
Abstract
Background:
Duchenne muscular dystrophy (DMD) is an X-linked recessive genetic disorder, that is characterized by progressive muscle degeneration and loss of ambulation between 7–13 years of age. Novel pharmacological agents targeting the genetic defects and disease mechanisms are becoming available; however, corticosteroid (CS) therapy remains the standard of care.
Objective:
The purpose of this longitudinal study was to elucidate the effect of CS therapy on the rate of muscle strength and gross motor skill decline in boys with DMD and assess the sensitivity of selected outcome measures.
Methods:
Eighty-four ambulatory boys with DMD (49–180 months), 70 on CS, 14 corticosteroid naïve (NCS), participated in this 8-year multi-site study. Outcomes included; isokinetic dynamometry, the Standing (STD) and Walking/Running/jumping (WRJ) dimensions of the Gross Motor Function Measure (GMFM), and Timed Function Tests (TFTs). Nonlinear mixed modeling procedures determined the rate of change with age and the influence of steroids.
Results:
Despite CS therapy the rate of decline in strength with age was significant in all muscle groups assessed. CS therapy significantly slowed decline in knee extensor strength, as the NCS group declined at 3x the rate of the CS group. Concurrently, WRJ skills declined in the NCS group at twice the rate of the CS group. 4-stair climb and 10 meter walk/run performance was superior in the boys on CS therapy.
Conclusion:
CS therapy slowed the rate of muscle strength decline and afforded longer retention of select gross motor skills in boys on CS compared to boys who were NCS. Isokinetic dynamometry, Walk/Run/Jump skills, and select TFTs may prove informative in assessing the efficacy of new therapeutics in ambulatory boys with DMD.
INTRODUCTION
Duchenne muscular dystrophy (DMD) is an X-linked recessive genetic disorder that is due to a mutation in the dystrophin gene. The severe reduction or absence of dystrophin [1], an important structural component of muscle tissue, leads to contraction-induced injury to the sarcolemmal membrane, and activation of a cascade of inflammatory pathways leading to fiber necrosis, fibrosis, and impaired fiber regeneration. Progressive muscle deterioration results in delayed acquisition, and subsequent loss of motor skills, with cessation of ambulation typically between 7–13 years of age without corticosteroid treatment, and 2–3 years later with corticoste-roids [2].
Although novel pharmacological agents targeting the genetic defect and mechanisms of the disease process continue to be developed, a curative treatment does not exist and incurred muscle damage cannot be reversed. Corticosteroid therapy, which delays muscle deterioration, remains the standard of care despite adverse side effects that potentially impact quality of life [3, 4]. It has been recognized that corticosteroid therapy has altered disease progression in boys with DMD, decelerating the loss of muscle strength and providing a longer period of time over which functional abilities are retained [5–10]. Slowing the rate of disease progression has expanded the age range for assessing the efficacy of new therapeutics, allowing the participation of older boys in clinical trials, and accentuated the need to expand the repertoire of outcome measures across different phases of the disease process.
The purpose of this 8 year prospective study (NCT00312247) was to further our understanding of disease progression in boys with DMD receiving corticosteroids using quantitative outcome measures (three-dimensional motion analysis, community based step activity monitoring, energy consumption, isokinetic dynamometry), functional motor outcomes (gross motor skills, timed functional tests) and patient reported outcomes (PROs). It was hypothesized that the selected outcomes would be responsive to declines in muscle strength and the impact on ambulatory function. This paper will not report on motion analysis [11], community based step activity monitoring [12], energy consumption (accepted Gait and Posture), or PROs [13]; rather will present the results of longitudinal assessment of quantitative muscle strength, functional motor skills, and timed functional tests.
MATERIALS AND METHODS
Eighty-five ambulatory boys with DMD (mean age 93 months, range 49–180 months at baseline) were recruited into this multi-site study from 2006–2014 from the DMD clinics of three pediatric hospitals. Participants were assessed yearly for the first 4 years of the study and every 6 months for the following 4 years. Participants were followed until cessation of ambulation or end of study in 2014. One boy was removed from analysis due to confirmation of Becker muscular dystrophy secondary to genetic testing, initially deemed unnecessary by parent secondary to sibling with diagnosis of DMD. Of the 84 participants, 70 participants received corticosteroid therapy (CS), while 14 remained corticosteroid naïve (NCS) (Table 1). All participants on corticosteroid therapy at any time for ≥1 month during duration of the study were allocated to the CS group for data analysis to control for possible influence of CS on motor performance, and MRI confirmation of altered muscle tissue 3 months following initiation of CS [14]. At baseline time on corticosteroids ranged from 1–70 months, with a mean of 16 months for total group. Whether boys received corticosteroid therapy was dependent upon family preference with the guidance of the participant’s local physician. Boys were treated with Prednisone or Deflazacort, as determined by parent and clinician preference. Target doses of 0.75 mg/kg for prednisone or 0.95 mg/kg for Deflazacort were desired on a daily schedule. Due to behavioral or weight gain issues doses were modified to lower levels, or a weekend only dosage regimen, upon parental request. Compliance with dosage recommendations were not systematically monitored. Corticosteroid therapy was continued at cessation of ambulation, unless family requested discontinuation.
Group demographics
All study participants/parents signed informed assents and consents approved by local Institutional Review Boards. Study inclusion criteria included: 1) male, 2) a diagnosis of DMD as determined by clinical evaluation by a team experience with DMD (abnormal gait, Gower’s sign, calf hypertrophy, etc.) 3) one or more of the following: documentation of disease-causing mutation in the dystrophin gene, elevated serum creatine kinase levels, and a family history of an affected relative with either a disease-causing mutation in the dytrophin gene and/or complete dystrophin deficiency as shown by immunostaining on muscle biopsy, 4) four years of age or older, 5) ability to walk independently at self-selected speed for 10 minutes, 6) ability to cognitively understand directions for testing procedures. Assessments were completed in one three-hour visit when feasible, or two consecutive days. The order of assessments, instructions provided were standardized, and evaluators held constant per site. All evaluators had > 5 years pediatric orthopedic experience and were familiar with all assessments prior to study onset. Intraclass correlation coefficients (ICC) for interrater and intrarater reliability were 0.97–0.99 for the GMFM dimensions [15, 16], and > 0.91 for timed tests [17], consistent with the published literature. All investigators and evaluators met prior to study onset and yearly for the duration of the study for protocol review to ensure procedure standardization and reliability were maintained.
Outcome measures
Quantitative volitional muscle strength
Quantitative muscle testing has been reported to be reliable and precise, thus preferable for clinical trials [18, 19]. In this study volitional muscle strength was quantified using the Biodex System 3 Pro isokinetic dynamometer. Muscle groups were assessed unilaterally (based on hand dominance), as prior investigation has reported comparable strength bilaterally in boys with DMD [20, 21]. Isometric hip flexor strength was assessed in supine at 45° hip flexion, extensor strength at 85° hip flexion. Isometric knee flexor strength was assessed in sitting at 30° knee flexion, extensor strength at 90° knee flexion. The isometric testing protocol for hip and knee consisted of three five-second contractions performed consecutively by each muscle group, 10 second rests between contractions. Isometric ankle dorsiflexion/plantarflexion were assessed in semi-reclined sitting with the ankle in 0–5° of plantarflexion. If ankle contractures of > 5° of plantarflexion developed and participant could not be positioned comfortably in the Biodex footplate attachment, assessment of the ankle was discontinued. The isometric ankle protocol consisted of three five-second contractions, alternating plantarflexion and dorsiflexion, with 10 second rest between each contraction. Isokinetic testing about the knee was included in order to allow for examination of changes in muscle strength during two different types of muscle contraction. Isokinetic concentric knee flexor/extensor strength was assessed at 60°/sec, consisting of three consecutive repetitions through the full volitional range. Participants were passively moved through the desired motion to ensure understanding and given a practice session prior to onset of each testing procedure. Verbal coaching and visual feedback (computer screen) were used to elicit maximum torque during all contractions. The peak torque (Nm) per muscle group, normalized by body weight (kg) was used in the analysis.
Functional motor skills
At the inception of this study disease-specific outcome measure such as the North Star Ambulatory Assessment (NSAA) [22] and Motor Function Measure-32 (MFM-32) [23] were newly developed and unfamiliar to study researchers. Thus, the Gross Motor Function Measure (GMFM), which consists of skills mastered by typically developing (TD) children by 5 years of age, and reflects alterations in skill acquisition due to motor deficits, was used to assess functional ambulatory skills [15]. Although the GMFM was developed for children with cerebral palsy, it has been reported to be a reliable and valid assessment of change in children with Downs Syndrome as well as pediatric onset neuromuscular disease such as Spinal Muscular Atrophy (SMA) [15, 25]. The GMFM is a listed clinical outcome for DMD/BMD by the National Institute of Neurological Disorders and Stroke (commondataelements.ninds.nih.gov), Outcomes and Endpoints Summary. The skills included in the Standing (STD) (13 items) and Walking/Running/Jumping (WRJ) (24 items) dimensions were utilized in this study [15]. Dimension point score sums were used in the analysis.
Timed Function Tests
Timed function tests (TFTs) [26] have been recognized as practical and reliable measures of disease progression in DMD and have the potential to inform therapeutic development [27, 28]. In this study four TFTs were assessed in the following order and included; 10-meter walk/run, sit to stand, supine to stand, and 4-stair climb. Subjects were instructed to complete all measures as quickly as possible. Subjects wore comfortable walking shoes for all TFTs. The time (seconds) to complete the TFTs was recorded. Recently the use of TFTs time allowances (30–45 second cut-offs) have been instituted and the calculation of velocities (reciprocal of the time) preferred for analysis as representative of linear pattern of decline and maturational effects [29]. Utilizing the 45 second cut-off for performance resulted in 3 data points being removed for the TFT of supine to stand for 3 participants in CS group. Velocities were calculated and used as units for analysis of group comparison. Analysis of total group were performed using seconds as the unit of measurement.
Analysis
Nonlinear mixed modeling (NLMIXED) procedures were used to develop exponential growth curve models [30]. Growth curve models have become an increasingly powerful method of approaching longitudinal data analysis in the developmental sciences. Current approaches to growth modeling are highly flexible in terms of inclusion of the complexities often encountered in developmental research (missing data, unequally spaced time points, non-normal distributions, etc.) [31] The application of this approach provides a method of estimating between-person differences in within-person change and promotes a better understanding of individual differences in developmental change and responsiveness to therapeutic interventions [31–33]. In this analysis the change in outcome per month was the defined unit across time in which data points were available.
In the base model, exponential trends, γ o · e γ1·age for the full sample (N = 84) were examined. Age (months) was centered around the baseline mean, providing an interpretation of the intercept as the predicted value for the subject at baseline. Each mixed model had a random intercept (values varying across participants), but growth parameters were fixed. Estimates of residual and intercept variance were also obtained, representing the random effects of the within- and between-person variance, respectively. A successive model included a group×rate interaction to determine whether there was a significant difference in rate between the CS and NCS groups on the study outcome measures. Group and rate parameters also were as lower-order effects in the models. The model equation was γ00 + γ01 drug · e γ01·age+γ11·age.drug, N = 84. To allow for examination of group contributions to significant group×rate interactions, each group’s rate of change value was examined and tested for significance [34]. As it was anticipated boys in the NCS group would tend to lose strength and functional ability earlier than those on CS, the model was retested with the age variable centered around 120 months and the group variable centered around its average value. This approach (i.e., Johnson-Neyman technique [34]) allowed for comparison of outcome measure scores at a stage of the disease process that the two groups would be anticipated to be diverging.
RESULTS
Quantitative volitional muscle strength
Longitudinal analysis of the total group revealed that isometric muscle strength declined, indicated by a negative rate of change, with age at a significant rate in all the muscle groups (p≤0.002). Isokinetic concentric strength of the knee extensors and flexors declined as well; however, only the decrement in knee extensors was significant (p < 0.0001). Between subject variance was significant (p≤0.0001) for all muscle group and contraction types, with concentric knee flexor strength being the only exception (p = 0.115) (Table 2, Supplementary Figure 1).
Total cohort means at baseline (intercept), rate of change, and between subject variance
Est-estimated, CI-confidence interval, Nm/kg-Newton meters per kilogram, * statistical significance p < 0.05, negative rate of change indicates a decrease in value, positive indicates an increase value, con-concentric
When the group parameter was added to the model, no significant main effect for group was found; however, significant interaction effects were seen for knee extensor strength (isometric p < 0.0001, isokinetic concentric p = 0.0006) and ankle plantarflexor strength (p < 0.004), indicating a significant difference in the rate of muscle strength decline with age between the two groups. (Table 3, Fig. 1). Examination of the rate of decline in muscle group strength, per treatment group revealed that the rate of decline in knee extensor strength was 3x greater in the NCS group than the CS group. Ankle plantarflexor/dorsiflexor strength declined at a significant rate in the CS group, in contrast to the NCS group in which plantarflexor strength was increasing and dorsiflexor strength was decreasing but not significantly. (Table 3) (Fig. 1). In order to determine whether corticosteroid influence may be more apparent in older boys the model was rerun with the age variable centered on 120 months (10 years); however, no difference was seen in the analysis outcome. (Supplementary Table 2).
Per group mean at baseline (intercept), between group mean difference, rate of change, and interaction effects
Est-estimated, CI-confidence interval, Nm/kg –Newton meters per kilogram, NCS-Corticosteroid Naive, CS-Corticosteroid, * statistical significance p < 0.05, negative rate of change indicates a decrease in value, con-concentric, m/s-meters per second.
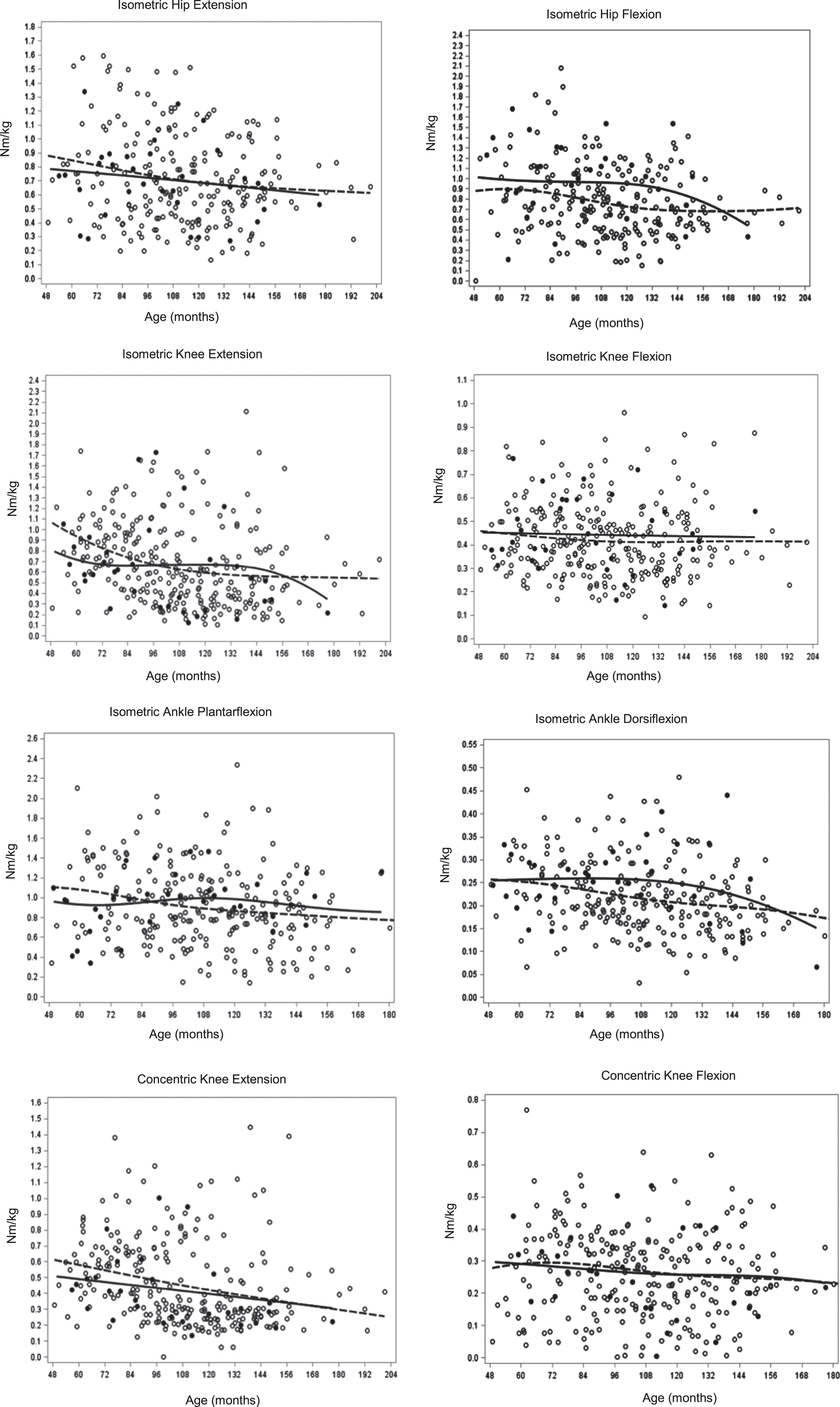
Muscle group strength change with age per group. (dashed line-CS, solid line-NCS).
Functional motor skills
For both the STD and the WRJ dimensions of the GMFM motor skills declined significantly (p < 0.0001), indicated by a negative rate of change, with increasing age for the total group (Table 2, Supplementary Figure 2). Between subject variance was also significant (p < 0.0001) for both dimensions, indicating variation in skill ability between subjects. There was no significant main effect for group for the GMFM dimensions (Table 3) (Fig. 2); however, a significant group x rate interaction effect was seen for the WRJ dimension (p = 0.004) indicating the groups were diverging in WRJ skill ability as they aged. Comparison of the rate of change of the two groups for the STD and WRJ dimensions revealed the NCS group lost skills at a rate 2x that of the CS group, although only the WRJ dimension reached significance. Centering of the age parameter at 120 months (10 years) did not alter previous findings (Supplementary Table 2).
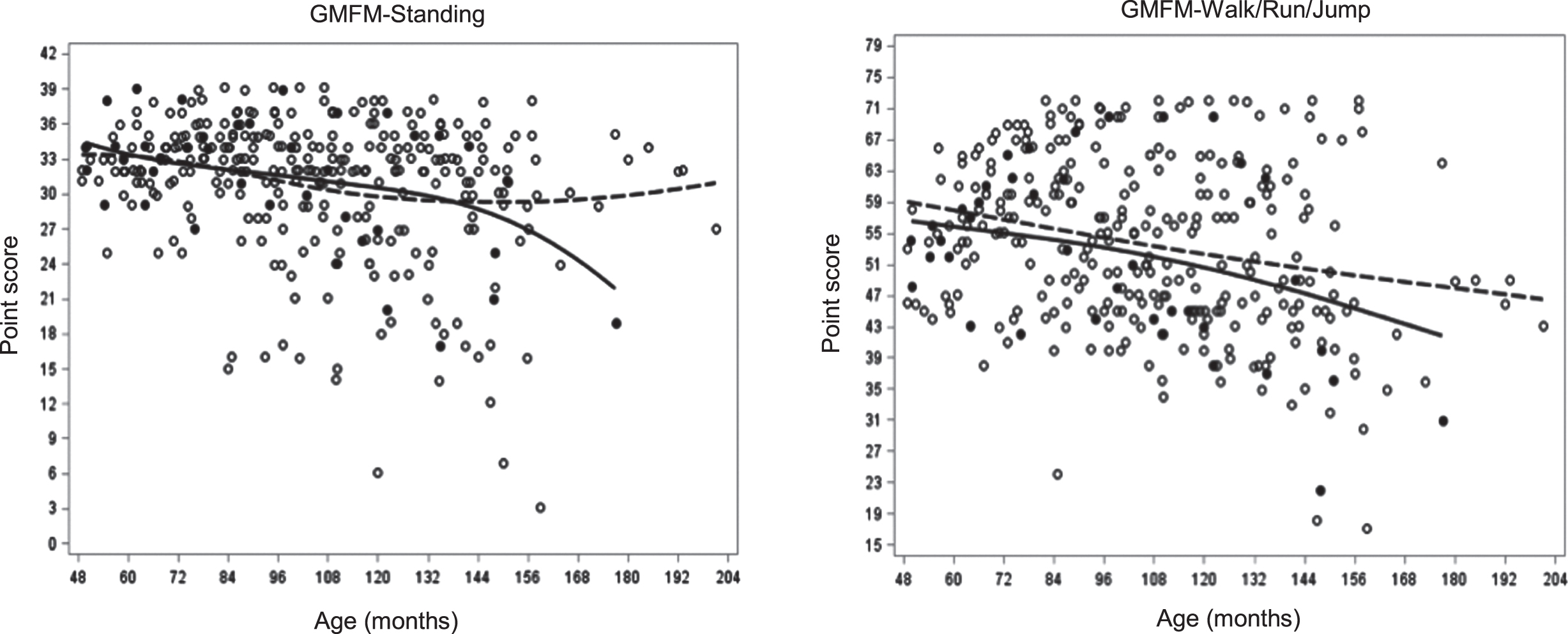
GMFM Dimension change with age per group. (dashed line-CS, solid line-NCS).
Timed function tests
The four TFTs of 10-meter walk/run, sit to stand, supine to stand, and 4-stair climb all demonstrated a significant (p < 0.0001) positive rate of change with age for the total group, indicating the length of time required to perform each of the TFTs was increasing, thus it was taking longer to perform the task (Table 2, Supplementary Figure 3). Between subject variance was significant (p < 0.0001) for three of the four TFTs, with sit to stand being the exception, indicating this TFT was least likely to reveal variations in motor capability. No significant main effect of group was seen for the TFTs when 45 second performance time and velocity units were used for analysis; however, a significant group x rate interaction effect was seen for the TFTs of 10-meter walk/run (p = 0.02) and 4-stair climb (p = 0.003) (Table 3). A comparison of the rates of change for these TFTs between the two groups revealed the velocity of the NCS group was decreasing at 2-3x the rate of the CS group. Although qualitative assessment of TFT performance was not included in this study it was observed that participant performance attributes changed across time with movement strategies adapted in attempts to maximize performance speed with decreasing strength. Stair climbing afforded a number of alternative upper (rail use) and lower limb strategies (alternative vs step to patterns), which most likely contributed to its responsiveness as an outcome. Centering of the age parameter at 120 months (10 years) did not significantly alter findings (Supplementary Table 2).
DISCUSSION
Quantitative volitional motor strength
Prior to the widespread use of corticosteroid therapy, the muscle strength of boys with DMD was reported to be significantly less than age-matched controls by 5 years of age [20, 35], decline linearly until 13 years of age, with the rate of decrement slowing early in the second decade [7]. Deterioration was reported to be greater in proximal muscle groups, specifically in the hip and knee extensors. In this study, isokinetic dynamometry revealed muscle strength is declining at a significant rate across time (4–17 years of age), with the rate of decline greatest in knee extensors, followed by hip extensors, with or without corticosteroid therapy. Interestingly, the impact of CS on the preservation of muscle strength did appear to be muscle group dependent and may reflect differential patterns of muscle involvement. Hip extensor isometric strength declined faster than flexor strength; however, the rate of decline in both muscle groups was comparable between the participant groups. A notable preservation of isometric and concentric knee extensor strength, and to a lesser degree knee flexor strength, was seen in those on CS therapy. Conversely, muscle strength about the ankle was declining significantly in the boys on CS therapy only. A previous investigation utilizing isokinetic dynamometry to assess muscle strength in ambulatory boys with DMD on corticosteroid therapy reported gains in strength prior to 7.5 years of age, with decrements occurring thereafter, suggesting corticosteroid efficacy may be greatest early in disease process, as the reduction of the inflammatory processes preserves contractile muscle tissue [4]. While the mean age at baseline in this study was 7.75 years, examination of boys < 7.5 years on corticosteroids confirmed 41% gained strength in the first year of the study; however, this indicates that greater than 50% of the boys less than 7.5 were losing strength in lower limb muscle groups.
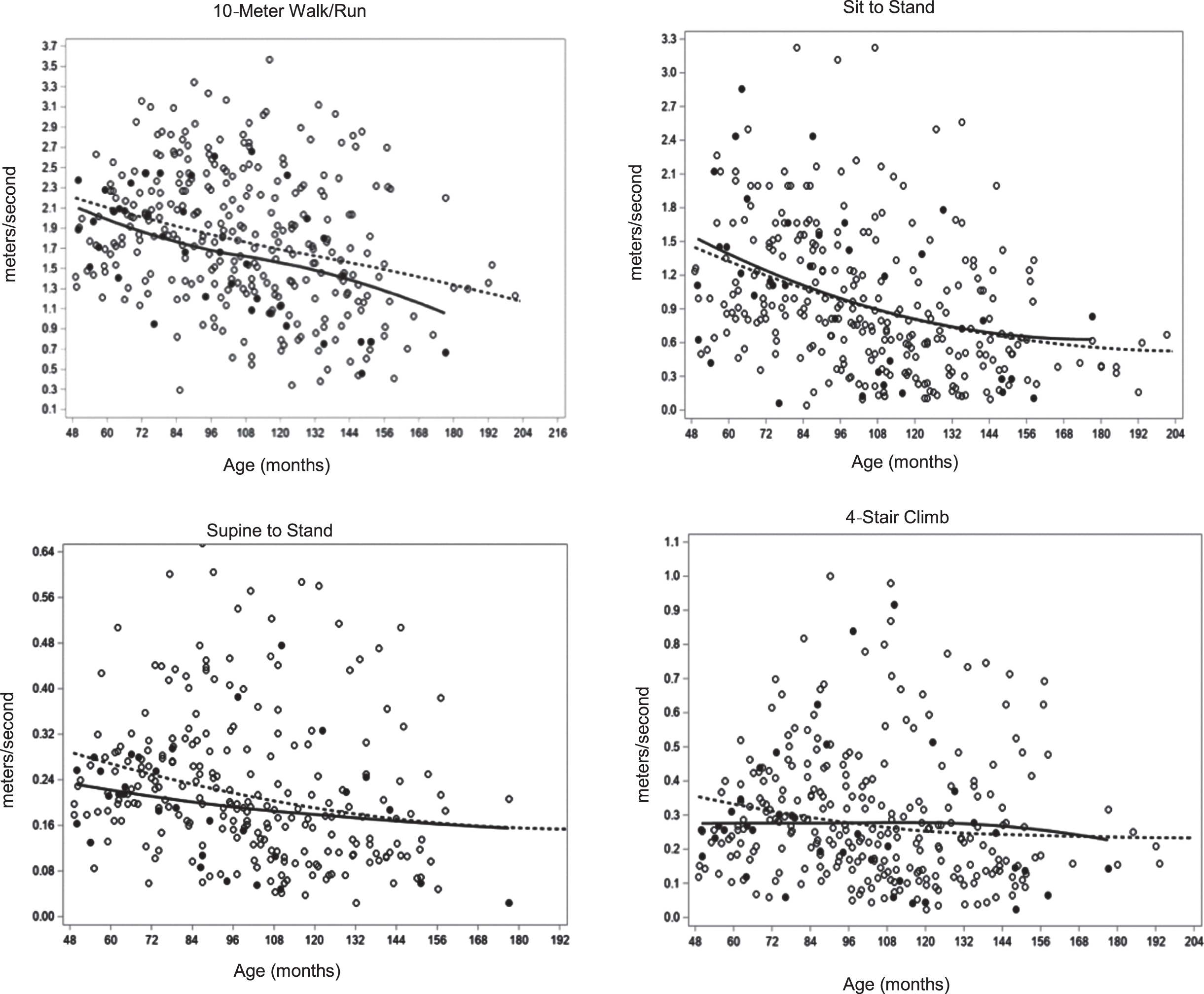
TFTs change with age per group. (dashed line-CS, solid line-NCS).
Previous studies that have combined quantitative strength assessment and magnetic resonance imaging (MRI) have provided insight into the intramuscular changes that occur in the absence of dystrophin and the loss of muscle strength with age [36–40]. Two discrete pathological processes, progressive fatty infiltration and alterations in muscle volume have been identified, with differences noted in the how muscle groups are affected over time [41]. While the relationship between pathological changes in muscle tissue and torque production are not well understood, both are seen in boys with DMD at a young age (4–5 years) [42], with progressive deterioration earlier and more pronounced in proximal leg muscle groups, such quadriceps, than in distal muscle groups [37, 41]. Isometric muscle strength in lower limbs normally increases with age; however, in a cohort of boys with DMD 8-14 years only the gastrocnemius and tibialis anterior were found to increase in strength with age. MRI results confirmed the cross sectional area (CSA) of the tibialis anterior was comparable to controls and although muscle hypertrophy was present in the gastrocnemius, its contractile CSA was comparable to norms [41]. These findings may elucidate the divergence in distal muscle group decline seen between boys on corticosteroids and those who were naïve in this study. Distal muscle groups are impacted later in the disease process and due to the unequal group size in this study, a larger percentage of older boys in the CS group could contribute to this finding, as well as possibility of less severe disease in the NCS group.
Recent investigation has suggested that in addition to the heterogeneous pattern of involvement across different muscles, variation is also seen within the length of the muscle with greater disease visible near the myotendinous junctions and that these changes relate to ability [43].
Muscle contraction force generation is known to vary with contraction type with eccentric providing greatest force, followed by isometric and concentric. In this study concentric force generation was less than isometric indicating this relationship remains intact in boys with DMD. While most quantitative studies of muscle strength have focused on isometric contraction due ease of application, alterations in concentric force production may be more informative in that force production can be assessed with changes in muscle length.
Muscle imaging and quantitative muscle testing have identified pathological changes in muscle tissue and the resultant loss of functional strength; however, further investigation is needed to better understand the heterogeneity of intramuscular and muscle group involvement and how these relate to the progressive loss of functional strength with aging. As isokinetic dynamometers are costly, and testing protocols potentially time-consuming, it may be informative to restrict assessment to a primary muscle group such as the knee extensor and flexors, as the testing protocols of these muscle groups are easily mastered by young boys and a pediatric attachment for the knee is available.
Functional motor skills
The ability to perform the STD and WRJ skills of the GMFM, mastered by typically developing (TD) children by 5 years of age, was 77% and 72% in the CS group and 76% and 65%, in the NCS group, respectively at baseline. The skills that tended to differentiate between the boys on CS and those who were NCS were the STD skills that involved position transitions such as sit to stand, half-knee to stand, stand to floor, and squatting; and the WRJ skills that involved jumping, hopping, and stair ascent/descent. Similarly, Schreiber et al. 2017 compared ambulatory boys with DMD (mean 7.9 yrs.) on corticosteroid therapy, to an untreated group, using the Motor Function Measure (MFM) a generic scale developed to monitor progression in neuromuscular disease, and reported higher standing/transfer scores in the corticosteroid group at baseline assessment as well as greater retention of motor function over the two year follow-up [44].
During the course of this study the North Star Ambulatory Assessment (NSAA) was developed to identify ambulatory changes in boys with DMD and has become widely adopted as a secondary outcome measure in clinical trials [45–47]. The NSAA skills, mastered by TD children by 4 years of age [48], assesses 17 ambulatory skills,14 of which are within the STD and WRJ dimensions of the GMFM. A large cohort study used the NSAA to examined the effect of early corticosteroid therapy initiation on the natural history of ambulatory function in boys with DMD and reported a decline in boys > 7 years of age; however, skill gains were reported in boys < 7 years, with higher scores seen in those who had initiated corticosteroid therapy early (between 3–5 years) [45]. A further investigation utilized the NSAA to cluster boys with DMD based on rate of disease progression and observed that despite similarities in age at diagnosis, boys with a more rapid disease progression tended to have corticosteroids prescribed earlier [49]. In this study cohort of boys with DMD, 41% of the boys in the CS group (treatment onset mean age 4.8 years), and 25% in the NCS group were < 7 years at their baseline assessment. Of this subgroup, at one year, one boy in the NCS group demonstrated a gain in STD and WRJ skills, while in the CS group 68% gained STD skills and 82% gained WRJ skills. Additionally, of the boys > 7years of age, 22% in the CS group and 33% in the NCS group demonstrated gains in STD and WRJ skills at one year. It is probable that corticosteroid therapy contributes to the skill development seen in select boys > 7; however, variability in disease progression secondary to genotype and other contributing factors most likely contribute [49–51].
The GMFM is sensitive to the changes in motor function across time in boys with DMD and in agreement with previously reported findings using the NSAA [45, 52]. While the GMFM offers a greater range of motor skills, and greater granularity in the scoring system, it was not developed for DMD and is presently rated as an exploratory outcome for this diagnosis. Rasch analysis of the NSAA [53] and the recent development of a revised version suitable for younger boys (3–5 yrs.) [48], has expanded its applicability to clinical trials of ambulatory younger boys. Additionally, the Motor Function Measure (MFM), which incorporates a greater range of motor skills and expanded scoring system, with similarities to the GMFM, has shown sensitivity to change across the disease spectrum and has also been incorporated into clinical trials. The NSAA and MFM, in combination, cover the majority of the skills of the STD and WRJ dimensions of the GMFM. Future longitudinal studies will reveal whether the psychometric properties of present outcomes are sensitive to the changes of interest.
Timed function tests
Timed function tests (TFTs) were initially shown to be responsive to corticosteroid therapy in young boys with DMD and are a commonly used measure of efficacy in clinical trials [8–10, 26]. In this longitudinal study TFTs capacity declined with age in both groups, as reported previously [2, 27]; however, a slower rate of decline in the 4-stair climb and 10-meter walk/run was seen in boys on corticosteroid therapy. A recent study of ambulatory boys with DMD examined longitudinal changes in TFTs, the ability of individual TFTs to predict loss of ambulation in the following year, and the relationship between TFTs and the 6MWT [27]. Significant functional declines over a year in boys > 7 years of age were reported with the TFTs with lost in the predictable order of: supine to stand, 4-stair climb, and 10-meter walk/run [27]. It was concluded that the TFT of 10-meter walk/run was more sensitive to change than the 6MWT, had stronger predictive value, and was performed in a greater percentage of ambulatory boys up until 12 years of age, thus a potentially better measure of muscle power [27]. While the TFTs of supine to stand and 4-stair climb were also found to be sensitive measures of motor function in boys with DMD, 7–10 years of age, a large percentage of older boys lose the ability to perform these TFTs limiting their utility.
McDonald (2018) suggested TFTs may be effectively used as primary endpoints in clinical trials when the mechanisms of the therapeutic agent and its anticipated impact on disease progression are considered, thus agents directed at improving muscle strength should include the TFTs of supine to stand or 4-stair climb, due to their sensitivity to that targeted outcome. The TFT of 4-stair climb, specifically has been reported to correlate most highly with quantitative knee extensor strength [54]. The results of this study support the premise that both the 4-stair climb and 10-meter walk/run are sensitive to changes in motor performance in boys with DMD and able to differentiate the impact of corticosteroid therapy; however, their efficacy is limited by disease progression. In addition, the use of qualitative ordinal performance scales, in combination with the quantitative performance time, may be informative of alteration in muscle strength, as compensatory performance strategies secondary to strength decline are more probable during TFTs of supine to stand, and 4-stair climb. In conclusion evidence suggests that TFT attributes should be given careful consideration when chosen to assessing efficacy in clinical trials. As noted by McDonald (2018) TFTs have “withstood the test of time” as an important endpoint [55].
Limitations
The sample size of this study was relatively small with an N = 84, and unbalanced with n = 70 on CS and NCS = 14 naïve. Due to the study duration, age range at baseline, and heterogeneity of disease progression, there was variation in the number of data points contributed by each subject. The significant decline in data points across time (Supplementary Table 1) was seen due to the decline in the number of boys able to perform study assessments with increasing age. Thus, the therapeutics presently available to the majority of boys with DMD only mitigate disease progression and the outcomes utilized in this study are applicable primarily during the first decade of life. Although standard of care dosage of corticosteroids was recommended, the full dose may not have been taken due to side effects, primarily behavioral or weight gain. Boys who had taken corticosteroids for ≥ one month were placed in the corticosteroid group. The number of study visits prior to steroid initiation is delineated in Table 1. It is likely that this approach moderated the overall effects of CS therapy in this study, indicating its benefit may be greater than reported. Both Prednisone and Deflazacort were administered, and their effects may not be equivalent. Most boys on CS therapy were on a daily regime; however, 20% were on other regimes.
CONCLUSION
As corticosteroid therapy is ‘standard of practice’ in the management of boys with DMD, and often an inclusion criteria for clinical trials, understanding its influence on the rate of disease progression, specifically muscle weakness, is helpful to ascertaining the efficacy of novel therapeutics. The results of this long term longitudinal study demonstrate that corticosteroid therapy slows the rate of muscle strength decline in boys with DMD, although decline remains significant with age and variable amongst lower extremity muscle groups. Quantitative muscle testing, via isokinetic dynamometry, is sensitive to subtle changes in strength, and in combination with existing MRI protocols, may advance our understanding of how muscle group requirements (contraction types) impact the variability reported in intramuscular and muscle group decline. Quantitative muscle testing, in combination with motor skill assessments, and the TFTs, specifically the 4-stair climb and 10 m walk/run, demonstrated the sensitivity and specificity necessary to detect variations in disease progression in ambulatory boys with DMD, denoting their potential for use in future trials of new therapeutics in young boys with DMD.
Footnotes
ACKNOWLEDGMENTS
We would like to thank Jason T Newsom, PhD, Professor, Department of Psychology, Portland State University for his assistance with statistical analysis, the Shriners Hospitals for Children for supporting this study (#79115), and most sincerely the boys and families who participated in this study.
DISCLOSURES OF CONFLICT OF INTEREST
“The authors have no conflict of interest to report.”