
Abstract
Background:
In recent years, an increasing number of people adapt to a vegetarian, pescatarian or flexitarian dietary pattern that reduces the consumption of meat and fish. Although these dietary patterns have a risk for developing vitamin B12 deficiency associated polyneuropathy, it is unknown whether this risk is still increased when vitamin B12 levels are adequate.
Objective:
To examine whether a vegetarian, pescatarian or flexitarian dietary pattern is associated with an increased risk for idiopathic axonal polyneuropathy.
Methods:
We conducted a case-control study that included 256 idiopathic axonal polyneuropathy patients with adequate vitamin B12 blood levels and 630 controls. We used questionnaire data to determine the frequency of meat and fish consumption and defined dietary patterns.
Results:
The vegetarian (no meat or fish consumption) and the pescatarian (fish consumption, no meat consumption) dietary patterns showed no increased risk of axonal polyneuropathy. Frequency-effect analysis and quantity-effect analysis also did not show that a reduction of meat or fish consumption (flexitarian dietary pattern), either small or large, changed the risk of axonal polyneuropathy.
Conclusions:
We did not find an increased risk for axonal polyneuropathy among people with a vegetarian, pescatarian or flexitarian diet and an adequate vitamin B12 level.
INTRODUCTION
In recent years there is a trend to reduce the intake of meat and fish in the western world [1, 2]. Diets with no fish or meat consumption (vegetarian), with fish but without meat consumption (pescatarian) and with reduced meat consumption (flexitarian) appear to have a positive effect on body weight, risk of type 2 diabetes and metabolic health markers [2]. However, decreased meat and fish consumption can lead to a reduced intake of vitamin B12, which deficiency is an important factor in the development of axonal polyneuropathy [3, 4].
Axonal polyneuropathy is one of the most prevalent neurological conditions in clinical practice, with increasing incidence in the elder population [5]. Possible causal factors are, among others, diabetes mellitus, alcohol abuse and vitamin B12 deficiency. In about 25% of the patients the cause remains unknown [6]. This idiopathic axonal polyneuropathy probably does not represent a single disease entity, but encompasses multiple subgroups which are each associated with causal factors that have not been discovered yet.
Considering the present tendency to reduce the intake of fish and meat, patients diagnosed with idiopathic axonal polyneuropathy (by definition with an adequate vitamin B12 level in the blood) in our tertiary referral clinic frequently ask if these dietary habits had a contributive effect to the disease. To date no study had investigated this association.
We therefore conducted a large case-control study on idiopathic axonal polyneuropathy (with an adequate vitamin B12 level in the blood) and determined whether a vegetarian, pescatarian or flexitarian dietary pattern increases the risk for this form of polyneuropathy.
MATERIALS AND METHODS
Study design
A case-control study design was initiated in 2008 to investigate potential risk factors for idiopathic axonal polyneuropathy in the Netherlands, using multiple questionnaire data [7].
Participants
Patients with idiopathic axonal polyneuropathy were recruited from our outpatient clinic in a tertiary neuromuscular referral center in Utrecht, The Netherlands and fulfilled the clinical and nerve conduction study (NCS/EMG) criteria for idiopathic axonal polyneuropathy [7]. Thorough history taking, clinical examination, and extensive laboratory testing (including complete blood count, erythrocyte sedimentation rate, glucose, HbA1c, insulin, renal function, liver enzymes, creatine kinase, C-reactive protein, vitamin B1, vitamin B6, folic acid, vitamin B12, homocysteine, cholesterol, triglycerides, HDL cholesterol, LDL cholesterol, thyroid-stimulating hormone, serum and urine M-protein, and serological screening for celiac disease using total IgA level and IgA antibodies against tissue transglutaminase and endomysium) were performed, ruling out other causes of polyneuropathy. Patients with a vitamin B12 level below 130 pmol/l and patients with vitamin B12 levels between 130 and 300 pmol/l plus homocysteine levels above 15.0μmol/l were considered as vitamin B12 deficient [8] and were excluded.
Controls with a similar age and sex distribution as the patients were obtained from a case-control study on amyotrophic lateral sclerosis in The Netherlands [9]. In this study, participants noted their previous medical history. When polyneuropathy was present, controls were excluded. Controls with diabetes or average alcohol consumption above three units per day were also excluded, because these exclusion criteria (that were also used in our patient group) are important risk factors for the development of polyneuropathy.
Definitions of dietary patterns
To define the different dietary patterns we used the frequency of meat and fish servings during breakfast, lunch and dinner [10]. Vegetarianism was defined as consuming meat or fish less than one day per week on average. Pescatarianism was defined as consuming meat less than one day per week on average, but fish one or more days per week. Flexitarianism was defined as consuming meat one to five days per week. Regular consumption was defined by eating meat six or seven days per week.
Data collection
Patients and controls were asked to fill in a general questionnaire and a structured food-frequency questionnaire [11]. The food frequency questionnaire is a validated 199-item questionnaire, that is designed to collect all dietary intake during a one-month time period. Patients were instructed to recall their dietary intake during the month prior to the onset of symptoms. If this month was not representative for their dietary behavior at that time, the last representative month prior to symptom onset was used. The general questionnaire included questions about smoking, alcohol consumption, body metrics and education. Education was divided into 6 categories; the participants had to choose the highest level completed. Participants included their height and (premorbid) weight; BMI was calculated by dividing weight by the square of height. Participants stated whether they smoked and what their average alcohol intake was. Age for controls was the age they completed the questionnaire; for patients, it was the age at onset of symptoms.
In the food-frequency questionnaire, only completed questionnaires with no missing data could be analyzed. If necessary, we contacted patients to obtain missing data. With this approach, we acquired a questionnaire without missing data from 67% of the patients contacted to participate in this study. Total energy intake was calculated based on the data in the food-frequency questionnaire [12]. The frequency of meat and fish consumption during the warm meal was asked in separate questions where the possible answers were ordinal arranged (“none”, “one day per month”, “2-3 days per month”, “1 day per week”, “2-3 days per week”, “4-5 days per week”, “6-7 days per week”). The first three items were combined into one category (“< 1 day per week”). The amounts of servings (100 grams) for meat and fish during these days were acquired.
Data analysis
All statistical analyses were performed with the statistical software R version 3.6.0 (http://www.r-project.org/). Power calculations were performed using G*Power (V.3.1 Heinrich Heine Universitat Dusseldorf, Germany).
Baseline characteristics were compared between patients and controls with chi-squared statistics (ordinal and nominal variables) and Student’s t-tests or Mann-Whitney U-tests (continuous variables). The Kruskal-Wallis test was used to compare vitamin B12 levels between dietary patterns.
For each dietary pattern a logistic regression analysis was performed, corrected for age, sex and BMI (the minimal adjusted logistic regression) and corrected for age, sex, BMI, education, smoking, alcohol consumption, use of vitamin B12 supplements and total energy intake (the maximal adjusted logistic regression). For the logistic regression tests regarding the pescatarian diet, vegetarians were excluded from the reference group. For the logistic regression test regarding the flexitarian diet, vegetarians and pescatarians were excluded from the reference group. Frequency-effect analysis and quantity-effect analysis were performed using a multivariate logistic regression on an ordinal division of the variables (days meat and fish per week and kilograms meat and fish per month), with the lowest intake category as the reference category. Linear trends were determined by a logistic regression with the four categories as continuous variant. These regressions were adjusted for the same variables as in the maximal adjusted logistic regression analysis on dietary patterns.
Ethical statement
This study was approved by the Medical Ethics Committee on human experimentation of the UMC Utrecht. All participants gave written informed consent before inclusion.
RESULTS
In total 886 participants (256 idiopathic axonal polyneuropathy patients and 630 controls) were included in this study; their characteristics are outlined in Table 1. Only patients with adequate vitamin B12 levels were included, the levels of vitamin B12 in our patients were comparable between the different dietary patterns (P = 0.66).
Baseline characteristics
In the patient group, 4.3% consumed meat less than once per week and 46.1% consumed fish less than once per week. In the control group this was 4.0% and 45.1%, respectively. The proportions and absolute numbers of vegetarians, pescatarians and flexitarians in patients and controls are listed in Table 2. We conducted a logistic regression analysis adjusted for multiple covariates known to be associated with the risk of polyneuropathy and dietary patterns. The covariates and their distributions in the different dietary patterns are listed in Table 3. Due to the low numbers of some of the dietary patterns, we also analyzed the data using a minimal set of covariates, only adjusting for age at onset, sex and BMI, to prevent overfitting. Both these minimal and maximal adjusted logistic regression analyses did not show any significant increase the risk of idiopathic axonal polyneuropathy between the dietary patterns (Table 2).
Logistic regression analyses of dietary patterns with idiopathic axonal polyneuropathy
*Adjusted for age, sex, BMI. §Adjusted for age, sex, BMI, education, smoking, alcohol consumption, vitamin B12 supplement use and total caloric intake.
Characteristics of patients per dietary pattern
The frequency-effect analysis, assessing the effect of different frequencies of meat and fish consumption, and the quantity-effect analysis, assessing the effect of different amounts of meat and fish consumption, also did not show significant changes in the risk of idiopathic axonal polyneuropathy (Fig. 1).
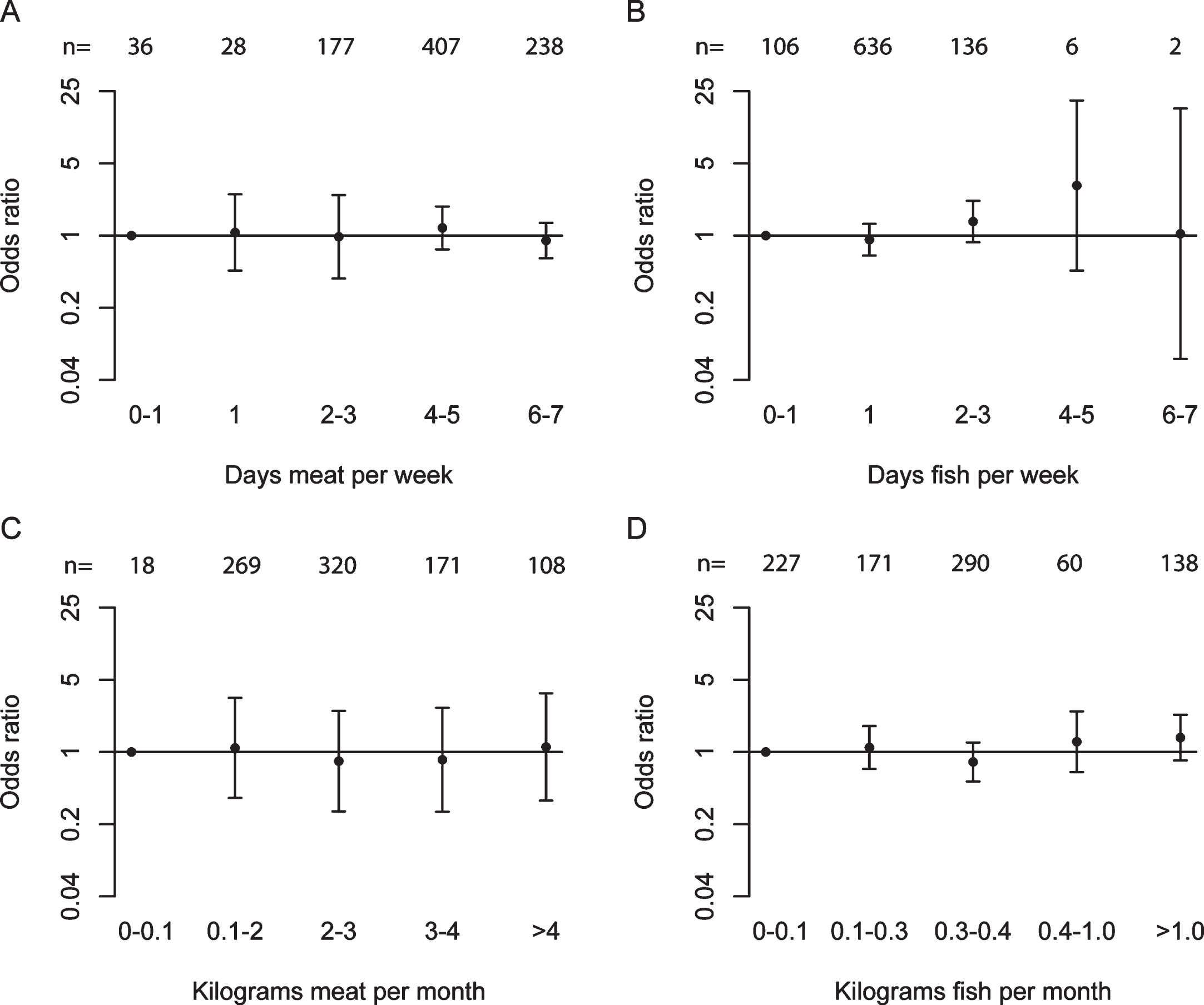
Maximal adjusted odds ratios for the association between idiopathic axonal polyneuropathy and ordinal categories. The total number of observations for each category (n) is depicted at the top. A) Frequency of meat consumption, linear trend P = 0.58; B) Frequency of dietary fish consumption, P = 0.20; C) Quantity of meat consumption, P = 0.91; D) Quantity of fish consumption, P = 0.10.
DISCUSSION
In this case-control study, we could not find an indication that a vegetarian or pescatarian dietary pattern had an increased risk for idiopathic axonal polyneuropathy. Also, a flexitarian diet, either with a small or large reduction of meat or fish intake, showed no increased risk.
The proportion of people with a vegetarian or pescatarian dietary pattern in our cohort (4.2%) was comparable to the reported prevalence in the adult population in the Netherlands (4–6%) [10, 13–15]. With this cohort we had sufficient power (one-sided alpha = 0.05, probability = 0.05, power = 0.8) to find an effect that we previously defined as clinically relevant (odds ratio≥2.0) [7]. Although we cannot rule out that there is a smaller effect for which this study has insufficient power, the clinical relevance of such a small effect is questionable.
A vegan dietary pattern could not be included in this study due to low prevalence in our cohort. The results of this study can therefore not be extended to this specific dietary pattern.
In this study, only homocysteine levels were available to exclude relative vitamin B12 deficiencies. Methylmalonic acid levels were not measured. In recent years it has been shown that methylmalonic acid is a more adequate marker for relative vitamin B12 deficiency, since homocysteine levels can be influenced by other factors (such as folate deficiency, age or kidney function) [16]. This results in a lower specificity of homocysteine compared to methylmalonic acid [17]. Due to this lower specificity, we might have excluded some patients that were not truly vitamin B12 deficient. Since the sensitivity of homocysteine is comparable to that of methymalonic acid, [17] no patients with a relative vitamin B12 deficiency were incorrectly included in this study. Thus, the absence of methylmalonic acid had no effect on the outcomes of this study, but it only reduced the power of this study. Nevertheless, we still included sufficient patients to achieve adequate power to answer our research question.
A disadvantage of case-control studies using questionnaire data is that this analysis is prone to recall bias. By blinding the participants for the research question, by including the relevant questions in an extensive questionnaire including many other topics, and by using indirect questions about meat and fish consumption instead of direct asking about a vegetarian, pescatarian or flexitarian diet, we aimed to reduce this bias. Another disadvantage could be that patients were asked to recall their dietary pattern from before the onset of symptoms. However, a vegetarian dietary pattern is often a specific lifestyle choice that people can recall even after a longer period of time, [18] which reduces recall errors. We therefore believe that we minimized the effects of recall bias.
Another possible disadvantage of this study is referral bias. Patients were all referred to a tertiary neuromuscular clinic. Compared to a population-based study in the Netherlands, [6] the patients in this cohort are younger (median age 58.5 vs 71 years). This might indicate a referral bias, since younger patients are probably more likely to be admitted to a tertiary referral center. The proportion of vegetarians and pescatarians in this study is comparable to the general population. Vegetarians and pescatarians are also probably not less likely to be referred to our center (which would result in a false negative outcome). Therefore, we believe the effect of referral bias on dietary patterns had no significant effect on the outcome of this study, although this could not be ruled out completely.
In conclusion, we found no indication that people with a reduced meat and/or fish intake and an adequate vitamin B12 level have an increased risk of polyneuropathy.
Footnotes
ACKNOWLEDGMENTS
This study is supported by the Prinses Beatrix Spierfonds (WAR 07-24).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.