
Abstract
Background:
Myotonic dystrophy type 1 (DM1) is the most prevalent adult form of neuromuscular disorders, for which a decrease of participation with age is known. However, little is known about facilitators and barriers to participation, especially from the perspective of both patients and caregivers.
Objective:
This study explored and explained changes in participation post-diagnosis with myotonic dystrophy type 1 from the perspective of six adults, their relatives and nurse case managers.
Methods:
A multiple case study was carried out with these triads (n = 6) using semi-structured individual interviews, medical charts, and a participation patient-reported outcome measure. The six cases were built around three women and three men (age: 40–56 years; disease duration: 19–39 years). Their “relatives” were mainly family members. Nurse case managers had done annual follow-ups with all the adults for approximately ten years. Changes in participation were characterized generally by: 1) heterogeneity, 2) insidious increase in restrictions, and more specifically by: 3) redesigning accomplishment, 4) progressive social isolation, 5) restrictions in life-space mobility, and 6) increasingly sedentary activities.
Results:
Important facilitators of participation were the adult’s resilience, highly meaningful activities, social support, living arrangement, and willingness to use technical aids. Barriers were mostly related to symptoms and a precarious social network, and were affected by misfit and potential syndemic interactions between personal (e.g., comorbidities) and environmental (e.g., stigma) factors.
Conclusion:
This study identified key facilitators and barriers and their underlying processes, which should be integrated into the evaluation and intervention framework to optimize participation over time.
Keywords
INTRODUCTION
Myotonic dystrophy type 1 (DM1), the most prevalent adult form of neuromuscular disorders, is a dominant autosomal hereditary disease often compared to premature aging [1–4]. It is a progressive multisystemic condition [5] that frequently leads to multiple impairments and increased restrictions in participation in daily and social activities [6, 7]. Participation could be defined by the level of accomplishment and need for assistance in daily and social activities [8, 9]. Although important steps have been made in understanding the pathophysiology of DM1, as yet there is no cure [10, 11].
Managing the symptoms and optimizing participation and quality of life, therefore, are often the main goals of the people directly involved, i.e., adults with DM1, their families, and health professionals. To achieve these goals, experts recommend using a prognostic approach, i.e., health supervision with anticipatory guidance [12], and annual follow-ups for preventive and management interventions [13]. Implementing such an approach requires a better understanding of short- and long-term changes in participation as well as potential facilitators and barriers and their underlying processes. Efforts to find a cure with well-designed therapeutic trials or longitudinal study also need a deeper understanding of potential factors affecting the outcomes being studied, such as participation, and control of potential confounding factors (adjust for specific personal or environmental factors in analyses) [14].
For adults with DM1, it is known that participation decreases slowly over the long term and more and more activities are impeded [6, 16]. However, little is known about perceived changes in participation over time, i.e., changes in daily and social activities and the sequence in which restrictions occur. In the aging population, participation restrictions usually start with instrumental activities of daily living (e.g., household chores) followed by activities of daily living (e.g., self-care) and mobility [17]. In a literature overview of the population with neuromuscular disorders, only one long-term longitudinal study [18] including among others participants with DM1 aimed to elucidate experiences of living with the disease and its impact on activities over ten years. It was found that more time was needed and new strategies were used to continue doing daily and social activities. Housing, mobility, interpersonal relationships, work, and recreation were the main categories perceived as declining over time [18], but the sequence of restrictions occurrence was not investigated. More recently, transversal qualitative studies had similar findings from the perspective of adults with DM1 and their next-of-kin [19]. In addition, the adults reported giving up more demanding activities [20]. A deeper understanding of perceived changes and the sequence of occurrence of participation restrictions is needed, including what affects these changes. Quantitative and qualitative studies in DM1 have identified potential associations between participation restrictions and personal and environmental facilitators [21] and especially barriers [6, 21–31]. Using technical aids and adjusting expectations regarding participation were the main facilitators [21]. Muscle weakness and fatigue were among the primary barriers to participation [18, 24–29]. Other barriers frequently found were: pain [22, 25], limited family income [21, 29], and lack of initiative or motivation [18, 30] for personal factors, as well as a lack of social support [18, 24], perceived obstacles in the physical environment and accessibility [29] for environmental factors. However, most studies did not use a holistic conceptual framework to investigate these factors and did not capture an in-depth comprehensive picture of the processes underlying facilitators and barriers to changes in participation. Moreover, although multiple perspectives are required to understand a complex phenomenon like participation, most of these studies only described potential associations from the perspective of adults with DM1; a few [19, 20] added a relative’s perspective, and none considered health professionals’ views. To identify personal and environmental factors that act as facilitators and barriers to participation and explain how these factors interact, a better understanding of changes in participation and the underlying processes is needed from the perspective of the people directly involved. This study thus aimed to explore and explain changes in participation between diagnosis and the present time (15–37 years) from the perspectives of the adults with DM1, their relatives, and nurse case managers. The use of triads aimed to triangulate the perspectives to obtain the most holistic understanding possible, with less focus on similarities or differences of viewpoints.
MATERIALS AND METHODS
Design and participants
This study is part of a larger interdisciplinary longitudinal study characterizing DM1’s natural progression over nine years (two measurements taken during this 9-year period), including a description of changes in participation and identification of predictors of change [7, 32]. Structured by the Human Development Model –Disability Creation Process (HDM-DCP) framework, a qualitative multiple case study design [33] provided an in-depth description of each case, i.e., individual changes in participation and the involvement of personal and environmental facilitators and barriers. A purposive sample of six cases was recruited, with each informed by a triad: 1) an adult with DM1 (n = 6), 2) a close relative (n = 6), and 3) their nurse case manager from the Neuromuscular Clinic (n = 3). The adults with DM1 were participants in the longitudinal study [7, 29]. To be eligible for the current study, they had to: 1) have DM1 confirmed by genetic analysis with the juvenile or adult phenotype; 2) be 18 years of age or older; 3) speak French, 4) have a clinically significant change (improvement or decline of at least 0.5/9 [34] on the Assessment of Life Habits 3.1 [LIFE-H 3.1]; [35]) in three or more categories of participation (12 categories in all) in the longitudinal study, and 5) have a close relative (mainly but not exclusively family members) and a nurse case manager who agreed to participate in the study. Since they had different prognoses, individuals with the other phenotypes of DM1 were excluded as well as those with another disease affecting participation (like stroke). Of the 115 participants from the longitudinal study, 87 were still alive at the time of this study and 49 met the inclusion criteria. A maximum variation sampling strategy [36] considering expert triage [37] was based on sex, age, and direction of participation change of the adults with DM1 (improvement or decline in participation). They were first contacted by a research assistant, invited to identify a significant relative (someone seen more than once a month for over ten years, including family and friends), and asked if their nurse case manager could be interviewed regarding her perception of their changes in participation over time. Before data collection, individual written informed consent to participate in the study was given by all participants. Grocery gift cards were given to the adults with DM1 and their relatives to compensate for their time. Nurse case managers were paid to participate by the Neuromuscular Clinic. The Ethics Review Board of the Centre intégré universitaire de santé et de services sociaux du Saguenay–Lac-St-Jean approved the study protocol (#2015-006).
Research context
The study was conducted in Saguenay–Lac-St-Jean (eastern part of the province of Quebec, Canada) which has the highest prevalence (<158/100,000) of people with DM1 [38]. Post-diagnosis, all study participants received health services from an interdisciplinary team coordinated by a nurse case manager from the local Neuromuscular Clinic. Quebec’s healthcare system provides free province-wide health insurance. Like Quebec’s other rehabilitation centers, the Neuromuscular Clinic uses the HDM-DCP as a main framework. This holistic framework provides a conceptualization and operational definition of participation and considers interactions between personal and environmental factors that may facilitate or impede participation [8]. For example, a restriction in participation arises when the social and physical environment cannot compensate for a personal impairment. Considering the person’s perspective as well as the level of participation and the personal and environmental factors, the HDM-DCP also provides nomenclature and classification for these concepts [8]. The research group is located on the same floor as the Neuromuscular Clinic, but only one research team member (CG) has her office there. In the present study, the principal investigator (KR) was a doctoral candidate supervised by two senior professors/researchers with expertise in neuromuscular disorders and participation. All researchers were occupational therapists.
Data collection
Questionnaires
Sociodemographic characteristics of all participants were collected using a generic questionnaire or extracted from their medical files. For adults with DM1, recalled time since diagnosis, self-rated health, ambulatory status, and participation level were also collected. To assess self-rated health, they answered the question: “How is your health generally right now?” on a scale of excellent, good, fair, or poor. Based on the HDM-DCP, participation was assessed using the LIFE-H 3.1 [35] for three measurement points: the first two extracted from the longitudinal study in 2002-04 (T1) and 2011-13 (T2) and the third collected at the end of data collection for adults with DM1 by the principal investigator in 2017-18 (T3). The principal investigator was trained to administer the LIFE-H by the occupational therapist who conducted the longitudinal study and, to limit interrater discrepancies, to use the same procedure and examples. The LIFE-H 3.1 is a 77-item questionnaire assessing level of accomplishment and satisfaction globally and for two domains, daily and social activities, each encompassing six categories. Daily activities categories are nutrition, fitness, personal care, communication, housing, and mobility, while social activities encompass responsibilities, interpersonal relationships, community life, education, employment, and recreation. Since none of the adults with DM1 were at school or employed during the longitudinal or current study, the education and employment categories were not applicable. Accomplishment and satisfaction levels were assessed respectively with 10- and 5-point scales, where higher scores indicate greater participation and satisfaction. Used as one of the inclusion criteria for this study, a minimal clinically important difference (MCID) of 0.5 was previously set for accomplishment level [34]. The LIFE-H presents excellent intrarater (intraclass correlation coefficients [ICC]: 0.80 to 0.91) and interrater (ICC: 0.86 to 0.92) reliability in the DM1 population for all scores except two because of very homogeneous scores (fitness: ICC of 0.20 and 0.21; communication: ICC of 0.12 and 0.47 [39]).
Semi-structured interviews
The principal investigator conducted individual semi-structured interviews with each triad participant separately, at their home for adults and relatives and at the Neuromuscular Clinic for nurses. Adults with DM1 were interviewed twice, before and after other participants in their triad; each interview lasted about 60–90 minutes. Most relatives and nurses were interviewed once for about 60–90 minutes and 45–60 minutes, respectively. This interview sequence allowed the principal investigator to add specific questions in the second interview with adults with DM1 based on information given by their relatives and nurses. All interviews were conducted with semi-structured interview guides developed for this study and adapted for each type of participant (adults with DM1, relatives, and nurses). To get a holistic understanding of participation, the interview guides were structured based on the HDM-DCP. Guides for relatives and nurses focused on their perspective of the adult with DM1’s changes in participation. To explore global changes in participation as well as the main facilitators and barriers and their interactions, the guide for the first interview with adults with DM1 included open-ended questions such as: “Since you were diagnosed with DM1, what changes have occurred in how you do your usual activities?” and “What does have caused these changes?” For the second interview, changes in specific activities as well as more specific facilitators and barriers were explored, with open-ended questions such as: “Describe to me how [this activity] changed” and “What does have caused the changes in [this activity]?” Before data collection, interview guides were reviewed by two DM1 research team members not involved in this study (MLa, a nursing professor/researcher, and MT, a doctoral candidate in social work). The interview guide for adults with DM1 was pretested with a patient/partner of the research group, resulting in minor changes to questions. The guides evolved during data collection and specific open-ended questions were added, such as “What is your motivation to do the activity now and before your diagnosis?”. Interviews were digitally audio-recorded and transcribed in full. Following the interviews, a synthesis of the discussion was mailed to each participant. A week later, the principal investigator followed up by phone to verify synthesis accuracy, ask further questions or make clarifications and corrections, if necessary. Only one change was made about the purchase of a technical aid in the synthesis of one adult with DM1.
Medical chart reviews
Between the two interviews with adults with DM1, the principal investigator reviewed their medical charts from the Neuromuscular Clinic. An extraction grid (see Supplemental Appendix) was used to identify information about the sequence of occurrence of participation restrictions along with personal and environmental factors acting as facilitators or barriers. This information was retrieved from the diagnosis in the chart review and extracted from the clinical notes of the interdisciplinary team (nurse, neurologist, physician, physical therapist, and occupational therapist).
Artifacts
Artifacts of important facilitators and barriers to participation identified in the environ–ment of adults with DM1 were photographed by the principal investigator immediately after the first interview with them. Although they had consented in writing, participants also had to consent verbally before the artifacts were photographed and anonymized.
Field notes
Field notes, mainly audiotaped and handwritten, were used during data collection and analysis to document observations (e.g., interview context) and analytical thoughts about the cases.
Data analysis
To explore and explain changes in participation along with the processes underlying facilitators and barriers in personal and environmental factors, a thematic content analysis [40] was performed using all the interview transcripts, medical charts, clinical interpretation of LIFE-H scores, artifacts, and field notes. An evolving mixed coding manual and data extraction grids were used. The analysis was first inductive followed by a deductive approach, i.e., the themes first emerged from the data and then were organized and renamed according to the HDM-DCP. Between the diagnosis and this study, changes in participation were identified qualitatively when an increase or decrease in level of accomplishment or satisfaction was reported by participants during the interview or documented in the medical chart. Changes in participation between the longitudinal study and current study were identified quantitatively when changes in LIFE-H scores were above the MCID, indicating an increase or decrease in accomplishment level. As the LIFE-H measures partly covered the current investigation’s timeframe, they were used to enrich our overall understanding of changes in participation from the longitudinal study and to supplement information regarding the sequence of occurrence of participation restrictions. A preliminary analysis was performed between each interview to adapt interview guides and provide a synthesis. In-depth analysis was carried out at the end of the data collection. Although it was possible to add other cases if research questions were not fully answered, no addition was deemed required. The participants agreed to be contacted again at need. No additional contact was however necessary. Analysis and interpretation were monitored constantly to ensure rigor [41]. In particular, codes were reviewed and discussed with the last two authors and another member of the research team (MT). The data saturation point appears to have been reached, i.e., no new themes emerged when the last case was analyzed. To contextualize and triangulate the perspectives of each triad participant, an intra-case analysis of the interview transcripts, LIFE-H scores, medical chart reviews, artifacts, and field notes was first performed with pattern matching logic [42]. As suggested by Yin [42], to identify recurring and contrasting themes from one case to the next, an intercase analysis was then carried out with cross-case synthesis logic, i.e., themes related to changes in participation and facilitators and barriers were compared using syntheses and matrices. Finally, to illustrate a temporal sequence of occurrence of participation restrictions in function of time since first symptoms onset and according to age (supplementary analysis), medical chart data were crossed in a chronological sequence with LIFE-H scores and interview transcripts if participants provided sufficient temporal markers (e.g., “I stopped dancing when I was 30–35”). To identify the onset of the first symptoms (e.g., weakness, clinical myotonia) that determined the start of the temporal sequence, the neurologist’s notes were used. QRS NVivo (version 12.0 for Windows; QRS International) was used for the analyses, Microsoft Word for the additional syntheses and matrices, and SPSS (version 25.0 for Windows; SPSS Inc) for the temporal sequencing.
RESULTS
Demographics
Of the eight adults with DM1 invited to participate, six accepted and two refused (not interested). Three women and three men between the ages of 40 and 56 participated in the study; the majority (4; 66.7%) had the juvenile form of DM1 (Table 1). All had a high school education or less and a variety of mobility capacities (from ambulant to wheelchair-bound); half rated their health as fair. They presented multiple comorbidities and antecedents, the most common being musculoskeletal disorders, depression, anxiety, vascular disorders, and diabetes. The majority (4; 66.7%) of relatives were female family members, and half were over age 60. Contact frequency in the previous year between adults and relatives varied from at least once a day to twice a month. Nurse case managers were all women between the ages of 35 and 45. They had done in-person annual follow-ups with the adults with DM1 for approximately ten years and, when necessary, additional phone contacts.
Characteristics of triad participants in each case
*Extracted from medical files Notes. M = man; W = woman; J = juvenile; A = adult; Y = yes (ambulant); N = no (wheelchair-bound). Participants in each triad: Adult with DM1 (A#); Relative (R#); Nurse case manager identification-case number (N$-#)).
Changes in participation since DM1 diagnosis
Six themes described the changes in participation between DM1 diagnosis and the present time. General changes included heterogeneous changes and an insidious increase in restrictions while specific changes encompassed redesigning accomplishment, progressive social isolation, restrictions in life-space mobility, and increasingly sedentary activities (Table 2). Each theme included up to three secondary themes. As experts of their experience, adults with DM1 provided the richest descriptions, and relatives and nurses confirmed the facts, sometimes with the help of file notes for the interveners.
Exploration of changes in participation since diagnosis
Note. A# = Adult with DM1 with relevant triad #; R# = Relative with relevant triad #; N$-# = Nurse case manager $ identification with relevant triad #, where applicable. C = convergence of viewpoint with the theme; D = divergence of viewpoint with the theme; the box was left blank when the participant did not address the theme.
General changes –Heterogeneous changes
Since diagnosis, all cases presented heterogeneous changes mainly characterized by a slow progressive decline in participation (Table 2) with varying degrees of restrictions depending on activities. LIFE-H results showed a clinically significant decline in domains and many categories for all adults with DM1 (Table 3). Between T1 and T2 (nine-year interval), as an inclusion criterion, they had to present a clinically significant change in at least three categories, but results showed various patterns of change with different categories affected in each case (see underlined scores in Table 3). Between T2 and T3 (four-year interval), a possible acceleration in the decline was observed overall (see bolded scores in Table 3). Participation varied greatly from one category to another, leading to a heterogeneous portrait of changes over time, i.e., pattern of decline, improvement, stability, and a combination thereof.
Participation scores over time in each case
†Extracted from longitudinal study. Notes. Clinically significant changes (|≥0.5|/9) in LIFE-H are shown as underlined scores for the longitudinal study (T1-T2) and bold scores for changes between T2 and T3; a higher score indicates greater participation.
Due to fluctuations in some symptoms,
“I don’t know if I’ll be able to go to my nephew’s birthday party. I [only] know from day to day. I can’t plan to do [activities], make future plans.”
When comparing all cases, a trend towards a temporal sequence of occurrence of participation restrictions was identified in function of time since the onset of the first symptoms (Fig. 1). This trend was similar according to the age of the adults with DM1 (Supplementary Figure 1). Three categories, i.e., education, employment, and responsibilities, tended to be restricted earlier in the disease course (about five years post-onset of the first symptoms). Personal care, community life, and communication tended to be restricted later (about 20 years after symptoms onset). For most categories, occurrence of participation restrictions after the onset of the first symptoms varied greatly, from 5 to 25 years.
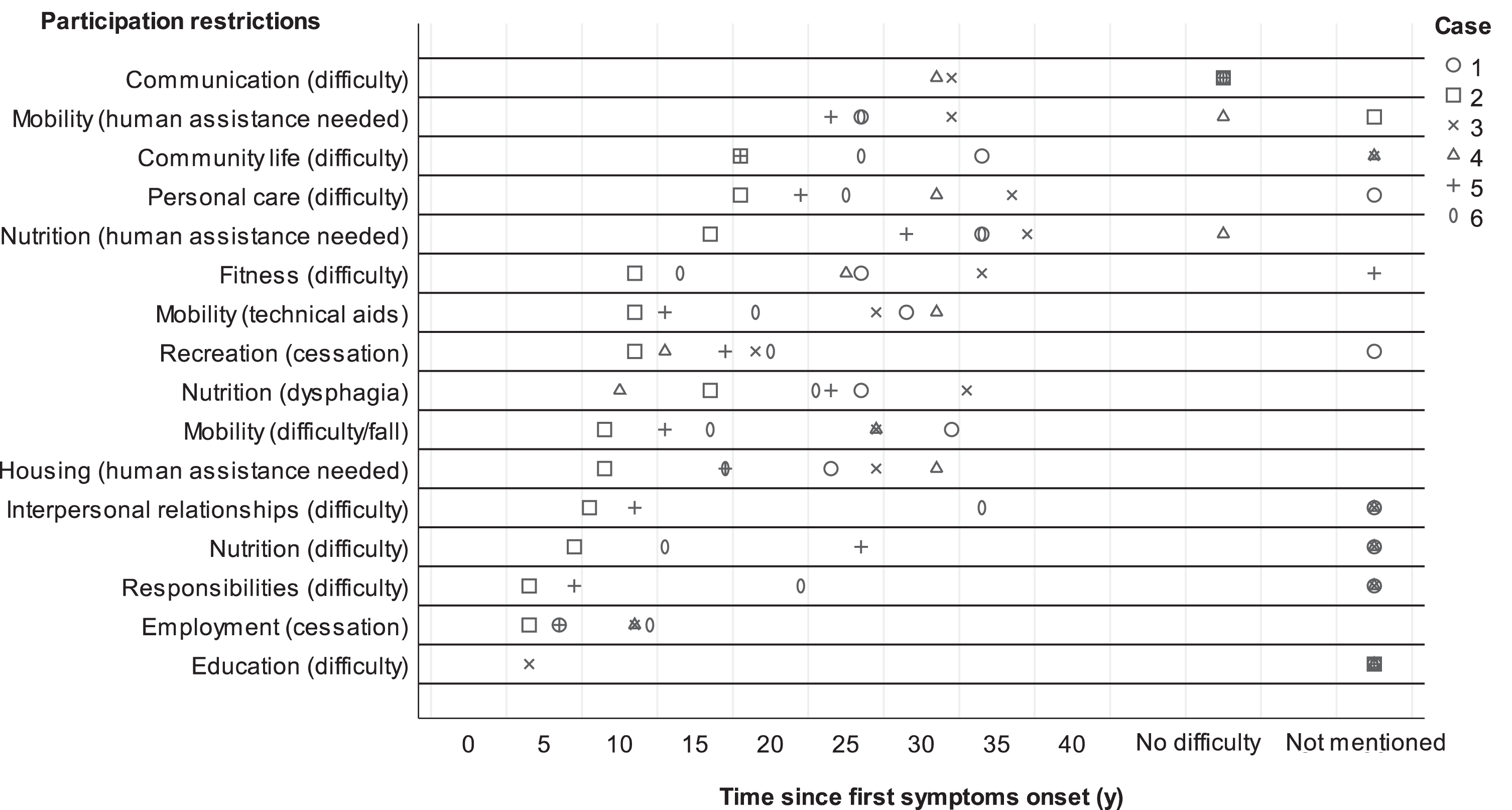
Temporal sequence of participation restrictions since first symptom onset. Notes. Complete description of participation restrictions in order from bottom to top: Education (first-reported difficulty with education); Employment (first-reported employment cessation); Responsibilities (first-reported difficulty with budget or caring for family member); Nutrition (first-reported difficulty handling kitchen objects); Interpersonal relationships (first-reported difficulty with family relationships); Housing (first request for household assistance service or first-reported human assistance); Mobility (first-reported walking difficulty or fall); Nutrition (first-reported episode of dysphagia); Recreation (first-reported cessation of active or social recreational activity); Mobility (first request for mobility aids, not including electric wheelchair or 3- or 4-wheeled electric scooter); Fitness (first-reported episode of sleep disturbance); Nutrition (first request for meal delivery service or first-reported human assistance); Personal care (first-reported difficulty with dressing or washing); Community life (first-reported difficulty with using a business (shopping) or participating in a community group); Mobility (first request for electric wheelchair or 3- or 4-wheeled electric scooter or adapted transportation service or first-reported human assistance); Communication (first-observed signs of dysarthria affecting communication).
General changes –Insidious increase in restrictions
With the slow progression of disease, restrictions in activities occurred insidiously, i.e., so slowly they were often imperceptible in the person’s daily life (Table 2). Most adults with DM1 described
“Two years ago, I used to make macaroni. [. . .] I thought I could [stir the macaroni], but when I picked up the spoon, I found that, without warning, I couldn’t do it anymore.”
A1 and nurse identified as b (Nb) noticed that
Specific changes –Redesigning accomplishment
All triads’ participants recognized the need and importance to rethink how to do activities based on individual interests and changes in abilities and environment (Table 2). Redesigning accomplishment involved adults with DM1 and also their relatives, depending on which activities they participated in. Except for two relatives, all participants noted that the six adults with DM1 had to
Adults with DM1 redesigned accomplishment by
During the redesigning accomplishments process,
Specific changes –Progressive social isolation
As time went by, social networks of adults with DM1 got smaller, leading to progressive social isolation (Table 2). For some, current social networks were limited to one or three family members and one or two friends at most, as explained for A4 by Nb-4:
“He is often lonely. [. . .] His network is his family. People with motor problems go out less, fewer people visit them, they self-isolate.”
For the relative from the fourth triad (R4) however, she felt her son was less isolated as a mature adult than when he was younger. Nearly all cases had
“I don’t have friends any longer. They all [left] when they saw that I couldn’t do anything anymore.”
After their network disintegrated, it was hard for nearly all cases to re-create, then maintain, a large social network.
Contributing to progressively socially isolated situations, all cases had
Specific changes –Restrictions in life-space mobility
Over time, all cases exhibited more difficulty with going out often or going far from home (Table 2). First, all cases
Second, four adults with DM1
“Before, I used to go to restaurants downtown, I’d take the bus [. . . ] but now I go to the [fast food restaurant near me]. [. . . ] It’s my monthly outing.”
As time passed, R2 found that her cousin was staying closer to home, although A2 felt that she could go anywhere she want if she had a car. Nc-5 thought A5 used to stay closer to her home when she lived with her ex-husband but now, living in a private home facility, she used her four-wheeled scooter to go further away.
Specific changes –Increasingly sedentary activities
Over time, activities became more sedentary, i.e., an increase in activities done mostly sitting or lying down and requiring less energy. For five cases, watching television became the main activity in their occupational routine. Nb-3 described this for A3:
“He watches TV. [. . . ] He’s not as active as before. With the wheelchair and his weakness, it’s challenging to go out [and] do recreational activities.”
While adults with DM1 do a selection of activities that are less demanding physically when redesigning accomplishments, are increasingly socially isolated and experience more and more restrictions in their life-space mobility, more sedentary behaviors occurred across all three previous themes.
Facilitators and barriers to participation over time and their underlying processes
Only slightly more than one quarter (11/37 factors; 29%) of personal factors were considered facilitators or both facilitators and barriers (Table 4). Conversely, nearly three quarters (18/25 factors; 72%) of environmental factors were facilitators or both. Processes underlying each facilitator and barrier accounted for participation changes (Table 4). They were also related to themes in the previous section 3.2 (Table 2) or to participation domains and categories (Table 3). However, interactions between facilitators and barriers in personal and environmental factors presented a more comprehensive explanation of participation changes through two distinct processes, namely the fit between factors and a potential syndemic interaction.
Personal and environmental factors and interactions affecting participation since DM1 diagnosis, structured using HDM-DCP framework
Notes. A# = Adult with DM1 + relevant triad #; R# = Relative + relevant triad #; N$-# = Nurse case manager $ identification + relevant triad #, where applicable. (+) = facilitator; (–) = barrier.
In personal factors, the most important
“It took a long time before she accepted the disease. But now, she is able to overcome daily problems; find solutions when she encounters difficulty [in her activities]”
To foster participation of adults with DM1 over time, support from family, adaptation and arrangement of the home and community, and use of technical aids turned out to be essential environmental factors (Table 4). To address health-related questions and receive appropriate care to minimize participation restrictions over time, personalized follow-ups with a nurse case manager were also a very important component of healthcare improvement. As a dedicated resource, nurses were available to manage the needs of adults with DM1 when they contact them. Frequently, nurses had to give immediate systemic health-related counselling or referred and supported the adult to provide the appropriate resource. Such management improved participation at a specific moment for all adults. The most common
In addition,
The

Suboptimal environment of case 3 when participating in bathing activity. Note. The adult with DM1 was unable to get close enough to the bathtub with his wheelchair to transfer safely because of limited space, combined with placement of toilet and bathtub, and a floor-to-ceiling pole.
Interactions between personal and environmental factors through a
“All the symptoms [of DM1 and comorbidities] are obstacles for them. [. . . ] Their family members do not understand the disease [or] are not considerate about the symptoms. Not to say about the attitude of some people in the community. To get out of the house, they have to overcome so many [obstacles].”
Facilitators and barriers, formulated as themes, from the triads’ perspectives were identified in all conceptual domains of the HDM-DCP (Fig. 3). Temporal interaction linked to the fit and to a potential syndemic interaction between facilitators and barriers in personal and environmental factors could account for the strongest trends in participation changes (Fig. 3), including their heterogeneity.
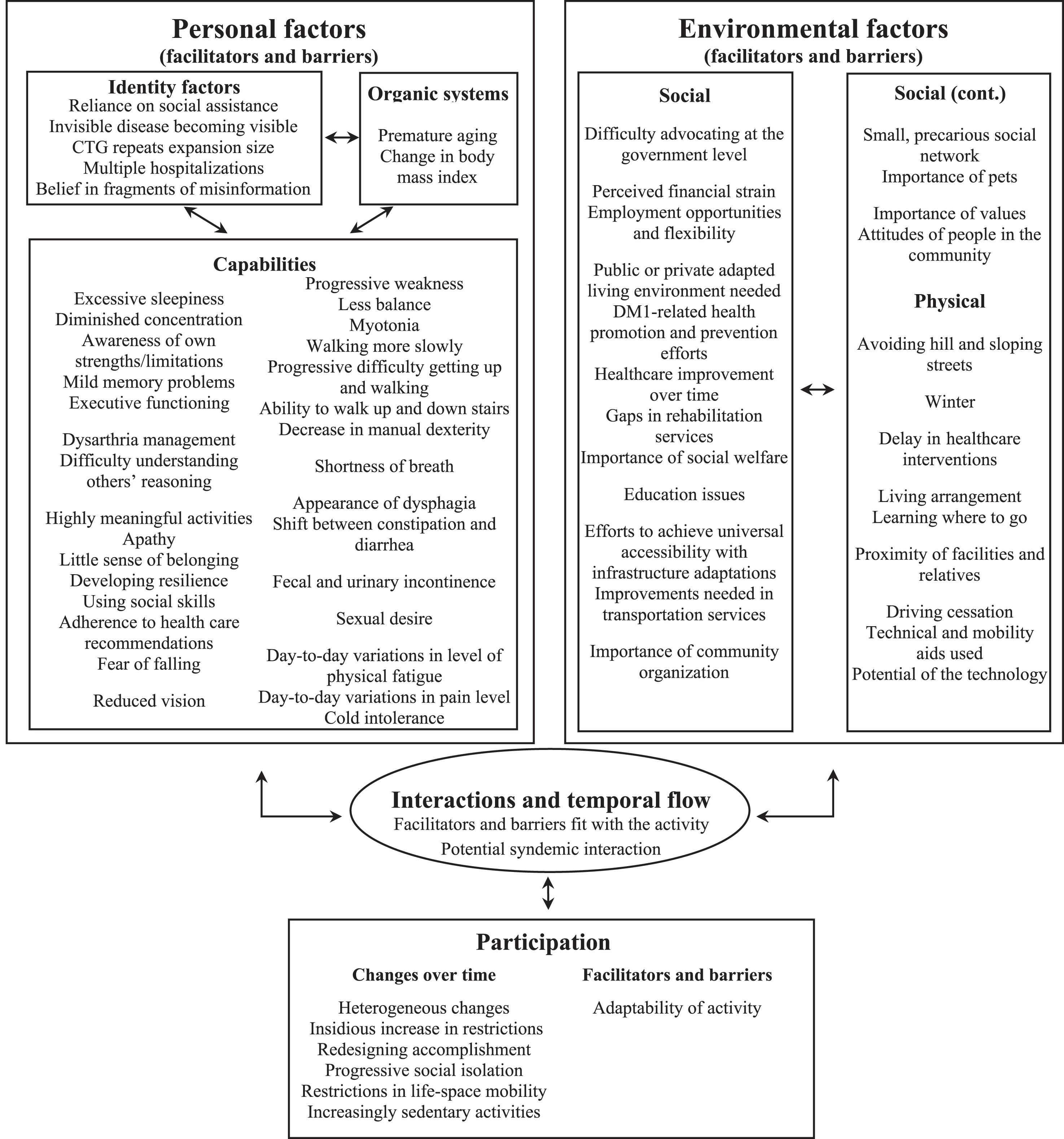
Synthesis of changes in participation over time, and facilitators and barriers for adults with DM1, based on an adapted version of the HDM-DCP framework that aimed to integrate multiple individual’s perspectives to obtain the most holistic understanding possible.
DISCUSSION
This study used a holistic framework to explore changes in participation of adults with DM1 from the perspective of the people directly involved, and explain changes with potential facilitators and barriers along with their underlying processes. Since their diagnosis, i.e., over several decades, adults with DM1 experienced a slow, heterogeneous, and insidious decline in their participation. They redesigned how they did some or most of their daily and social activities, but progressive social isolation, restrictions in life-space mobility, and sedentary behaviors increased. The lack of fit between multiple personal and environmental factors (similar to Lawton’s ecological model of aging [44]) and the co-occurrence of comorbidities and sociocultural obstacles (similar to the syndemic concept of health [43]) exacerbated participation restrictions over time. These results have implications in terms of the decline in participation since DM1 diagnosis, multifactorial nature of participation changes, and clinical practice.
Decline in participation since DM1 diagnosis
Mainly characterized by a slow decline in participation post-diagnosis, the heterogeneous changes found in this study are in line with previous studies on the evolution of participation in slowly progressive neuromuscular disorders, including DM1 [6, 19]. The sequence of occurrence of restrictions in participation was consistent with the work in DM1 of Nätterlund et al. [16] and Boström et al. [15] that identified an increase in restrictions in housing and mobility over five to ten years, and in personal care and recreation after ten years. Progressive social isolation related to loss of social network was also highlighted in a previous study [18]. In addition, the redesigning of accomplishment by adults with DM1 and some of their relatives is consistent with the modification of activities in previous studies [18–21]. The efficacy of redesigning accomplishment was partly dependent on executive functions (e.g., problem-solving skills) of adults with DM1, which was also highlighted in other studies by individuals with DM1 [45] and their caregivers [46]. In the current study, adults with DM1 and their relatives had redesigned their participation to constantly adjust to small day-to-day challenges and cope with progressive social isolation and life-space mobility restrictions. The insidious increase in restrictions, with adults with DM1 facing turning points that reactivated their grieving process, might be attributable to minor adjustments made over an extended period. Photovoice used with nine adults with DM1 described a similar constant grieving process with a cyclical pattern of loss [21]. For some adults with DM1 in the current study, participation restrictions appeared to be normalized. Since DM1 is a hereditary disorder with many members of the same family having the disease [5, 48] and disease awareness is known to be diminished in this population [49], the normalization process might rely on referents or individual models in the social network of adults with DM1 [50]. Normalization, however, could lead to the trivialization of important and possibly life-threatening episodes, such as falls or coughs caused by dysphagia. Boström et al. [18] found a similar insidious decline in participation and perception of restrictions as part of “normal” everyday life for people with various neuromuscular disorders, including DM1.
Insidious increases in restrictions along with more sedentary behaviors might lead to progressive deconditioning and involuntary muscle disuse, exacerbating progressive weakness over time. Recent advances in knowledge about the benefits of exercise training for adults with DM1 showed the potential to reverse deconditioning and disuse phenomena [51, 52]. More research is needed to clarify the impact of sedentary behaviors and exercise training on adults with DM1.
Multifactorial nature of occurrence of changes in participation
Although rarely described in the literature, some facilitators that enhanced participation of adults with DM1 were found among personal factors; most, however, were environmental factors. As in the present study, resilience was previously found to be an important factor that contributed to participation in DM1 [21, 28] and to community belonging in older adults [53]. Many barriers found in this study were discussed individually in previous research but were not all covered in one study. In line with the present results, Ladonna et al. [21] described premature aging affecting body image and interpersonal relationships as well as limited finances as restricting participation in recreation. A lack of understanding from relatives and the public [20, 21] and social stigmatization [28] faced by adults with DM1 were similar to the barriers identified in this study, which increased the risk of participation restrictions. Of note, the present study found that some adults with DM1 tended to socially self-isolate because of concern about being stigmatized. Nevertheless, other factors might contribute to progressive social isolation, such as phobic anxiety and lower self-esteem for most severe form of the disease [54], but they were not identified in this study.
This study highlighted a decline in participation over time influenced by personal and environmental factors. It is important to consider this when planning longitudinal studies or clinical trials exploring intervention efficacy. In fact, controlling for specific personal and environmental factors, especially comorbidities, living arrangement (adapted or not), use of technical aids, and social network size and quality, could be important when assessing outcomes in such studies.
Occurrence of participation changes was found to be multifactorial for adults with DM1, including via a potential syndemic interaction. Initially developed for transmissible diseases, the syndemic framework is increasingly used to understand complex non-communicable diseases, such as inflammatory arthritis [55] or type II diabetes [56, 57]. Potential recognition that medical and environmental problems cluster and interact in the DM1 population could lead to improved care. For example, it would increase focus on: 1) enhancing health professionals’ health promotion and disease prevention roles; 2) supporting a holistic nurse-led management of DM1 that could consider both medical and participation needs [58]; 3) adding allied healthcare professionals (e.g., special educators, kinesiologist, zootherapist) to interdisciplinary teams; or 4) adding macro-level interventions, such as community-based rehabilitation approaches that enable health professionals and stakeholders to build consistent interventions across health, education, livelihood, and social systems [59]. Further research examining the syndemic framework in the DM1 population is needed before recognizing a formal syndemic interaction.
Clinical practice implications
The results highlighted potential ways to optimize participation over time by refining the evaluation process and maximizing interventions by capitalizing on facilitators and reducing barriers. This study found a progression in participation restrictions for the same participation category (i.e., difficulty first, then need for technical aids, then need for human assistance). These results might help health professionals to
With redesigning accomplishment and the insidious increase in restrictions over time, adults with DM1 could benefit from health professionals’ support to ease the burden of making constant readjustments and grieving. For example,
As stigma appears to be a barrier to participation,
Strengths and limitations
To our knowledge, this is the first study to conduct an in-depth qualitative exploration with a holistic framework of changes in participation of adults with DM1 from the perspective of six cases informed by triads. Using the HDM-DCP framework helped to structure the main facilitators and barriers to participation over time and provided a holistic understanding of processes involved in participation restrictions. Nonetheless, like other qualitative studies, the inductive-deductive analytical approach could be subject to the researcher’s expectations about the framework, which might affect the credibility of the results to some extent. Rigor was ensured through data triangulation, extensive data collection, intra- and inter-case analyses, and monitoring analysis and interpretation [65]. Inclusion of only six cases based on a subsample from a longitudinal study, however, limited the transferability of the results. Using a maximum variation sampling strategy and describing the research context offset this limitation by ensuring diversity in the purposely selected cases. Adults with DM1 with shorter disease duration or without a relative or nurse case manager follow-up might be underrepresented. As this research was carried out within a nurse-led management setting, the importance of their role might be overrepresented, and another health professional management model that is sensible to medical and participation needs might have similar benefits on participation. Important facilitators and barriers to changes in participation pertaining to different profiles of adults with DM1 might have been missed. Although the interviews fostered a general understanding of changes in participation, this phenomenon was explored retrospectively, meaning that a potential recall bias existed. Given potential cognitive deficits, during the interviews with adults with DM1, a contextualization strategy was used to enhance participation recall over time. Data triangulation, a plurality of methods, and apparently reaching a data saturation point limited this bias and increased the credibility and plausibility of the study.
CONCLUSION
This study explored and explained short- and long-term changes in participation from the perspective of the people directly involved. A heterogeneous, slow and insidious decline in participation leading to redesigning accomplishment was found to be a core element in understanding the changes over time. This study also highlighted the multifactorial nature of participation changes, where a misfit between personal and environmental factors and potential syndemic interactions led to participation restrictions over time for adults with DM1 and their relatives. A better understanding of participation changes, as well as facilitators and barriers, supports the decision-making of adults with DM1, relatives and health professionals concerning disease management with a prognostic approach. These results open up new avenues for research on resilience, stigma, and syndemic interactions that exacerbate participation restrictions in adults with DM1. Further research is needed with a larger sample; it could also benefit from interviewing a younger cohort of adults with DM1 and including multiple follow-ups. Using more than one conceptual framework (e.g., syndemic framework or International Classification of Functioning, Disability and Health) to compare and contrast different interpretations may help to get a better understanding of the phenomenon. Since the global COVID-19 pandemic might have exacerbated the participation restrictions of people with DM1 and impacted their future, health professionals need to intervene to limit their social isolation. Focusing on delivering essential rehabilitation services that help to adapt participation, managing symptoms with telemedicine [66], and supporting the resilience process could be crucial strategies during and after the pandemic.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest related to the publication of this manuscript. CG received an honorarium for conference presentation, research funding and data sharing for preparation of a therapeutic trial from IONIS and Biogen Idec. All authors have approved the final article.
Footnotes
ACKNOWLEDGMENTS
We wish to thank all the participants who took the time to take part in this study as well as the outside members of the research team, Mélissa Lavoie (MLa), who reviewed the interview guides, and Marjolaine Tremblay (MT), who reviewed the interview guides, data analysis and interpretation. This work was supported by the Canadian Institutes of Health Research (CIHR) MOP-49556 and JNM-108412. Individual authors are supported by the Centre de recherche Charles-Le Moyne –Saguenay–Lac-Saint-Jean sur les innovations en santé (KR), the Fonds de recherche du Québec –Santé 30844 (KR), 31011 (CG) and 298996 (ML), and the CIHR 360880 (ML). Funding sources had no involvement in the conduct of the study or publication process.