
Abstract
Background and objective:
Non-invasive ventilation (NIV) is an established treatment for respiratory failure in patients with amyotrophic lateral sclerosis (ALS). Several studies have shown room for improvement with regard to respiratory care for ALS patients, including latency of referral. These studies focused on the time period starting at the moment of referral to a home ventilation service (HVS) onwards. In the current study we performed a nationwide survey to gain insight in the trajectory before referral. We questioned the assessment of respiratory impairment by ALS physicians/care teams, including criteria for referral to an HVS.
Methods:
We requested 40 ALS care teams in the Netherlands to fill in an online questionnaire on respiratory management in ALS patients.
Results:
Thirty-two ALS care teams (80%) responded. Forced vital capacity was the most frequently used test at each outpatient visit (72%) and often served as a criterion (78%) for referral to an HVS. Other respiratory function measurements that were performed less often included peak cough flow (50%), maximum inspiratory/expiratory pressure (31% /28%) and sniff nasal inspiratory pressure (13%). Morning headache was the most frequently questioned complaint (94%), followed by daytime sleepiness (91%). Dyspnoea and orthopnoea were reported by 38% and 59% as important complaints. Out of all patients under the care of the ALS care teams, the mean estimated proportion of patients that was referred to an HVS was 69% (range 20-100%). When physicians refrained from referral, the most often cited reasons were patient’s decision to withhold NIV (94%) and cognitive impairment (50%). Sixteen percent of the respondents stated bulbar impairment as a reason to refrain from referral.
Conclusion:
Despite findings in previous studies on the superiority of SNIP and PCF as compared to FVC, our study shows that a majority of ALS care teams still prefers to use FVC for the assessment of respiratory dysfunction and for the timing of referral to an HVS. Another finding is that bulbar impairment is not an obstacle for referral for NIV.
Abbreviations
INTRODUCTION
Amyotrophic lateral sclerosis (ALS) is a fatal neurodegenerative disorder, characterized by progressive muscle weakness including the respiratory muscles [1]. Respiratory failure often begins as nocturnal hypoventilation and can be treated with non-invasive ventilation (NIV). NIV may improve survival and quality of life of patients with ALS, in particular those with limb onset ALS [2–4]. Physicians rely on complaints of respiratory muscle weakness and measurements of respiratory function to decide on a timely start of NIV [1]. According to a survey in the UK among consultant neurologists who cared for ALS patients, forced vital capacity (FVC) was the most frequently used test [5]. Previous studies have shown some limitations on the use of FVC and recommended the use of other tests, such as peak cough flow (PCF) or sniff nasal inspiratory pressure (SNIP). These latter tests may be superior predictors of a clinically relevant decline of respiratory muscle strength and of overall survival of patients with ALS [6–11].
In the Netherlands, 40 multidisciplinary ALS teams care for most of the ALS patients. Eighty-nine percent of the ALS physicians have implemented multidisciplinary care, which has shown to improve quality of life [12, 13]. One of the shortcomings of the multidisciplinary guideline, as reported by referring physicians in 2001, is the uncertainty about timing of referral to a home ventilation service (HVS) and the timing of initiation of NIV [14]. A recent study in the Netherlands suggested room for improvement in the respiratory care of ALS patients [6]. Data from referral letters and first visits to an HVS showed that a significant proportion of patients with ALS already had a degree of respiratory failure that necessitated immediate or short term start of NIV. It is noteworthy, that this situation is not unique for the Netherlands [5, 16]. In the current study, we performed a nationwide survey among physicians of ALS care teams to gain insight in multiple aspects of assessment and management of respiratory muscle weakness during the trajectory before referral to an HVS.
METHODS
Referral process of ALS patients to home ventilation services
In the Netherlands, all patients with ALS have access to NIV care. ALS care teams monitor respiratory functions, on average, trimonthly, before referral to an HVS. When physicians suspect respiratory muscle weakness, they refer those patients who want to, to one of the four HVS (Utrecht, Groningen, Rotterdam and Maastricht - based on postal code of the patient). According to the Dutch clinical practice standard on home mechanical ventilation, this referral is indicated when one or more of the following occurs: FVC < 70%, symptoms of nocturnal hypoventilation, signs of increased work of breathing or daytime hypercapnia (pCO2 > 45 mmHg) [16]. Following referral, the HVS-physician discusses treatment options (non-invasive ventilation (NIV), invasive ventilation or palliative care) with the patient, and, when indicated, starts ventilatory support.
Study design, data collection and processing
In February 2016, we sent an online questionnaire to all physicians of 40 ALS care teams in the Netherlands. We sent two reminders one and two months later, to all non-responders. The survey consisted of 30 questions covering a) characteristics of the ALS care teams (type of hospital, number of ALS patients currently under the care of the team), b) monitoring of respiratory function (examiner, intervals, respiratory tests used, complaints) and c) the criteria for referral to an HVS. Most answers consisted of multiple-choice options, with the possibility to add free text. An open question involved the decline of respiratory test values over time that would trigger a referral to an HVS. Responded surveys were anonymised and analysed.
Data and statistical analysis
Data are reported as number and proportions. Differences in the use of criteria between large and small ALS teams were assessed by a Pearson’s chi-square analysis.
Statistical analysis was done using IBM SPSS statistics version 23. A p-value of <0.05 was considered significant.
RESULTS
Thirty-two ALS teams responded to the survey (response rate 80%). In case of more than one physician in a team, one of them responded on behalf of the team. ALS teams cared for diverging numbers of patients at the moment of the survey: more than half of the teams (53%) cared for at least 10 patients (Fig. 1).
Number of ALS patients under care of referring physicians. Legend: Bars represent the number of patients under the care of referring physicians.
Monitoring of respiratory functions: Frequency, examiner and tests used
The time interval between outpatient visits varied among the responders. Depending on disease progression ALS care teams invited ALS patients every two months (16%), every three months (41%), between three and six months (38%) and every six months (6%) for follow-up.
Respiratory function tests used by physicians caring for ALS patients
Data represent the number of the referring physicians who responded (n = 32). ALS: Amyotrophic Lateral Sclerosis, FVC: Forced Vital Capacity, PCF: Peak Cough Flow, MIP/MEP: Maximum Inspiratory/Expiratory Pressure, SNIP: Sniff Nasal Inspiratory Pressure.
Referral to a home ventilation service: Frequency and respiratory tests used as selection criterion
Most physicians referred to an HVS directly (94%) and a minority referred to a pulmonologist within their own hospital.
Half of the respondents referred their latest patient with ALS to an HVS within the previous month; 38% did so one to six months ago. Eighteen respondents (56%) reported criteria for referral to an HVS. The use of criteria did not differ between large and small ALS teams (p = 0.29). Out of these 18 respondents, 14 (78%) based their referral on FVC: they used FVC in the supine position or the difference between sitting and supine measurements. Thirteen (72%) out of the 18 respondents who used selection criteria, reported a FVC cut-off value for the timing of referral to an HVS. The mean (SD) FVC was 65±9% (range 50–80) (Fig. 2).
Stated cut-off values of FVC for the timing of referral. Legend: FVC: Forced Vital Capacity (% predicted value). The cut-off values of FVC are plotted against the percentage of physicians who reported this as a selection criteria for referral to a home ventilation service, n = 13.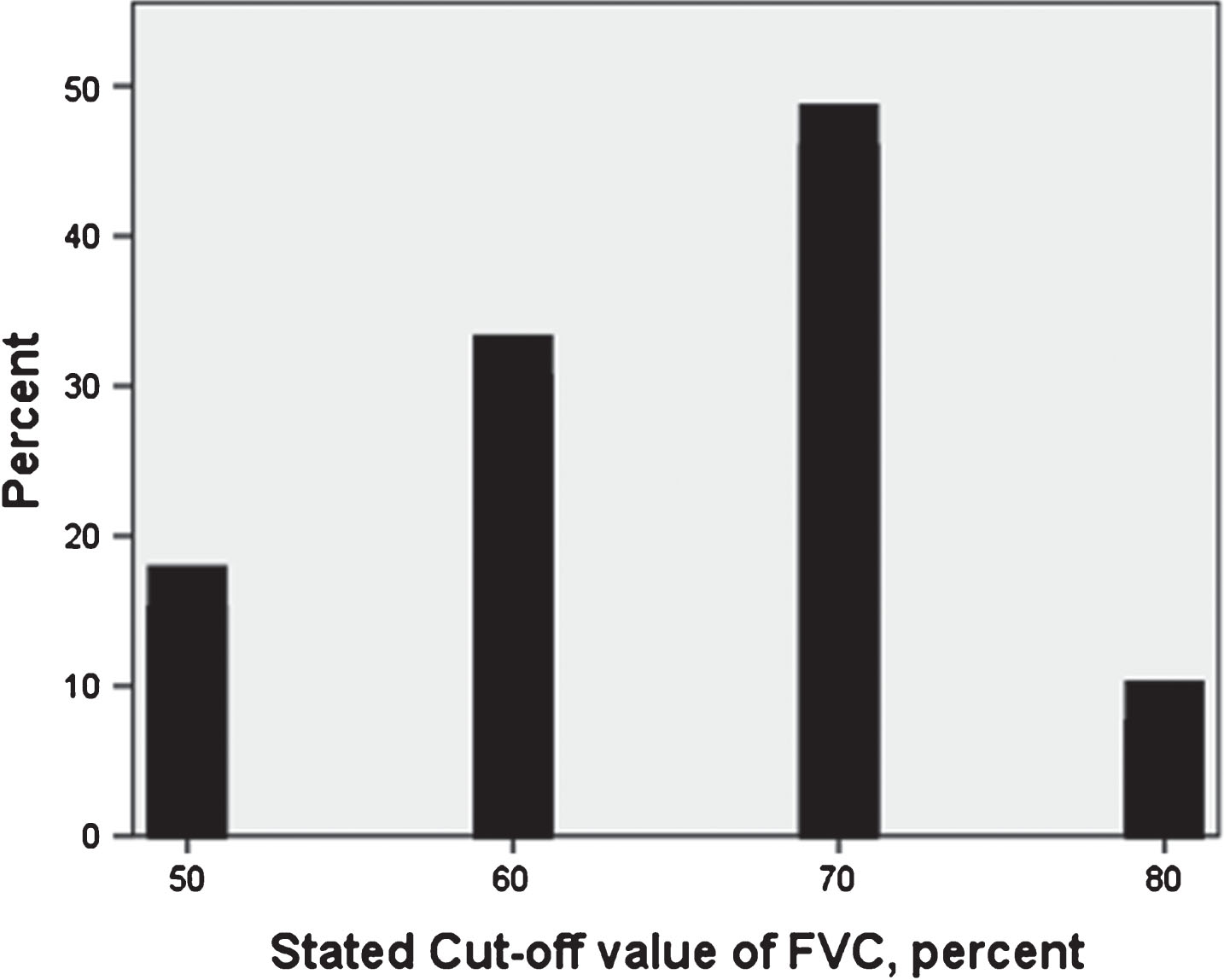
Respondents used MIP/MEP (39%), SNIP (11%), PCF (39%) and blood gas analysis (33%) less frequently in order to time referral; pulse oximetry was not reported as a referral criterion. Four respondents stated PCF cut-off values of 100, 270 and 300 L/min (mean 243±96 L/min). Respondents reported no cut-off values for other tests.
Referral to a home ventilation service: Complaints and signs of respiratory impairment
Figure 3 shows the complaints of respiratory impairment deemed important in relation to referral to an HVS (n = 32). Ninety-four percent of the respondents reported morning headache, followed by daytime sleepiness (91%), disturbed sleep (81%) and nightmares (81%). Dyspnoea and orthopnoea were reported by 38% and 59% as important complaints. In addition, we questioned signs of respiratory muscle weakness which are paid attention to in the physical examination for considering referral. These showed the following proportions; dyspnoea/tachypnoea (94%), use of accessory respiratory muscles (91%), use of short sentences (88%), orthopnoea (66%), paradoxical breathing (56%), transpiration (38%) and cough impairment (9%).
Complaints of respiratory muscle weakness important for referral to a home ventilation service. Legend: Data are presented as percentage of referring physicians who reported each complaint important for referral to a home ventilation service; n = 32.
Referral to a home ventilation service: Proportion of patients and reasons for refraining from referral
The respondents estimated the proportion of patients that had been referred to an HVS out of all patients that had been under their care: the mean of this estimate was 69% (range 20–100%). When physicians refrained from referral to an HVS, the most often cited reasons were the patient’s request not to be referred (94%), followed by cognitive impairment (50%). Sixteen percent of the respondents mentioned bulbar impairment as a reason to refrain from referral (Fig. 4).
Reasons to refrain from referral. Each bar represents the percentage of referring physicians for whom each item was reason to refrain from referral to a home ventilation service, n = 32 physicians.
DISCUSSION
In the current nationwide survey we investigated multiple aspects of the respiratory management of patients with ALS, in particular the trajectory before referral to an HVS. Our most important findings are that the vast majority of physicians of ALS care teams agree upon the complaints and signs which are deemed important for the presence of (nocturnal) hypoventilation and, accordingly, for referral to an HVS. Secondly, respondents most frequently use FVC in order to time referral to an HVS, and they use other respiratory function tests (MIP, MEP and SNIP) (far) less frequently. Thirdly, considerable differences exist between ALS care teams regarding the proportions of patients being referred, and cut-off values of respiratory function tests that trigger referral.
Use of respiratory function tests
The assessment of respiratory function in ALS patients in the Netherlands is performed by physicians (pulmonary physician (28%), rehabilitation physician (28%)), or physiotherapist (41%). The latter two groups have been formally trained to perform the procedures, and operate according to the guidelines. FVC is the most frequently used test in our study, both at the first visit and follow up visits. In a previous survey in the UK, 37% of responding neurologists assessed FVC at presentation and 19% did so during follow up visits, compared to 59% and 72% in the present study. When patients were symptomatic, 46% of UK neurologists assessed FVC, most commonly in the sitting position [5].
Compared to FVC, other pulmonary function tests have shown additional value in previous studies: SNIP prognosticates mortality of ALS patients more accurately [7, 19]. Our previous study showed a significant decline of SNIP in the months before receiving NIV, further corroborating the ability of SNIP to monitor disease progression and detect deterioration of respiratory muscle strength in a clinically meaningful period [9]. An impaired cough, reflected by a peak cough flow (PCF) below 300 L/min, is associated with a higher risk for developing respiratory complications and may be a valuable tool, in addition to SNIP for the timing of NIV [20–22]. MIP and MEP may have a higher sensitivity for the detection of nocturnal hypoventilation as compared to FVC [23]. In the present study, the use of SNIP, PCF, MIP/MEP and pulse oximetry at every outpatient clinic visit (and the ability to report cut-off values) is considerably lower compared to FVC. This is comparable to the UK survey, which showed that 2% and 4% of the physicians, at every outpatient clinic visit, used MIP/MEP and SNIP (PCF was not investigated in the latter study) [5]. Despite recommendations in international guidelines to use SNIP and PCF, our and other studies show a discrepancy between guidelines and clinical practice [12, 25]. We suggest that future studies will explore the underlying reasons (e.g. unfamiliarity, experience and time).
Criteria for referral to a home ventilation service
Multidisciplinary care has shown to improve survival of ALS patients, also in the Netherlands [13]. In 2001 Dutch physicians noticed a shortcoming in the protocol for multidisciplinary care of ALS patients, being the uncertainty about criteria regarding the timing of referral to an HVS [14]. The current study underlines the persistent presence of this uncertainty, as 59% of the respondents could not state an FVC cut-off value related to the timing of referral. This is not a typical Dutch phenomenon: 33–67% of neurologists from the UK and Canada, respectively, specified a FVC threshold for the initiation of NIV - varying 50 and 70% of the predicted value, which is comparable to our finding of 50–80% [5, 25]. International guidelines suggest that FVC lower than 80% of predicted, in combination with complaints, is a criterion for the initiation of NIV in ALS patients [18]. Recent studies have shown that this cut-off value is a too strict criteria for being referral to an HVS or initiation of NIV. Although FVC has good predictive power for ventilator-free survival, the cut-off value indicating a poor prognosis lies within the normal range (>80% predicted), which is related to findings that relatively high FVC values may be observed close to a clinical meaningful event (e.g., start of NIV) [8, 9].
Previous studies have shown a predictive effect of cough flow/pressure measurements on either the need for NIV or survival - albeit modest compared to inspiratory measures [9]. Our previous study of serial measurements of respiratory function tests preceding referral to an HVS, suggested the ability of PCF, but not other tests, to predict the need for NIV within the following three months [12]. This finding is in line with the work of Polkey et al. which showed a descending trend of the peak cough pressure in the months previous to NIV or death [9].
The present study shows that 50% of the physicians in the Netherlands use PCF at every visit, with 13% reporting cut-off values. Again, this low number of reported cut-off values is not restricted to the Netherlands, and together this indicates room for improvement on PCF use and the investigation and communication of cut-off values [5, 25].
As for complaints deemed important for considering referral to an HVS, morning headache and daytime sleepiness were reported most frequently (approximately 90% of the physicians).
Only thirty-eight percent of the physicians in our study questioned dyspnoea as meaningful complaint. Nonetheless, dyspnoea/tachypnoea are assessed in the physical examination by 94% of the physicians as sign of hypoventilation, in accordance with the European study of Heiman-Patterson et al. [25]. Regarding sensitivity of daytime dyspnoea, it is our clinical impression that some patients who are hypercapnic - based on an arterial blood gas analysis during daytime – do not report (daytime) dyspnoea, or shortness of breath or any equivalent symptom. In particular those patients with a relatively slow decline of respiratory muscle strength do not seem to experience dyspnoea until only very late in the process of decline, or not at all. Regarding specificity of symptoms of nocturnal hypoventilation, the presence of sleep disorders, including (obstructive) sleep apnoea in ALS patients complicates the questioning of symptoms even more [26]. Tests for nocturnal hypoventilation, such as transcutaneous blood gas analysis and (nocturnal) oximetry, are not routinely performed in outpatient settings in the Netherlands; these tests are administered at the HVS, after referral. These findings suggest that possibilities and benefits of easier access to nocturnal assessments by ALS care teams should be explored and investigated.
Deterrents to refer patients with ALS to a home ventilation service
In the current study cognitive impairment is the second most frequently reported reason to renounce referral – the patient’s preference to withhold NIV being the most frequently reported reason. Moderate to severe cognitive and behavioural impairment occurs in up to 30% of ALS patients and frontotemporal dementia in 8–15% [27]. There is some evidence from previous studies showing that in particular severe behavioural changes are related to a lower use of NIV [27–29]. Our study corroborates the finding that ALS clinicians are aware of the clinical impact of these non-motor symptoms, which have been shown to reduce survival, in part attributed to reduced compliance with NIV [30, 31].
Another finding of the current survey is that a lower number of responding physicians than expected (16%), reported bulbar involvement as a reason to refrain from HVS referral; this is also comparable to the UK survey (20–25%). There is uncertainty about the effect of NIV in patients with bulbar ALS: a randomised clinical trial showed no survival benefit (n = 21), whereas a large retrospective cohort study showed a 19 months survival benefit (n = 312) [2, 3]. Despite the fact that NIV is ineffective in some bulbar ALS patients due to facial weakness leading to leakage of air, the finding of the large retrospective study seems in accordance with the tendency of physicians to refer not only patients with spinal onset, but also bulbar onset ALS to an HVS.
A limitation of our study is the potential discrepancy between reported activities and clinical practice, even though we aimed to reduce this bias by anonymising the survey.
CONCLUSION AND RECOMMENDATIONS
In the trajectory before referral to an HVS, our study shows that respiratory management of patients with ALS leaves room for improvement, specifically in terms of the use of SNIP and PCF. Furthermore, in accordance with another nationwide survey in Europe, we show a discrepancy between international recommendations and current practice [5, 25]. Future research should focus on: 1) reasons why most physicians do not perform other tests than FVC; 2) examination of cut-off values (including percentage of decline) for respiratory function tests in ALS; 3) correlation between complaints and test results. The ultimate goals are timely referral to an HVS and prevention of acute respiratory failure in ALS patients [32].
DECLARATIONS
Ethics approval
No approval by the ethics committee was needed.
Consents for publication
Not applicable.
Funding
No funding.
Availability of data and materials
The data that support the findings of this study and additional information are available from the corresponding author upon request.
Competing interests
The study was performed at the departments of Neurology and Rehabilitation at the Radboud university medical center, Nijmegen, the Netherlands. The authors do not report any financial or other conflicts of interest.