
Abstract
In amyotrophic lateral sclerosis (ALS) lower plasma creatinine level has been associated with shorter survival and faster functional decline. It has not been clear if creatinine is associated with respiratory outcome. We analyzed retrospectively a population of unselected ALS patients. Multiple-regression and Cox-regression analyses were performed. We included 233 patients, mean age 62.8, mean disease duration of 18.6 months. At baseline, creatinine was significantly associated with ALSFRS-R, but not with its decline rate. No predictive value was disclosed for FVC, its decline rate, or with survival. We did not confirm that creatinine is a marker of respiratory outcome.
INTRODUCTION
In amyotrophic lateral sclerosis (ALS) a low pl-asma creatinine level has been associated with poor survival, faster functional decline, as assessed by the ALS Functional Rating Scale –Revised (ALSFRS-R), and more rapid progression of muscular weakness [1–7]. A meta-analysis concluded that mortality was 25% lower if the plasma creatinine level was gre-ater than the median value [8] and found a signific-ant pooled negative correlation coefficient between ALSFRS-R decline and creatinine level (0.42. p = 0.033) [8]. The relationship between low creatinine levels and shorter survival in ALS patients is not well-understood, but one possibility is a faster respiratory decline. Consistent with such possibility, Van Eijk et al., [6] found a weak longitudinal correlation between vital capacity and plasma creatinine (0.32, p < 0.001) when investigating data from the EMPOWER study. Furthermore, they confirmed a previous report [3] that plasma creatinine level is correlated with the respiratory subscore of the ALSFRS-R (R-ALSFRS-R), more so in women (p = 0.0001) than men (p = 0.0032) [3]. Ikeda et al., [1] reported an inverse correlation between baseline creatinine level and the annual decline in forced vital capacity (FVC) (0.81 and 0.44, for men and women, respectively). Furthermore, the initial creatinine level has been associated with initial and last FVC results [7]. We have studied the predictive value of plasma creatinine applying complementary statistical methods.
METHODS
Patients followed in our specialized multidisciplinary ALS clinic from 2000 to 2018 were analyzed retrospectively. Inclusion criteria were: 1) patients with possible, probable, or definite disease on revised El Escorial criteria and disease progression on regular follow-up; 2) patients with 2 or 3 consecutive evaluations at approximately 3–4 months interval, including ALSFRS-R and FVC data; 3) patients who had full laboratory evaluation, including the quantification of creatinine levels, at baseline. Baseline assessment did not coincide with time to diagnosis, since many patients were referred to our clinic from other hospitals where they were followed before. We excluded patients with other medical or neurological diseases, in particular patients with laboratory abnormalities suggesting renal dysfunction or dehydration such as increased urea level and hematocrit, and patients with missing baseline creatine measuring. Creatinine was measured using the colorimetric method of Jaffe and its values given in mg/dl.
Multiple-regression analyses were used to examine the predictive value of creatinine on baseline va-lues of ALSFRS-R, its respiratory subscore, and % FVC, as well on as the rates of decline (variation from the first to the third assessments per unit time, measured in months) of those three variables. In the regression model for the decay rate only patients without missing values of the dependent variables were used in the analysis. In all analyses, we used the same additional set of independent variables: age, gender, disease duration (at diagnosis), onset pheno-type, body mass index, and clinical signs of fronto-temporal dementia. Cox-regression analysis was applied to determine the predictive value of creatinine on “survival time”, which was calculated from the moment of diagnosis to death or censoring date (60 months after diagnosis), controlling for the same set of potential confounders (that is, using the same set of independent variables). Specifically, we did two Cox regression analyses: one using the continuous creatinine levels (as for the multiple-regression analyses) and the other using creatinine levels dichotomized according to the respective median value (median-split method), so that we could also compare survival between two (above-median and below-median) gro-ups. All variables used in the multiple-regression and Cox-regression analyses were normalized so that their maximum absolute value was equal to 1, to facilitate direct comparison of the estimated coefficient values. Bonferroni correction for multiple comparisons was separately applied to each type of multiple regression (that is, to regressions concerning baseline and decline-rate assessments, which resulted in the following significance threshold: p-value, or p, below 0.05/3). Statistical analyses were performed on MATLAB R2015A® or SPSS Statistics 22®.
This project was approved by the local Ethics ‘committee.
RESULTS
We excluded 1042 patients, the main reasons were concomitant medical disorders and missing baseline creatine measurement. This population included 57% men, 72% with spinal-onset, mean age 62.1 (SD, 12.5), mean % FVC was 84.3 (SD. 24.3), mean was ALFFRS-R 41.7 (SD, 6.7).
We studied 233 patients (131 men, 56%, 52 with definite, 140 with probable and 41 with possible), mean age 62.8 years (SD 12.2), 171 (73%) with sp-inal onset, and 8.2% with clinical signs of FTD. At study entry, mean BMI was 24.9 (SD 3.7), mean % FVC was 81.9 (SD 23.4), and mean ALSFRS-R was 42.0 (SD 6.7). The clinical features were similar between excluded and included patients (p > 0.05 for all comparisons).
Mean disease duration at baseline assessment was of 18.6 months (SD 21.3), 50% of the patients died 20 months after study entry, and 62% after 24 months. The mean creatinine level was 0.78 mg/dl (SD 0.28) at baseline for the whole population, and a similar value was found for spinal-onset (0.78 mg/dl) and bulbar-onset (0.79 mg/dl) groups (p = 0.6). However, men had higher values as expected (0.85, SD 0.19 vs 0.69, SD 0.21, p < 0.001). % FVC declined 0.91% (SD, 1.78)/month, ALSFRS-R 1.02% (SD, 1.58)/month, and respiratory subscore 0.14% (SD, 0.27)/month (Fig. 1). The rate of decay was similar between the first and second half of the follow-up period for the functional assessments and % FVC (p > 0.05)
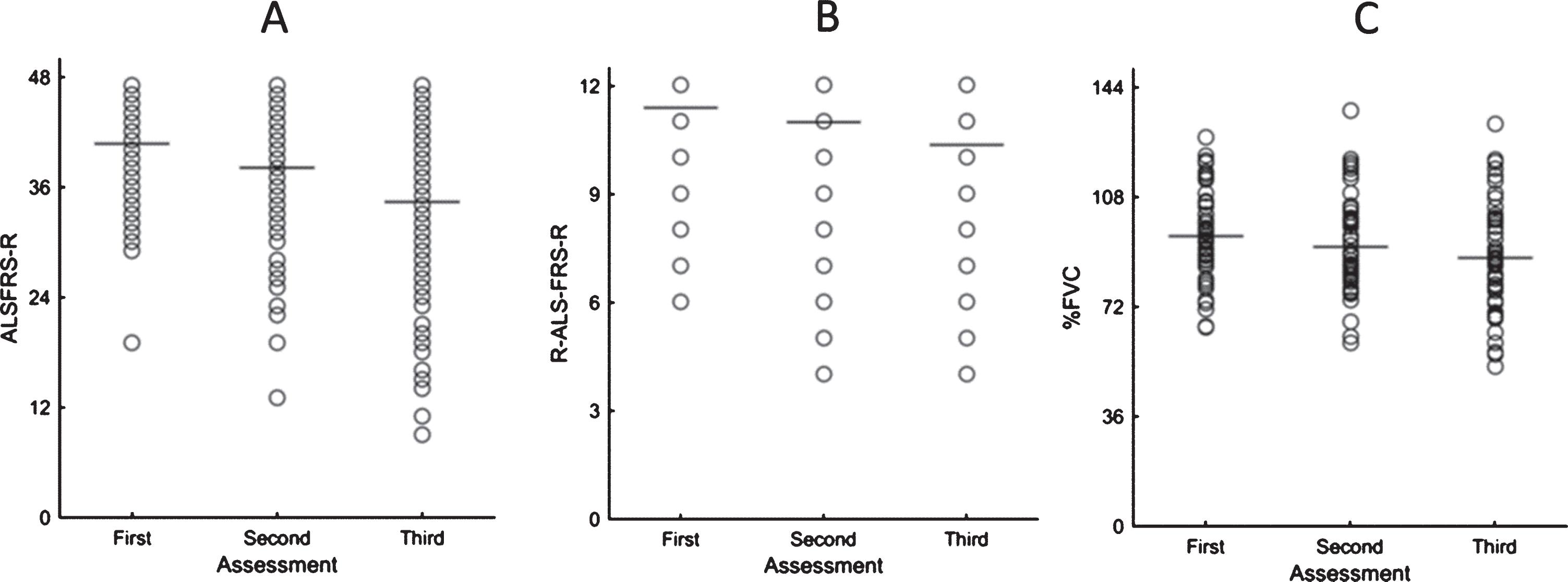
Represents the decay of individual and mean values for: A- ALSFRS-R; B- respiratory subscore (R-ALS-FRS-R) and predictive value of forced vital capacity (% FVC).
The results concerning the predictive values of creatinine at baseline, and on the decline rates of ALSFRS-R, its respiratory subscore, and % FVC val-ues are summarized in Table 1. At baseline, creatinine was significantly positively associated with the global functional score (ALSFRS-R score; p = 0.016). Furthermore, at baseline, age was significa-ntly negatively associated with all clinical variables; that is, higher age was predictive of lower global (p < 0.001) and respiratory (p = 0.016) functional scores, as well as of lower % FVC values (p = 0.003). No association was found between creatinine levels and the decline rates of ALSFRS-R (p = 0.251), its respiratory subscore (p = 0.435), or % FVC (p = 0.574). The decline rate of ALSFRS-R, however, was found to be negatively associated with disease duration at baseline (p = 0.007).
Table1
Multiple-regression analyses. Each row relates to a specific dependent variable; the respective n indicates the number of patients included in that regression. Each column represents an independent variable (common to all regressions; bulbar and onset forms were coded in a Boolean fashion). Each cell contains the value of the respective coefficient. Coefficients that were significantly different from 0, before Bonferroni correction for multiple comparisons (p < 0.05), are marked with an asterisk. Coefficients that were significantly different from 0, following Bonferroni correction (p < 0.05/3), are additionally shown in bold. Abbreviations: ALSFRS-R –Amyotrophic Lateral Sclerosis Functional Rating Scale –Revised; BMI –body mass index; FTD –frontotemporal dementia; R-ALSFRS-R –respiratory subscore of the ALSFRS-R (questions 10 + 11 + 12); % FVC –predicted forced vital capacity. *Number of patients with 3 longitudinal evaluations.
Concerning survival (n = 215), the only significant independent predictors were age [regression using continuous creatinine values: hazard ratio (HR) = 14.91, p = 0.0003; regression using median-split creatinine values: HR = 14.88, p = 0.0002] and bulbar-onset (continuous creatinine values: HR = 2.18, p = 0.037; median-split creatinine values: HR = 2.16, p = 0.041). Creatinine levels did not have predictive value for survival (continuous creatinine values: HR = 0.50, p = 0.399; median-split creatinine values: HR = 0.82, p = 0.328), as summarized in Table 2.
Table2
Cox-regression analyses (on the data from 215 patients) using continuous (above) or median-split (below) creatinine values. Each row represents an independent variable (with bulbar and spinal-onset coded in a Boolean fashion). B represents a given coefficient value. Significant coefficients (p < 0.05) are shown in bold. Abbreviations: BMI –body mass index; FTD –frontotemporal dementia.
DISCUSSION
We have confirmed that in ALS plasma creatinine level is related to functional disability at baseline. This is not surprising since function depends on muscle strength, and strength decreases with progressive muscle wasting and weakness. However, contrary to most previous reports, our results do not support that plasma creatinine levels at the time of diagnosis are associated with rate of decay in functional score or with respiratory impairment. Further, we did not find that creatinine levels predicted survival, and there was no association between baseline level of creatinine and the rate of FVC decay. Respiratory involvement in ALS is related to diaphragm weakness [8], and the volume of this muscle is not related to the creatinine level. Typical bulbar-onset ALS, widespread disease involvement at presentation, and first symptoms later in life can all occur with long survival in some patients, if respiratory function is not much affected [9]. The results of a recent systematic review and meta-analysis [10] were not conclusive regarding the use of plasma creatinine levels to predict survival. The plasma creatinine level has considerable physiological variability, depending on gender, age, exercise routine and comorbidities limiting its likely value as a biomarker for progression in ALS. Moreover, creatinine and % FVC change are not linear in ALS, which can limit its use as a biomarker for respiratory function.
Our study has several limitations with potential impact on results. The study was retrospective, pat-ients were heterogeneous regarding their ALS syndromes, regarding FVC measurement several patients missed their 3rd evaluation time, the number of patients was not very large, the rate % FVC decay was low (< 1% /month) suggesting that this population had a more benign respiratory outcome, and since not all patients followed in our center were included we cannot exclude the hypothesis that our study lacked power to identify significant associations. An important limitation is that creatinine level was only measured at baseline, in particular considering that creatinine level does not follow a linear decay over disease progression [5].
Selecting, among ALS patients, potential candidates for a trial could lead to more positive results, as reported elsewhere [5]. In this regard, our results do not reject that creatine can be a useful biomarker in trials. However, they do suggest that, in everyday practice, in which a very heterogeneous population of patients is dealt with, creatine is unlikely to be a significant predictor of respiratory outcome.
CONFLICT OF INTEREST STATEMENT
None of the authors has any conflict of interest to disclose.