
Abstract
Background:
Duchenne muscular dystrophy (DMD) is characterized by progressive cardiomyopathy. Left ventricular (LV) function may worsen by factors increasing LV afterload such as hypertension and obesity.
Objective:
To identify potential modifiable risk factors for progression of cardiomyopathy in Duchenne muscular dystrophy (DMD).
Methods:
We retrospectively analysed systolic blood pressures (SBP) and body-mass indexes (BMI) from 273 visits of 65 DMD patients aged 4–18 years between 2003 and 2016, divided in 14 age groups. Values were normalized using Z-scores (Z-SBP and Z-BMI). A linear mixed model was used to analyse correlations between Z-SBP and BMI, steroid use, age, ambulatory status and cardiac medication (CM) use. To study the relationship between SBP and BMI and myocardial deformation prior to the onset of clinical cardiomyopathy, LV deformation, defined by global longitudinal strain (GLS), was quantified in a subset of 36 patients <11 years. Multiple linear regression was used to study the relation between GLS and clinical parameters.
Results:
Median follow-up was 5 years. SBP was significantly elevated in all age groups under 14 years (p≤0.04) and 15–16 years (p = 0.033) and correlated positively with BMI (p = 0.001) and negatively with CM use over time (p = 0.018). Z-BMI followed a bell-shaped distribution and plotted approximately one standard deviation above the mean in patients between 7 and 15 years. In the subset of younger patients, reduced GLS was associated with higher BMI (β= 0.348, p = 0.004).
Conclusions:
SBP and BMI may be potentially modifiable factors to retard deterioration of LV function in DMD.
Keywords
INTRODUCTION
Duchenne muscular dystrophy (DMD) is an X-linked recessive neuromuscular disorder caused by mutations in the gene encoding dystrophin, critical for stabilization of striated muscle membranes [1]. Its absence leads to progressive weakness in skeletal muscle while cardiac loss of dystrophin results in dilated cardiomyopathy. Patients with DMD have a reduced life expectancy, with heart failure due to dilated cardiomyopathy as the main cause of death [2, 3].
Cardiomyopathy in DMD is characterized by progressive fibrosis in the left ventricle (LV) leading to LV dysfunction and dilatation [2]. Echocardiographic signs of cardiac dysfunction start in the second decade of life and are almost universally present in adults [4]. However, research into identifying additional, potential modifiable risk factors for progression of cardiomyopathy is limited. Studies in mdx mice, a mouse-model of DMD, indicate that dystrophin-lacking myocardium is more vulnerable to pressure overload of the LV than normal myocardium [5]. Increased LV afterload may pose the already vulnerable myocardium of DMD patients at risk for accelerated myocardial dysfunction.
LV afterload is influenced by hypertension, obesity and aortic stiffness [6]. Presence of these factors has been shown to increase risk for LV dysfunction in adults and children without DMD [7, 8]. Obesity is frequently encountered in DMD due to use of corticosteroids and lack of mobility [9]. Prevalence of obesity has been described up to 73% in steroid-native DMD patients <13 years [10] and higher BMI was associated with longer duration and higher cumulative dose in ambulant DMD patients using prednisone [11].
In turn, obesity and chronic steroid use can induce hypertension, but detailed longitudinal data on blood pressure values in DMD patients are lacking.
Ventricular function can be studied in detail with two-dimensional speckle-tracking echocardiography (STE), through quantification of the global longitudinal strain (GLS of the myocardium representing LV deformation. STE can show subclinical LV dysfunction while conventional echocardiographic measures, such as shortening fraction (SF) and ejection (EF), are still preserved [12]. A less negative, more abnormal, LV GLS has been associated with the presence of afterload increasing factors in pediatric patients [13, 14]. However, no studies on this subject have been performed in DMD.
Thus, several LV afterload increasing factors are present in DMD patients, and may aggravate the formation of myocardial fibrosis of the LV, leading to accelerated myocardial dysfunction. Therefore, we examined the distribution of blood pressure values during follow-up in pediatric DMD patients and determined the prevalence of hypertension in different age-groups. Next, we investigated the longitudinal relations between blood pressure, body mass index (BMI) and medication use. Finally, we correlated these variables to myocardial deformation assessed by STE in a subgroup of patients prior to the onset of clinical cardiomyopathy.
METHODS
We conducted a retrospective review study of medical records of all DMD patients who annually visited the pediatric outpatient neuromuscular clinic of the Leiden University Medical Center (LUMC) between February 2002 and December 2016. Diagnosis had been confirmed by genetic mutational analysis in all subjects. Ethical approval was obtained from the LUMC review board and informed consent was waved by the ethical committee.
Clinical data abstraction
Serial measures of age, height, weight, blood pressure (BP), heart rate (HR), ambulatory status, steroid use (type, regimen, duration), and use of cardiac medication (CM). Height had been measured using a wall-mounted stadiometer (Seca) until boys were unable to stand. Either ulna length (XSENS MVN Segometer) [15] or arm span was used to calculate height hereafter. Weight had been measured using an electronic scale (Terraillon) or patient hoist (Arjohuntleigh) when boys lost ambulation. BMI was calculated as kilograms/squared meters. Seated blood pressure had been recorded by an experienced nurse using an automatic device (Philips Sure Signs VS 3) on the right arm with an appropriate sized cuff. Age-, sex-, and height-specific z-scores were calculated for systolic blood pressure (Z-SBP) and diastolic blood pressure (Z-DBP) based on the 4th report criteria of the National High Blood Pressure Education Program Working Group [16] to compare the data to pediatric reference values. Hypertension was defined as SBP/DBP z-score≥1.65 (equivalent to the 95th percentile). Z-SBP/Z-DBP scores were divided in 14 subgroups according to age at measurement (from 4–5 to 17–18 years) to determine mean blood pressure per age group. Matching BMI measures were converted to BMI Z-scores (Z-BMI) based on values of Centers For Disease Control [17]. Obesity was defined as z-score≥1.65 (equivalent to the 95th percentile). One measure per patient was allocated for analysis within each year with an interval of at least 10 months.
Myocardial deformation analysis in younger patients
To study the association between early myocardial deformation and factors influencing LV afterload prior to the onset of clinical cardiomyopathy, we included patients younger than 11 years who did not use CM. LV peak systolic GLS was assessed using STE (GE Medical Systems EchoPAC version 201) in previously recorded transthoracic echocardiograms. All echocardiograms had been performed in supine position using a commercially available system equipped with a 3.5 MHz transducer (Vivid 7 or 9, GE Vingmed Ultrasound AS, Horten, Norway). M Mode SF was measured in the parasternal long-axis view according to standards of American Society of Echocardiography [18] to assess global cardiac systolic function.
For assessment of peak systolic GLS, the endocardial border of the LV was traced manually in the parasternal apical 4-chamber view by one investigator. A single cardiac beat with the best quality was used. Tracking was automatically performed by the software. Analysis was accepted after visual inspection, and when the software had indicated adequate tracking. In some cases, the endocardial border was manually modified to achieve optimal tracking. If adequate tracking was not achieved within two attempts, the patient was excluded from analysis. The software divided the myocardium into six segments (the septum and lateral border where each divided into basal, mid and apical segments). GLS was calculated as average of segments when at least five segments were available. Patients were divided in two groups based on age (until 9 years and 10–11 years) to compare means to age-matching values for six-segments based GLS published in a recent meta-analysis by Levy et al. [19].
Statistical analysis
The Shapiro-Wilk test was used to assess normality of data. Results are displayed as mean (SD) or median (interquartile range) for non-normally distributed continuous variables. Categorical variables are reported as frequency (percentage). Means were compared with one sample t-test. For longitudinal blood pressure study, data were analyzed using a linear mixed model. Separate models were run for Z-SBP and Z-DBP. Age was divided in yearly categories and added as fixed factor. Also, BMI was added as a covariate to the model. Additional factors in the model were steroid use, ambulatory status and use of cardiac medication. A participant level random effect was included to account for within-subject dependence due to repeated measurements. Standard multiple regression was used to assess the relation between peak systolic GLS BMI, SBP, age and years on steroids, adjusted for HR as potential confounder. Analyses were conducted using SPSS 23.0 (IBM, Inc). Significance was set at two-sided P≤0.05 for all tests.
RESULTS
Patient characteristics
Data from 67 patients with 303 visits were collected. Two patients were excluded due to missing data at all 3 (0.9%) available visits. Twenty-six (8.5%) encounters from 15 other patients were excluded to due missing data, providing a total of 273 visits from 65 patients for longitudinal analysis. Median follow-up time was 5 years (range 1–12). Mean age at loss of ambulation was 10.4 (±1.9) years. Mean starting age of steroids was 5.6 years (IQR 5.0–6.8). Fifty-three patients (97%) were on intermittent corticosteroid regime (10 days off/10 days on) during follow-up while one patient used steroids every other day, and one patient was on daily regime. Six patients had never used steroids, two had stopped for≥2 years, and two patients had stopped for 3–5 months at included encounters. To provide more detailed information of steroid use at included blood pressure measurements, assessments of patients were divided into age <5 and≥5 years. Out of the 11 assessments of patients aged <5 years, one (9.1%) was while using prednisone. Ambulant patients aged≥5 years used steroids in 83.0% of the 141 encounters (85.5% prednisone, remaining deflazacort). Non-ambulant patients aged≥5 years used steroids in 72.7% of the 139 visits (75.8% prednisone, remaining deflazacort). Out of the 273 visits, 44 (16.1%) were with use of cardiac medication. 34 of these were with concomitant steroid use. All patients used angiotensin-converting enzyme inhibitors (ACEi), and one patient also used a diuretic and β-blocker. Mean starting age of cardiac medication was 13.6 (±1.9) years. Demographic data of subgroup of young patients included in the cross-sectional STE study is shown in Table 1.
Demographic data
*Applies to all outcome measures, unless otherwise indicated. Data expressed as Mean (SD), Median (IQR) or frequency (percentage). Hypertension was defined as Z≥1.65. Abbreviations: y, years; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; SF, shortening fraction.
Blood pressure and BMI in DMD patients
Figure 1A illustrates the mean Z-SBP/DBP per age group. Mean Z-SBP was significantly elevated in all age groups under 14 years (p≤0.04), and in patients between 15 and 16 years (p = 0.033) compared to an expected mean Z-score of zero. See Supplementary Table 1 for age group specific outcome of mixed model analysis. Mean Z-DBP was only significantly increased in young patients aged≤7 years (p≤0.005) and 9–10 years (p = 0.019), and declined with aging of patients (Supplementary Table 2). The percentage of systolic blood pressure measurements meeting the criteria for hypertension ranged between 22–39% from 4 until 16 years of age. Patients aged 16 and 17 years had systolic hypertension in 17% and 0% of the measurements respectively, see Fig. 1B. Average Z-BMI per age group followed a bell-shaped curve and plotted a mean of Z = –0.102 at 4–5 years to Z = 0.146 at 17–18 years of age (Fig. 2). In general, the prevalence of obesity increased from lower age groups to the middle age groups, reaching up to 43% in age groups 12–13 and 13–14.
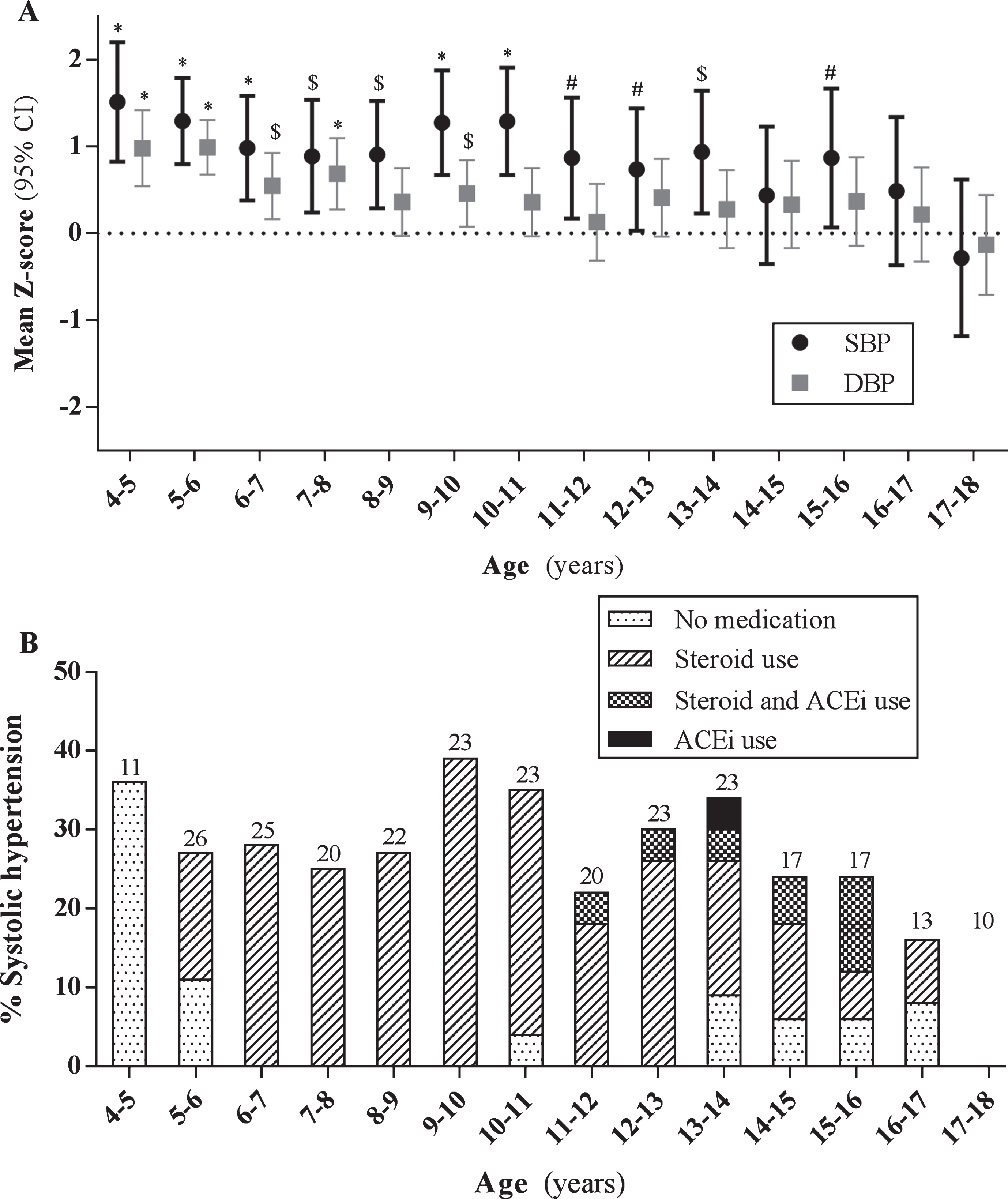
Longitudinal mean systolic and diastolic blood pressure per age group. (A) Mean (95% Confidence Interval, CI) blood pressure Z-score per age group. SBP; systolic blood pressure, DBP; diastolic blood pressure. Mean BP were adjusted for BMI, use of steroids and cardiac medication. Dotted line represents 50th percentile for BP. # p≤0.05, $ p≤0.01, *p≤0.001. (B) Percentage of systolic hypertensive measurements (Z≥1.65) per age group. Different filling patterns in bars represent measures with no medication, steroid use, steroid and angiotensin converting enzyme-inhibitor (ACEi) use and only ACEi use. Numbers above bars indicate total of BP measures in age group.
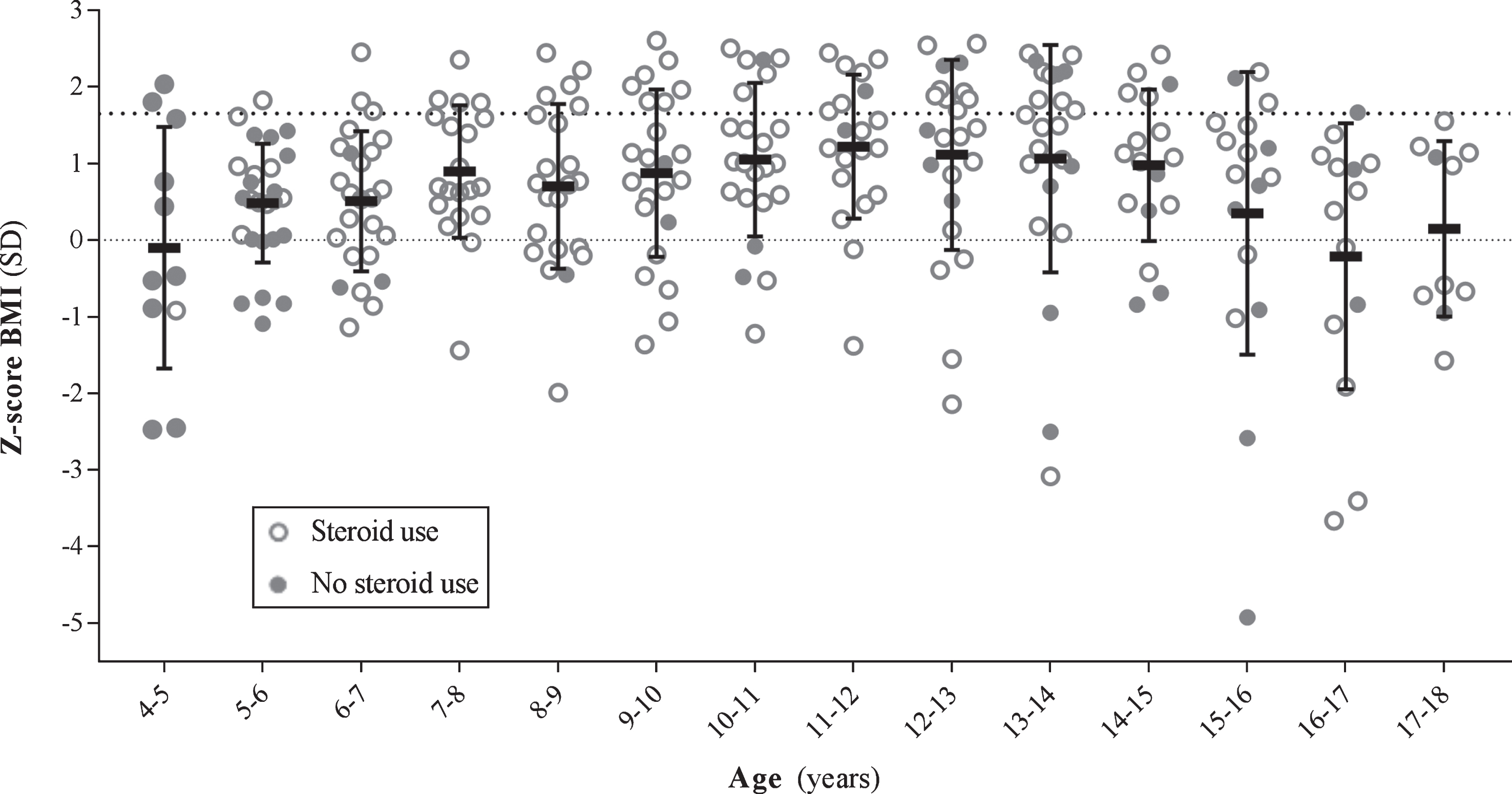
Body mass index measures per age group. Each dot represents one measurement of one patient (open dots: steroid use, closed dots: no steroid use). The densely dotted line at Z = 0 is the expected mean compared to overall pediatric population. Obesity was defined at Z≥1.65 (loosely dotted line). Mean (standard deviation, SD) body mass index Z-score per age group. BMI; body mass index.
Longitudinal blood pressure analysis
Z-SBP and Z-DBP were modelled as a function of age, with adjustment for BMI, steroid use, ambulatory status and use of cardiac medication. Longitudinal Z-SBP increased significantly with higher BMI (β 0.07 [95% CI 0.03; 0.11], p = 0.001) and decreased with use of heart medication (β –0.67 [95% CI –1.22; –0.12], p = 0.018). Use of steroids (p = 0.134) and loss of ambulance (p = 0.339) were no significant determinants of Z-SBP over time. Longitudinal Z-DBP correlated positively with BMI (β 0.05 [95% CI 0.03; 0.08], p = 0.000), but not with use of steroids (p = 0.151), use of cardiac medication (p = 0.257), and loss of ambulance (p = 0.515).
Myocardial deformation analysis
For the subgroup analysis, we assessed myocardial longitudinal deformation in 36 patients <11 years of age. Median age of this cohort was 8.9 years (IQR 6.8–10.1). No patients had clinical symptoms of heart failure. Echocardiographic signs of cardiomyopathy (SF < 28%) were present in one (2.8%) patient, in whom cardiac medication was started after this visit.
One patient was excluded to due inadequate tracking. Median frame rate was 56 frames/second (IQR 53–70). Among 216 analysed segments, strain could not be obtained in four (1.4%). Mean peak systolic GLS of the whole cohort was –18.6% (3.1). Mean GLS of 23 patients aged≤9 years (–19.5% (2.6), p = 0.013) and 13 patients aged 10–11 years (–17.1% (3.3), p = 0.003) were significantly lower than the mean GLS of a pediatric reference cohort [19] (–21.0% and –20.5% respectively). In the multiple regression model, reduced peak systolic GLS was associated with increased BMI (p = 0.004), but not with other predictors (Table 2). Adjustment for HR did not affect the association between BMI and peak systolic GLS.
Association between GLS and parameters using multivariate regression adjusted for HR
Abbreviations: GLS, global longitudinal strain; HR, heart rate; y, years; BMI, body mass index; SBP, systolic blood pressure.
DISCUSSION
In this study, mean systolic blood pressure was significantly elevated in the majority of pediatric DMD patients. The percentage of systolic hypertension measurements varied between 22% and 39% from 4 until 16 years of age. Systolic blood pressure was lower in patients on CM. During follow up, systolic and diastolic blood pressure increased with higher BMI, whereas steroid use was not an independent determinant of blood pressure in patients with DMD in the linear mixed model. Subsequently, increased BMI, but not systolic blood pressure, was related to early myocardial deformation defined by peak systolic GLS in young DMD patients < 11 years of age. The results of this study suggest that factors influencing afterload, such as increased blood pressure and BMI, may play a role in the deterioration of cardiac function in DMD.
A number of studies have published cross-sectional data on the prevalence of hypertension in DMD [20–22], but none describe detailed prevalence per year of age. Wong et al. reported that 25.5% of patients on daily steroids aged 10–13 years had systolic hypertension which is comparable to 28.3% in our cohort [20]. In patients aged 13–16 years, they reported systolic hypertension in 10.3% of patients which is lower than 27% in the present study. Ricotti et al. [21] found hypertension in 5% of the patients aged 3–15 years on intermittent steroids while in a study by Braat et al 45% of the patients had hypertension [22]. One study described a correlation between low BP and younger age in DMD with ethnicity (Hispanic origin) as a contributing factor [23]. However, the mean age of that cohort was 15.9±8.2 years compared to 10.4±3.7 years in our cohort and analysis did not take repeated measures into account. In the cohort described here, no patients were from Hispanic origin.
Increased blood pressure is a well-known side effect of treatment with corticosteroids [24]. Use of corticosteroids has led to prolongation of the ambulant phase in DMD by approximately 3 years [25]. It has also been associated with a delayed onset of DMD-related cardiomyopathy [26, 27]. Corticosteroid treatment is thus an essential part of the standards of care in DMD and is recommended from the age of 4 to 5 years onward. An extensive study comparing longitudinal blood pressure values in DMD patients with and without steroids will therefore not be feasible, and the high percentage of patients on steroids in this study may well be the reason that steroid use was not an independent factor in the linear mixed model. However, 36% of the measurements in the youngest age group (4–5 years) of our cohort were compatible with hypertension while none of these patients used steroids. This suggest that blood pressure may be also influenced by dystrophin deficiency itself. Several studies have demonstrated that cardiac autonomic dysfunction in DMD may be associated with impaired parasympathetic activity, leading to a predominance of sympathetic activity with subsequent higher blood pressure [28]. Another mechanism may be increased peripheral vasoconstriction and dysregulated blood flow of skeletal muscle by neuronal nitric oxide synthase deficiency, as shown in DMD animal models [29, 30].
Longstanding hypertension correlated with decreased strain values in adults [31]. In DMD, treatment with ACEi lowers blood pressure and is the first-line treatment for cardiomyopathy in DMD [32]. Until recently, treatment was initiated upon the first echocardiographic signs of reduced cardiac function [33]. Recent studies have shown that preventive treatment with ACEi in the absence of clinical systolic dysfunction attenuates the progression of left ventricular dysfunction [34, 35], possibly through afterload reduction [34]. Treatment with ACEi is now recommended at the age of 10 years irrespective of cardiac function [32]. However, it is not directed towards the lowering of blood pressure per se. We did not find a significant association between blood pressure and GLS in the younger children with DMD. Thus, mild increases in afterload caused by high blood pressure may not affect LV function in an early stadium, but only after long-term exposure.
BMI was the only independent determinant in this study, related to both increased SBP in the whole cohort, and to decreased GLS in the DMD patients <11 years. Although BMI too may be influenced by steroid use, obesity has already been described in 73% of the DMD patients under 13 years of age prior to the introduction of steroids as standard treatment [10]. Overall, the prevalence of obesity in our cohort increased in patients up to 43% in patients aged 12–14 years, which is comparable to results described by Davidson [9]. Obesity is associated with systolic hypertension in around 35% of obese children [36]. Several studies have evaluated the effect of increased weight on left ventricular function in children without signs of clinical cardiomyopathy and demonstrated reduced longitudinal systolic strain in obese children compared to non-obese children [14, 37–39]. The relationship between higher BMI and reduced GLS in our study suggests that increased BMI may exert an early, negative, effect on left ventricular function in DMD children as well. BMI may therefore be an important modifiable factor in the deterioration of cardiac function in DMD.
Our study was limited by its retrospective design. Blood pressure measurements were taken only once and therefore the definite diagnosis of hypertension could not be established retrospectively. Additionally, single blood pressure measurements may be influenced by stress-related factors and position of body while blood pressure was taken. BMI measurements of the non-ambulant patients may have been influenced by the less accurate measurements of height, but this is inherent to studies including non-ambulant DMD patients. STE-derived longitudinal deformation was only assessed cross-sectionally in a relatively small subgroup of patients. We opted for this approach to rule out bias from use of CM, reduced echocardiographic window due to scoliosis and obesity and less accurate BMI measurements in non-ambulant patients.
In conclusion, mean Z-SBP was elevated in the majority of pediatric DMD patients in this retrospective study. During follow-up, BP increased with higher BMI in patients <18 years of age, and higher BMI was also associated with reduced peak systolic GLS in DMD patients <11 years of age. Thus, increased BMI, and possibly increased blood pressure, may lead to an accelerated decline in LV function of DMD patients. Long-term use of steroids also leads to an increase in BMI, and BMI itself is associated with hypertension in non-DMD patients. Steroids may thus exert their effect on blood pressure indirectly by increasing BMI. Therefore, the etiology and interaction between these factors and the role of dystrophin deficiency itself remain to be determined. Prospective studies using standardized assessment of blood pressure are needed to confirm our findings and to determine if blood pressure and BMI are modifiable risk factors for the progression of cardiomyopathy in DMD.
CONFLICT OF INTEREST
EHN reports grants from Spieren voor Spieren, Duchenne Parent Project, ZonMW and AFM, and was local PI in studies conducted by BioMarin, GSK, Lilly, Santhera, Italfarmaco, and Roche outside the submitted work. He also reports consultancies for BioMarin and Summit. All reimbursements were received by the LUMC. No personal financial benefits were received. No conflicts of interest exist with the submitted work from any of the authors.