
Abstract
Background:
Few studies have examined falls and their predictors in patients with amyotrophic lateral sclerosis (ALS).
Objective:
The aim of this study was to survey fall incidence and to identify variables predicting the presence or absence of falls occurring within 3 months after discharge of patients with ALS from hospital.
Methods:
The following variables were evaluated in 14 patients with ALS: timed up and go test (TUG), functional reach test, 10-m comfortable gait speed, single-leg stance time, manual muscle test (MMT) scores for the lower limb, total modified Ashworth scale score for the lower limbs, fear of falling, and pull test score. The primary outcome variable was the occurrence of a fall within 3 months after discharge. The fall rate was calculated based on fall record forms. The specific circumstances of each fall were also recorded. Univariate and multiple regression analyses were used to identify fall predictors.
Results:
Seven of the 14 ALS patients (50%) experienced a fall within 3 months. Five fallers reported experiencing a fall that had caused injury, and three reported experiencing a fall that had required a hospital visit. Univariate logistic regression analysis identified TUG time, gait speed and MMT of the ankle dorsiflexors as factors associated with falls (p = 0.02–0.04). Multiple linear regression analysis of fall numbers identified age and TUG time as predictor models (p = 0.03).
Conclusion:
TUG time and MMT of ankle dorsiflexors may help predict falls in ALS patients. Validation studies in larger cohorts are needed.
INTRODUCTION
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease that involves degeneration of the motor system at all levels [1]. In patients with typical ALS, the symptoms are primarily those of weakness [2]. This would be expected to cause declines in walking ability, and subsequent increases in the prevalence of falls [3]. However, although patients with neuromuscular diseases reportedly experience falls more often than healthy individuals [4], few studies have examined falls in ALS patients [5–7]. Dal Bello-Haas et al. reported that 46% of ALS patients in their study had experienced falls since the onset of ALS [5], and Miller et al. reported a fall incidence of 33.4% with frequent falls in ALS-related conditions [6]. In addition, Ganzini et al. reported that trauma and falls accounted for 24% of cases of pain in ALS patients [7]. Schell et al. showed that lower extremity muscle strength correlated negatively with the number of falls in the past 3 months in a cohort of 31 ALS patients [8]. Montes et al. reported that fall risk increased with increases in timed up and go test (TUG) time among ALS patients [9]. Measuring both muscle strength of the lower extremities and TUG may allow fall risk to be followed, but the characteristics of fall risks inferred from such linear associations remain unclear. For example, the difference between fallers and non-fallers remains unclear, and whether assessment at one point in time can predict future falls has not been determined.
Understanding the factors that contribute to falls in ALS patients and identifying criteria that can predict falls would enable better daily life guidance. The assessment of fall risk is generally based on walking ability, along with muscle strength, balance, and a history of falls. These variables may also be useful in ALS patients [10]. The search for predictors of falls in ALS patients using the generalized assessments mentioned in previous reports may reinforce the utility of these variables. The purpose of this study was therefore to identify variables predictive of the presence or absence of falls in ALS patients in the first 3 months after discharge from hospital. No previous reports have included investigation of the specific circumstances of falls, and identifying detailed preliminary data for fall cases may provide a useful basis for future fall research.
MATERIALS AND METHODS
Consecutive patients with ALS who underwent rehabilitation at National Higashi Saitama Hospital were recruited from July 2011 until May 2013. The inclusion criterion was a probable or definite diagnosis of ALS, as defined by the revised El Escorial criteria [11]. Patients were excluded if they: 1) had performed no daily ambulation within the preceding week (walking with the use of a walking aid was acceptable); 2) had not been told of the ALS diagnosis; or 3) showed severely decreased respiratory function (forced vital capacity < 50% of predicted value for age) or cognitive decline (Mini-Mental State Examination score < 24).
The study was approved by the ethics committee at National Higashi Saitama Hospital. This study was performed in accordance with the ethical standards as per the 2000 Declaration of Helsinki and the 2008 Declaration of Istanbul. All participants provided informed consent prior to inclusion in the study.
Potential predictors of fall risk
To minimize differences in all tests, data were collected by the same examiner within 3 days before discharge. Age, sex, site of onset (upper limb, lower limb, or bulbar), duration since the diagnosis of ALS, and ALS Functional Rating Scale Revised (ALSFRS-R) score [12] were extracted from patient medical records at admission. Information about history of falls and the use of walking aids was self-reported by patients.
The following measures were assessed: TUG time, functional reach test (FR), 10-m comfortable gait speed (CGS), single-leg stance (SLS) time, MMT scores for the lower limb (MMT-lower), modified Ashworth scale (MAS) score for the lower limb, fear of falling (FoF), and the pull test. Considering the influence of fatigue on participants with ALS [13], we applied best values instead of average values.
The TUG [14] is a test of basic functional mobility. Application of the TUG has also been reported in ALS patients [9]. The time taken to rise from an armchair, walk 3 m as fast as possible, cross a line on the floor, turn, walk back, and sit down on the armchair was measured. Participants who routinely used a walking aid such as a cane or brace were allowed to use this aid during the test. The TUG was performed twice and the fastest time was used in analyses.
The FR [15] measures forward reach distance from a standing position. The FR was performed twice and maximum FR distance was used in analyses. Participants who wore leg braces were allowed to wear these during the test. If FR could not be performed because the subject was unable to achieve the required start position, the FR distance was recorded as 0 cm.
To measure CGS [16], the participant was asked to walk at their usual pace. Gait speed was measured over the middle 10 m of a 14-m runway, to allow 2 m for acceleration and 2 m for deceleration. The time taken to complete the middle 10 m of the walkway was recorded with a digital stopwatch that was started when the first leg crossed a line marked on the floor with tape and stopped when the first leg crossed a second line marked 10 m away. The test was performed twice. Participants who routinely used a walking aid such as a cane or brace were allowed to use the aid during the measurement.
To measure SLS [17], the participant was in-structed to balance on one leg and stance time was measured using a digital stopwatch. The SLS was measured twice for each leg and the maximum time was used in the analysis. If patient could not stand on one leg, SLS was recorded as 0 s. The upper limit was taken as 60 s.
MMT-lower represented MMTs for hip flexion and extension, knee flexion and extension, and ankle dorsiflexion of the left and right limbs [18]. Left and right values were concatenated, so individual MMT scores ranged from 0 to 10. Furthermore, total MMT score summed up the five movements, and were thus distributed within the range of 0–50.
MAS [19] score was evaluated for the hip flexors and extensors, hip abductors and adductors, hip internal and external rotators, knee flexors and extensors, and ankle dorsiflexors and plantar flexors of each leg. A grade of 1 + was converted to 1.5 for analysis. The MAS score was taken as the total of scores for all 10 muscles groups from both legs, and this total score was used in analyses (range, 0–80).
FoF [20] has also been adopted as a fall predictor. FoF is quantified using a visual analog scale [21], with participant asked to indicate their FoF on a 100-mm line using the fingertips or a pen. The line was anchored on the left (0 mm) by ‘No fear of falling’ and on the right (100 mm) by ‘Very fearful of falling’. Distance of the mark from the left edge of the line was measured and used as the FoF (range, 0–100 mm).
The pull test was performed as described in the Unified Parkinson’s Disease Rating Scale [22]. To simplify scores, the examiner evaluated whether the patient fell.
Outcome variables
The primary outcome variable was the occurrence of a fall within 3 months after discharge. Fall occurrence was investigated prospectively. A follow-up period of 3 months was defined in accordance with previous studies [23]. At discharge from hospital, participants or their families were provided with fall record forms. They were contacted by letter and asked to return the completed fall record forms every month from discharge up to 3 months after discharge. If fall record forms were not returned, the participant was contacted by telephone.
Participants filled out a separate form for each fall and were required to fill out a form at the time of the fall. Fall record forms asked for the following information: fall date; brief description of the fall; location of the fall; any injury or need for hospitalization resulting from the fall; and any walking aid used at the time of the fall. We counted the total number of falls experienced in the 3-month period for each participant. For fallers, the fall situation was reflected in the result. A fall was defined as “falling down to the ground, or to a lower level, against one’s will”, as described by Gibson [24].
Statistical analysis
Participants were classed as fallers if they reported one or more falls during the 3-month follow-up period, and as non-fallers if they reported no falls during the 3-month follow-up period. The proportion of fallers was calculated and used as an indicator of fall incidence.
Each variable was compared between fallers and non-fallers in univariate logistic regression analyses, and unadjusted odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated. To extract predictors of numbers of fall, single and multiple linear regression analyses were performed with the number of falls as the dependent variable. Multiple regression analysis was performed with stepwise selection by including age, ALSFRS-R and variables showing values of P < 0.10 from single regression analyses.
Statistical processing was performed using JMP version 10.0-J statistical analysis software, and the level of significance was set at 0.05. Data were summarized as mean and standard deviation for continuous outcomes, and frequency and percentage for categorical variables.
RESULTS
This study recruited 15 patients and analyzed 14 participants after excluding 1 patient who had been non-ambulatory at all surveys up to 3 months after discharge (Fig. 1). Participant characteristics are shown in Table 1. No participants required acute treatment and all were hospitalized for evaluation of medical conditions or to obtain a second opinion.
All 14 patients completed the follow-up survey (response rate, 100%). Seven patients reported at least one fall within 3 months and were classified as fallers, while the seven patients who reported no falls within 3 months were classified as non-fallers. Fall incidence was therefore 50%. The total number of falls was 15. Five fallers (71.4%) reported multiple falls. In addition, 5 fallers (71.4%) reported experiencing at least one fall that had caused injury, and three (42.9%) reported experiencing at least one fall that had required a hospital visit. Fall results are shown in Table 2. Falls occurred not only while walking, but also while standing up and reaching. Falls occurred across a range of times, from early morning to midnight.
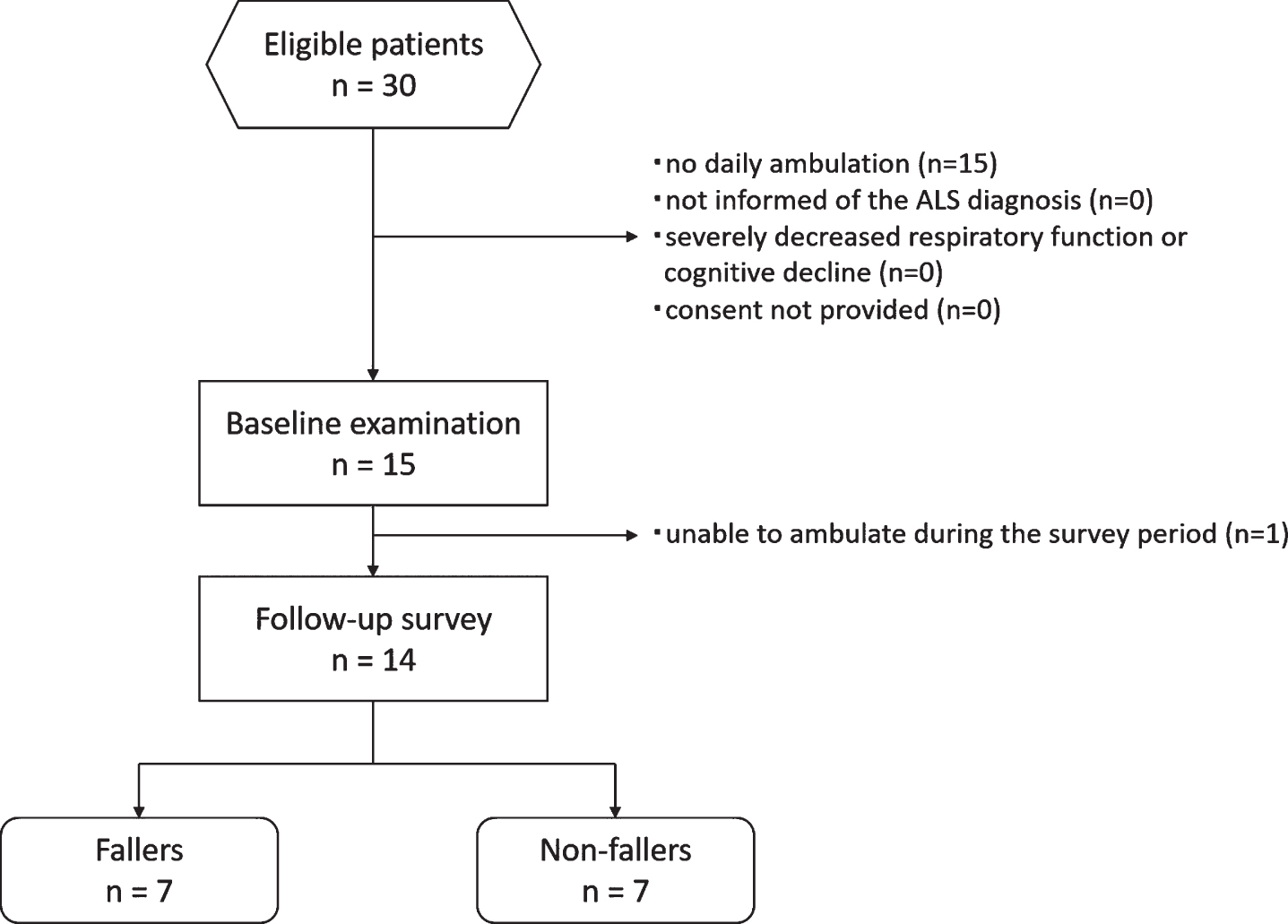
Flow chart of participant recruitment.
Participant characteristics
Abbreviations: ALSFRS-R, amyotrophic lateral sclerosis functional rating scale –revised; AFO, ankle foot orthosis. *Site of onset was classified as upper limb (UL), lower limb (LL), or bulbar (B).
Fall survey results
Missing items are marked as not known. Subjects 1, 2, 7, 10, 11, 13, and 14 experienced no falls during the 3-month period.
Table 3 shows the results of univariate logistic regression analysis to identify differences between fallers and non-fallers. TUG time, CGS and MMT for ankle dorsiflexors showed significant relationships as explanatory variables in univariate analyses with presence or absence of falls after 3 months as the objective variable. For the results of multiple regression analysis with the number of falls as the outcome, age, TUG, and MMT ankle dorsiflexion were selected as significant models (p = 0.038) (Table 4). The adjusted R2 of the model was 0.41. Age and TUG correlated independently with the number of falls, but MMT ankle dorsiflexion did not show an independent association (p = 0.18).
Univariate logistic regression models for predicting falls in ALS patients
ALSFRS-R, amyotrophic lateral sclerosis functional rating scale- revised total score; TUG, timed up and go test; FR, functional reach; CGS, comfortable gait speed; SLS, single-leg stance time; MMT, manual muscle test; FoF, fear of falling. Site of disease onset was classified as upper limb (UL), lower limb (LL), or bulbar (B). Continuous variables are represented as mean (SD) and categorical variables as n (%). *p < 0.05
Single and multiple linear regression models for predicting fall numbers in ALS patients
ALSFRS-R, amyotrophic lateral sclerosis functional rating scale-revised total score; TUG, timed up and go test; FR, functional reach; CGS, comfortable gait speed; SLS, single-leg stance time; MMT, manual muscle test; FoF, fear of falling.
DISCUSSION
In this study, both TUG time and ankle dorsiflexor strength showed potential clinical utility as predictors for the occurrence of future falls. Furthermore, TUG was shown to be potentially useful in predicting the number of falls. The results of this preliminary experiment demonstrate the potential of using functional tests to predict short-term falls and highlight the need for future studies generalized to larger samples.
The results showed that 50% of community-dwelling ALS patients experienced falls within a 3-month period. A previous retrospective study of 12 patients with motor neuron disease reported that 33% experienced a fall over a 100-day period [4], while a longitudinal study of 234 ALS patients reported that 46% experienced a fall over the 2-year study period [5], and a study of 1707 ALS patients in the ALS Patient Care Database reported that 33.4% had experienced a fall at enrollment [6]. Previous studies have used varying study periods and methods, and have included patients who were not walking regularly in daily life. This precludes simple comparison of results between previous studies. The present study only included ALS patients who were walking on a daily basis, which may have led to a higher incidence of falls. In this study, we asked patients to describe the fall situation, and our results indicate that falls occurred for a variety of reasons and situations. The possibility of a fall should be considered in all situations. Patients and caregivers should thus be guided to consider these characteristics of falls in ALS patients.
The result of this study indicated that TUG time and MMT for ankle dorsiflexors might be related to falls in ALS patients. TUG time has previously been reported as a fall predictor for various populations [9, 26]. Axer et al. listed the retropulsion test, velocity of gait, ‘get up and go’ test, and single-leg balance test as standard rating scales to evaluate fall risk in patients with neurological diseases [25]. Thurman et al. reported TUG time as useful for predicting falls in patients with neurological conditions [10]. Montes et al. reported that fall risk was associated with TUG time using generalized linear mixed-effects models, with a TUG time of 14 s indicating a 10% chance of falling in ALS patients [9]. Our exploratory results from a broad functional assessment also support previous reports showing the utility of TUG.
Declines in MMT for ankle dorsiflexors also seem to have potential for fall prediction. Ankle dorsiflexor muscle force has been previously reported to tend to decrease compared to the proximal muscles in ALS [27]. Weakness of the ankle dorsiflexors is associated with gait function [28]. Decreased strength of the ankle dorsiflexors is thought to lead to drop foot during walking and increased fall risk [10, 30]. However, no reports have yet clarified the relationship between ankle dorsiflexion muscle force and falls in ALS patients [31]. The reduced swing leg capacity due to drop foot might potentially increase the risk of falling, although functional walking levels seem to be maintained. Overall lower extremity muscle strength was not associated with future falls. This is inconsistent with the report of Schell et al. [8], but may be due to differences between past and future falls. In addition, the present results showed that fall history and FoF were not significantly associated with future falls. In general, a history of falls is a well-established predictor of falls [10], but our results suggest that the absence of a history of falls in ALS does not simply translate to a low risk of future falls. Given the rapid progression of functional decline in ALS, we believe that prospective prediction of falls, including periodic functional testing, is likely to prove effective.
One strength of the present study was that it represents the first study to investigate many fall predictors in ALS patients. The significance of our research is that the fall situation and part of the fall factor, which had been unclear in ALS patients, were identified. The present results provide pilot data to clarify factors associated with and predictive of falls among individual with ALS. In the future, if patients at risk of falls can be easily identified in clinics, prevention of unnecessary fall events may be achievable through education for patients. This may affect the timing of prescriptions for walking aids and other devices. Disuse muscle weakness in ALS patients may be preventable with physical therapy interventions [32]. Attention to orthotic support for dorsiflexors or prevention of disuse muscle weakness may thus be helpful in preventing falls.
Some limitations of this study should also be noted. First, the study was conducted at only one institution. Second, the subject cohort was small, and some variables may have failed to show significant differences between groups due to type II error because of the small sample size. Finally, ALS participants in this study may have shown relatively slow disease progression, because mean ALSFRS-R was relatively good compared to the mean duration of disease. The results of this study should thus be interpreted with caution. For future research aimed at minimizing falls among patients with ALS, falls need to be investigated in an expanded population and fall predictors must be validated.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.