
Abstract
Air pollution exposures ought to be of significant interest for the United States (US) public as health issues will play a role in the 2024 elections. Citizens are not aware of the harmful brain impact of exposures to ubiquitous anthropogenic combustion emissions and friction-derived nanoparticles, industrial nanoplastics, the growing risk of wildfires, and the smoke plumes of soot. Ample consideration of pediatric and early adulthood hallmarks of Alzheimer’s disease, Parkinson’s disease, frontotemporal lobar degeneration, and amyotrophic lateral sclerosis and associations with neuropsychiatric and neurodevelopmental disorders in the process of setting, reviewing, and implementing standards for particulate matter (PM)2.5, ultrafine PM, and industrial nanoparticles must be of interest to US citizens.
Keywords
INTRODUCTION
Exposures to criteria air pollutants (ground-level ozone, particulate matter, nitrogen dioxide, sulfur dioxide, carbon monoxide, lead) as specified by the Environmental Protection Agency (EPA) in the United States (US) [1] and other environmental toxicants cause detrimental brain effects, starting in utero [2–9]. We have shown anthropogenic ultrafine particulate matter (UFPM) and industrial and natural nanoparticles (NPs) are present in normal term, preeclamptic, and early postconceptional human placentas from women residing in polluted Mexican cities [9]. UFPM and NPs are reaching fetal brain tissues [9]. The placental barrier is not limiting the access of environmental nanoscale Fe, Ti, and Al alloys, Hg, Cu, Ca, Sn, and Si. Thus, we ask: should the neuropathological hallmarks of Alzheimer’s disease (AD), Parkinson’s disease (PD), and the 43 kD transactive response DNA/RNA-binding protein (TDP-43) documented in forensic autopsies of children and young-adult residents in Metropolitan Mexico City (MMC) [7, 8], the accumulation of nanoparticles in placentas and fetal brains [9], the cerebral, cerebellar, and caudate atrophy in brain MRIs [10], and the cognitive impairment [11] in their seemingly healthy MMC young be of any concern for US residents?
They should be.
Brain damage in MMC residents likely starts in utero [9] and continues in pediatric ages, impacting academic and behavioral performances and health [7, 11], and increasing the risk of suicide in Apolipoprotein E allele 4 carriers, the most significant genetic risk factor for AD, with peripheral and neural effects starting in childhood [4]. While all pollutants are a concern, fine particulate matter (PM2.5, particles≤2.5μm), UFPM, and industrial nanoparticles (≤100 nm) composed of toxic metals, metalloids, and natural elements, are likely neuropathology culprits [7–15]. UFPM/NPs containing Fe, Ti, Al, V, Ni, Hg, Co, Cu, Zn, S, Si, Ag, Pt, Ce, La, Pr, and W are identified in the neurons, glia, and endothelium, compromising mitochondria, endoplasmic reticulum, Golgi apparatus, nuclei, and DNA of young MMC residents [7–9, 12–15].
AD, PD, and TDP-43 pathologies overlap in MMC residents’ first four decades of life [4, 15] (Fig. 1A,1B). Similar neuropathology has been documented in 365 University of Kentucky [16] autopsies of unimpaired and cognitively impaired white individuals, ages 83.8±8.8 years (Fig. 1C).
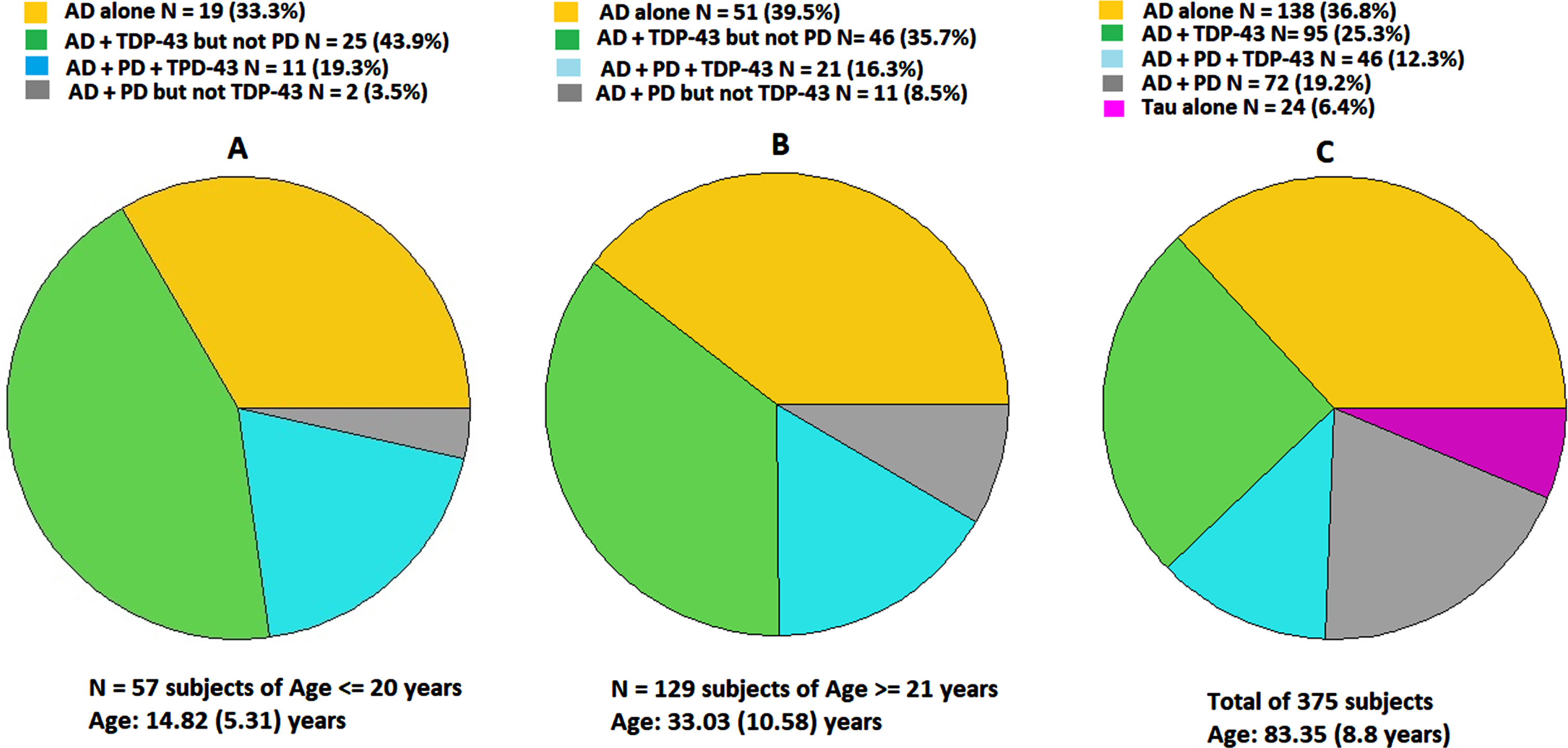
The overlap of AD (hyperphosphorylated tau, amyloid-β plaques), PD (α-synuclein), and TDP-43 pathology in the forensic autopsies of 14.8±5.3-year-old MMC residents (A) is also documented in 33.0±10.5-year-old MMC residents (B). Unimpaired and cognitively impaired older US residents show similar quadruple proteinopathies (C), a common substrate for cognitive impairment [16].
Karanth et al. [16] used a group-based multi-trajectory model to identify cognitive trajectories, including no decline, mild, moderate, and accelerated declines over the decade before death, using the Mini-Mental State Exam, Logical Memory-Immediate, and Animal Naming performance. Strikingly, AD neuropathologic change (ADNC) was present in over 80% of University of Kentucky Alzheimer’s Disease Research Center (UK-ADRC) cohort and > 86% of the National Alzheimer’s Coordinating Center (NACC) brains, along at least one comorbid pathology. Individuals in the moderate and accelerated decline groups had higher frequencies of quadruple misfolded proteins and the presence of TDP-43 with cerebrovascular pathologies. In Karanth et al. [16], random forest results suggested key cognitive trajectory predictors were strongly associated with Braak neurofibrillary tangle stage, brain atrophy, age at death, and brain weight and very relevant to our findings in young MMC urbanites: multiple pathologies were most common in trajectories with moderate or accelerated decline [16].
DISCUSSION
Why should AD, PD, and/or TDP-43 neuropathology documented in consecutive, MMC forensic autopsies, affecting 100% of 186 Mexican urbanites, aged 27.45±11.89 years with lifelong PM exposures and no extraneural significant pathology [14], be of interest to US residents? Because they present a serious and unattended health alarm and a grim picture for people elsewhere, exposed to PM2.5, and UFPM/NP pollution.
Braak and Del Tredeci described early subcortical and cortical tau pathology in AD sporadic preclinical phase [17] and stated, “ongoing formation of these tau lesions persists into end-stage Alzheimer’s disease and is not subject to remission”, thus hyperphosphorylated tau in MMC children and young adults is interpreted as a key AD hallmark, not subject to remission, and associated with a strong environmental component [7–9, 13–15].
On February 7, 2024, the US EPA announced a new and lower annual National Ambient Air Quality Standard for PM2.5 to 9.0μg/m3, down from 12.0μg/m3 [18]. The action is welcome news for public health. EPA had concluded the previous 12μg/m3 annual standard did not protect public health with an adequate margin of safety, as required by the Clean Air Act. In EPA cited studies [19] from the 131 references supporting a causal relationship between long- and short-term exposures to PM2.5 included cardiovascular and respiratory effects, and cancer. Key findings associating exposures to PM2.5 and neurodegenerative diseases, susceptible windows of prenatal and postnatal exposures, and neurobehavioral changes and brain structural pediatric changes in the US and across the globe were not cited [2, 20–32].
The new 9.0μg/m3 PM2.5 annual standard is still higher than the current guideline issued September 22, 2021, by the World Health Organization (WHO) of 5μg/m3 [33]. Remarkably, significant air pollution exposures disparities will persist and increase, affecting mostly people of color in lower income brackets, with reduced access to health care, and high occupational exposure risks [34, 35]. Bramble et al. [34] showed that higher exposures to multiple air pollutants and cumulative effects are disproportionately impacting historically marginalized communities, i.e., UFPM are higher than average for Black, 15%; Hispanic, 6%; Native American, 8%; and Pacific Islanders 11%. Valencia et al. [35] estimated that minorities within 100 m from major roads are exposed to up to 15% more PM2.5 and up to 35% more NO2 than their white counterparts.
We have an extraordinary, complex situation: de facto, millions of US residents will be living in PM2.5 non-attainment regions and in addition, we must deal with UFPM/NPs exposures because of 1) their ability to cross all biological barriers, reaching the brain and other critical organs (i.e., the heart), and 2) fossil fuel combustion- and friction-generated particle emissions are ubiquitous in the urban environment and not uniformly or even directly regulated. EPA will not adopt an ambient air quality standard for UFPM or UFPM emission regulations due to what it considers inadequate evidence. Yet, since this fraction of PM2.5 has strong neurodegenerative/neurobehavioral/brain structural associations [4, 20–32], the US may be well served by applying the precautionary principle and develop some policy interventions, especially since UFPM impact marginalized populations.
Use of advanced engine technology and fuels for the transportation sector, one of the largest sources of air and climate pollution in the US, might buy us some time. The use of modern engine designs, clean fuels, and robust post-combustion particle filtration have proven useful for addressing, at least partially, some UFPM emissions in some common applications.
The early development and progression of AD, PD, and TDP-43 proteinopathies, already killing thousands of Americans, and neuropathologically documented in UFPM/NPs exposed Mexican children and young adults should raise red flags about the need to understand this serious potential risk to urban and rural US populations.
An important, missing element in the US is an ambient air quality monitoring network for UFPM. This lack of monitoring data is hampering epidemiological UFPM studies. Monitoring UFPM should be federally implemented.
Neuropathological access to young forensic autopsies, i.e., in the first four decades of life, in cities across the US should help define precisely the aberrant neural protein pathology and its prevalence. Federal support for mechanistic research of neurodegenerative pathways associated with UFPM exposure is needed, along efforts for further regulatory interventions targeting mitigation of emissions and the explicit education of health workers in urban and rural communities.
We all should be aware that under lifetime exposures to PM2.5 above safe thresholds, the relentless development of AD, PD, and TDP-43 pathology could be in place. We need to be able to identify key neurotoxicants impacting neural risk trajectories in the developing brain, in the different environments across the US and pay special attention to the highly exposed, at-risk populations.
Wildfires are of particular importance to the US population [36, 37]. High levels of PM2.5 associated with the growing occurrence and intensity of wildfires in the US often exceed our current standards. From 2013 to 2022, an average of 7.2 million acres have burned annually, and the National Interagency Fire Center (NIFC) reported that 55,571 fires burned 2,633,636 acres in 2023 [37]. Humans were responsible for 89% of wildfires in the period 2018-2022 [37].
Wildfire UFPM emissions are a serious health problem [38–40]. They can result in short- and long-term health effects, including in utero brain damage, along with the development and progression of fatal neurodegenerative diseases and devasting effects on mental health, i.e., increased suicides [8–15, 38–40]. Molitor et al. [39] reported that in US rural counties, an additional day of wildfire smoke increases monthly mean PM2.5 by 0.41μg/m3 and suicide deaths by 0.11 per million residents. A 1μg/m3 increase in monthly wildfire-derived PM2.5 can lead to 0.27 additional suicide deaths per million residents (a 2.0% increase). These deaths are concentrated among demographic groups with high baseline suicide risk and high exposure to outdoor pollution: men, working-age, non-Hispanic Whites, with no college education [39].
Control of UFPM/NPs in ambient air, their atmospheric transformations, their industrial sources, wildfire prevention, education, and environmental management are important considerations if we are to prevent adverse effects in early pregnancies and all through neurodevelopmental stages.
Neurodegenerative diseases evolving from childhood and affecting populations living in air polluted environments ought to be preventable.
US voters would like to be assured that a significant part of the 13 million projected AD cases for 2050, the current 1 million PD, the 60,000 frontotemporal lobar degeneration, and the 18,000 ALS cases could be avoided, and future generations be protected if our pollution reduction efforts are strengthened and accelerated.
AD, PD, and TDP43 hallmarks in children have ushered a major evolving, difficult and yet unsolved health crisis of unprecedented magnitude in Mexico, with a current underprovided health infrastructure imposing serious limitations to an utterly progressively deficient health system [41] failing to protect its young vulnerable citizens.
US citizens need protection from environmental pollution.
We all care.
AUTHOR CONTRIBUTIONS
Lilian Calderón-Garcidueñas (Conceptualization; Data curation; Formal analysis; Investigation; Supervision; Validation; Writing – original draft; Writing – review & editing); Alberto Ayala (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Writing – original draft; Writing – review & editing); Partha S. Mukherjee (Conceptualization; Formal analysis; Investigation; Methodology; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
Lilian Calderón-Garcidueñas is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.