
Abstract
Background:
Studies have assessed the therapeutic effect of music, dance, and rhythmic auditory cueing for patients with Huntington’s disease (HD). However, the synthesis of evidence in support of their positive impact on symptoms is lacking.
Objective:
We conducted a systematic literature review to evaluate the potential benefits of music, dance, and rhythm on the cognitive, psychiatric and motor function in patients with HD.
Methods:
Two- and three-keyword searches and a manual search identified medical literature published from 1999 through 2019. We considered literature that assessed outcomes of art-based rehabilitation programs or individual modalities for persons with early, middle, or advanced HD. Structured analysis was conducted using data entry tables with categories for patient health status, art methods, and outcomes.
Results:
Seven articles and six abstracts met eligibility criteria, of which nine evaluated art-based rehabilitation programs. Studies mainly assessed cognitive, psychiatric, and motor functions through music, dance, or rhythm modalities. Although results were conflicting, in summary improvements to motor function were dependent on disease severity and more responsive to art therapy programs than rhythm-motor synchronization. Benefits to global cognition that resulted from rhythmic training correlated with microstructural changes. Qualitative data verified a positive impact on language production, chorea, behavior, and quality of life.
Conclusions:
Our review has shown a potential benefit of music, dance, and rhythm for patients with HD, which is particularly important for a disease that has no cure. Art forms seemed to affect cognitive, psychiatric, motor, psychosocial, and neuroanatomical domains. However, evidence is preliminary, warranting further investigation to establish the foundation for this field.
INTRODUCTION
Huntington’s disease (HD) is an autosomal dominant neurodegenerative disorder characterized by striatal and basal ganglion atrophy [1–4]. Cognitive, psychiatric, and motor dysfunctions progress through early, middle, and advanced phases that correspond to five HD stages on the Shoulson and Fahn Total Functional Capacity (TFC) scale [5–7]. Striatal neuropathology is associated with cognitive and psychiatric functions [8–10] that often precede motor deficits [8–12]. Cognitive impairments are observed in executive function, memory, affective processing, and psychomotor speed [7, 13–15]. Psychiatric symptoms, including irritability, depression, anxiety, apathy, disinhibition, and emotion dysregulation, are common in HD [16–19]. As the clinical hallmark of HD [20], motor impairments initially impact voluntary motor functions such as gait and balance [21] and evolve to involuntary choreiform movements [20]. The triad of HD symptoms are interconnected as a result of cortical loops that coordinate cognitive, emotional, and motor functions [22].
Factors of disease presentation, such as age at onset, rate of decline, and severity of symptoms vary among the HD cohort [7]. However, since there is currently no cure or disease-modifying therapy [23], there is a consistent need for long-term, multidisciplinary care through pharmacological [24, 25] and non-pharmacological [26, 27] interventions. These methods may reduce or stabilize disease progression in other progressive neurodegenerative disorders, such as Parkinson’s disease (PD) [7]. Recent studies have investigated the use of physical therapy for HD patients [28–32]. Multidisciplinary rehabilitation programs are safe and feasible interventions that positively affect verbal learning and memory, anxiety and depression, quality of life, balance, spatial-temporal gait parameters, and gray matter changes [33–36].
In addition to physical exercise, there may be beneficial health effects of using art such as music and dance in patients with neurological diseases [37–39]. Some of these effects could potentially arise from enhanced neuroplasticity; however, empirical data is lacking. Specifically, pathways of emotion are activated in localized brain areas such as the amygdala, cingulate cortex, and hypothalamus [38]. In addition, the use of sensorimotor processing in art interventions may strengthen synaptic connections between auditory and motor cortices and increase localized areas such as the corpus callosum and basal ganglia [37]. Neuroplastic features are specific for the therapeutic modality. For example, listening to music improves global neuroconnectivity and atrophic recovery, while playing a musical instrument, singing, or dancing increases gray and white matter in frontotemporal areas and alters neurochemical levels including endorphins and dopamine [37, 40]. As a result, music (MT) and dance movement therapies (DMT) in conjunction with conventional clinical interventions have a potential to positively affect cognitive, psychiatric, and motor functions for persons with progressive neurodegenerative disease. Studies give a particular focus on PD patients and associated benefits from dance exercise programs that use MT and rhythmic auditory cueing [39, 40]. Findings show improved motor control, gait, spatial memory, functional well-being, and quality of life [41–44]. The rationale for using MT and DMT in rehabilitation programs is the idea that music and dance are specialized auditory and motor forms that induce specific neuroplastic changes [37]. Therefore, the therapeutic outcomes associated with art-based rehabilitation are potentially distinct to that of traditional physiotherapy [37, 45–48].
Given the positive effects of art-based rehabilitation programs for persons with other neurodegenerative diseases [49], there may be similar benefits for patients with HD. However, few studies have examined MT, DMT, or rhythmic auditory cueing in clinical practices specific to HD, rendering us unable to define potential therapeutic outcomes associated with art-based rehabilitation in patients with HD. In the past decade, there has been a slight increase in the number of HD studies investigating MT protocol proposals [50], MT assessment tools [51], clinicians’ experiences of MT [52–54], and music perception abilities [55]. But yet, there lacks a greater focus on MT/DMT outcomes for persons with HD in comparison to other neurodegenerative diseases.
In 2015, a systematic review on the use of MT for patients with HD was published [56]. However, it reviews studies published from 1976 to 2001, including one study published in 2007, and focuses primarily on the history of MT and MT methods. As such, there is a need for an up-to-date systematic review of the literature in the past two decades that includes the cognitive, emotional, and motor outcomes of MT, DMT and rhythmic auditory cueing for HD. We did a systematic review to study the formats and effects reported in the literature on the therapeutic use of music, dance, and rhythmic auditory cueing for patients with HD.
MATERIALS AND METHODS
The systematic review adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement guidelines [57].
Search strategy for study selection
A literature search limited to English-language studies published from 1999 through October 2018 was first performed in November 2018 using PubMed, Scopus, and Web of Science electronic medical databases. Additionally, we conducted a manual search of included studies and systematic reviews in EMBASE. We repeated the literature search in April 2019, which was limited to English-language studies published from 1999 through 2019. This yielded one additional study for inclusion. The search strategy utilized a two- and three-keyword search. The two-keyword search used the following terms: (“Huntington’s [disease]”) AND (“music” OR “music therapy” OR “dance” OR “dance exercise” OR “dance rehabilitation” OR “[rhythm] [auditory] cueing”). The three-keyword search used the following terms: (“Huntington’s [disease]”) AND (“motor [function]” OR “cognitive [function]” OR “psychiatric [function]” OR “quality of life”) AND (“music [therapy]” OR “dance [therapy]” OR “[rhythm] [auditory] cueing”). A total of 278 searches were gathered, of which 184 were duplicates, yielding 94 unique search results.
Eligibility criteria
Included studies met the following criteria: 1) human participants received a genetically or clinically confirmed HD diagnosis 2) the therapeutic effect of art-based rehabilitation was evaluated quantitatively or qualitatively and 3) published research was an article, book chapter, or conference abstract.
This review considered protocols that incorporated MT, DMT, and rhythmic auditory cueing modalities for patients with prodromal, early, middle, or advanced HD and their caregivers. The rationale for including MT, DMT, and rhythmic auditory cueing is that each art intervention incorporates different methodologies. For example, MT and DMT utilize music and dance, respectively, to target domains of function. Conversely, rhythmic auditory cueing is a form of rhythmic training that synchronizes specific functional domains, such as speech and motor movements, with rhythmic patterns.
Studies that were carried out in the community (i.e., public dance studios), patients’ homes, rehabilitation centers, or hospitals were also considered. Quantitative syntheses included cognitive, psychiatric, and motor outcomes. Outcome measures of cognitive function included verbal communication, psychomotor speed, and executive functions. Outcome measures of psychiatric function included emotional regulation and levels of depression, anxiety, apathy, and aggression. Outcome measures of motor function included balance, spatial-temporal gait parameters, and fine motor skills. Studies that reported microstructural outcomes and psychosocial outcomes (i.e., quality of life) were also considered. Qualitative syntheses included patient and/or caregiver feedback regarding the efficacy, safety, and feasibility of the program.
Exclusion criteria were proposals of study designs, assessments of clinical protocols, evaluations of novel measurement tools, and systematic reviews or meta-analyses. Of the 94 unique literature searches, 81 met at least one exclusion criterion, yielding 13 total studies for inclusion in the systematic review (Table 1). The flow chart of the search process and outcome is shown in Fig. 1.
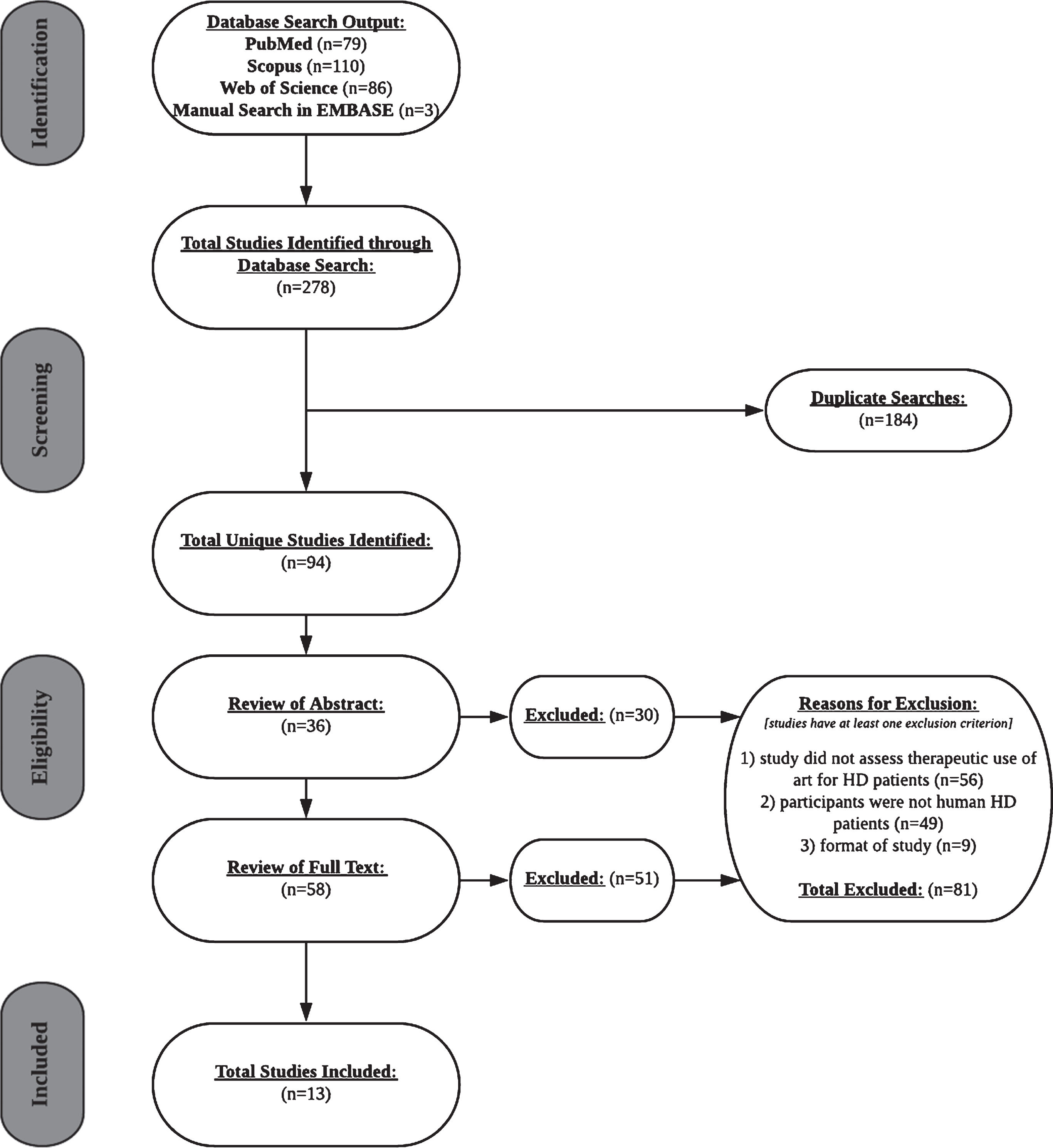
PRISMA flow chart of the selection process of included studies.
Design and study population of seven articles and six abstracts on the therapeutic use of art
Data extraction
After reviewing 36 abstracts and 58 full texts, 30 and 51 studies were excluded, respectively. 56 excluded studies neglected to examine therapeutic effects of art. Participants of 49 excluded studies were either clinicians, persons with other neurodegenerative diseases, or HD animal models. 9 studies were excluded due to literature format (i.e., study protocol proposal, systematic review). Data was extracted from published conference abstracts as a result of the lack of literature.
Outputs for keyword combinations in each database were recorded in structured tables during the search process. Data entry forms had the following categories: research setting, aims, study design, procedure, participant sample (sample size), participant age and gender (mean±SD), art form, measurement tools, outcome measures, and results.
Data synthesis and analysis
Due to the limited number of studies that assessed the cognitive, psychiatric, and motor outcomes of MT, DMT, or rhythmic auditory cueing for HD patients, findings from included studies were synthesized and summarized as descriptive results.
RESULTS
This systematic review included seven research articles published between 1999 and 2019 in English-language journals (Table 1). Data was collected from six conference abstracts (see Tables 1–3) but missing information led to its exclusion from the primary synthesis.
Descriptive characteristics of included studies
Studies originated from North American, European, and Australian countries. Research settings included participants’ homes (n = 2), a dance studio (n = 1), long-term care facilities (n = 1), and rehabilitation centers (n = 1). Two studies did not specify research setting. Cross-sectional studies [59, 68], randomized controlled trials (RCT) [69, 70], cross-over [62], and non-randomized [64] pilot clinical trials were included. Studies assessed a combination of cognitive (n = 3), psychiatric (n = 3), motor (n = 5), psychosocial (n = 2), and microstructural (n = 2) outcomes. One study evaluated program feasibility and safety [62]. Outcomes were quantitatively [59, 68–70] and/or qualitatively [62, 69] obtained.
Participants
Studies included patients with HD [62, 68] or compared patients to age-matched healthy control subjects [59, 70]. Early, middle, and advanced phases of HD were represented [61, 68–70]. Two studies did not specify disease phase but provided information on patient functionality. Participants included both males and females and were in early-to-middle adulthood (Table 1).
Research aims and procedures
The effect of MT, DMT, and rhythmic auditory cueing for patients with HD was examined by evaluating cognitive [64, 70], psychiatric [62, 70], motor [59, 69], psychosocial [62, 69], and/or neuroanatomical [64, 69] changes in response to art-based clinical programs [62, 70] or external rhythmic cueing [59, 68] (Tables 2 and 3).
Functional outcomes of two programs were compared to control treatments without art [62, 70]. All studies that independently assessed rhythm compared gait parameters [59, 68] or bimanual hand coordination [61] across cueing conditions and health status.
Features of MT, DMT, and rhythmic auditory cueing
Art modalities, genres, and instruments
Studies evaluated a combination of music (n = 4), dance (n = 1), and rhythm (n = 5) modalities (Table 2). Rhythmic patterns included Brazilian samba, Spanish rumba, West-African kuku, and Cuban son [64] as well as folk music [68] and contemporary dance [69]. All rhythmic patterns were external auditory cues since they required the use of an external source, such as an instrument or metronome, as opposed to an internal source, such as singing. One study allowed participants to select their preferred music genres [62]. Studies used instruments such as bongo drums [64], metronomes [59, 68], or computerized melodies [62]. These instrumental features distinguished the use of musical from non-musical stimuli, which are considered to be independent forms of auditory information [37]. In addition, the use of instruments to create live music or computerized music may influence the emotional salience of auditory input [37]. One study lacked this information [70].
Characteristics of art forms in seven articles and six abstracts
Aims, interventions, and outcomes in seven studies and six abstracts on the therapeutic use of art
Neurologic art therapy techniques
Included studies lacked information on the use of art therapy techniques. However, specific MT protocols were identified in abstracts [58, 63]. Of these studies, two used MT for speech and language rehabilitation via melodic intonation therapy (MIT) [63, 71] and modified-MIT in the form of the Speech Music Therapy for Aphasia (SMTA) program [58, 72]. MT was additionally used for sensorimotor rehabilitation by combining rhythmic auditory stimulation (RAS), patterned sensory enhancement (PSE), and therapeutic instrumental music performance (TIMP) techniques into one clinical program [60, 74].
Methods (structured direction or improvisation)
All studies required participants to follow structured directions administered by an in-person instructor [69, 70], a pre-recorded tape [62, 64], or set rhythmic patterns for motor synchronization [59, 68]. Two clinical programs combined structured direction and improvisation techniques by using a structured protocol that allowed participants to engage in artistic creativity through dance [69] and music [70].
Methods (individual or group sessions)
Studies that evaluated rhythmic auditory cueing independently from a clinical program administered protocol individually to participants [59, 68]. In studies that assessed the efficacy of a DMT program, individual [62] and group sessions [69] were utilized. Two of the included studies chose individual or group sessions based on patients’ needs [64, 70].
Methods (instructor and participant roles)
Instructor roles ranged from dictating rhythmic patterns for participants to follow through movement [59, 68] and MT [64] to guiding program safety [62] and structure [69, 70] as participants took the lead. Participants coordinated movements to external cues [59, 68], danced [62, 69], listened to music [70], or played instruments [64].
Cognitive function outcomes
One non-randomized pilot clinical trial evaluated changes to verbal working memory and attention, multi-tasking, verbal/category fluency, and processing speed that resulted from participation in a rhythmic drumming exercise program [64] (Table 1). Measurement tools included the standard dual task [75], Trails Making Test (TMT) [75], Stroop task [76], Digit Symbol Substitution Test (DSST) [77], and Delis and Kaplan executive function battery [78]. Findings showed significant improvements to memory and attention, verbal/category fluency, and DSST post-baseline accuracy scores as well as TMT and Stroop task response times [64] (Table 3). Another multi-center RCT compared MT to recreational non-MT therapy by assessing changes to social-cognitive functioning [70] on the Behavior Observation Scale Huntington (BOSH) [79] (Table 1). Improvements to social-cognitive subscale scores achieved significance for participants of recreational therapy but not MT (Table 3). In another RCT, a contemporary dance workshop was evaluated by observing changes to UHDRS cognitive scores including Stroop task [76], Symbol Digit Code [6], Mattis Dementia Rating Scale (MDRS), a measure for global cognitive functioning [80], and TMT [75]. Changes to cognitive scores were insignificant.
Cognitive outcomes were additionally examined in conference abstracts, which included language processing [58], memory and attention [60], and development of consciousness [67]. Positive patient feedback was collected on a novel MT program for speech rehabilitation [58].
Psychiatric function outcomes
A cross-over pilot clinical trial [62] evaluated the efficacy of a novel video-game DMT program by assessing balance confidence with the Activities-Specific Balance Confidence Scale [81] (Table 1). Changes to baseline scores did not reach significance. Another multi-center RCT used the Problem Behavior Assessment (PBA-s) [82] and BOSH [79] to compare improvements to mental rigidity, aggression, and behavior severity across MT and recreational therapy programs [70]. Improvements to individual estimated mean scores were not significantly different across treatment groups (Table 3). Another RCT that used the PBA-s [82] and Lille Apathy Rating Scale (LARS) [83] to evaluate the efficacy of contemporary dance workshops did not find significant improvements to behavior.
Other psychiatric outcomes were represented in conference abstracts, which included overall mood [60, 67], fear and anxiety [58, 65] and behavioral control [63, 65]. Preliminary qualitative findings showed that MT facilitated ease of speech production [58], increased patients’ motivation [60], and reduced challenging behaviors of an in-patient during morning-care procedures [63]. Additionally, DMT reduced fears and tensions associated with HD progression and increased caregivers’ empathic understanding of the illness experience [65].
Motor function outcomes
Two cross-sectional studies compared gait parameters [59] and modulation of gait velocity [68] across external rhythmic cueing and no cueing conditions (Table 1). A significant benefit of auditory cues for kinematic gait parameters and velocity modulation was not observed [59, 68] (Table 3). Although one study found a trend towards improvement in gait, significance was not achieved [59]. In fact, in one study that included musical cues, music, but not rhythmic patterns, impeded gait velocity modulation [68]. In another study that evaluated the effect of contemporary dance workshops on motor function using the UHDRS [5], findings showed a decrease in motor impairments post-DMT and an increase in motor impairments after usual care that did not involve art forms [69]. Another clinical trial [62] evaluated the efficacy of a novel video-game DMT program by assessing changes to spatiotemporal gait parameters through the GAITRite walkway system [84]. Significant improvements to certain gait parameters were dependent on the severity of HD, such as forward heel-to-heel base of support [62].
The clinical trial [62] also compared balance outcomes between DMT and non-DMT treatments through the Four Step Square Test (FSST) [85] and Tinetti Mobility Test (TT) [86] (Table 1). Significant differences in balance scores were not observed across treatment groups. Additionally, a cross-sectional study used bimanual cranks [87] to evaluate fine motor skills by comparing bimanual in-phase and anti-phase hand movements across external rhythmic cueing and no cueing conditions [61]. Findings showed that coordination accuracy and velocity were not influenced by the use of rhythmic cues [61] (Table 3).
Motor outcomes such as language production [58, 63], fine motor skills [60], posture [60], and choreiform movements [63] were also examined in conference abstracts (Table 1). Clinical observations collected in one case report showed improvements to motor control and speech production [63]. Patient feedback from another study was positive for the use of music in speech therapy [58]. Additionally, an MT clinical trial showed an improvement trend in fine motor sub-scores on the Unified Huntington’s Disease Rating Scale (UHDRS) [5]; however, significance was not achieved [60] (Table 3).
Psychosocial outcomes
Quality of life
One clinical trial examined the impact of DMT compared to non-DMT programs on patients’ quality of life by utilizing the World Health Organization Quality of Life-Bref scale (WHO-QoL) [88, 89]. Significant differences in WHO-QoL post-baseline scores across treatment groups were not observed. Another RCT did not find a significant impact of contemporary dance workshops on quality of life based on the Quality of Life Index (QLI) [90].
Two conference abstracts also evaluated quality of life connected to language production [58] and overall functionality [66]. Assessment methods included the Parkinson’s disease Questionnaire (PDQ-39) [91], the Nottingham Health Questionnaire (NHQ) [92], the Functional Independence Measure (FIM) [93], and Barthel Scales [94]. Preliminary patient feedback confirmed the positive impact music-based speech therapy had in the daily navigation through complex conversations [58].
Participant satisfaction
One RCT evaluated patients’ experiences of DMT through qualitative interviews [69]. Patient feedback suggested that “contemporary dance altered the way [patients] ‘felt and lived in their bodies.”’ Two conference abstracts assessed participant satisfaction of DMT programs through surveys [65, 66]. Preliminary findings suggested high satisfaction levels from patients [65, 66] and their caregivers [65], though specific outcomes were inconclusive.
Neuroanatomy
One non-randomized pilot clinical trial evaluated the effect of a rhythmic drumming exercise program on subcortical basal ganglia volume [64]. Magnetic resonance imaging (MRI) showed significant changes to corpus callosal white matter microstructure, or myelinated nerve fiber bundles that positively correlated with improvements in global cognition. Another RCT evaluated the effect of contemporary dance workshops on brain volume [69]. Structured MRI (sMRI) and voxel-based morphometry (VBM) showed a volumetric increase in medial superior parietal and paracentral lobule structures post-DMT that is associated with compensatory mechanisms for spatial and somatosensory processing.
Program feasibility, adherence, acceptability, and safety
One cross-over clinical trial made comparisons between a video-game DMT program and a non-DMT program based on feasibility, adherence, acceptability, and safety [62]. Feasibility of DMT was confirmed through significant improvements to accuracy scores. High attendance and completion of both DMT and non-DMT indicated the adherence of programs. Additionally, positive feedback from patients suggested high acceptability of DMT and no adverse health events or injuries confirmed its safety. Another RCT found that contemporary dance workshops were adhered to through high attendance [69].
DISCUSSION
To our knowledge, this systematic review is the first to evaluate outcomes of MT, DMT, and rhythmic auditory cueing for HD patients. We synthesized quantitative and qualitative analyses from 7 prospective articles and 6 conference abstracts that assessed the impact of established art-based clinical programs or individual art forms on functioning. There was heterogeneity across all studies in the use of art modalities, methodologies, and therapeutic outcomes. The current review confirmed a potential positive effect of using art forms in conventional HD clinical practices. Half of the included articles found benefits of music, dance, and rhythm to cognitive, motor, and microstructural outcomes. Abstracts confirmed additional benefits to psychiatric symptoms and quality of life. Art forms were determined to be feasible and safe methods for HD patients. However, it is worth mentioning that limited studies led to the extraction of data from abstracts. Therefore, the field is currently underdeveloped, making it difficult to conclusively define the collective and distinctive benefits that result from MT, DMT, and rhythmic auditory cueing.
We found that improvements to cognitive function scores [64, 69] such as memory and attention, verbal and category fluency, and processing speed were significant. These changes were contradicted by insignificant changes to executive function subscales on the UHDRS [60]. Additionally, positive patient feedback of benefits to speech processing [58] conflicted with insignificant changes to social-cognitive baseline scores [70]. Inconsistencies in findings regarding cognitive outcomes may be explained by the comparisons between dissimilar art programs— rhythmic training [64] versus MT [60] and HSMT [58] versus general MT [70]. Additionally, outcome comparisons between dissimilar research designs— case report [58] versus RCT [70]— could inhibit consistencies in the synthesis. Our review may therefore suggest that the therapeutic effects of music, dance, and rhythmic training are unique to the art form, which potentially results from underlying differences in the neuroplastic effects of varying art interventions [37, 40]. For example, HSMT required persons to listen to music, which potentially stimulated global neuroconnectivity and atrophic recovery of speech production [58]. Conversely, social-cognitive scores improved upon persons improvising dance movements [70]. These findings may result from changes to dopamine levels that facilitated dopaminergic signaling in the amygdala, which is essential for social-cognitive functioning [95]. Findings additionally confirmed that a rhythmic drumming exercise program, which required sensorimotor processing, led to an overall volumetric increase in the corpus callosum [64]. These neuroplastic changes positively correlated with significant improvements in cognitive functions [64]. The results concur with findings from previous studies [37, 38], which suggest that there are potential neuroplastic effects of art interventions, specifically in subcortical basal ganglion areas, that positively affect functioning in cognitive domains. Rhythmic drumming may have additionally induced stronger synaptic connections between auditory and motor cortices that facilitated an intact exercise performance. It is worth mentioning that this was a within-study comparison that was not examined in other studies in the review.
We also found consistent patient feedback on perceived benefits for psychiatric functions. Studies demonstrated that both MT and DMT reduced fears and tensions associated with speech and motor dysfunctions, respectively [58, 65]. MT and DMT also motivated patients to continue a consistent exercise regime [60, 62]. These findings may result from the ability of MT and DMT to activate emotional pathways in the amygdala, cingulate cortex, and hypothalamus that improve mood and reduce anxieties related to HD progression [38]. However, qualitative syntheses were inconsistent with changes to balance confidence [62], depression, and apathy scores [69]. We predict that inconsistences in findings manifest from our synthesis of one patient’s feedback in a case report [58] or that of a very small sample size [60] with outcomes that represented larger samples [62, 69]. Additionally, studies’ lack of information on HD phase represented in participant samples potentially led to outcome cross-comparisons amongst patients with varying degrees of disease progression. As functionality of patients changes with severity of HD, so should the goals of art therapy. Therapeutic effects of art for HD patients should therefore be uniquely interpreted for each disease phase. While certain studies in the review indicated a relationship between feelings of fear and anxiety and motor dysfunctions [58, 65], other studies reported mood symptoms of depression and apathy without reference to an underlying cause [69]. There may be value in defining the causal relationship between features of HD pathology and psychiatric symptoms so that informative between-study comparisons can come to fruition.
In addition, the review has shown consistent benefits of art forms for motor function, which was found through positive clinician feedback and significant improvements in UHDRS scores [63, 69]. These findings complimented the consistent positive feedback from clinicians and patients on the use of MT for speech production [58, 63]. We expected to see a positive effect of art on motor control, considering that published studies have validated the evidence-based clinical use of dance to improve motor impairments of PD patients [41–44]. Additionally, we expected to find that improvements in UHDRS motor scores were accompanied by an increase in medial superior parietal and paracentral lobule volume as a result of participating in contemporary DMT [69]. These neuroplastic effects may result from sensorimotor processing, which is integral to dance [45]. Although HD and PD pathologies differ, various art forms provide similar benefits to these patient cohorts. MT, DMT, and rhythmic auditory cueing may therefore be pertinent for persons with other forms of neuromuscular disease. Our review also found positive effects of DMT on gait [62], which was not observed in studies that evaluated rhythmic auditory cueing [59, 68]. Generally, studies in the review found that synchronization of gait and hand movements to external auditory cues was impaired for all patients, yielding comparable outcomes to that of free movement [59, 68]. Therefore, our review has demonstrated a distinctive purpose of DMT for gait function that may be more adaptable to the HD phase.
We did not expect to synthesize psychosocial outcomes from less than a third of the included studies in the review. Considering that the concurrence of conventional and alternative treatment methods aims to promote quality of life and patient satisfaction, we expected to synthesize psychosocial functions across the majority of the included studies. Furthermore, to our surprise, findings showed inconsistencies in the comparison of positive patient feedback [58] to insignificant changes to life quality scores [62, 69]. It is worth mentioning that items on the WHO-QoL and QLI are not specific to the HD illness experience, which may account for observed inconsistences. However, levels of satisfaction were comparable between patients and their caregivers [65, 66], suggesting the potential for art forms to transcend healthcare roles.
In the synthesis of positive outcomes represented in the review, we present probable explanations that are supported by the included studies. First, the therapeutic use of art for persons with HD promotes neuroplastic effects to the brain that may reduce cognitive, psychiatric, and motor impairments or perhaps restore function. Because artistic activities such as music performance and dance require specialized cognitive and motor abilities to that of non-artistic activities, these changes may be distinct from that of conventional HD rehabilitation. Only two studies investigated neuroplastic effects as a result of art-based rehabilitation, so our understanding of this comparison is currently inconclusive. Second, music, dance, and rhythmic auditory cueing are conduits for motivating HD patients to engage in exercise. For a disease in which apathy is a clinical hallmark, it is essential to develop strategies to promote patients’ long-term and consistent engagement in exercise regimes. Our review has shown that art forms can maintain excellent attendance and achieve high satisfaction. Last, we have synthesized studies that represented patients across the entire spectrum of HD severity. As such, art methods work regardless of patients’ functionality, suggesting that it can be a consistent method of treatment that is flexible for change.
It is worth addressing limitations of this review. First, approximately half of the included studies were conference abstracts, limiting our access to vital details on art methodologies, participants, and general outcomes. For example, some conference abstracts provided minimal information on participants’ HD phase and the art therapy designs involved. We included conference abstracts because of the small number of relevant studies currently available. As a result, we had to synthesize studies with potentially few characteristic consistencies, making it difficult to gather informative comparisons. Without informational access, outcome comparisons between different art forms and patients at different HD stages was inevitable. Second, many of the studies we reviewed included small sample sizes, weak protocols, and a general span of investigated outcomes. This also contributed to between-study comparisons that involved unaccounted variability, hindering a collective synthesis. Although these limitations made it difficult to synthesize the therapeutic effects of art for patients with HD, recognizing these confounders allows us to understand the factors that may influence outcomes and therefore, avenues for improvement in future studies. Third, we limited our search to medical databases, excluding sources from artistic databases. Although this may have led to an unawareness of other relevant art-based programs and methodologies, we aimed to focus on the integrity of neurological information and scientific research designs, which is optimally supported by medical resources.
We present considerations for future research. First, art-based exercise programs should be tailored to individual phases of HD so that music, dance, and rhythm benefit rather than impede functioning. The development of phase-specific protocols may give patients with HD consistent access to clinical art forms that produce meaningful outcomes. Second, studies should determine the ways in which to effectively incorporate variety within one art method. Utilizing different artistic genres, instruments, and activities, for example, may increase patients’ affinity for art-based programs by catering to their preferences. As a result, programs can maximize benefits by directly targeting apathy. Third, the investigation of the therapeutic use of art should take the form of different study designs. As such, we can establish ideal methodological features to implement for the HD cohort. For example, one study concluded that an RCT was undesirable for evaluating cognitive functioning of patients with advanced HD [70]. Therefore, research designs must be altered to accommodate different disease presentations. Additionally, the investigation of differential outcomes of music, dance, and rhythm through neuroimaging techniques may better inform the future development of art-based rehabilitation programs. Lastly, few studies in the review assessed the impact of art therapy on the quality of life of family members or utilized caregiver feedback to determine the impact of music, dance, and rhythm on patients. Understanding caregiver roles may be particularly useful for characterizing outcomes for patients at middle-to-advanced disease phases as well as the ways in which these outcomes transcend patients to indirectly influence caregiver burden.
In conclusion, the review has provided preliminary support for the clinical use of music, dance, and rhythm for patients with HD, with a particular benefit to gait, global cognitive function, and subcortical plasticity. While it is evident that art forms are feasible and safe methods that garner caregiver and patient satisfaction, limited research has rendered us unable to conclusively determine the manner in which various neurologic art therapy techniques produce therapeutic outcomes. We recommend that future research compares responses of functional domains to art forms by evaluating the mechanistic differences of music, dance, and rhythm that may account for therapeutic outcomes.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
Footnotes
ACKNOWLEDGMENTS
This work has been possible through a grant from the U.S.-Norway Fulbright Foundation.