicate that domperidone helped to blunt BP changes [25, 26].
Large retrospective and cross-sectional studies have provided evidence to support the assertion that domperidone may contribute to QT prolongation and predispose to VT/SCD in some PD patient populations. However, the largest of these studies, despite a sample size of over 200,000 persons, found a trend, but no statistically significantly increased risk in PD patients without preexisting heart disease. The baseline absolute rate of VT/SCD in the PD population was relatively low (3.28 per 1,000 person-years) [31]. No consistent relationship between dose of domperidone and risk of these adverse effects was reported.
It should be noted that there are other medications used in PD that may prolong the QT interval in addition to domperidone. In the study conducted by Cunnington et al. (2013) other medications that PD patients were using that may prolong the QT interval included antidepressants (citalopram, amitriptyline and mirtazapine), antipsychotics (quetiapine and olanzapine), hydroxychloroquine and quinine [32]. The concurrent use of multiple medications that prolong the QT interval increases the risk of VT/SCD [41]. Therefore, any cardiac risk associated with domperidone may be minimized through the avoidance of concurrent prescription of other medications that may prolong the QT interval. It should also be noted that domperidone is metabolized through the CYP3A4 pathway and concurrent use of CYP3A4 inhibitors (such as erythromycin or ketoconazole – which may also cause QT prolongation themselves) may result in increased plasma levels of domperidone [42]. There are numerous drugs that influence the CYP450 system, including CYP3A4, which have been summarized previously [43]. Overall, given these findings, and the often-disabling nature of OH in PD, it is unclear whether QT interval concerns should preclude a trial of domperidone in the absence of pre-existing heart disease and absence of medications that are likely to interact with domperidone.
Domperidone is available in most countries. However, in some locations, the availability of domperidone may limit its use. Since 2004 domperidone has not been available in the USA, although it may be used for gastrointestinal disorders under an Investigational New Drug (IND) application [44]. In 2014 the European Medicines Agency’s (EMA) Pharmacovigilence Risk Assessment Committee (PRAC) made the recommendation that domperidone prescribing be limited to a course of 10 mg TID for usually less than one week for the management of nausea and vomiting [45, 46]. The Co-ordination Group for Mutual Recognition and Decentralised Procedures – Human (CMDh) confirmed this recommendation [47]. In the 2014 EMA Assessment Report it was recommended that relevant Market Authorisation Holders submit a Risk Management Plan regarding, among other uses, the off-label use of domperidone for OH in PD patients [46]. There are currently two Post-Authorisation Safety Studies (PASS) planned regarding domperidone, including a retrospective observational cohort study assessing methods of domperidone prescribing [48, 49]. In 2012 Health Canada released an alert regarding the risk of VT/SCD associated with domperidone use at doses >30 mg per day and in individuals >60 years of age [50]. In 2015 Health Canada released a statement, which signaled the commencement of a study in collaboration with the Drug Safety and Effectiveness Network, specifically assessing risk of VT/SCD in PD (Renoux et al., see above) [31, 51].
Some limitations of this review should be noted. One limitation of this review is the exclusion of non-English language publications. Publication bias or studies selectively reporting outcomes may have also influenced the results of this review. Another possible limitation is that non-adherence to treatment with domperidone may have altered study results. In a study conducted by Ng et al. (2007) it was identified that in a cohort of PD patients (n = 71) the highest rates of medication change non-completion occurred with domperidone (52%) [52]. In 86% (12/14) no reason was provided for this domperidone change non-completion. Ng et al. hypothesize that this non-completion may be due to patient reluctance to take further medications that they consider not to be essential to their PD treatment regimen [52]. Another possible reason for discontinuation of domperidone may be that the side effects of dopaminergic medications can lessen with time, and accordingly with time domperidone may no longer be required to control these side effects.
Note that this review has focused on the adverse effects associated with domperidone use specifically in PD patients. A recent meta-analysis was conducted assessing rates of ventricular arrhythmia and sudden cardiac death with domperidone use across a variety of patient populations [53]. This study concluded that larger observational studies or RCTs are required but that from the available evidence it appears that current domperidone use is associated with a 70% increased relative risk of arrhythmia or sudden cardiac death. Although one cannot be definitive, it appears that the relative risk of VT/SCD associated with domperidone use may be lower in PD than in the general population. It is unclear why this may be the case. Preclinical studies indicate that the mechanism by which domperidone may be associated with QT prolongation is through its interactions with cardiac potassium currents via blockade of channels derived from the human-ether-a-go-go related gene (HERG) [54].
Future research in this area is needed. In particular, further randomized controlled trials to test domperidone for the reduction of OH without recent dopaminergic medication changes would be important. Such studies should have larger sample sizes than have been conducted previously, and should directly measure effects on QT interval prospectively with ECG. Other studies aiming to further characterise the safety of domperidone in PD patients without preexisting cardiovascular disease may be beneficial.
Conclusion
Domperidone may help to ameliorate OH associated with dopaminergic medications in PD, namely when used in conjunction with apomorphine. However, RCTs with larger sample sizes are required to further elucidate this effect and domperidone may not alleviate hypotension caused by certain dopaminergic agents. There is preliminary evidence to support the observation that domperidone may lead to QT prolongation in PD patients and that its use is associated with an increased rate of VT/SCD in PD patients with preexisting heart disease. However, in PD patients without preexisting heart disease confidence intervals of all estimates in the largest identified study cross zero. There is no consistent relationship reported between domperidone dose and these adverse effects. When considering whether to use domperidone in PD, factors that should be taken into account include pre-existing heart disease and drug interactions, as well as the impact of OH on mobility, cognition and quality of life.
FINANCIAL DISCLOSURES
A/Prof Ron Postuma received personal compensation for travel, speaker fees, and consultation from Biotie, Biogen, Boehringer-Ingelheim, Roche, and Teva Neurosciences, and is funded by grants from the Fonds de Recherche du Québec - Santé, the Michael J. Fox Foundation, the W. Garfield Weston Foundation, and the Canadian Institutes of Health Research. The other authors have nothing to disclose.
Footnotes
ACKNOWLEDGMENTS
This research did not receive any specific funding.