
Abstract
Background:
Boys with dystrophinopathies (DMD) are at increased risk of low bone mineral density and fracture. Femoral fracture is the most common extremity fracture and is accompanied by significant risk of functional loss. Care considerations for DMD have stressed that aggressive management may be needed to maintain ambulation and that surgical fixation allows early mobilization.
Objectives:
Describe 5 cases of femoral fracture in ambulatory boys with DMD and the course of care undertaken to optimize function.
Patients:
Five boys with DMD median age 15y (12–16) who were independently ambulatory. Median 10m walk speed prior to their first fracture was 8 sec (7–17.37) and 4 of 5 were less than the 9 seconds predictive of 2 year ambulation retention. Three of the cases had a single incident causing fracture; the remaining cases had 2 and 3 incidents respectively representing a total of 8 fractures 6 of which were surgically stabilized.
Results:
Following the first fracture, all 5 subjects regained some form of ambulation. Three patients regained independent ambulation and 2 with hand held support or contact guard. Two subjects went on to have additional falls with associated fracture. No patient regained the ability to rise from the floor and only one of the 5 regained the ability to climb steps and all demonstrated a decline in walking speed.
Conclusion:
Prompt orthopedic intervention, early mobility, and intensive rehabilitation even in the end stage ambulatory patient, were factors in helping preserve function in these patients with dystrophinopathies.
INTRODUCTION
Duchenne muscular dystrophy is one of a group of disorders affecting the muscle. It occurs in one in 3,500 live male births [1]. Diagnosis is typically made at about 4 years of age [2] with the boys often having difficulty climbing steps, running or getting off the floor when compared with their peers. The functional progression of the disease is typically characterized by mildly delayed motor skills and onset of ambulation [3]. This is followed by improvement in ambulatory and gross motor skill albeit at a diminished rate when compared with peers. As school age approaches, the weakness and functional divergence from their peer group becomes apparent, though motor skills progress up until approximately 7 years of age [4, 5]. Following this stage there is a period of functional plateau followed by a progressive loss of motor skill and a diminution of ambulatory stability and speed. This overarching phenotypic progression is expressed with considerable variability across the severity range, from the classic Duchenne phenotype (ambulation loss prior to 13 years) to the milder Becker Phenotype (ambulation loss after 16 years). This spectrum of disease is accompanied by varying rates of progression with these overarching functional stages occurring at varying age depending on disease severity [2, 6].
Both weakness and diminished ambulatory ability contribute to altered forces placed on the bone. Bone strength and bone development are both partially dependent on these forces. Many disorders that effect muscle force production also present with decreased bone mineral density as the result of diminished and abnormal forces placed on the bones [7]. Boys with DMD typically demonstrate diminished bone mineral density which becomes more severe as they age, with up to 80% of ambulant boys having osteoporosis of the femoral neck [8–11]. In addition, one of the only effective treatments for Duchenne muscular dystrophy is corticosteroids. This has as a side effect the increased formation of osteoclasts facilitating bone resorption and apoptosis as well as impairing the function of osteocytes and osteoblasts [12]. The result is an impairment in the formation of bone and decreased bone mineral density [13, 14]. The weight gain that often accompanies corticosteroid use has the effect of somewhat diminishing the impact of gains in strength. This is counterbalanced by the diminished stature that ameliorates the additional antigravity strength required to carry the additional body weight [14]. Fracture risk is influenced by many factors; weakness, decreased weightbearing forces, and steroid use all contribute to the exacerbation of osteoporosis. This places these children at significant risk of fracture, and with fracture, functional decline.
Boys with Duchenne muscular dystrophy have increased rates of fracture as compared to age matched controls, with fracture rates reported at between 21%–40% [15, 16]. Between 35 and 44% of ambulatory boys and up to 67% of non-ambulatory boys who have had lower extremity fractures suffer a permanent loss of function [9, 17]. Early mobilization following injury has long been felt important in maintaining function in boys with DMD and prolonged bedrest is to be avoided, [18]. Open reduction and internal fixation allows earlier mobilization as compared with casting or splinting [19] though there are not uniform recommendations available in the literature. Care considerations for boys with DMD recommend anticipatory guidance around fracture prevention and indicate that open reduction and internal fixation during the ambulatory phase of disease might be indicated to preserve ambulation [20]. Limited evidence [21, 22] is available to guide the best choice of orthopedic treatment for the fracture with a number of effective methods available for fixation depending on the characteristics of the injury. There are only limited resources on the specifics of physical therapy management to guide practice [23]. To inform the approach to care of this population one must draw on the literature in other populations and age groups in the context of Duchenne specific considerations [24, 25]. Here we present 5 consecutive cases with surgical fixation following fracture combined with post-operative rehabilitation. Our objective is to present details that can be used to inform clinical decision making regarding the potential successes that can be achieved managing this relatively common comorbidity.
CASE DESCRIPTION
Background
Patient 1 has a diagnosis of Intermediate muscular dystrophy secondary to an out of frame deletion of exon 51. He experienced a right femoral fracture at 16 years of age. He had been treated with deflazacort since the age of 10 years. One month prior to fracture, he was ambulatory for short distances and utilized a scooter for community distances; please see Table 1 for pre-fracture status.
MMT – Manual muscle testing; Myometry represents Pounds of force (standard deviations from the normative mean)
10 m – Time to walk or run 10 meters measured in seconds; PROM – Passive range of motion degrees from neutral. Dzt – deflazacort; Atlrn – ataluren; Pred – Prednisone; HS – Hamstrings; Quad – Quadriceps; N/A – not available.
Fracture history
At the age of 16 years and 11 months old, he experienced a fall and suffered a right comminuted three-part fracture through the distal one third of the diaphysis of the femur without significant displacement, angulation with apex directed laterally. One day following fracture, surgical management included an open reduction and internal fixation and application of an external fixator (Fig. 4). He was non weight bearing (NWB) for 7 days and then progressed to weight bearing as tolerated. He was cared for at home during this time with appropriate splinting and stretching to maintain his flexibility.
Rehabilitation admission
Inpatient rehabilitation began 1.5 weeks after his fracture and lasted for 16 days consisting of twice-daily PT and OT (one 30 min and one 60 min session each) 7 days a week. He then transitioned to a day hospital program for an additional 3 weeks that included daily hour-long Physical Therapy and Occupational therapy sessions Monday through Friday. His course of care included gait training with an Up n’ Free® and LiteGait™ for partial weight bearing (PWB). The LiteGait™ provides a fixed overhead harness based strap system that will take 100% of the patient weight if needed while the Up n’ Free® provides partial weight support from a gait trainer mounted seat that adjusts to unweight a portion of body weight. When an assistive device was first used; a walker with forearm support was employed, then progressed to an anterior rolling walker. Passive range of motion and resting splints continued to be used to maintain ankle flexibility. The external fixator was removed after 12 ½ weeks and he was re-admitted to day hospital for a 7 week stay. Once the external fixator was removed, aquatic therapy and a stationary bike was also initiated. The aquatic therapy allowed more natural weight shift during ambulation in combination with body weight support.
Functional status
Upon discharge from day hospital he was ambulating with modified independence with a gait trainer. He required contact guard to ambulate 25 feet and to transfer to and from his scooter and was able stand with contact guard, requiring light physical contact; but no actual assistance for 3 minutes. His strength was assessed via myometry [26, 27] with a microfit 2 myometer. For knee extension, he measured 9.8lb right (–3.92 standard deviations) and 11lbs left (–3.86 standard deviations). For knee flexion he measured 14.9lbs right (–3.94 standard deviations) and 27.9lbs left (–3.22 standard deviations) (Fig. 3). His ankle dorsiflexion passive range of motion was 0° right and –6° left (Fig. 2). He transitioned to an outpatient physical therapy program and began to walk with an anterior walker. He gained the ability to ambulate with bilateral hand held assist after 5 weeks and to walk with contact guard after 7 weeks of outpatient PT 2 times per week. Different tasks were employed to facilitate weight shift, a bike was used for endurance and task specific transfers and ambulation was practiced.
Background
Patient 2 has a diagnosis of Intermediate muscular dystrophy secondary to an out of frame duplication in exon 2 and had a history of prednisone treatment from the age of 6 till 11 when he started on deflazacort, please see Table 1 for pre-fracture status.
Fracture history
He has a history that includes 3 fractures; an occult right femoral fracture at 13 years 11 months; a distal fibular Salter Harris II fracture at 14 years 3 months; and bilateral femoral fractures (left distal femoral fracture and right basicervical femoral neck fracture) at 15 years 11 months. Prior to the occult fracture his 10m walk/run was 7 seconds (Fig. 1). The fracture was not visible on xray but identified on MRI. He was non-ambulatory for a week then continued to walk with an anterior walker and a knee immobilizer. He was referred to outpatient PT for bodyweight support treadmill training where he regained ambulation and the ability to climb steps, this subject was the only one who regained this ability and no subject regained the ability to transfer from the floor (Fig. 1).

Timed tests: 4 stair climb - time to climb 4 steps, Gowers time - time to rise from the floor, 10 m walk/ run – time to go 10 meters. The X-axis represents years prior to or following the first fracture.
The distal fibular fracture was treated with short leg cast and minimal weight bearing with a walker and continued physical therapy following which he again regained independent ambulation, walking 10 m in 8.12 seconds (Fig. 1).
The left distal femoral fracture and right basicervical femoral neck fracture was treated one day following injury with a closed reduction and pinning of the left femoral shaft and an open reduction and internal fixation of the right femoral neck(Fig. 4). He was NWB for 6 weeks and cared for at home: the parents were instructed in transfers and ankle splint use, and a reclining wheelchair provided as well. He was then progressed to weight bearing as tolerated.
Rehabilitation admission
Inpatient rehabilitation was initiated 9 ½ weeks from initial injury. His 2 ½ week inpatient rehabilitation course of care included aquatic therapy, gait training with partial body weight support, stander tolerance, transfer training, sitting balance, and strengthening. He continued to stretch and to use his AFOs at night. A combination of aquatics and gym based partial weight support allowed a gradual progression of weight bearing as his confidence improved.
Functional status
Upon discharge from inpatient rehab, he was ambulating short distances with a gait trainer (Up N’ Free®), assisting in transfers, and utilizing a stander. His strength was assessed via myometry. For knee extension, he measured 12.2 lbs right (–3.8 standard deviations) and 10.4 lbs left (–3.89 standard deviations). For knee flexion he measured 20.5 lbs right (–3.63 standard deviations) and 17.1 lbs left (–3.82 standard deviations) (Fig. 3). His ankle dorsiflexion passive range of motion –17° right and –23° left (Fig. 2).

Dorsiflexion passive range of motion measured by goniometry with the knee extended. The X-axis represents years prior to or following the first fracture.

Strength as measured by break test hand held dynamometry. Standard positions sitting with the knee at 90 degrees for quadriceps and 45 degrees for hamstring [26].
Outpatient rehabilitation
He then transitioned to an outpatient program where he was serial casted for ankle range of motion. Seven weeks of weekly cast changes; application in prone; knee flexed; and the foot in maximal comfortable dorsiflexion resulted in improved ankle range of motion. Initial range was –6° and –22° right (knee flexed/extended) and –5° and –25° left (knee flexed/extended) final dorsiflexion improved to +2° and –2° left (knee flexed/extended) and+1° and –3° right (knee flexed/extended) (Fig. 2). Following the casting he participated in a balance training and gait-training program that included progressive active weight shift and dynamic activities designed to facilitate the use of postural reactions and active weight shift this was both in the gym and aquatic environment. Wedging of the heel of the shoe to accommodate the remaining heel cord contracture, to align his center of gravity, and improve comfort with weight bearing.
Functional status
He gained the ability to stand with minimal assistance and transfer to standing with a table in front of him and continued to stand with hand held assist in the home and ambulate with minimal assist from his parents in the home until age of 20.
Background
Patient 3 has a history Duchenne muscular dystrophy due to a point mutation in the exon 19 splice site (IVS19 + 2T>C) producing an out of frame mutation. He had been on deflazacort since 5 years of age, please see Table 1 for pre-fracture status
Fracture history
At the age of 12 he experienced a fall down two steps at home, twisted, and fell onto his right leg. He suffered a comminuted fracture of the distal femoral diaphysis with varus angulation of the distal fragment and a posterior and lateral displacement of the distal fragment approximately 1/3 the shaft width. That day he underwent an open reduction and internal fixation of the right femoral shaft with a submuscular plate (Fig. 4). He was kept in a Knee immobilizer for 6 weeks, Initially NWB.
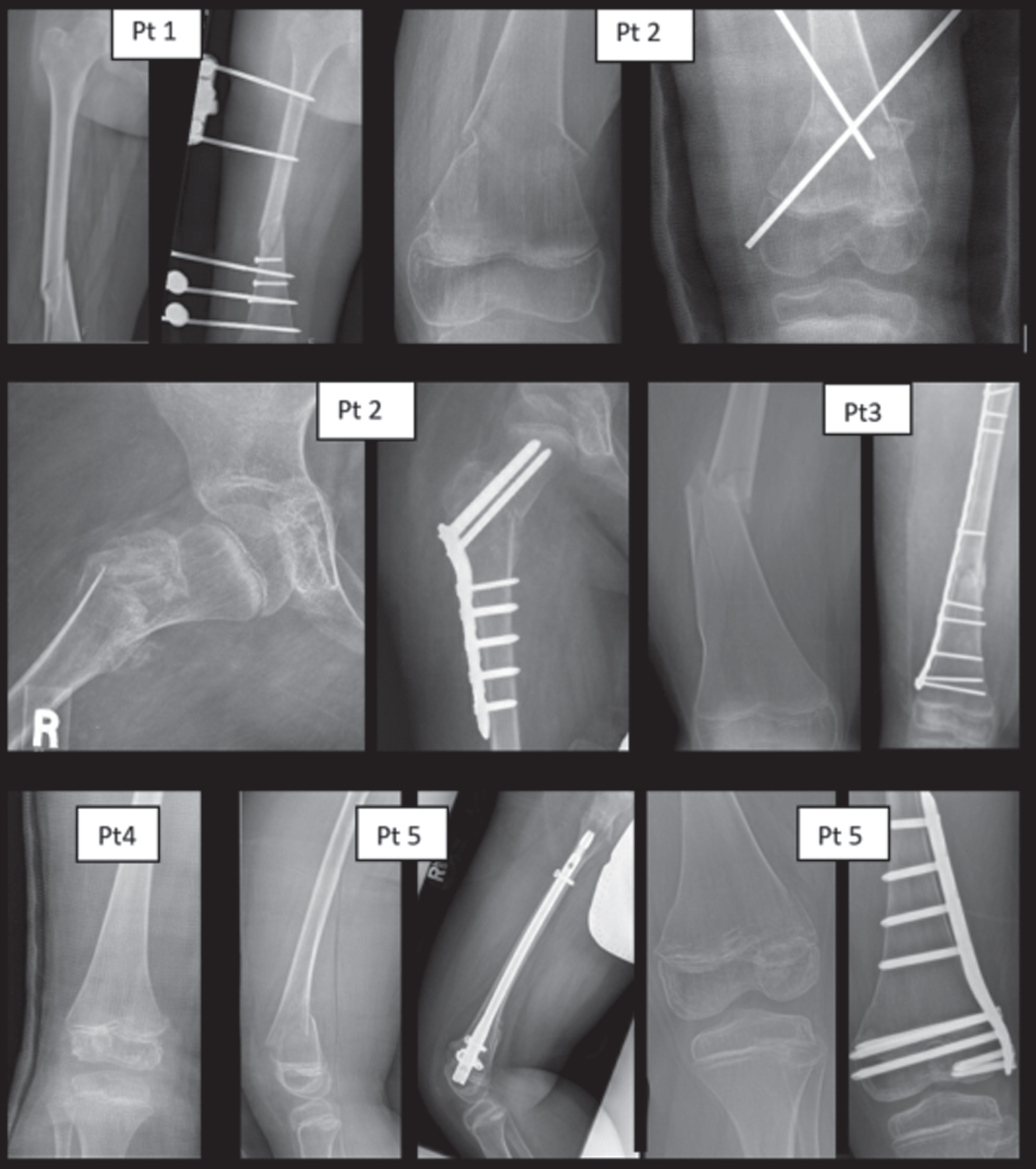
Initial xray on the left and internal fixation on the right for all cases other than patient 4 where only an initial xray is provided.
Rehabilitation admission
Inpatient rehab was initiated 2 weeks post fixation with the precautions of NWB to toe touch weight bearing with PWBpermitted in the pool and on the tilt table. Following a 2 ½ week admission he was discharged home for 2 weeks with ongoing pool therapy and returned for a 6 week Day Hospital program after being cleared for weight bearing as tolerated. His therapy course consisted of gait training initially with a Rifton® pacer gait trainer that provided a sling support seat and allowed him to practice with varying degrees of weight bearing to his tolerance; then a LiteGait™ body weight support over ground training was initiated; followed by an anterior rolling walker. Ambulation with no assistive device was initiated in the pool, this allowed for PWB and was gradually reduced in frequency once weight bearing was progressed and his strength, balance and confidence improved. Other activities included the use of a bike to maintain lower extremity strength and a tilt table to initiate weight bearing and standing tolerance. Passive range of motion was maintained with splinting and passive range of motion. Transfer training made use of varied height seated support surfaces to titrate the effort needed for initiation. He was transferred to outpatient following inpatient rehabilitation where he worked on endurance ambulation; an adaptive tricycle; and continued with transfer training, balance and contracture management.
Functional status
Seven months post fracture he was able to walk 10 m in 58.5 seconds (Fig. 1) requiring 3 rest breaks, 3 weeks later his time had improved to 10.6 seconds and no rest was required. Dorsiflexion range of motion was 5
Background
Patient 4 was diagnosed with Duchenne muscular dystrophy due to a premature stop mutation at c.2866C>T (p.Q956X) of the dystrophin gene. Treatment history included ataluren since 5 years of age and deflazacort since 4yrs 4months, please see Table 1 for pre-fracture status.
Fracture history
At the age of 14years 4 months he experienced a Salter-Harris III fracture of the distal end of the right femoral shaft (Fig. 4) following a fall. He was splinted at an outside hospital and placed in a Long leg NWB cast 2 days later and was permitted to weight bear in a stander a week later which he followed through with at home with his parents.
Rehabilitation admission
Three weeks post fracture he began a 4-week Day hospital admission, where he received one session of PT and one session of OT daily Monday through Friday as an outpatient and stayed with his family at home at night. Initially he was standing with a knee immobilizer and minimal assistance assist, this gave him confidence that his knee wouldn’t buckle in standing. He was dependent for transfers, but was ambulating 4 feet at a time with maximal assistance. His physical therapy program consisted of night splints, range of motion, gait training, and therapeutic exercise. The exercise program included both endurance bike exercise and a pool therapy program. Standing balance with body weight support with ZeroG® Gait and Balance System was also utilized during the day hospital stay and allowed weaning of the knee immobilizer as he gained confidence. Following day hospital he received outpatient PT twice a week for 8 weeks where he worked on standing balance bike activities and closed chain exercise.
Functional status
At discharge from day hospital, he was ambulating 5 feet without his knee immobilizer requiring moderate assist and was standing with minimal to moderate assist for 30 seconds at a time. Following his outpatient course of PT his improvements resulted in his ability to tolerate standing for >5 min and transfer sit to stand with contact guard to close supervision and ambulate 20’ at a time with contact guard, no 10 m walk time was taken on discharge. Fifteen months after fracture he was no longer able to ambulate. He continued to use his stander but he was having trouble standing on his own.
Background
Patient 5 had a diagnosis of Duchenne muscular dystrophy secondary to an out of frame deletion of exons 53–55. He had been on deflazacort since 4 years 9 months; please see Table 1 for pre-fracture status.
Fracture history
He has a history of 2 fractures at 15 years of age and at 17 years of age. The first was a displaced right distal femoral metaphyseal fracture and the second a distal left femoral fracture. The distal femoral metaphyseal fracture was treated at an outside hospital with a closed reduction and long leg cast. Ten days later he underwent open reduction and internal fixation with an intramedullary nail (Fig. 4). Post op day 1 he was standing bedside weight bearing as tolerated with supervision and an anterior walker and knee immobilizer with moderate to maximal assistance for transfer.
Rehabilitation admission
One week post surgery he was admitted for a 10 day inpatient rehabilitation stay followed by outpatient physical therapy. During his inpatient stay his transfers improved to moderate assist and was initially ambulating 12 feet with walker and knee immobilizer with contact guard. His inpatient program consisted of gait training and transfer training with the walker; standing balance activities; therapeutic exercise; and bike based endurance exercise. He did not require the use of body weight support or aquatic therapy as his strength and functional ambulation did not warrant that degree of support.
Functional status
At discharge from inpatient rehabilitation, he was ambulating over 150’ with walker and standing for 2–3 min at a time with supervision. During his outpatient PT, by 5 weeks post-surgery, he was able to walk 50 feet without an assistive device and 12 months later he was able to ambulate 10 meters in 20 seconds. (Fig. 1)
Fracture history
His second fracture was a distal femur fracture; it was fixated by open reduction and plate and screws.
Rehabilitation admission
Following the surgical stabilization and PT to instruct in a standing program he was discharged to home and outpatient PT with 50% weight bearing allowed in a locked hinged knee brace where he worked on standing endurance, sit to stand activities as well as isometric exercise both in standing and on the mat as well as concentric mat exercises. Five weeks later he was admitted to inpatient rehabilitation and was progressed to weight bearing as tolerated and cleared to wean the brace.
Functional status
At discharge from rehabilitation he had progressed to independent sit to stand transfers and short distance ambulation with a rollator walker.
DISCUSSION
Dystrophinopathy represents a spectrum of disease from the classic Duchenne through the less severe Becker phenotypes with Intermediate muscular dystrophy representing a middle ground. Three out of our 5 patients presented with a typical Duchenne presentation and began on corticosteroids between the age of 4 and 6 years with two having presented with a phenotype more characteristic of Intermediate muscular dystrophy beginning on corticosteroids at 10 years (patient #1) and 6 years 11months of age (patient #2). The patients with earlier onset Duchenne muscular dystrophy had demonstrated a steeper rate of progression over time and would have been expected to continue to progress more rapidly, one of the patients (patient 2) who remained ambulatory was among to two with Intermediate muscular dystrophy.
Fracture care
There was a range of weight bearing permitted following fracture, this was dependent on both the type of fixation used and the callus formation at the fracture site. The type of fracture fixation chosen depended upon both patient-and fracture-specific factors. Patient specific concerns include the age of the patient (Due to the need to respect the growth plates), functional level, and bone density. Fracture characteristics include location, angulation, displacement, and comminution (Fig. 4). The general principles are to choose treatment that limits immobilization and allows weight bearing and ambulation as soon as possible. This minimizes disuse osteopenia and muscle wasting and provides the greatest opportunity for the ambulatory patient with DMD to return to their pre-fracture functional level. For these reasons, the preference in this series was to avoid casts and use operative techniques wherever possible. However, other considerations accompany surgical fixation in patients with DMD. These patients were all on long-term corticosteroid treatment and as a result had adrenal insufficiency and more profoundly impacted bone density. With the presence of adrenal insufficiency, stress dosing is required to accommodate the physiologic stress of surgery and to assure the maintenance of appropriate hormone levels perioperatively.
Three patients had internal fixation, including intramedullary rod (patient #5), submuscular plating with 3.5 mm distal femoral plate (patient #3), and percutaneous pinning left and internal fixation right (patient #2). Patient #1 had an external fixator placed and patient #4 was casted. Patient #5, treated with the intramedullary rod (Fig. 4), was permitted weight bearing as tolerated on post op day 1 and was one of the two patients that returned to ambulation, though 12 months later his walk speed was 20 seconds. At the other end of the spectrum was patient #2, with bilateral fractures. Patient #2 returned to functional ambulation following his first fracture which didn’t require surgery (10 m time 8.12 seconds) but prior to his last fracture his 10 m time was 19.95 seconds. He remained NWB for 6 weeks and despite the period of immobilization he ultimately continued to walk at home with his parents (and demonstrate this in clinic) for a number of years. The other three patients began weight bearing in post op weeks 1, 2, and 3 with patient #2 beginning in the pool and the others in various ways on land.
Prior functional status impact:
Four of the patients in our cohort were relatively good ambulators prior to their first fracture with 10-meter walk speeds of 8 seconds (patient #1) and 8.99 seconds (patient # 5) and two with walking speed of 7 seconds (patients # 2 and 3). Two fracture incidents were in patients who were at the end stage of ambulation prior to one of their fractures and had walk speeds of 17.37 (patient # 4) and 19.5 seconds (patient #2 prior to last fracture). Ultimately, 3 regained the ability to walk independently following their first fractures, though their walk speed all suffered in follow up evaluations and continued to progress over time (Fig. 1). One patient who regained ambulation had a first 10 meter walk speed that was 58.5 seconds that then improved as he recovered. The patients who regained ambulation were all in the group that had relatively faster walk speeds and only one regained the ability to get off the floor with one regaining the ability to climb stairs (Fig. 1). Of the two patients with the slowest walking speed, both experienced important functional gains following rehab. One of these patients regained the ability to ambulate with either hand held assist or contact guard and one retained that skill for an additional 4 years. Strength was relatively more variable over time, but 4 of 5 patients showed improvement after fracture as recovery occurred with one, patient #2, demonstrating continued loss of both quadriceps and hamstring strength (Fig. 1). Aside from those who gained the ability to ambulate again, the remaining patients gained the ability to transfer or stand with assist. This ability provided meaningful benefit and helped forestall the onset of disuse atrophy associated with the absence of weight bearing that often necessitates dependent transfers in this population.
Physical therapy program characteristics
The rehabilitation course employed uniformly consisted of progression from supported PWB in either the pool, ZeroG® Gait and Balance System, LiteGait™ or gait trainer followed by progression to an anterior walker beginning with assisted ambulation, though there was variation based on therapist preference and patient response. The choice of initial support device was driven by patient specific factors, for example one patient had an external fixator and could not go into the pool, and also by therapist preference or available technology. The ZeroG® is an overhead suspension system that allowed an adjustable fixed percentage of body weight to be supported; this is a newer device and was not available for all subjects. The LiteGait™ is also an overhead suspension but provides a fixed point of contact that will take 100% body weight. Similar to the ZeroG® is the Up n’ Free® where an adjustable percentage of body weight can be removed but the weight is born from a gait trainer mounted seat. Some of the device choice was based on patient comfort with the various support systems as many of the boys were very nervous getting up for the first time. With the initiation of independent ambulation (with or without a walker), therapists often choose the use of a knee immobilizer to protect against inadvertent collapse. With the progression of strength and confidence, the knee immobilizer was able to be weaned. Some therapists also included a gait trainer in their progression depending on the child’s pain, anxiety, and confidence in standing. Additionally management of the child’s ankle contracture was an important part of the post fracture management on both the fractured and the intact leg. Awareness that contractures develop rapidly and that the lack of weight bearing alters the maintenance of flexibility was an important consideration in all cases and in each case it was stressed to the parents the importance of splinting both day and night when not weight bearing. In addition, an awareness of the effect of ankle flexibility in restraining anterior weight shift within the base of support also drove therapist decision making related to casting or accommodating contractures with heel posting. This allowed the reestablishment of a stable symmetric base of support and the ground reaction forces of the gastrocsoleus complex optimized the resulting knee extension moment at the knee and aided standing balance. All patients showed progression of contracture, which was in line with the trajectory of range of motion loss that was experienced prior to fracture, aside from patient 2 who had a somewhat more abrupt loss of range on one side (Fig. 1). This resulted in the choice to serial cast.
The range of therapy intensity applied in this series varied from inpatient rehabilitation to day hospital and outpatient. The transitions from higher to lower intensity were driven by patient progress and goal attainment. In general when patients had achieved a stable plaque to carry over to the next setting a transition was considered. It is not known from this series what the minimum effective frequency would be and further investigation would be needed for this to be established.
CONCLUSION
Care guidelines for Duchenne Muscular Dystrophy have broadly outlined the principles of fracture care and the importance of early mobility following femoral fracture in patients with dystrophinopathy in preserving function. Orthopedic intervention with open reduction and internal, or external, fixation allows prompt weight bearing following surgery. Intensive rehabilitation, including management of flexibility and utilization of partial bodyweight support or aquatics for ambulation, to diminish the development of contracture and ameliorate the effects of disuse atrophy, can help preserve meaningful function. This can diminish the burden of care by allowing mobility, where otherwise dependent transfers would be needed. This was the case even for our patients in the end stages of ambulation.
CONFLICTS OF INTEREST
AMG: Consulting for Atom-International.
Footnotes
Appendix
Partial body weight support: any harness system typically over a treadmill for gait practice
LiteGait™: harness system for gait training with a fixed overhead tether
ZeroG® Gait and Balance System: overhead harness system with an adjustable degree of body weight support.
Gait trainer: wheeled mobility device that has the option to provide a seat, trunk support, and forearm weight bearing
Rifton® Pacer: a gait trainer that provides dynamic support allowing both vertical and horizontal pelvic displacement during ambulation
Up n’ Free®: a gait trainer that provides an adjustable degree of dynamic partial body weight support
Anterior rollator walker: wheeled mobility device, typically with weight bearing on the hands but available with forearm weight bearing
Contact Guard – therapist provides physical contact but no assistance
Minimal assistance – therapist provides less than 25% of work to complete the task
Moderate assistance – therapist provides 25%–50% of work to complete the task
Maximal assistance – therapist provides 50%–75% of work to complete the task
Day hospital – Frequency 5 times a week PT and OT each for 60 min with patient being transported to the hospital by the parent daily an residing in the home with the parent responsible for carrying out supportive care including night splints.
Inpatient rehabilitation – 7 day a week PT and OT program with 90 min of each therapy Monday through Friday and both PT and OT on the weekend, 45min each both Saturday and Sunday.