
Abstract
Keywords
INTRODUCTION
Evaluation of circadian patterns of nonmotor symptom (NMS) fluctuations in advanced Parkinson’s disease (PD) using a NMS diary similar to the PD motor symptom diary [1, 2] revealed similar occurrence patterns of motor and NMS Off state periods (defined as NMS rated as present) over the day for most psychiatric NMS (anxiety, depression, inner restlessness) with morning, early afternoon and early evening Off periods [3]. The other NMS including fatigue showed relatively stable frequencies over the day. In contrast, switches between NMS On (time periods with NMS rated as absent) and NMS Off time periods (NMS present) occurred largely independent of switches between motor On and Off periods with concordance rates of only 26–43% of all switches for psychiatric and 7–17% for autonomic NMS. These data implicate similar circadian fluctuations patterns of most psychiatric NMS compared to those of motor fluctuations, but without close timing and/or different kinetics of NMS and motor fluctuations. To dissect timing and kinetics of NMS fluctuations, we here synchronized motor Off periods from diary data by summation of all motor Off state hours using the first hour of each particular motor Off period as the trigger event. Subsequently, we analyzed the temporal connection and length of NMS Off periods in comparison to motor Off periods.
SUBJECTS AND METHODS
NMS and motor diary data were used from our previous two-center inpatient study on NMS fluctuations in advanced PD, which has been described in detail elsewhere [3]. The study was approved by the Ethics Committees of participating centers and all patients provided written informed consent. We included a total of 32 PD subjects (21 [66%] women) with motor fluctuations (n = 15, 10 [67%] women; mean age: 62.9±6.6 [range: 54–75] years; mean disease duration: 10.5±3.3 [6–18] years; mean duration of motor fluctuations: 50±51 [2–153] months) or without motor fluctuations (n = 17, 11 [65%] women; mean age: 66.4±9.6 [51–81] years [P = 0.236 when compared to fluctuators group; unpaired two-sidedt-test]; mean disease duration: 4.3±2.8 [2–11] years [P < 0.001]). Fluctuating subjects were asked to classify their motor complications as end-of-dose akinesia, On-Off fluctuations, No-On response, dystonia during Off state, peak-dose dyskinesia, biphasic dyskinesia and/or freezing. All fluctuators displayed at least one type of motor complication with a median of 4 different motor complications (interquartile range [IQR]: 2/5, see [3] for details).
All subjects completed a pair of diaries on 5 consecutive days: (a) the modified diary for motor function introduced by Hauser and colleagues with four different motor states (asleep, motor Off, On without dyskinesia, and On with dyskinesia) [2] and (b) a NMS diary asking to rate four key psychiatric (anxiety, depressive mood, inner restlessness, difficulties with concentration/attention), fatigue and four autonomic NMS (excessive sweating, sialorrhea, bladder urgency and dizziness) as present or absent during awake time. For hours with NMS rated as “present”, the NMS state in that hour was defined herein as NMS Off state and if NMS was rated as “absent” the state was interpreted as NMS On state to allow for an easier comparison with motor states.
To analyze the temporal connection between motor and NMS fluctuations, motor Off periods (defined herein as an Off state of at least 1 hour duration following a motor On period of at least 2 hours) from all patients were synchronized by summation of all motor Off hours using the first hour of the motor Off period as the trigger event (start). The NMS Off state hour frequencies were then cross-classified by putting the nominal frequency data (symptom present or absent) into 2×2 contingency tables for each motor Off state hour. Lengths of Off state periods were compared using Mann-Whitney U-tests. We did the same analysis for dyskinetic On periods (defined herein as a dyskinetic On state of at least 1 hour duration following a motor On period without dyskinesia of at least 2 hours). All diary sets were included for analysis. Individual time periods were excluded from analysis if there was no response or more than one response on either diary, or if the patient indicated they were asleep in one diary but not the other diary. Data were analyzed using SPSS 21.0 (SPSS Inc., Chicago, IL). If not mentioned otherwise, all data are displayed as means±SD [range], median [IQR] or numbers (%), significance level was set at P < 0.05 (two-sided test).
RESULTS
Motor Off periods were synchronized with the first hour in motor Off as the trigger event. The results for all motor Off periods (n = 120) are displayed in Fig. 1. Median length of motor Off periods was 2 hours (IQR: 1.0 to 4.0 hours). We detected a clear temporal connection of motor Off periods only with anxiety, depression, problems with concentration and bladder urgency showing an increase of NMS Off frequencies for these NMS in temporal conjunction with the start of motor Off periods (Fig. 1). Except for bladder urgency, NMS Off periods appeared to have longer durations compared to motor Off periods (indicated by the green bars at the end of motor Off periods in Fig. 1 displaying NMS Off hours in motor On state). Statistical analyses confirmed that psychiatric NMS Off periods showed higher median lengths of 3 to 4 hours (P < 0.05, Mann-Whitney U-test; Table 1). Time periods of bladder urgency showed a median length of only 1 hour in most cases (IQR: 1/3 hours). For fatigue, inner restlessness and autonomic NMS other than bladder urgency, we did not observe NMS Off state periods in conjunction with motor Off state periods (see Fig. 1 for dizziness as an example for non-fluctuating autonomic NMS).
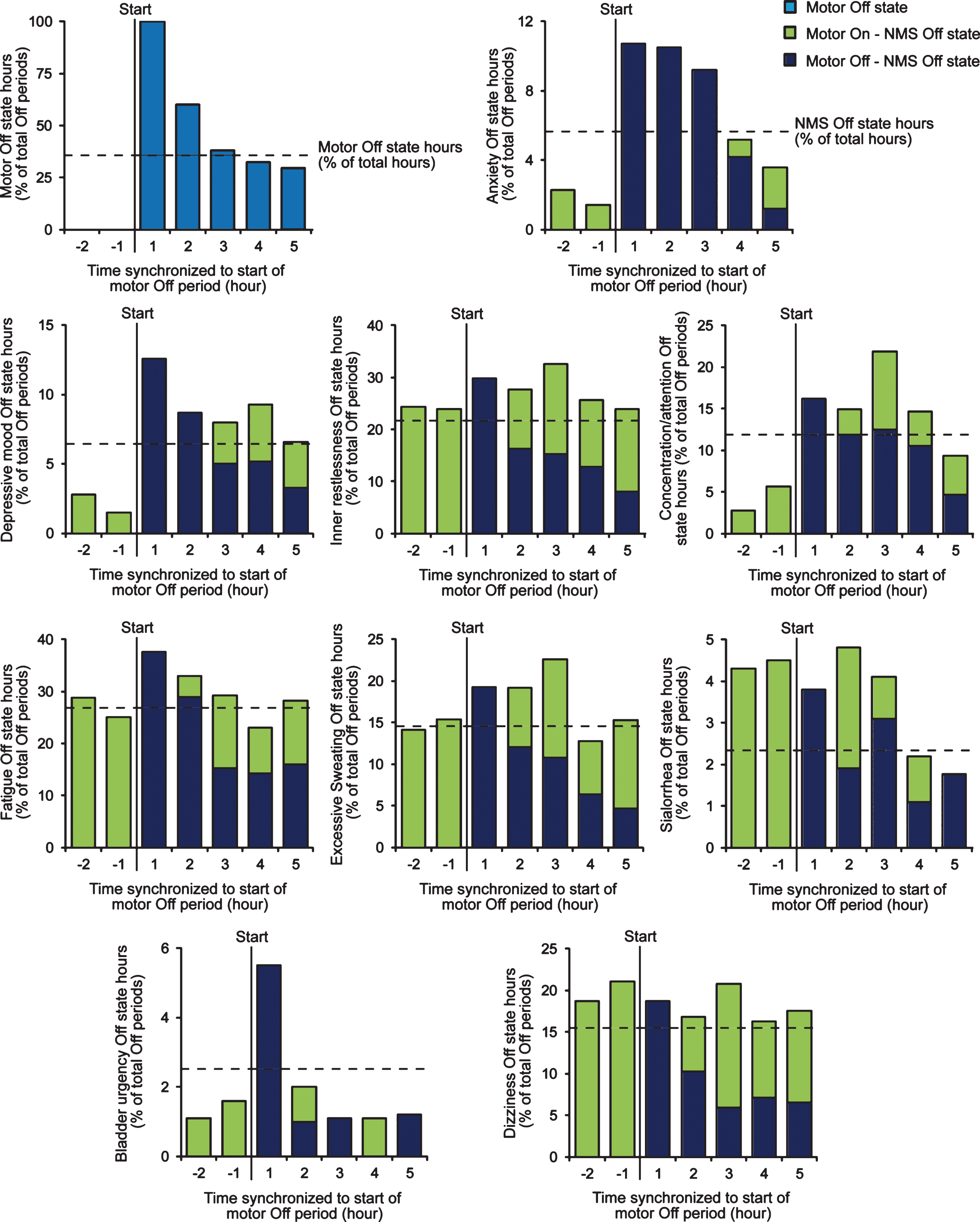
Temporal connection of NMS and hypokinetic motor fluctuations in fluctuating PD patients. To analyze the temporal connection of motor and NMS fluctuations, motor Off state periods (here defined as an Off state of at least 1 hour duration following at least 2 hours in motor On state) from PD home diary data were synchronized with the first hour in motor Off as the trigger event (marked with “start” in diagrams). The NMS Off state hours (hours with NMS rated as present) from NMS diary data were then cross-classified using 2×2 contingency tables for each motor Off state hour. Displayed data are from all motor Off periods detected throughout the study and normalized to the total number of motor Off periods (n = 120).
Length of NMS and motor Off periods in fluctuating PD patients
Data are displayed as median (IQR, interquartile range). P values are from Mann-Whitney-U test.
We detected 58 dyskinetic On periods with a median length of 2 hours (IQR: 1.0 to 5.0 hours). The median length of dyskinetic On periods was not different from the length of motor Off periods (P = 0.358, Mann-Whitney U-test). We observed a temporal connection of dyskinetic On periods only with the mood symptoms anxiety and depression showing short increases of NMS Off frequencies for these NMS one hour before the start of the dyskinetic On period (Fig. 2). The median lengths of the NMS Off periods were short (1.5 hours [IQR: 1.0 to 3.0], but not different from the length of dyskinetic On periods (P > 0.05, Mann-Whitney U-test). A mild temporal connection was also found for excessive sweating Off state and dyskinetic On state hours with a mild increase of excessive sweating starting 1 hour before and lasting until 4 hours after the start of the dyskinetic On period. We did not detect a temporal connection between dyskinetic motor On state periods and NMS ratings for inner restlessness, concentration/attention, fatigue, sialorrhea, bladder urgency and dizziness (Fig. 2 displays exemplarily data on dizziness).
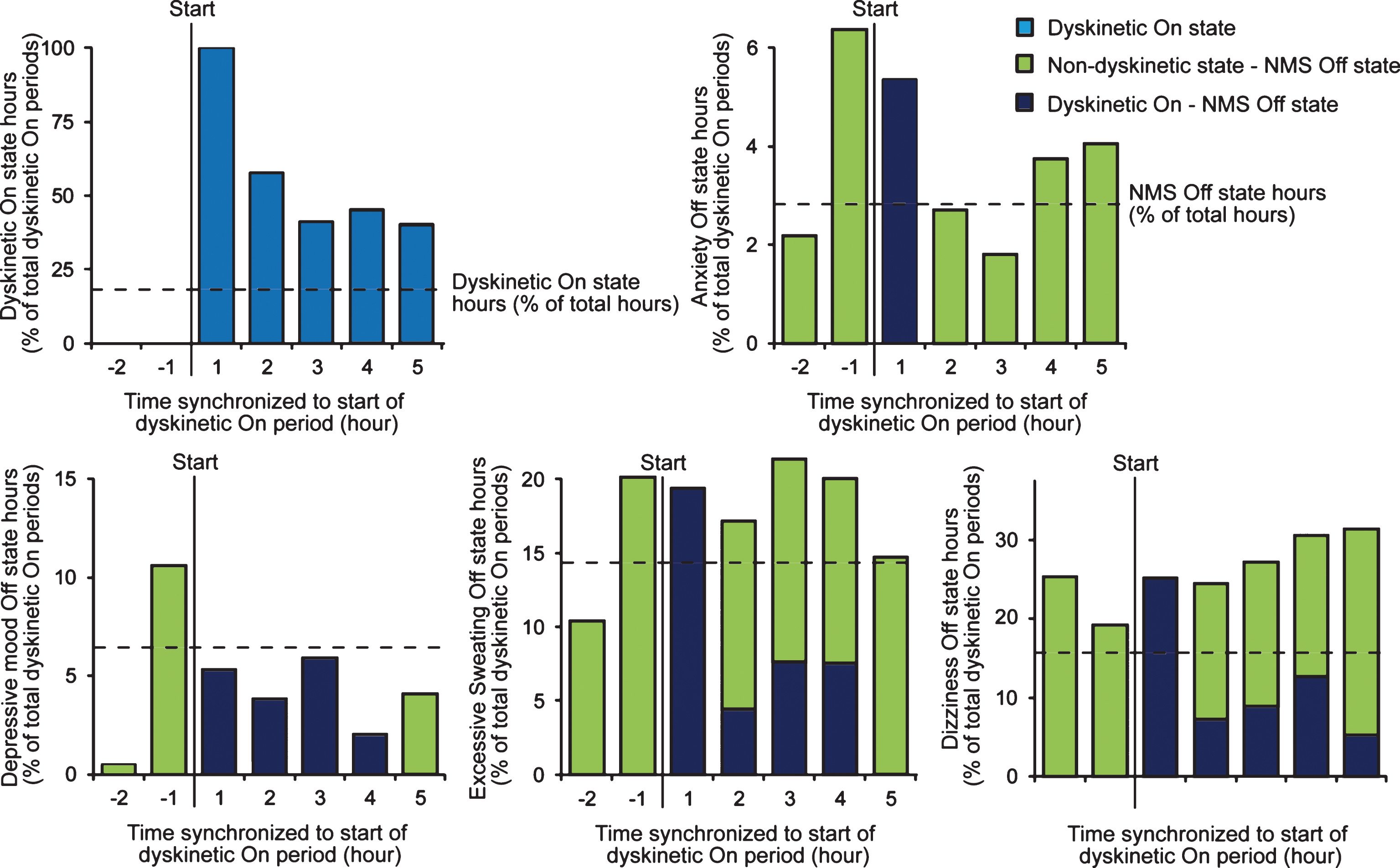
Temporal connection of NMS and hyperkinetic motor fluctuations. To analyze the temporal connection of motor and NMS fluctuations, dyskinetic On state periods (here defined as a dyskinetic On state of at least 1 hour duration following at least 2 hours in non-dyskinetic On state) from PD home diary data were synchronized with the first hour in dyskinetic On state as the trigger event (marked with “start” in diagrams). The NMS Off state hours (hours with NMS rated as present) from NMS diary data were then cross-classified using 2×2 contingency tables for each dyskinetic On state hour. Displayed data are from all dyskinetic On periods detected throughout the study and normalized to the total number of motor Off periods (n = 58). Data for inner restlessness, concentration/attention, fatigue, sialorrhea and bladder urgency showed similar patterns as dizziness with no temporal connection to dyskinetic On state periods and thus omitted from the figure for clarity.
Although we used strict criteria for the definition of non-fluctuating patients [3], three patients (17%) reported short (1 hour) motor Off periods in their diaries due to unknown reasons. In these non-fluctuating PD patients, we did not observe any temporal connection of the very few motor Off state periods (n = 11, all with a duration of 1 hour) with Off periods for all NMS.
DISCUSSION
We here provide first pilot data on timing and kinetics of NMS fluctuations for key psychiatric and autonomic NMS by synchronizing motor Off periods and subsequent cross-classification of NMS Off state hours for each motor Off state hour. We thereby detected a strong temporal connection of motor Off periods with the occurrence of anxiety, depression, concentration/attention deficits and bladder urgency. However, the lengths of NMS Off periods were higher for the psychiatric NMS when compared to motor Off periods. The short duration of bladder urgency periods might be explained by micturition in a timely manner (but we did not check for this in the present study). All other NMS did not show any Off periods in conjunctions with motor Off periods, but relatively stable frequencies of NMS Off state hours before, during and after motor Off periods as in our previous analyses [3]. In addition, we detected a temporal connection of dyskinetic On periods with mood symptoms with a short increase of mood NMS Off frequencies one hour before the start of the dyskinetic On period. The reason for the occurrence and early start of mood NMS Off periods remain enigmatic but might be related to medication timing and different response kinetics of motor and mood NMS to dopaminergic medication [4]. Unfortunately, we do not have data on medication timing in our cohort. The mild increase of excessive sweating during dyskinetic On periods might be related to physical strain due to the hyperkinetic motor state.
The variances in both timing and kinetics of NMS fluctuations might explain the discrepancies between similar circadian fluctuations patterns of most psychiatric NMS compared to those of motor fluctuations and the rather low concordance rates between motor and NMS switches [3]. Indeed, the differences between NMS and motor Off kinetics might also elucidate –at least in part –the weak or even absent correlation of NMS fluctuation severities with motor function measures as observed in previous studies [5, 6].
In the comparison of motor and psychiatric symptoms on an hour-to-hour basis, one issue might be the potential influence of impaired mood on motor ratings in the PD home diary. Moreover, the hour-by-hour rating of psychiatric and autonomic NMS using a novel NMS diary with questions similar to those of the NMSQuest [7] might have a limited validity and diary adherence. However, there is currently no other tool available to assess NMS with high frequency. The diary seems utilizable since the comparison of fluctuating PD patients with non-fluctuators and healthy controls displayed much higher frequencies of Off hours and On-Off state switches for all tested NMS in fluctuating patients [3] showing that the diary assesses –at least in part –NMS fluctuations specifically occurring in fluctuating PD patients. Moreover, we showed moderate convergent validity of diary data with independent measures of related constructs [3]. The selection of nine key NMS together with the heterogeneous and complex pattern of NMS fluctuations for the various NMS [5, 6] limits the interpretation of the results to the nine investigated NMS. In particular, sensory disturbances including pain were not part of the NMS diary and it is thus not possible to draw any conclusions on the temporal connection of pain and motor symptoms/complications from our study [8–10] (for a detailed discussion on the selection of key NMS, refer to [3]). Another limitation of our study is the lack of data on timing of antiparkinsonian medication to correlate the kinetics of motor and NMS fluctuations with medication [4].
Together, timing and kinetics of NMS and motor fluctuations show a strong temporal connection of motor Off periods with the occurrence of some NMS (mood, concentration/attention deficits and bladder urgency) with a sizable length of psychiatric NMS Off periods. These differences in Off period kinetics might explain the low concordance rates of motor and NMS state switches. These data are of particular interest, since they might also explain –at least in part –the weak or even absent correlation of NMS fluctuation severities with motor function measures seen in previous studies [5, 6, 10–14] and thus add a new dimension to the complexity of NMS fluctuations.
CONFLICT OF INTEREST
AS has received unrestricted research grants and consultancy fees from Global Kinetics Corporation, Melbourne, Australia. The authors have no other conflict of interest to report related to this manuscript.
Footnotes
ACKNOWLEDGMENTS
The authors thank all patients for their participation and the study center personnel, namely Cecile Bosredon, Dorena Galle, Rowena Karl and Antonia Maass. This study was supported in part by an unrestricted research grant from Global Kinetics Corporation (GKC), Melbourne, Australia. The financial sponsors of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had the final responsibility for the decision to submit for publication. We also acknowledge the international Parkinson’s disease non-motor group who has contributed to the concept of this work.