
Abstract
Background:
In boys with Duchenne muscular dystrophy (DMD), loss of upper limb function becomes more evident after the onset of wheelchair-dependency, because of the inability to lift the arms against gravity. With an increasing population of older wheelchair-dependent boys with DMD it is worthwhile to know whether training can delay the loss of upper limb functions. Dynamic arm supports may enable boys with impaired arm function to train their muscles without becoming exhausted by providing external mechanical compensation for muscle weakness.
Objective:
This study investigated the effect of gravity-compensated 3D-training for the arms on the functional abilities in boys with DMD.
Methods:
An explorative RCT was conducted among boys with DMD with impaired arm function (n = 16). Boys in the intervention group (n = 7) trained their arms by playing virtual reality games while using dynamic arm support during 20 weeks. The primary endpoint was the difference in change in Performance of the Upper Limb (PUL) score between the intervention and control group (n = 9) after 20 weeks. Secondary outcome measures were at the different ICF-CY levels.
Results:
No significant group differences were found for the PUL. Elbow range of motion (p = 0.018) and extension strength (p = 0.038) improved in the intervention group and worsened in the control group.
Conclusions:
Although this study did not show a significant effect of training on the primary outcome measure, there are indications that training may decline the loss of range of motion and strength. This may prolong the functional abilities on long-term.
Trial registration:
Netherlands Trial Register 3857.
Keywords
ABBREVIATIONS
INTRODUCTION
Duchenne muscular dystrophy (DMD) is a progressive neuromuscular disorder affecting 1/5000 live-born boys [1]. Boys with DMD have muscle fibers that are prone to contraction-induced damage because of the absence of the protein dystrophin [2]. The absence of dystrophin leads to ongoing cycles of degeneration and regeneration, resulting in chronic inflammation, impaired muscle tissue repair and replacements of muscle fiber by fat and connective tissue [3]. The clinical course of DMD is characterized by a loss of muscle strength, resulting in wheelchair-dependency at a mean age of ten years without treatment with corticosteroids [4]. Long-term use of corticosteroid has shown to delay loss of ambulation, preserve respiratory and upper limb function and avoid scoliosis surgery [5]. Recent studies also show benefits from starting corticosteroids before significant decline occurs [6, 7]. Symptomatic treatments, in particular respiratory ventilation, have extended the life expectancy of boys with DMD to the early thirties [8, 9]. Although disease modifying drugs slowly become available, there is no cure yet [10].
Regular (gentle) submaximum functional activities or exercises are recommended to avoid disuse atrophy and other secondary complications of physical inactivity in ambulatory and recently wheelchair-dependent boys with DMD [11]. These exercise recommendations are mainly based on the pathophysiology and on training studies in mice-models for DMD [12–14]. The recommendations are confirmed by the results of two randomized controlled trials (RCT’s) showing that (motor-assisted) bicycle training for the legs and/or arms can delay the loss of functional abilities in ambulatory and recently wheelchair-dependent boys with DMD [14–16]. Older studies, in which participants were not randomly allocated to groups, also concluded that submaximal resistance exercises do not cause any harm in ambulant boys and may have limited positive effects on muscle strength [17–19]. Exhausting high-load resistance and eccentric exercises should be avoided, because they cause damage to the stretched sarcomeres, resulting in a loss of force-regenerating capacity and a subsequent fiber degeneration [20, 21].
With an increasing population of older wheelchair-dependent boys and men with DMD, it is worthwhile to know whether physical training can delay the loss of upper limb functions in this population as well. Upper limb functions such as reaching are decreasing soon after the onset of wheelchair-dependency, because of the inability to lift the arms against gravity [22]. Simultaneously, elbow flexion and pronation contractures develop which further accelerate the loss of activities of daily life (ADL) such as eating. The loss of ADL’s may be compensated by innovative dynamic arm supports that are now being developed. Dynamic arm supports provide external mechanical compensation for muscle weakness of the upper arm and shoulder and increase active joint range of motion [23, 24]. The results of a recently published feasibility study indicate that boys with DMD can safely train their arms with dynamic arm support [25]. However, to make optimal use of these modern dynamic arm supports, boys with DMD should maintain optimal joint mobility and muscle elasticity.
As we expect that assisted physical training can delay the functional deterioration and development of joint contractures in boys with DMD who have difficulties with lifting their arms against gravity, we developed the Gainboy® study: a virtual reality computer gaming training program for the upper limb with dynamic arm support. There are indications that playing a virtual reality game while using dynamic arm support slows the loss of arm functions [25]. A virtual reality game is attractive for children and challenges participants to move their arms in three dimensions and can be played at home. The assistance provided by the dynamic arm support reduces the work-load and enables boys with severe muscle weakness to train their muscles without becoming exhausted. According to the task-oriented approach of motor learning, training in a virtual reality environment can be even more functional than the standard low-resistance (bicycle) exercises that often focus on training isolated muscles rather than movements [26]. In the Gainboy® study we intended to challenge the boys to move their arms in 3D and preserve joint motion and muscle elasticity, consequently leading to preservation of functional abilities in the arms. The aim of this study was to investigate the effectiveness of virtual reality computer gaming with dynamic arm support on the functional abilities of the upper limb.
MATERIALS AND METHODS
Design
An explorative RCT was conducted between January 2014 and June 2016 (Fig. 1). Two weeks after the screening assessment to become familiar with the clinical tests and to gain information about test-retest reliability, participants had their baseline assessments (T0). At T0, the intervention group started with their training program, while the control group received usual care (no specific intervention) for 20 weeks. Two assessments were conducted during this period; after 10 (T1) and 20 weeks (T2, primary endpoint), with a 10 week follow-up period (T3). After this period, the control group trained for 20 weeks. Primarily to allow these participants to train as well, but also to allow us to do within-subject analysis. One assessment was done 20 weeks after T3 (T4). This study has been approved by the Medical Ethics Committee Arnhem-Nijmegen, the Netherlands (2012/390).
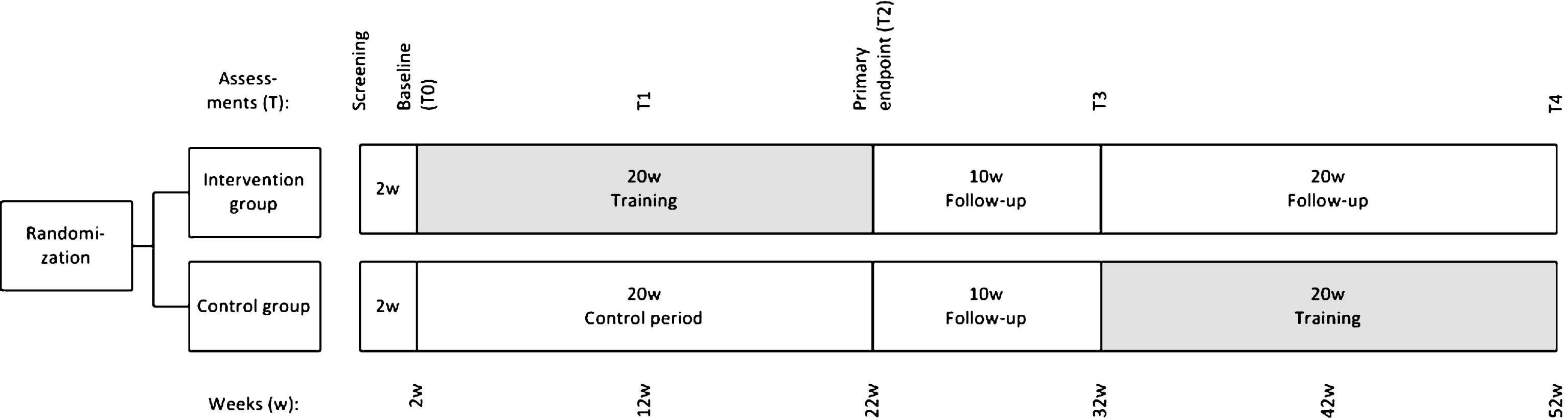
A schematic overview of the study design.
Participants
Eligible participants were ambulatory and wheelchair-dependent boys with DMD. Inclusion criteria were a DNA-established diagnosis of DMD and an impaired arm function (able to raise arms above head only by flexing the elbow or using accessory muscles during 10 repetitions, or; unable to raise hand above head, but can raise an 8-oz glass of water to the mouth, or; able to raise both hands to the mouth, but cannot raise an 8-oz glass of water to the mouth). Exclusion criteria were age <7 years old, able to raise both arms 10 times above the head without elbow flexion or using accessory muscles, presence of other disabling diseases influencing mobility, a clinical symptomatic cardiomyopathy, unable to bring the hands to the mouth and participation in another clinical trial that aims to delay the physical deterioration. We aimed to include 20 to 30 eligble boys in this explorative study. This sample size seemed appropriate for an explorative study and was not based on a sample size calculation. The average rate of decline was not known for the primary outcome measure at the start of this study (2014). Parents and boys ≥12 years provided written informed consent.
Randomization and blinding
Participants were randomly allocated by computer randomization by a coach (YvE) [27]. Randomization was stratified according to upper limb capacity (able to bring hands above head with compensation versus unable to bring hands above head). Participants were not blinded to treatment allocation, but had no information about previous test results during each assessment. The clinical evaluators (MJ and LH) were blinded to treatment allocation.
Intervention
The gravity-compensated 3D-training for the arms consisted of 5 sessions per week of 15 minutes during 20 weeks. Literature shows improvements of muscle functions induced by training can be seen after six weeks of physical training [28]. However, to also aim at reducing disuse and because the training effect over time is expected to be small, a longer training period was chosen. Participants practiced reaching and lifting exercises with their arms by playing virtual-reality computer games (Playstation II, Sony) while using dynamic arm support (Gainboy®, Focal Meditech B.V., Tilburg, The Netherlands), see Fig. 2. They were allowed to move their arms over the full range of motion which may cause a feeling of stretch but not pain.
The set-up of the Gainboy®.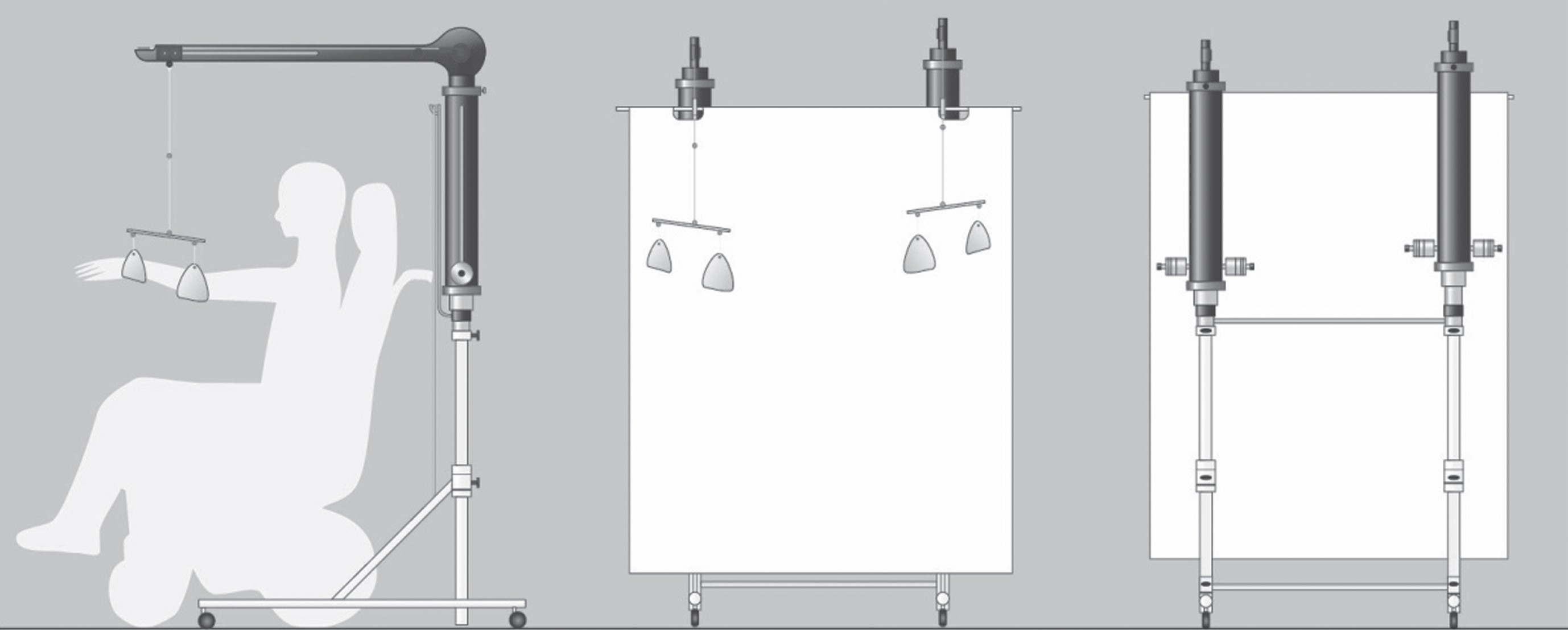
Virtual-reality computer games
The Playsation II is a video game console that works with a standard television and a digital camera (EyeToy) (https://www.playstation.com/en-us/games/eyetoy-play-2-with-camera-ps2/). The EyeToy recorded the participant and projected a virtual image of the arms of the participant on the television screen. This allowed them to interact with a virtual reality environment by capturing movements of arms and hands. Participants were instructed to play the first 10 minutes of each training session one or more of the following games of EyeToy Play 1: Kung Foo, Wishi washi, Keep ups, Plate spinner, Ghost catcher, Mirror time, Rocket rumble and Beat freak. During the last 5 minutes participants were free to choose any game of EyeToy Play 1, Play 2 or Play sports to make training more attractive.
Dynamic arm support
The Gainboy® provided a constant amount of gravity compensation during 3D arm movements by means of two overhead slings (suspension type arm support) mounted on a moveable frame, see Fig. 2 (http://www.focalmeditech.nl/nl/content/gainboy). Each sling supported one arm at the elbow and wrist. Counterweights make the arms of the user virtually weightless. In this study, the amount of gravity compensation was approximately 100% in the horizontal plane (90° shoulder anteflexion, elbow extended). To ensure optimal horizontal movement, the amount of counterweight was adjusted for each participant. Participants with relatively good arm function started with no counterweight, whereas participants with decreased arm function started with sufficient counterweight to enable them to lift their arms. The mean resistance of a balanced device to move in down- or upward direction is 153 gram (SD = 12). The distance from the television depended on the joint range of motion of the participant.
Supervision
Participants trained independently at home, but were supervised by a coach (YvE). The coach visited the participants at the start of the intervention and after ten weeks of training. The control group did not meet with the coach during the control period. Therapy burden (e.g. pain and fatigue) and compliance were evaluated by the coach every two weeks with a questionnaire, an OMNI score for perceived exertion, and a training diary. If any problems were monitored, the coach adapted the training intensity and/or contacted the principal investigator (IdG).
Co-interventions
The 3D-training for the arms was additional to any other types of regular therapy (e.g. physical therapy and corticosteroids) or daily physical activity (e.g. wheelchair-hockey and swimming). Allco-interventions were registered.
Outcome measures
Body weight, height, medication use, physical therapy, sport participation and Vignos and Brooke grades for lower and upper extremity functioning were registered during each visit [28]. The duration of corticosteroid use was not accounted for. Outcome measures included assessments at the levels of the International Classification of Functioning, Disability and Health for Children and Youth, see Table 1 [30]. The primary outcome measure was the Performance of the Upper Limb module for DMD (PUL) [31]. The PUL assesses upper limb function and consists of an entry item (instruction: “Lift your arm as high as you can”, ranging from score 0: “No useful function of hands” to 6: “Can abduct arms above head without compensation”) and 21 items in 3 dimensions: 1) high shoulder level (4 items, score = 0–16), 2) mid-elbow level (9 items, score = 0–32), and 3) distal wrist and hand dimension (8 items, score 0–24). The total PUL score was calculated (score range = 0–72, excluding the entry item) and sum scores were calculated for each dimension separately.
Outcome measures
At T0 and T2.
At t2 and T4. Abbreviations: PUL, Performance of Upper Limb; HHD, hand held dynamometer; MVC, maximal voluntary contraction; ROM, active joint range of motion; QMUS, Quantitative Muscle Ultrasound; A6MCT, Assisted Six Minute Cycle Test; MFM, Motor Function Measure.
Secondary outcome measures were muscle strength, active range of motion, quantitative muscle ultrasound (QMUS), the Assisted 6-Minute Cycle Test (A6MCT), the Motor Function Measure - dimension 3 “Distal Motor Function” (MFM), the Abilhand-plus, the Kidscreen-52 dimension “Physical well-being” and the Global Health Question [32–34, 39]. Muscle strength (lbs) of the deltoid, triceps and biceps muscles of both arms was measured with a hand held dynamometer (HHD). Participants were to push as hard as possible during 3 seconds. The highest score of 3 attempts was used for analysis. Additionally, participants performed maximum voluntary isometric contractions (MVC) using a static frame myomometer (consisting of a KAP-E Force Transducer, measurement range 0.2 –2000N (Angewandte System Technik, Dresden, Germany) and a height and position adjustable frame (at baseline and T2). The MVC was quantified for the deltoid, pectoralis major, trapezius, biceps brachii, triceps brachii, the wrist flexors and extensors and a total score (shoulder, elbow and wrist). A 3D movement analysis was used to determine the active range of motion (at baseline and T2). The analysis was performed with an 8 camera VICON motion analysis system (Oxford Metrics, Oxford UK). Participants performed active movements 3 times at a controlled velocity. The maximal active joint angles were determined for the shoulder (sum of shoulder abduction, -adduction and -flexion), the elbow (sum elbow flexion and extension, pro- and supination of the lower arm), the wrist (sum of wrist flexion, extension, ulnar and radial deviation), and a total range of motion (sum of shoulder, elbow and wrist). QMUS was used to calculate the echo intensity (EI) of the biceps brachii, the wrist flexors, the rectus femoris, and the tibialis anterior. The EI is a gray value quantified by a histogram-based analysis that shows the infiltration of connective tissue and fat. In boys with DMD, muscle EI increases with age and disease severity [35]. EIs were expressed as z-scores (ie, the number of SD from the mean of the reference group) and were then integrated in a total sum score, and a sum score for the lower and upper limb. At T2 and T4, we used a global health question: “Think about the last six months. Do you think your health has been improved, a little bit improved, not improved but also not decreased, a little bit decreased, or decreased?”.
Statistical analysis
The primary endpoint was the mean change in motor function from baseline (T0) at week 2 to T2 at week 22 (primary endpoint) assessed with the PUL [36]. Results of the intervention and control group were compared with an independent t-test.
The difference in change from T0 to T2, between intervention and control group was also assessed for the secondary study outcome measures with a parametric independent t-test or a non-parametric Mann-Whitney U test.
Within-subject analysis was used to determine the training effect of the control group (the change in the training period (T4-T3) and the control period (T2 vs. T0)).
For test-retest reliability of the outcome measures, we performed paired t-test between screening and baseline (T0) and calculated the intraclass correlation coefficients (ICC) using a two-way random model and absolute agreements (supplementary material 1). ICCs above 0.7 were considered acceptable (0.70 to 0.79 reflect good reliability, >0.80 reflect excellent reliability). Items of the PUL were converted to weighted scores, to ensure all items were of equal importance to the total score. No significant differences were found between screening and baseline for the outcome measures, except for shoulder abduction right (measured with the HHD) (p = 0.016), the Abilhand questionnaire (parent version) (p = 0.037) and the z score of the echo of the biceps (p = 0.028). The total score of the PUL, the shoulder dimension of the PUL, the elbow dimension of the PUL and HHD showed excellent test-retest reliability (ICCs ≥0.80). TheA6MCT and the Abilhand children showed good to excellent reliability (ICCs 0.73 and 0.79, respectively). ICCs of the hand dimension of the PUL, echo intensity, the MFM and the Kidscreen (children and parents) were <0.70.
Participants were analyzed as-treated, i.e. participants who were randomized to the study and do not have major protocol deviations. Statistical analysis were performed using SPSS (SPSS Inc., Chicago, IL, USA) with a significance level set at p < 0.05.
RESULTS
Participant flow through the study and characteristics
Figure 3 shows the participant flow through the study. Of the 9 boys who were allocated to the intervention group, 7 boys completed the training and follow-up period. One boy stopped before the screening measurement because of the burden of participation (travelling to study location). The other boy was lost to follow-up immediately after the baseline measurement due to an unplanned holiday for several months. Both boys were excluded from analysis. Ten boys were allocated to the control group, of whom, 9 completed the control period. One boy stopped before screening, because of the burden of participation and he was excluded.
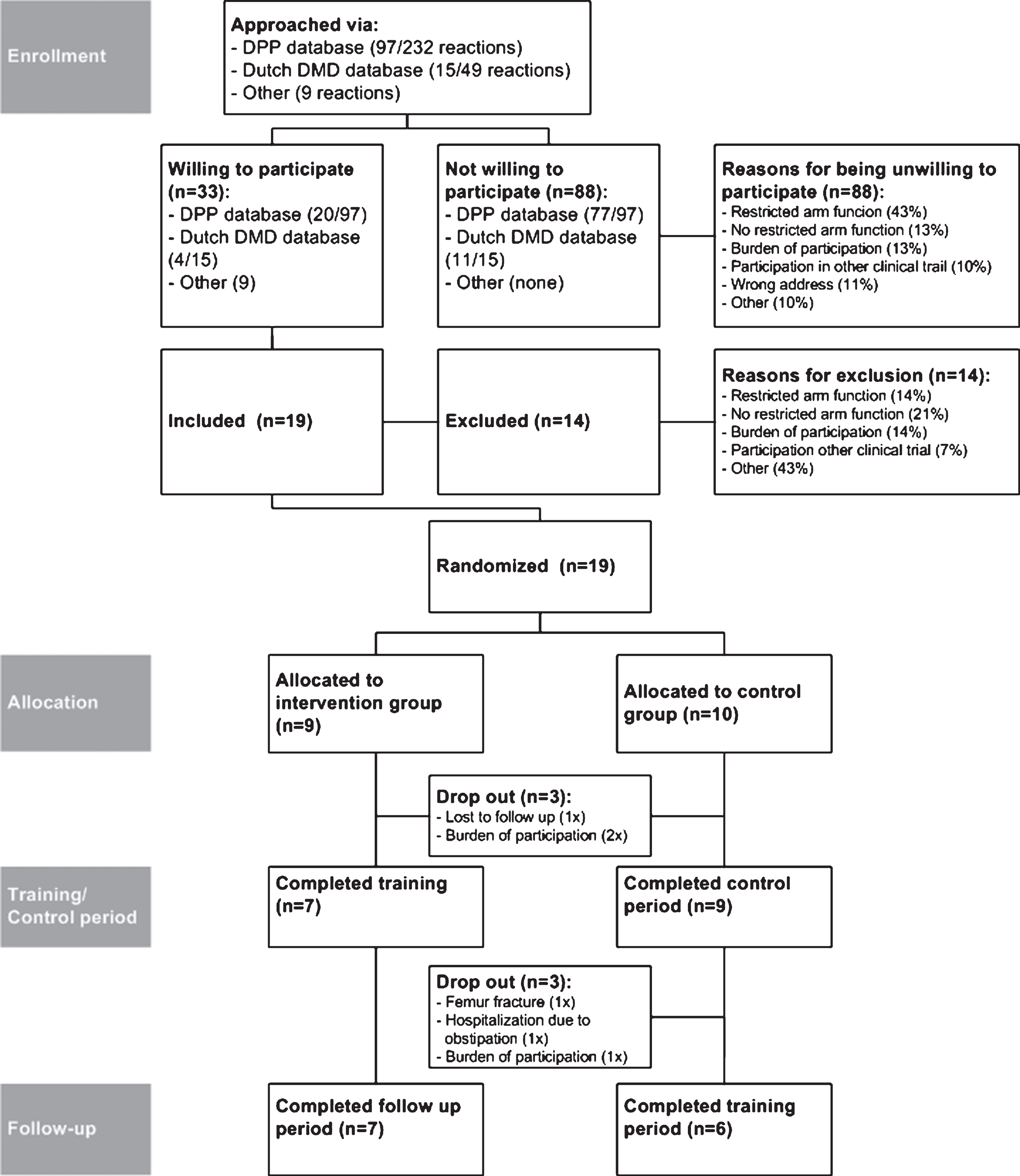
Participant flow through the study.
Table 2 shows the participant characteristics of the remaining 16 participants at baseline. Six out of 7 boys in the intervention group, and 6 out of 9 boys in the control group were still able to lift their arms above their head. Three boys were ambulant and 4 boys were wheelchair-dependent in the intervention group, compared to 3 and 6 in the control group respectively (p = 0.719). All participants had regular physiotherapy. In the intervention group, one boy did not engage in sports, in the control group all boys engaged in sports. The intervention group spend significantly more time on sports (p = 0.015). There were no other significant differences between the groups regarding patientcharacteristics.
Participant characteristics at baseline (T0)
0.5×per week physiotherapy = once per 2 weeks, 0.3×per week physiotherapy = once per 3 weeks.
Feasibility and compliance
All participants were able to perform the training. The training group trained on average 4.6 times a week (SD = 1.1). The mean OMNI score during the training was 1.6 (SD = 1.0).
Training effect at primary endpoint (change T0-T2): Primary outcome measure
The mean change of the PUL (T0-T2) was –1.6 (SD = 2.9) for the intervention group and –3.1 (SD = 3.4) for the control group (Table 3), which was not significantly different (p = 0.361). The individual differences in total PUL score and the elbow dimension of the PUL between T0 and T2 are displayed in Fig. 4.
Outcome measures T0-T2
Significant difference between the intervention and control group at the 0.05 level.
Mann-Whitney U test. Abbreviations: PUL, Performance of Upper Limb; MFM, Motor Function Measure; A6MCT, Assisted Six Minute Cycle Test; HHD, hand held dynamometer; MVC, maximal voluntary contraction; ROM, active joint range of motion.
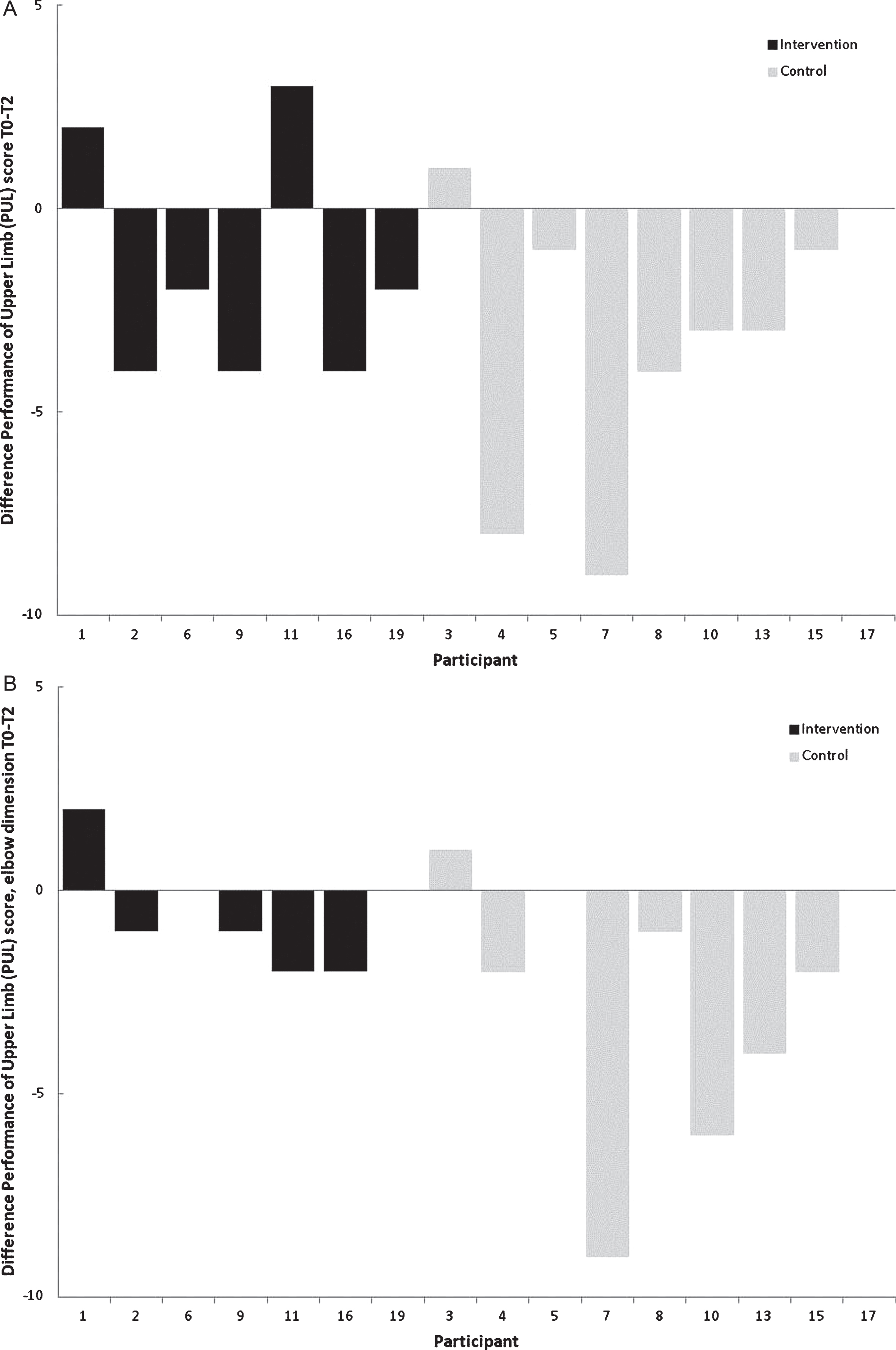
Individual differences in Performance of the Upper Limb (PUL) score between T0 and T2. (A) Individual differences in total Performance of Upper Limb (PUL) score between T0 and T2. (B) Individual differences in elbow dimension of the Performance of Upper Limb (PUL) score between T0 and T2.
Secondary outcome measures (change T0-T2)
The active range of motion in the elbow increased in the intervention group (mean = 15.7 degrees; SD = 22.1), whereas it decreased in the control group (mean = –18.9 degrees; SD = 25.3) (p = 0.018). The elbow extension strength of the left arm measured by the HHD increased with 1.5 lbs (SD = 1.8) in the intervention group, whereas it decreased in the control group with –0,2 lbs (SD = 1.6) (p = 0.038). Other secondary outcome measures showed no significant differences, see Table 3.
Training effect control group
Three boys were excluded after T3, see Fig. 3. From these boys, data from screening, baseline (T0), T1 and T2 was included in the analysis. The mean change in PUL score from T0 to T2 (–3.1, SD = 3.4) (control period for the control group) was not significantly different from the change in score from T3 to T4 (–0.2, SD = 2.1) (training period for the control group). The Kidscreen for children showed a difference of 1.4 (2.4) between T0 and T2 and a difference of –0.9 between T3 and T4 (p = 0.034). A higher score on the Kidscreen indicates a better quality of life. There were no significant differences between T0-T2 and T3-T4 for the other secondary outcome measures.
Adverse events
None of the participants reported constant pain during the training. Pain in the shoulders and thumbs were reported once, but disappeared after adjustment of the straps of the arm support by the coach. One participant in the control group fractured his femur during a fall between T3 and T4 and dropped out. One participant was hospitalized because of constipation. Both were unrelated to the training.
CONCLUSIONS
The Gainboy® study is the first explorative RCT in boys with DMD testing the effects of virtual reality computer gaming with dynamic arm support for both late ambulatory and non-ambulatory boys. The aim was to challenge the boys to move their arms in 3D and preserve joint motion and muscle elasticity, consequently leading to preservation of functional abilities in the arms. We found no significant differences in the decline of the primary outcome between the training and control group. However, we found a significant effect on the active joint range of motion of the elbow. The training group showed an increase in active range of motion, whereas the control group showed a decrease. Also, the training group showed an increase in elbow extension strength of the left arm after the training period, whereas the control group showed a decline. No study related adverse events were recorded.
Previous studies on training in DMD found positive effects of training. Assisted bicycle training prevented functional deterioration measured by the total MFM score [15]. Upper extremity training with an arm ergometer showed positive effects on ambulation scores, endurance, the degree of arm elevation and proximal muscle strength [16]. Our study did not show a significant training effect on the primary outcome measure. Still, the decline in PUL score in the control group was almost twice as big compared to the training group (–3,1, SD = 3.4 versus –1.6, SD = 2.9). The control group showed a decline of only –0,2 (SD = 2.6) on the total PUL score during their training period (T3-T4). Also, the elbow dimension showed a decline of –0.6 (SD = 1.4) for the training group, while the decline of the control group was four times higher (–2.6, SD = 3.2). During the training period of the control group, the decline was –0.7 (SD = 3.1). Although the differences are not significant, they seem quite large if you take into account the maximum scores of the PUL. Therefore we explored the individual differences in total PUL score of the participants (Fig. 4A), and of the elbow dimension of the PUL (Fig. 4B). Intuitively, it seems that the control group shows a larger decline in total PUL score and elbow dimension than the training group. During the training, the boys mostly practiced reaching and grasping movements with the arms. These movements are mainly represented in some items of the elbow dimension of the PUL (only items H-L), which might be an explanation why we did not find a significant training effect on the total PUL score and also on the elbow dimension. Although the PUL shows good reliability, it may not be sensitive enough to measure the functional effects of the Gainboy® training in a study population with relative good arm function (12 of the 16 boys had Brooke 1-2) [37].
The increase in elbow strength in the intervention group was only present in the left arm. This might be explained by the handedness of the boys. All boys, except for 2 in the control group, were right handed. When the preference arm is right, there might be more disuse in the left arm, and this arm might benefit more from training.
There is little information about which training intensity and training methods are suitable and effective for boys with DMD. The intensity of our training might have been too low or the stimulus of the type of training might have been too a specific. More studies are needed to implement adjusted strength and endurance training to eventually design a training method which is safe, suitable and effective for boys with DMD. Training is a useful way to engage in sufficient daily physical activity, which remains a challenge for boys with DMD [38].
During and after the training, participants mentioned to the coach that they felt that their health and arm function were improving. Quotes of the participants or parents were: ‘I feel the training is working for me’, ‘my son benefited from the training’, ‘I feel a difference in my arms’ and ‘it’s fun to play the games’. Although we did not find an effect on the quality of life measures (which showed poor reliability), there seems to be a positive trend among the participants.
Our study has several limitations. It remains a challenge to find enough eligible participants for intervention studies who are willing to participate. Also, because of the small number of participants, we did not correct for corticosteroid use and physical activity levels, which might be confounders. In addition, a higher percentage of the control group was wheelchair dependent, which can indicate a more severe population. However, we did not find significant differences between the intervention and control group in the functional scales. Furthermore, there is the possibility of a physical activity bias. Boys who are willing to participate in a training study might already have relative active lifestyles and will therefore benefit less from training compared to boys with an inactive lifestyle. This is supported by the engagement in sport activities/weekly physical activity by all of our participants. A practical limitation of the 3D training used in this study is the size of the frame of the dynamic arm support, which may be too large for use at home. Nevertheless, the device allowed all boys to move their arms against gravity and they were all able to use the device at home and the reported compliance was high.
This study is a first step in exploring the effect of training for late ambulatory and non-ambulatory boys with DMD. Our study indicates that positive effects on strength and range of motion of the elbow exist, which might prolong the ability to independently execute daily life activities such as eating on long-term. To further investigate the effect of training in boys with DMD, larger studies powered to control for potential confounders such as corticosteroid use and physical activity are needed. Future research should study whether effect of training is transferable to daily activities by measuring frequency and intensity of daily activities.
Conflict of interest
None of the authors has any conflict of interest to disclose.
Footnote
Preliminary results of this study were presented in a poster presentation at the ‘World Muscle Society’ in Granada on October 4th–8th 2016.
Footnotes
ACKNOWLEDGMENTS
The authors thank all boys and parents for their participation. Also, we thank Duchenne Parent Project for the grant and making this study possible. We thank Focal Meditech BV for helping us design and develop the Gainboy® device. We thank Sony for providing Playstations and games. Mariska Janssen, thank you for your help with the measurements andanalysis.