
Abstract
Background:
Duchenne muscular dystrophy (DMD) is an X-linked recessive neuromuscular disorder resulting from loss of dystrophin. In addition to its role in muscle, isoforms of dystrophin are expressed in different cell types of the brain, and DMD has been linked to language delays, behavioral abnormalities and learning disabilities.
Objective:
To determine whether disruption of specific DMD isoforms, age, corticosteroid use, ambulation status, or country are associated with behavioral and/or learning concerns in DMD.
Methods:
De-identified data were collected from the Duchenne Registry from 2007–2019. Females, patients with BMD, and those without genetic testing reports were excluded from the cohort. For the genetic analysis, patients were divided into four subgroups based on the location of their mutation and the predicted isoforms affected. Bivariate analysis was conducted using chi-square for categorical variables. Two multivariate logistic regressions were used to assess independent associations with behavioral and learning concerns, respectively, and to estimate the effect size of each variable.
Results:
DMD mutations disrupting expression of Dp140 and Dp71 were associated with a higher likelihood of reported behavioral and learning concerns. Corticosteroid use, categorical age, and country were other factors associated with behavior and learning concerns.
Conclusion:
This data adds to our current understanding of DMD isoforms, their mutational consequence and impact on behavior and learning.
INTRODUCTION
Duchenne muscular dystrophy (DMD) is an X-linked recessive neuromuscular disorder resulting from absent dystrophin protein. In addition to its role in muscle, isoforms of dystrophin encoded by DMD are expressed in different cell types of the brain, and DMD has been linked to language delays, behavioral abnormalities and learning disabilities [1–3]. These less visible aspects of brain dysfunction impact DMD patients’ well-being and quality of life.
DMD is comprised of 79 exons with seven promoters. These promoters yield three full length isoforms Dp427c (found in heart), Dp427m (muscle), and Dp427p (brain) beginning at the 5’ end of the gene, and four shorter isoforms: Dp260 (retina), Dp140 (brain, kidney, and retina), Dp116 (peripheral nerves), and Dp71 (brain and liver) [4–5]. Dp140 and Dp71 are expressed in the fetal brain and mutations affecting these isoforms are associated with neuropsychiatric conditions such as autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), and intellectual disability [6–8].
Recent studies demonstrate a substantial risk for behavioral and learning complications in DMD [9–12], highlighting potential correlations between mutations in DMD that disrupt specific isoforms and neuropsychiatric conditions. Our study adds to these reports by utilizing the Duchenne Registry, an international, patient-reported registry for individuals with Duchenne and Becker muscular dystrophy (BMD) [13–18]. The large, geographically dispersed sample provided by the registry allows us to quantify these associations with greater power. The objective of this study is to determine whether disruption of specific DMD isoforms, age, corticosteroid use, ambulation status, or country are associated with behavioral and/or learning concerns in DMD. We hypothesize that the neurocognitive effects of DMD are multifactorial, however, there may be an underlying genetic predisposition based on mutations affecting DMD isoforms expressed in the brain.
MATERIALS AND METHODS
De-identified data from 2007 through 2019 were exported from the Duchenne Registry. Participants who completed the behavioral and learning surveys were included in the study. Females, patients with BMD, and those without genetic testing reports were excluded from the final analysis. The Duchenne Registry is a core member of the TREAT-NMD Global Registry Network and is approved by the institutional review board through the Geisinger Health System. All participants consent to research prior to registering (Geisinger Medical Center, Danville, Pennsylvania [IRB #2014-062]).
Behavioral and learning concerns were primarily reported by parents or caregivers, although patients aged eighteen or older are permitted to complete their own surveys. Survey participants could choose from three options for behavior and learning respectively: I have a concern and a diagnosis was made; I have a concern and no diagnosis was made; No concern. In our analysis, behavioral and learning concerns were split dichotomously: those reporting a concern (with or without a diagnosis) and those reporting no concern. Surveys through the Duchenne Registry may be updated over time, and our results reflect a participant’s most recent response. Country of residence was divided into two groups: participants from the United States and those from other countries (all continents are represented).
For the genetic analysis, patients were divided into four subgroups based on the location of their mutation and the predicted isoforms affected, as demonstrated by Taylor et al. [19]. The subgroups include those with mutations involving exon 1 to 44, exon 45 to 50, exon 51 to 62, or exon 63 to 79. Full-length dystrophin (Dp427p), Dp140, and Dp71 are expressed in the brain and the groups were created to separate and compare mutations disrupting these isoforms. Owing to the variable expressivity of Dp140 based on mutations in its long 5’untranslated region, those with mutations in exons 45-50 were separated from those with mutations affecting the coding exons of Dp140 [19].
Since all DMD isoforms have alternate start sites and a shared final usage of exons 63 to 79, a mutation disrupting a distal isoform will affect expression of all proximal isoforms. As a result, mutations disrupting Dp71 also disrupt expression of Dp116, Dp140, Dp260, and Dp427. For this reason, the C-terminal end of a patient’s mutation determined which subgroup the patient would be assigned. For example, a patient with a deletion from exon 45 to 52 would be placed in the exon 51 to 62 category, as this mutation would disrupt expression of Dp140 and all proximal isoforms. Figure 1 demonstrates the position of the promoters for each isoform along DMD [20].
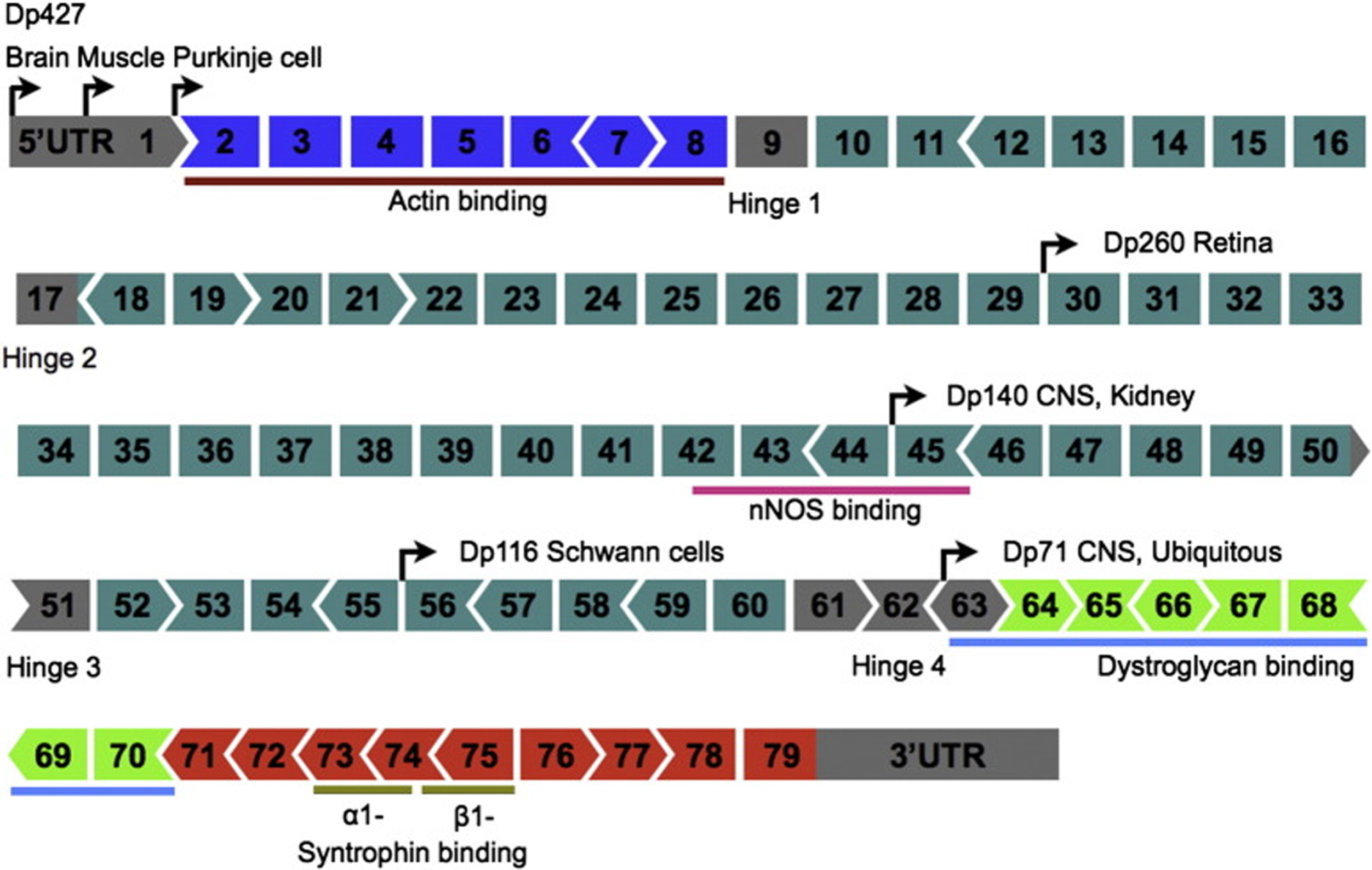
Position of promoters for each isoform along DMD and the tissue types where they are predominately expressed.
Statistical analyses were performed using SAS version 9.4 (SAS institute, Cary, North Carolina). Bivariate analysis was conducted using chi-square for categorical variables. Chi-square testing was used to measure the difference between observed and expected frequencies of outcomes for categorical variables, and to generate P-values for comparisons listed in the results section. Two multivariate logistic regression models were used to assess independent associations with behavioral and learning concerns, respectively, and to estimate the effect size of each variable.
RESULTS
After application of the inclusion/exclusion criteria, the final cohort had 1,381 participants. The mean age of participants was 10.5y (SD 5.8) (Table 1). Most participants were ambulatory (65%), from the United States (74%), and on a corticosteroid (64%). As expected, mutations affecting the Dp140 isoform and its 5’untranslated region were the most prevalent (57%), as this is the known hot spot for DMD mutations. Those mutations disrupting the Dp71 isoform were the least frequent with only 3% of the cohort, but still represented a sizeable group of 45 individuals which permitted sufficient power to search for genetic association. Overall, 39.4% (544/1,381) reported a behavioral concern, and 38.7% (535/1,381) reported a learning concern.
Genetic, physical, behavioral, and learning characteristics of surveyed participants
In the bivariate analysis, DMD isoform, categorical age, and corticosteroid use were associated with behavioral concerns (Table 2). Sixty-two percent of patients with mutations affecting Dp71 reported a behavioral concern, compared to 35% of patients with mutations solely affecting neural expression of Dp427 (P = <0.001). Forty-seven percent of those aged 6–10y had a reported behavioral concern, compared to 26% of those under the age of six (P < 0.001). Corticosteroid users were significantly more likely to report a behavioral concern than the steroid naïve (42% vs. 32%; P = <0.001). Among those using steroids, there was no statistically significant difference in behavior between prednisone and deflazacort users (41% vs. 41%; P = 0.92).
Bivariate analysis for behavioral concerns. (%), row percentage
DMD isoform, categorical age, country, and corticosteroid use had significant associations with learning concerns in the bivariate analysis (Table 3). Seventy-eight percent of patients with mutations affecting Dp71 expressed a learning concern, compared to 28% of patients with mutations only affecting Dp427 CNS expression (P < 0.001). Those who had used a corticosteroid were more likely to report a learning concern compared to the steroid naïve (41% vs 33%; P = 0.006). Among those using steroids, there was no statistically significant difference in learning concerns between prednisone and deflazacort users (43% vs. 37%; P = 0.08).
Bivariate analysis for learning concerns. (%), row percentage
Twenty-seven percent of participants reported both a behavioral and learning concern. Of those reporting a behavioral concern, 68% also reported a concern with learning. Participants who self-reported a behavioral concern were 8.8 times more likely to also report a learning concern (CI 6.86–11.28), compared to those who did not.
The first multivariate regression model assessed for associations between DMD isoform, categorical age, country, and corticosteroid use with behavioral concerns (Table 4). Those with mutations affecting Dp71 expression (exon 63 to 79) were more likely to report a behavioral concern than those with proximal mutations only affecting Dp427 (OR = 3.32; CI 1.70–6.15). Likewise, those with mutations disrupting the coding exons of Dp140 had increased odds of reporting a behavioral concern (OR = 1.61; CI 1.23–2.10). Participants aged 6–10y were 2.59 times more likely to have a reported behavioral concern than those under the age of six (CI 1.86–3.61). Those who had used corticosteroids and discontinued were twice as likely to report behavioral concerns than the steroid naïve (OR = 2.01; CI 1.26–3.18). There was no significant association between prednisone or deflazacort use and behavior in the regression.
Multivariate logistic regression for associations between categorical age, DMD isoform, country, and corticosteroid use with behavioral concerns
The second multivariate regression model had learning concerns as the outcome, and found significant associations between learning and DMD isoform, categorical age, corticosteroid use, and country (Table 5). Disruption of isoforms Dp140 and Dp71 were associated with learning concerns when compared to loss of Dp427 alone. Participants aged between 6–15y were significantly more likely to report a concern compared to those under the age of six. Those from the United States were 1.58 times more likely to report a learning concern than those from other countries (CI 1.20–2.06). Discontinuation of steroids (OR = 1.68; CI 1.05–2.71) and prednisone use (OR = 1.42; CI 1.03–1.96) were associated with increased odds of learning concerns in this model.
Multivariate logistic regression for associations between categorical age, DMD isoform, country, and corticosteroid use with learning concerns
DISCUSSION
The emotional, behavioral, and cognitive aspects of DMD have historically remained secondary to the physical manifestations of this multisystem disease. Recent works have described the impact of those psychological components on the patient and their families, as well as the importance of caring for these symptoms [9, 21]. Our study utilizes the Duchenne Registry, a large international, self-reported registry for patients with Duchenne and Becker muscular dystrophy, to quantify the behavioral and learning concerns of families. We want to utilize this patient-reported data to further understand contributors to neuropsychological issues in DMD.
Recent studies have observed correlations between DMD isoforms and neurodevelopmental disorders. A described correlation is between the Dp71 isoform and cognitive dysfunction [2, 22–24]. Data from the Duchenne Registry supports these findings, as the majority (78%) of participants with mutations affecting Dp71 expression reported a learning concern. Likewise, mutations in Dp71 were significantly associated with behavioral concerns in the bivariate and regression analyses. Dp71 is the prominent DMD isoform expressed in the brain, and our data suggests that mutations disrupting its expression are influencing both learning and behavior.
In addition to Dp71, mutations affecting the coding exons of Dp140 had significant associations with both learning and behavior. Recent studies have described a relationship between loss of Dp140 expression and intellectual disability [25–27]. Dp140 functions in fetal neurodevelopment, and lack of its expression likely impacts behavioral and cognitive function. Of note, those with mutations disrupting the 5‚untranslated region of Dp140 (exons 45 to 50) did not have increased odds of reported learning or behavioral concerns. This finding suggests that mutations disrupting the coding exons of Dp140 have more effect on its neuronal gene expression than those in the 5‚untranslated region.
Overall, our data demonstrates an increasing prevalence of learning and behavioral concerns the further a patient’s mutation is towards the C terminal region. This may be due to the position of Dp140 (5’ at exon 45) and Dp71 (5’ at exon 63), both of which are expressed in the brain and play a role in fetal neurodevelopment [7]. Furthermore, the further downstream a mutation is the more collective isoforms it disrupts, as each isoform shares a terminal exon 79. Therefore, it is likely the cumulative effect of disrupting more isoforms, especially those expressed in the brain, that is impacting the observed increased strength of association with behavior and learning the further downstream a mutation is. Ultimately, we cannot determine whether it is primarily disruption of Dp71 that is impacting the observed associations or the cumulative effect of disrupting all isoforms, especially Dp427p and Dp140.
Categorical age was associated with both behavior and learning in the bivariate analysis and regression models. Patients aged between 6–15y were more likely to have a learning concern than those under the age of 6. It is plausible that learning difficulties are most easily noticed at school, as their performance can be quantified and compared to their peers. On the other hand, astute parents may notice language delays or difficulty with attention or memory, all features of learning deficits seen in young children with DMD [28, 29].
Behavioral concerns were most frequently reported among patients aged 6–10y. Children of this age with DMD tend to be more aware of their differences and limitations which may manifest as depression, anxiety, or a behavioral problem [30]. Those aged between 11–15y also had greater odds of reporting behavioral concerns. During these years, many DMD patients transition into wheelchair use and become increasingly dependent on others for help. Their growing physical disabilities may isolate them from peers and from personal goals [30]. These challenges persist with age, yet we found lower rates of behavioral concerns among those over the age of 15. Quality-of-life studies have observed that despite decreased physical functioning, young adults with DMD report better psychosocial quality-of-life scores than younger patients [31, 32], suggesting development of protective coping skills over time.
In the regression analysis, patients who discontinued corticosteroids had significantly greater odds of reporting behavioral and learning concerns than the steroid naïve. It is possible that steroid use adversely affected patient behavior, attention/concentration, and learning abilities, and that these issues contributed to the family‚s discontinuation of the steroid therapy. However, within the confines of this study, we are unable to determine a causal relationship between steroid use and concerns with behavior/learning or if these concerns contributed to discontinuing treatment. Despite this, a strong association exists between steroid discontinuation and reported neuropsychological concerns.
Prednisone use was associated with greater odds of reported learning and behavioral concerns, although only the association with learning was statistically significant. The effect of long-term prednisone use on behavior is controversial, with some studies reporting an association [33, 34], while other have not [35, 36]. Limited research has been conducted assessing the impact of prednisone on cognition in DMD, and more focused investigation must be done to discern the behavioral and cognitive effects of long-term corticosteroid use in this patient population.
Interestingly, deflazacort use was not associated with either behavior or learning in their respective regression models. The Chi-square testing comparing prednisone and deflazacort showed no significant difference in behavior or learning outcomes. Yet, after adjusting for categorical age, country, and mutation subtype in the multivariate regressions, prednisone had stronger statistical associations with reported behavioral and learning concerns than deflazacort. It is possible that deflazacort has less neuropsychiatric side effects than other steroids. However, given our study design, and lack of granular data on patient steroid use (dose, duration, side effects), we are unable to support this claim and merely offer this as a plausible explanation for our observed findings.
Participants from the United States were one and a half times more likely to report a learning concern than those from other countries. This may be due to societal differences in evaluation and expectations of learning, but further investigation is required. In the regression assessing correlations with behavioral concerns, there was no association between behavior and country.
This study has several limitations. Firstly, due to the nature of the surveys, we were unable to ascertain specific details about each family‚s learning and behavioral concerns. Additionally, the outcomes in this study were self-reported and we are unable to determine whether a family‚s concern was confirmed to be an underlying learning or behavioral disorder. Furthermore, we were unable to assess corticosteroid use in a more detailed manner as we lacked data on dosage, schedule, and length of treatment. Lastly, owing to each isoform sharing a terminal exon, we are unable to sufficiently isolate associations between individual isoforms.
The strengths of this study lie in the large size and the geographical diversity of this cohort, larger than any equivalent study. Data from the Duchenne Registry provides ample statistical power to assess for factors influencing learning and behavioral concerns in DMD. This sample allowed us to further corroborate the established correlations between DMD isoforms and behavior and learning. Overall, there is a need for prospective observational studies assessing behavioral and learning difficulties over time. These studies should focus on identifying areas for psychosocial intervention, allowing physicians and caregivers to improve the quality of life for patients with DMD.
Footnotes
ACKNOWLEDGMENTS
We thank Dr. Stanley F. Nelson, MD (UCLA) for providing his insights and revisions to the manuscript.
CONFLICT OF INTERESTS
None.