
Abstract
Congenital muscular dystrophies (CMD) cause progressive muscle weakness resulting in severe motor disabilities. Previous studies focused on the effects of motor disability. Here, we explore other factors affecting health related quality-of-life (HRQOL) in CMD. Qualitative interviews were conducted with participant-parent dyads to identify symptoms having the greatest impact on HRQOL. Symptoms were classified into themes and domains representing physical, mental, social health, and disease specific issues. Social role limitations and specific activity impairment were frequently mentioned. A greater understanding of symptoms impacting HRQOL will provide a framework for improved clinical care and patient centered outcomes as new therapies are developed.
INTRODUCTION
Congenital muscular dystrophies (CMD) cause progressive weakness and motor disability in childhood. The most common CMDs are the collagen 6-related muscular dystrophies (COL6-RDs) and merosin-deficient-CMD [1, 2]. COL6-RDs include a spectrum of severity, from the more severe Ullrich Congenital Muscular Dystrophy (UCMD), including the classic and intermediate forms, and the milder Bethlem Myopathy (BM) phenotypes [3–5]. COL6-RDs are characterized by muscle weakness, proximal contractures, distal joint laxity, respiratory insufficiency, and cutaneous indicators such as soft palms and soles and keloid formation [3, 6]. Merosin deficient CMD, caused by mutations in the laminin alpha2 gene (LAMA2), presents with congenital muscle weakness within the first months of life, contractures, delayed motor milestones, and respiratory insufficiency due to progressive muscle weakness [5, 8]. Cognitive impairment is absent in both populations.
Health Related Quality of Life (HRQOL) is a subset of QOL, defined as “goals, expectations, standards, or concerns about their overall health and health-related domains” [9]. There is limited information on the impact of COL6-RDs and LAMA2-RDs on HRQOL, particularly from the view of those affected by CMD and their caregivers. Prior research has focused on physical disability with little emphasis on social or emotional aspects of the disease [10]. HRQOL studies in other neuromuscular diseases have looked at physical impact of the condition, while few have shown the importance of under-recognized social and emotional aspects of these diseases [10–14]. A qualitative approach may more holistically identify the disease burden in those affected by CMD and their caregivers. By incorporating an individual’s viewpoint about their disease, there is a subjective component to HRQOL that is often overlooked [15].
This qualitative study identifies symptoms affecting those with CMD to develop a model representing HRQOL [11]. Future studies involving larger populations of CMD will use this model to create a disease-specific patient reported outcome for use in therapeutic trials.
MATERIALS AND METHODS
Participants were included with genetically-confirmed diagnosis of COL6-RD or LAMA2-RDs. The participant cohort was selected from a local clinical database. Purposive sampling was used to ensure appropriate range of ages, gender, and disease severity. COL6-RD participants were separated into UCMD, which includes both the classic UCMD and an intermediate phenotype, and BM according to accepted disease classifications [16]. LAMA2-RDs participants had symptoms at birth or shortly after and documented full merosin deficiency.
Telephone interviews were semi-structured and participants were asked the same set of open-ended questions that covered topics ranging from physical, mental, and social health, with the goal of identifying symptoms impacting HRQOL [17]. Qualitative interviews were conducted by K.M.C, trained by N.E.J. (Questions provided in Supplemental Methods 1).
Participants were sent a description of the project and consent electronically prior to the interview. At the time of the phone interview, participants older than 18 years old and parents of participants younger than 18 years old provided verbal consent, whereas participants younger than 18 years provided verbal assent. No participant refused to participate. Participants older than 18 years were interviewed independently. If the participant was less than 18 years old, a parent was also interviewed.
Interviews were audio recorded, transcribed, and coded according to symptoms mentioned by participants. Interviews lasted 45–60 minutes on average. Analysis, including coding and symptom classification, used a qualitative framework technique [18]. This technique provides a systematic and structured approach to analyzing large qualitative data sets and has been used in other neuromuscular populations to identify disease burden [11, 19]. Symptoms mentioned by participants and caregivers were indexed across interviews and categorized into themes by one researcher and verified by a second. Themes were classified into four over-arching domains, including physical, mental, and social health, and disease-specific issues, using WHO criteria to create a CMD model for HRQOL [9]. Participant enrollment was completed once additional interviews failed to yield new symptoms, defined as saturation, or when few or no new data are generated [20]. All study procedures were approved by the University of Utah institutional review board.
RESULTS
Interviews conducted included fourteen participant-parent UCMD dyads, seven BM participants, and four participant-parent LAMA2-RD dyads. Dyad interviews consisted of an interview with the parent and participant, respectively. Participant demographics are provided in Table 1.
Participant demographics
*All participants have a known mutation in COL6A1, COL6A2, or COL6A3 for COL6-RD or LAMA2 mutation for merosin deficient CMD. UCMD participants included the classic and intermediate phenotypes and were classified as loss of ambulation by adulthood. BM participants were classified as preserved ambulation into adulthood. For participants younger than 18 years old, both the participant and their parent were interviewed. For participants older than 18 years old, no parents were interviewed.
A total of 714 symptoms were identified, which were classified into 20 themes that fit into four overarching domains. Figure 1a presents the theme frequency. These themes were further categorized to create an initial CMD HRQOL model (Fig. 1b).
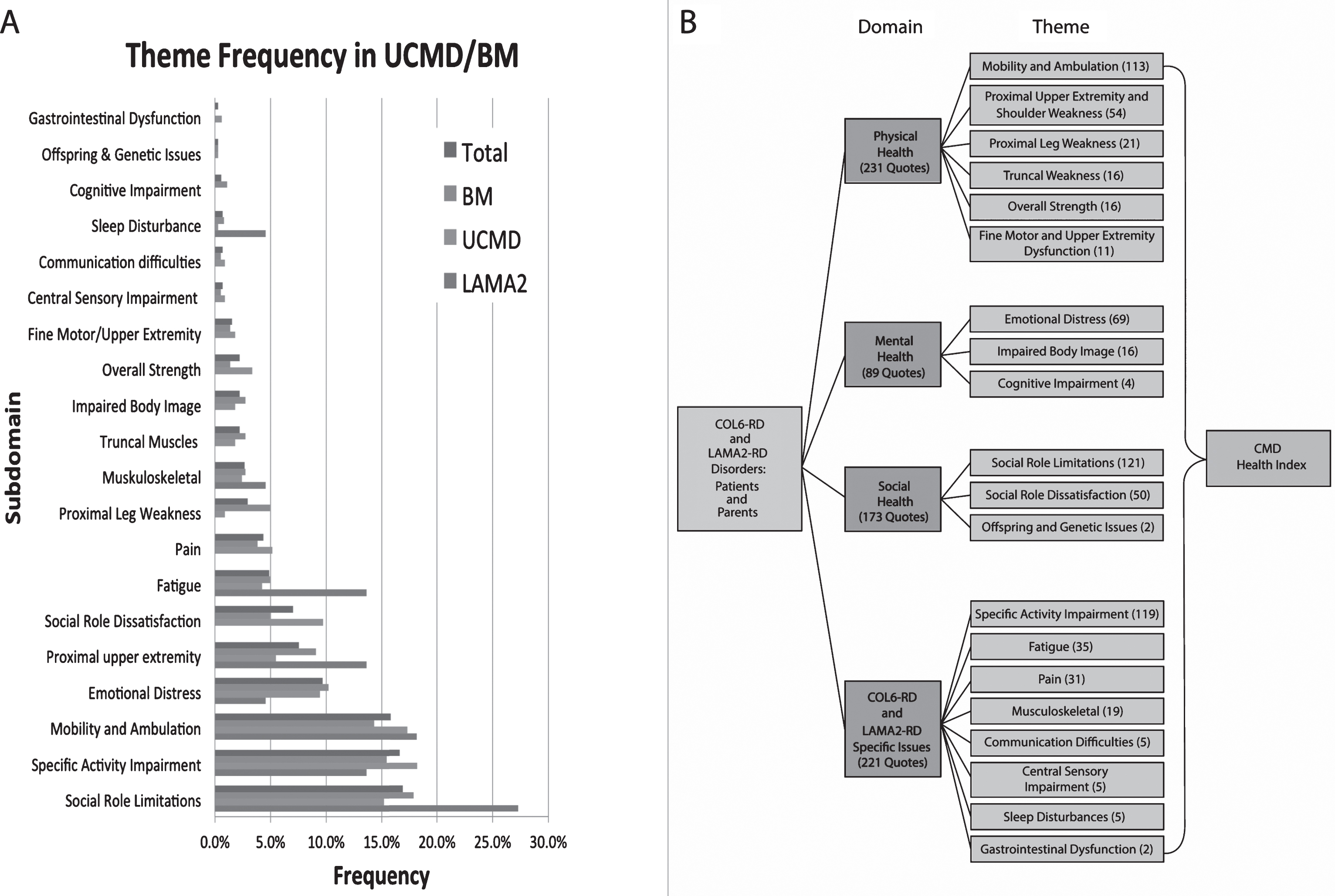
A Quote frequencies by theme. Participants mentioned 714 symptoms, which were then transcribed and coded into 20 themes affecting health related quality of life in participants with CMD. The most frequently mentioned symptoms relate to the themes of Social Role Limitations, followed by Specific Activity Impairment, Mobility and Ambulation, and Emotional Distress. Symptoms mentioned less frequently relate to the themes of Gastrointestinal Dysfunction, Offspring and Genetic Issues, and Sleep Disturbance. B. Themes were categorized into four over-arching domains, including, physical, mental, and social health, as well as disease specific issues. Each domain and its corresponding themes together make up an overall Health Related Quality of Life model applicable to CMD. All participants provided verbal consent or assent before beginning interviews.
More symptoms involved social role limitations (121 quotes) than any other theme.
The most common symptom related to social role limitations was decreased independence (17). One UCMD participant described her experience by saying, “It’s harder making friends because they think ‘she’s going to need help’…I have to exclude myself from the games that we play” and one BM participant stating “you have to get used to people helping you…you’re going to need a variety of equipment to help you through everyday living.” Other common social role limitation symptoms include reliance on family members (14), and limitations physically on what one can do (12).
The second frequently mentioned theme was specific activity impairment (119 quotes). One UCMD parent stated, “They don’t walk…being 11 years old he doesn’t get to play sports like his friends do. He has trouble dressing.” Specific activity impairment also included quotes involving difficulty playing sports (20), activities of daily living impairment (16), and problems getting dressed (12).
Mobility and ambulation (113 quotes) involved impaired walking (29), difficulty with stairs (19), and problems getting to and using the bathroom (14). One UCMD parent mentioned, “The inability to do things that we normally do like getting out of bed by himself, getting in the car…having the assistance in getting dressed and showering.”
The emotional distress theme (69 quotes) was demonstrated by one UCMD participant stating “People make fun of me, cause of the wheelchair” and one BM participant noting “it’s embarrassing” in regards to needing help to complete activities of daily living. Quotes regarding this theme also focused on an embarrassment of disability (9) and depression (6).
DISCUSSION
CMDs encompass a wide range of phenotypes. In COL6-RDs, symptoms are either present at birth or develop in early childhood with progressive muscle weakness leading to motor disability, contracture formation, and respiratory difficulties [3, 21]. LAMA2-RDs present within the first few months of life and involves progressive muscle weakness and respiratory difficulties later in life [5, 8].
As in other neuromuscular conditions, motor symptoms were a major contributor to decreased HRQOL in CMD [10–14]. However, other aspects outside of physical limitations, including social and mental components, were frequently mentioned, which raises awareness to other issues that affect HRQOL in this population not previously mentioned in prior studies [10].
Among those symptoms, social role limitations were most frequently mentioned as having an impact on HRQOL. Decreased independence and reliance on others was commonly mentioned in both populations. Specific activity impairment was the next most commonly mentioned and involve difficulty playing sports and activities of daily living.
Another common aspect of this study includes the mental health domain, which encompasses emotional and cognitive components. Emotional distress being frequently mentioned. In contrast to other populations of muscular dystrophies, particularly CDM, CMD participants sparsely reported cognitive impairment (4 quotes versus 71 in CDM), which was confined to needing additional time for planning [11]. Unique to CMD, within the disease specific issues domain, includes contractures, fatigue, and pain, however these were less frequent.
While physical symptoms have an impact on participants with CMD and their caregivers as previously mentioned, the frequency with which other aspects were mentioned deserves attention [10]. Previous studies that have focused on HRQOL in patients with hereditary neuromuscular diseases, emphasized the importance of subjective aspects of disease and emphasized how aspects of HRQOL are often overlooked by healthcare providers [15]. This work emphasizes the importance of an HRQOL model specific to neuromuscular populations, which supports previous work demonstrating the importance of social concerns in a population of DM1, CDM and FSH [11, 21]. As in these previous studies, this model underscores the importance of addressing key issues involving social, emotional, and specific activity with regards to patients who have CMD. Disease specific aspects clearly have to be taken into account as for instance in contrast to CDM, cognition is normal in COL6-RDs and LAMA2-RDs, resulting in different social and emotional implications.
There are several limitations to this study. First, interviews were limited to a small number of participants selected to represent a wide variety of people with CMD. Second, this study did not use an objective measure for strength or functionality. Third, in order to prepare a tool that could measure positive impact of future therapeutic interventions, this study focused more on the perceived negative impact of CMD. Although questions were open-ended allowing for comments about positive adaption to the disease, questions specifically focusing on such experiences were not provided. This is relevant as COL6-RDs and LAMA2-RD patients may experience disease burden much less negatively (known as the “disability paradox”). Future projects involving a larger sample size and more extensive physical characterizations will need to be performed to validate our findings and further develop a disease specific patient-reported outcome.
This study used a qualitative approach to identify symptoms affecting HRQOL of individuals with COL6-RDs and LAMA2-RDs. While physical symptoms were frequent, social and emotional symptoms were also mentioned as having an impact on HRQOL. These interviews provide a foundation for understanding what issues are important to the CMD population and the initial step in developing a disease specific patient-reported outcome instrument. Future studies will focus on validating these methods in a larger CMD population.
CONFLICT OF INTEREST
Ms. Cornwall, Mr. Hernandez report no disclosures. Dr. Johnson serves as an Associate Editor for Neurology: Genetics. He is funded by the NIH, grant #1K23NS091511-01. He has received research support from the Muscular Dystrophy Association, Myotonic Dystrophy Foundation, Valerion Therapeutics, Ionis Pharmaceuticals, and Biogen Idec. Dr. Heatwole has received grant funding from the NIH, FDA, and Cure SMA foundation. He is the founder and CEO of the Neuromuscular Quality of Life Institute. He receives royalties for the Myotonic Dystrophy Health Index, the FSHD-HI, the CMT-HI, and the SMA-HI. He has provided expert testimony for neuromuscular cases unrelated to this research. He has provided consultation to Biogen, Ionis, aTyr, Regeneron, and Acceleron Pharma. Dr. Butterfield is supported by NIH grant 1K08NS097631-01. He is receiving funding via contracts for clinical trials from PTC Therapeutics, Sarepta Therapeutics, Pfizer, Marathon, Biogen, Summit Therapeutics, Santhera Pharmaceuticals, and aTyr Pharmaceuticals. Dr. Butterfield serves on scientific advisory boards for Sarepta Therapeutics, Biogen, PTC Therapeutics, and Wave Life Sciences.