
Abstract
Background:
In 2020, our group published physical therapy clinical practice guidelines (CPG) for people with Huntington’s disease (HD). The guideline recommendations were categorized according to six primary movement impairment classifications.
Objective:
To facilitate implementation of this CPG, we have developed guideline-based algorithms for physical therapy assessments and interventions and recommendations for therapists to overcome barriers to CPG implementation for people with HD.
Methods:
We conducted a literature review of papers that evaluated physical therapy interventions in individuals with HD (n = 26) to identify assessments for each of the primary movement impairment classifications, and then searched for papers (n = 28) that reported their clinometric/psychometric properties in HD. Assessments were evaluated using modified Movement Disorder Society Committee on Rating Scales criteria and other relevant criteria.
Results:
We identified a “core set” of physical therapy assessments for persons with HD, including the Six Minute Walk Test, Timed Up and Go Test, Berg Balance Scale, and the Medical Outcomes Study Short Form 36 (SF-36). We then developed guideline-based decision trees to assist in decision making and implementation of the CPG into practice for persons with HD across the continuum of care. Finally, we developed strategies for overcoming barriers to implementation, such as seeking specialized training in HD, engaging caretakers or family members to help the person with HD to exercise, and establishing clinical pathways that support early physical therapy referrals.
Conclusion:
Knowledge translation documents such as this are essential to promoting implementation of the physical therapy CPGs into clinical practice.
INTRODUCTION
Huntington’s disease (HD) is a progressive hereditary neurodegenerative disease that causes death of neurons in the basal ganglia, impacting motor, cognitive, and psychological function [1]. HD affects approximately 40,000 Americans [2], with another 200,000 at risk of developing the condition [3]. The physical therapist is a key member of the interdisciplinary team for persons with HD. Without disease modifying therapies, physical therapy and other rehabilitation interventions offer the next best option for secondary prevention and optimizing functional abilities over the course of neurodegenerative diseases [4]. The role of the physical therapist in the care of persons with HD will vary through the course of the disease, ranging from prevention of mobility restriction in the prodromal and early manifest stages, to maintaining function and slowing down progression in the middle stages, and to limiting the impact of complications and providing supportive care in late stages of the disease [5].
Physical therapy improves motor function in persons with HD [6]. We recently published clinical practice guidelines to guide physical therapy interventions for persons with HD [7]. Specifically, there is Grade A evidence to support 1) aerobic exercise paired with strengthening exercises to improve fitness and to stabilize or improve motor function; and 2) one-on-one supervised gait training to improve spatiotemporal measures of gait. Grade B evidence supports 1) individualized exercise, including balance exercise, to improve balance and balance confidence; and 2) inspiratory and expiratory training to improve respiratory muscle strength and cough effectiveness. The clinical guidelines were further categorized according to six previously identified treatment-based classifications, referred to as primary movement impairment classifications in this paper, to better match clinical guidelines with the individual’s primary movement problems (e.g., mobility and function, balance and falls risk) [7].
As a next step to implementation of these clinical guidelines into practice, we have now developed guideline-based decision tree models and provide recommendations for physical therapy assessments. Visually-based decision tree models can assist physical therapists to plan and make decisions regarding the management of individuals with complex and heterogeneous disorders such as HD [8]. Clinical decision trees help guide clinicians through physical therapy evaluation and plan of care with specific attention to identifying the primary movement dysfunction, choosing appropriate assessments with published psychometrics for persons with HD, and selecting evidence-supported interventions. To improve the translation of clinical guidelines into practice, we identified the need for assessments to screen for dysfunction and to assess changes resulting from physical therapy interventions in body structure and function, activity, and participation [9].
This paper aims to: 1) recommend clinical assessments based on available literature for each of the primary movement impairment classifications; 2) provide guideline-based decision trees to aid in decision-making and implementation of a physical therapy plan of care for individuals with HD; 3) apply the proposed decision trees using patient examples, and 4) recommend strategies to overcome barriers and to facilitate implementation of the guidelines.
PHYSICAL THERAPY ASSESSMENTS FOR PERSONS WITH HD
Literature search
We conducted a literature review to determine assessments that have been used to evaluate physical therapy interventions in individuals with HD. A systematic approach was employed; we used the same search terms from our 2017 systematic review [6] to capture all studies included in the clinical guidelines and any studies published since from 2017 to January of 2022 (n = 26). We reviewed the assessments used in each study and then searched for articles that reported on their clinometric/psychometric properties in HD (n = 28). Our search focused on assessments that measure activity and participation levels of the International Classification of Functioning, Disability and Health (ICF) [10] and align with the primary movement classifications detailed in the CPG [4]. Impairment-based assessments that are used as part of the standard neurologic examination of a patient (e.g., manual muscle testing, range of motion) were not included.
Critical appraisal process
We evaluated each of the listed measures by adapting the criteria for rating scales proposed by the Movement Disorders Society Committee on Rating Scales Development [11]. Clinical assessments were recommended if the measures had (1) been used in the HD population; (2) used in HD by groups other than the original developers and data on their use were available; and if (3) the available clinometric/psychometric data in HD supported properties of reliability and/or predictive accuracy (i.e., test-retest reliability, minimal detectable change, sensitivity/specificity and score cut-offs), and validity (i.e., discriminative and/or concurrent), and responsiveness to interventions in clinical trials. For assessments not developed for use in HD, criterion 2 could also be fulfilled if used in at least one group in HD that reported any kind of clinometric/psychometric properties in HD. Clinical assessments were suggested if the measures had (1) been used in the HD population; and (2) only one other criterion (2) or (3) from the recommended category were fulfilled. Clinical assessments were listed if the measures had been applied to the HD population, but no further criteria were met. Through an iterative consensus process, we evaluated assessments with the modified MDS ratings scale recommendations (Table 1). Recommended measures for persons with HD were then examined to determine their 1) clinical research utility in terms of psychometrics (Table 1); 2) clinical utility in terms of time to complete, ease of use, and accessibility; and 3) alignment with the Academy of Neurologic Physical Therapy (ANPT) recommended core outcomes measures [12], to develop a recommended core set of assessments for physical therapists to use with all persons with HD (see Fig. 1).
Physical Therapy Assessments in Huntington’s Disease
AUC, area under curve; HD, Huntington’s disease; HD-ADL, Huntington’s Disease-Activities of Daily Living Questionnaire; MVPA, moderate-to-vigorous physical activity; ROC, receiver operating curve; Stage I, early stage with TFC 11–13; Stage II, middle stage with TFC 7–10; Stage III, late stage with TFC < 7; UHDRS-FAS, Unified Huntington’s Disease Rating Scale-Functional Activity Assessment; UHDRS-TFC, UHDRS-Total Functional Capacity; UHDRS-TMS, UHDRS-Total Motor Score; WHOQOL-BREF, World Health Organization-Brief Version. Bolded measures are the core assessments for persons with HD. **indicates that measure is an American Physical Therapy Association Academy of Neurologic Physical Therapy core outcome measure for assessing adults with neurologic conditions undergoing rehabilitation [12].
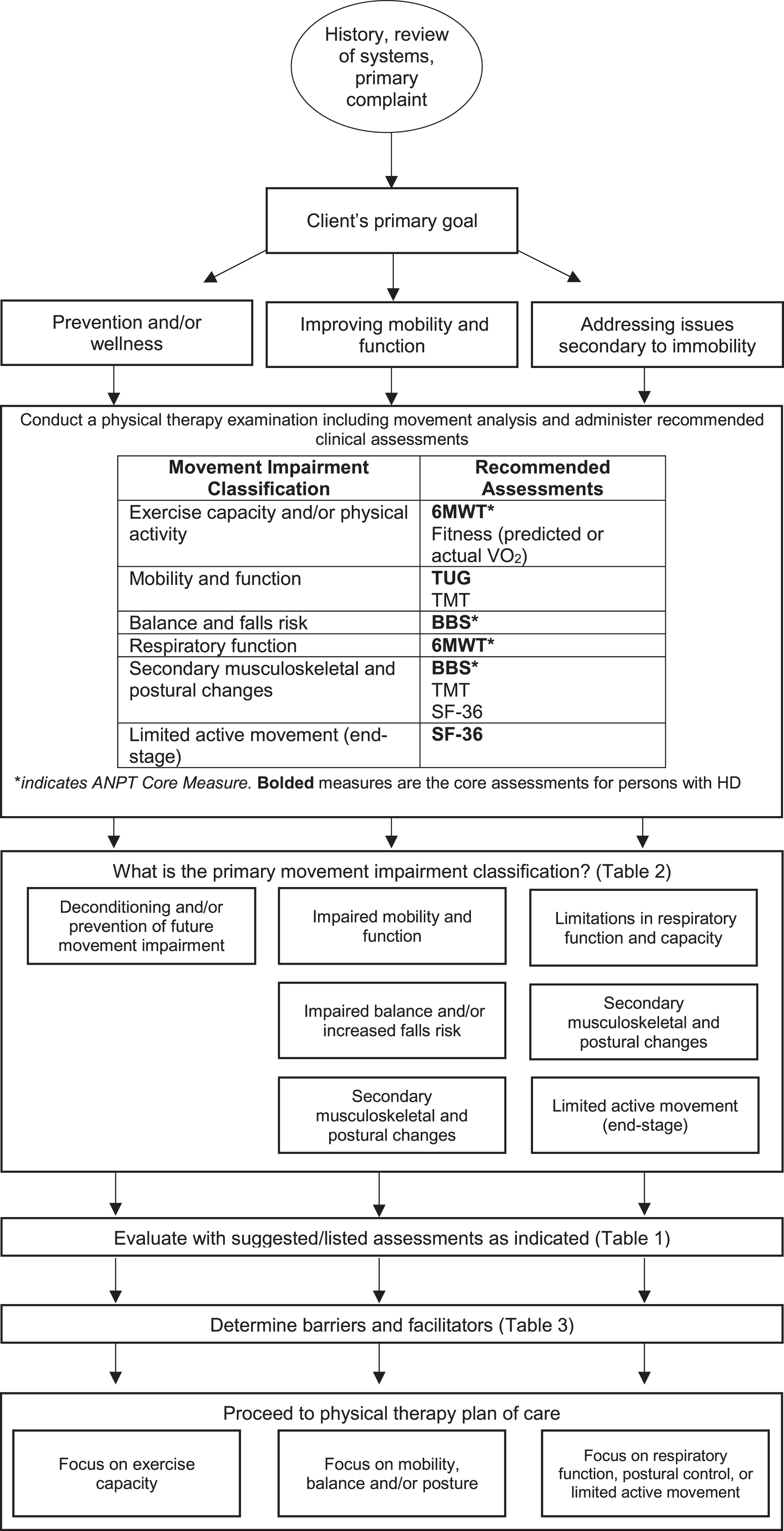
Physical Therapy Evaluation Decision Tree. This figure presents a recommended algorithm for physical therapists to follow in their evaluation of a person with Huntington’s disease. 6MWT, Six-minute walk test; BBS, Berg Balance Scale; SF-36, Medical Outcomes Study Short-Form 36; TMT, Tinetti Mobility Test.
Core assessments for HD
For measurement of aerobic fitness and endurance, we selected the Six Minute Walk Test (6MWT) as a core assessment because its psychometric properties have been evaluated in HD, it is commonly administered in physical therapy practice, and it is a core measure recommended by the ANPT. However, the 6MWT measures sub-maximal aerobic capacity rather than maximal capacity and may be challenging to administer in manifest HD because of the demands of sustained attention. While cardiopulmonary exercise testing using VO2 measures is considered the gold standard for measuring aerobic capacity, we did not select it as a core assessment because it has limited psychometric data in HD, and it is difficult for persons with HD to maintain consistent lip closure on the standard mouthpiece to provide accurate measurement. Further, VO2 measurement is limited by ecological utility as the required equipment and experienced administrators are not commonly available in the clinic setting. Future work needs to examine if predicted aerobic capacity using either standard algorithms (i.e., 220-age) or algorithms adapted for HD have clinical utility. The Timed Up and Go (TUG) test was selected over the Tinetti Mobility Test (TMT) as a core assessment for measuring mobility and function because it is more commonly used and takes less time to administer than the TMT. However, the TMT may be used by physical therapists needing a more detailed assessment of balance and gait deficits than the TUG. The Berg Balance Scale (BBS) met all of the criteria to be included as a core assessment of balance and falls risk. The Medical Outcomes Study Short Form 36 (SF-36) was selected as a core assessment because it was the only patient-reported health-related quality of life measure that met the modified MDS recommended criteria. However, it is more commonly used in research than in clinical practice and the length of time to administer it makes it impractical to use in a variety of clinical settings. Physical therapists may want to consider using the WHODAS for assessing quality of life because it has excellent clinical utility in HD, is able to distinguish between manifest and prodromal HD, is more responsive to change than the SF-36, and has moderate convergent validity with the SF-36. Additional research is needed on the WHODAS to determine reliability and minimum detectable change before including it as a recommended measure. The core assessments should be part of the clinical examination of all patients with HD and those with good responsiveness can be used as outcome measures while some may be used as screening tools to differentiate between fallers and non-fallers.
GUIDELINE-BASED DECISION TREES
Physical therapy evaluation decision tree (Fig. 1)
Physical therapists should conduct a thorough examination of each person with HD, beginning with a detailed history, review of systems and primary problem(s) [13]. The next step in the flow chart is selection, administration, and interpretation of the recommended clinical assessments for HD (Fig. 1). From the subjective and objective examination findings, the therapist prioritizes the individual’s goals throughout the continuum of care, beginning with prevention and wellness at the early stages of disease, improving mobility and balance during the early-to-mid stages, and addressing issues secondary to immobility during the mid-to-advanced stages of disease. Therapists may decide to administer additional suggested/listed assessments (Table 1) to obtain more information on the person with HD’s movement deficits for treatment planning. Table 2 presents primary movement impairment classifications, and related impairments in body structure and function, activity limitations and participation restrictions for ambulatory and non-ambulatory persons, respectively. The final step in the evaluation process is to determine potential barriers and facilitators to participation in physical therapy (Table 3).
Primary movement impairment classifications and recommended interventions for persons with HD
ADL, Activity of Daily Living; HD, Huntington’s Disease.
Barriers and Facilitators of Exercise in Persons with HD
Physical therapy plan of care decision tree (Fig. 2)
The plan of care should be derived directly from the therapist’s evaluation and the individual’s goals. Using the decision tree, the therapist determines the primary focus of the plan of care, which we have divided into three areas according to the therapist’s prioritization of the person with HD’s goals as described in Fig. 1 : 1) exercise capacity; 2) mobility, balance and/or posture; and/or 3) respiratory function, postural control and/or limited active movement (Fig. 2). This individualized plan of care should address specific movement system deficits that have been identified while optimizing factors that facilitate and/or remove barriers to compliance (Table 3). The plan of care is adjusted based on regular assessment of outcome measures and it considers the individual’s values and preferences. Caregivers are a crucial element of any plan of care for individuals with HD and should be involved when appropriate. Both the person with HD and caregiver should be educated regarding the importance of ongoing physical activity [14]. Therapists should consider all factors and for those not addressed by physical therapy include appropriate referral to other health care providers such as occupational, speech and respiratory therapists, social workers, nutritionists, nurses, and neuropsychologists (Fig. 2).
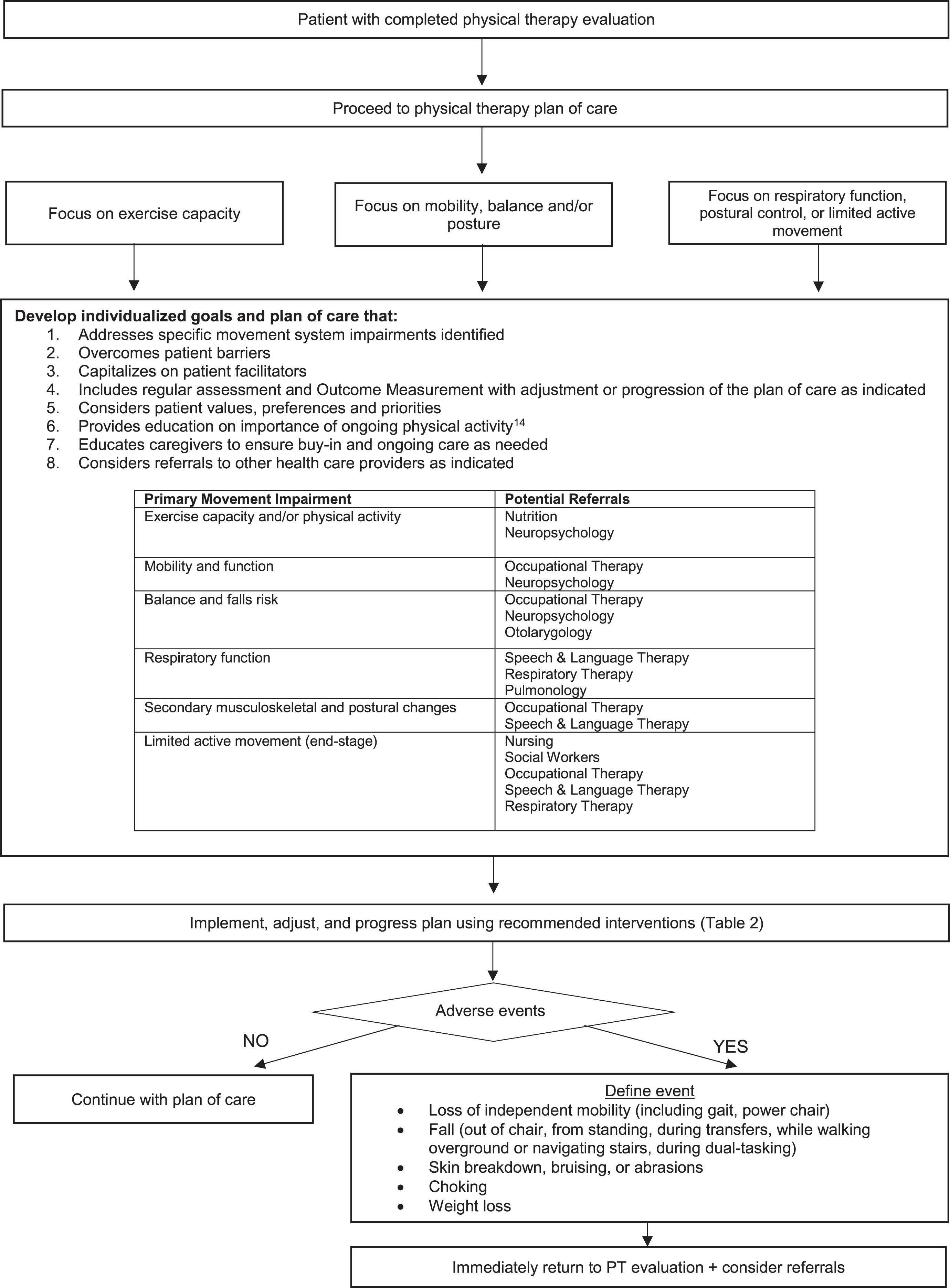
Physical Therapy Plan of Care Decision Tree. This figure presents a recommended algorithm for physical therapists to follow in their development of a plan of care for a person with Huntington’s disease.
Recommended interventions based on the primary movement impairment classification that were published in a clinical practice guideline are found in Table 2 [7]. Individuals with HD who engage in regular aerobic exercise in gym and home settings can improve their fitness. One-on-one supervised mobility training is recommended to improve walking. Therapist prescription of interventions such as task specific training or exercises that challenge balance by including narrowed base of support, reliance on vision and changes in direction are proposed as beneficial interventions for individuals with balance deficits. Respiratory training and an individualized program to improve postural control may be prescribed for individuals with respiratory and postural changes [7]. End-stage care for individuals with HD may include provision of positioning devices and encouragement of individuals with HD to remain active based on their abilities. Caregiver education and involvement are crucial during later stages of the disease. Throughout the plan of care therapists should monitor for adverse events and declines in condition that could result in a loss of independence and/or medical emergencies (Fig. 2). Appropriate referrals to health care professionals should be made.
APPLICATION OF THE DECISION TREES TO PATIENT EXAMPLES
To better illustrate the use of these algorithms (Figs. 1 and 2), we provide example patients (Table 4). As seen in this table, the decision trees allow therapists to adapt and individualize assessment and plan of intervention for persons at early, middle, and late stages of the disease.
Application of decision trees to patient examples
ADL, Activity of Daily Living, TFC, Total Functional Capacity; HD, Huntington’s Disease; UHDRS, United Huntington’s Disease Rating Scale.
SPECIAL CONSIDERATIONS IN THE PHYSICAL THERAPY MANAGEMENT OF PERSONS WITH HD
HD is a complex disease with most individuals presenting with a triad of cognitive, motor, and behavioral impairments that impact functional abilities. Cognitive dysfunction, in particular, can be a barrier to evaluation of the person with HD and implementation of the plan of care. Cognitive dysfunction may also manifest as mobility impairment [15, 16] or difficulty performing tasks requiring simultaneous motor and cognitive function [17, 18], thus impacting the ability to perform daily life tasks. In early HD, individuals may exhibit subtle problems with memory, thinking, and planning activities [19]. Thus, therapists may wish to include an assessment of dual-task [17, 20–26] in addition to the core set of recommended outcomes (Fig. 1) to monitor dual-task performance over time; our recent work suggests that the TUG Cognitive may be a sensitive measure of dual-task walking in HD [20]. Providing clear instructions and written materials and including the caregiver and/or family in education can help to overcome this barrier throughout the disease course. Considering the learning style of the person with HD may also be helpful; providing videos may allow for greater adherence in some persons with HD compared to photos of the exercises alone. Another strategy may be to introduce only a few exercises at once, allowing the person to become independent with these before adding additional home exercises. To ensure understanding, the therapist should ask the person with HD to demonstrate the exercise and repeat instructions to ensure safety.
Apathy or lack of motivation can also significantly impact engagement in exercise and affect outcomes [27]. A frank discussion with individuals with HD about activities they enjoy will allow the therapist to tailor the rehabilitation program to the individual’s interests, capitalize on salience and maintain sufficient intensity in the program. Apathy is common among persons with HD and related to quality of life and physical function [28]. The therapist should educate care partners on the importance of routine exercise (i.e., at the same time each day), keeping a log of their daily activity to see progress, and having a supportive exercise partner. Studies in persons with HD have demonstrated that a supportive caregiver can be the difference between success and failure with an exercise program [29]. The therapist should also stress the importance of frequent in-person check-ins to update the wellness plan and monitor function.
IMPLEMENTATION OF THE GUIDELINES
Clinical practice guidelines encourage the use of evidence-based practice and reduce variation in treatment. In a rare disease like HD, such guidelines can be particularly useful, as clinicians are unlikely to encounter persons with HD on a regular basis. To assist physical therapists to implement the guidelines, we propose strategies to address potential barriers, as well as facilitators, to implementation.
Strategies to overcome barriers to implementation
Physical therapists who plan to work with individuals with HD should seek specialized knowledge and training to be able to manage the unique symptoms and impairments of HD. Accessing freely available resources available from the Academy of Neurologic Physical Therapy (https://www.neuropt.org) Synapse Education Center (https://www.anptsynpasecenter.com) can facilitate the knowledge translation of the clinical recommendations [7].
Due to the complexity of the disease, time and resources needed to examine, evaluate, and treat people with HD may be more than with other neurodegenerative diseases. For example, it may be helpful to have a quiet space where therapy can be performed if the individual is easily distractible or becomes agitated. Care provided by physical therapists in the home is an environment that frequently works well for individuals with HD due to issues with transportation. Recommendations for home health therapists are to have a heart rate monitor and/or pulse oximeter available along with a gait belt and balance equipment such as a thick foam pad.
Finally, as mentioned earlier, caregiver support is critically important for the success of the person with HD undergoing rehabilitation. Physical therapists are encouraged to engage the caregiver in education early and often, including strategies on how to help people with HD stay active and adhere to physical therapy exercise recommendations. Specific education on the importance of exercise throughout the disease course is warranted. Caregivers may also benefit from resources available from the European Huntington’s Association (https://eurohuntington.org/active-huntingtons/).
Facilitators to implementation
Ideally, individuals with HD should receive care at a multidisciplinary clinic or within a health care provider network consisting of providers specially trained in HD who can work together to help manage patients with HD. However, clinical pathways that support patient early referral and treatment flows congruent with the decision trees in this paper can facilitate direct integration of patients with HD into local practice settings. This, in turn, will facilitate the use of evidence-based treatments in the management of persons with HD.
A critical step in the knowledge translation process is the wide-spread implementation of guidelines into clinical practice. In the context of models of implementation science,30 future research should develop knowledge translation tools that facilitate the adoption of these guidelines across settings and across the disability spectrum, to meet the needs of persons with HD. Within the translation phase of the implementation science model, a clear plan for dissemination is needed for individuals and organizations to use the information to improve the health of persons with HD. Importantly, adoption of knowledge translation by institutions requires training, financial resources and improving organizational capacity. To aid in implementation the European Huntington’s Disease Network Physiotherapy Working Group has made the CPG available in both lay language formats and in multiple languages (https://www.ehdn.org/de/clinical-guidelines/).
Additional research is needed to advance evidence-based practice for persons with HD. Our review of clinical assessments in HD revealed very few measures specifically developed for persons with HD; future work should not only determine psychometric properties of existing measures within the HD population, but also work to develop HD-specific assessments. Research to determine optimal clinical assessments for use with persons with HD through a Delphi process may be particularly useful. Large-scale collaborative trials are needed to systematically quantify outcomes through comparative effectiveness research to determine the best physical therapy interventions for persons with HD at each disease stage and within each movement impairment classification.
CONCLUSION
In summary, this work adds to the current literature by establishing a core set of clinical assessments for persons with HD and providing evidence-based decision trees to aid in the implementation of a physical therapy plan of care for individuals with HD. Our algorithms overcome limitations of prior approaches by spanning disease stages and guiding decision making based on the individual’s primary movement impairment classification. The tools developed by this study (decision trees and core set of measures) are immediately scalable and can be easily implemented by physical therapists into clinical practice to improve rehabilitation for persons with HD.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.