
Abstract
Background:
The healthcare needs of People living with Dementia (PlwD) (such as Alzheimer’s disease) are often unmet. Information about the needs of community-dwelling PlwD and their association with sociodemographic and clinical characteristics is needed to fill the knowledge gap regarding factors influencing unmet needs among PlwD and to conduct a comprehensive needs assessment to develop tailored interventions.
Objective:
To describe sociodemographic and clinical characteristics of the InDePendent study population with particular reference to determinants of unmet needs.
Methods:
We analyzed baseline data of the multi-centre cluster-randomized controlled trial (InDePendent) using descriptive statistics to describe patients’ sociodemographic and clinical characteristics and Poisson regression models to predict unmet needs, separated by sex. Data were collected personally via face-to-face interviews.
Results:
Most of the n = 417 participating PlwD were mild to moderately cognitively impaired, were not depressed, had an average of 10.8 diagnoses, took 6.7 medications, and had, on average, 2.4 unmet needs (62% of PlwD had at least one unmet need) measured by the Camberwell Assessment of Need for the Elderly (CANE). Low social support, a high body-mass-index, a lower education, functional impairment, and worse health status were associated with more unmet needs, regardless of sex. In women, higher unmet needs were associated with more depressive symptoms, a poor financial situation, living alone and not being recently treated by a general practitioner. In males, unmet needs increased with the number of medications taken.
Conclusions:
PlwD had a broad array of unmet healthcare needs, indicating primary healthcare provision improvement potentials. The results underscore the significance of early assessment of patient’s clinical characteristics and unmet needs as a basis for individualized gender-sensible intervention strategies.∥
Keywords
INTRODUCTION
Population aging is one of the most significant challenges healthcare systems face globally. This demographic change is associated with an increased prevalence of People living with Dementia (PlwD) (such as Alzheimer’s disease) [1, 2]. It is estimated that more than 55 million people worldwide are living with dementia, and according to forecasts, the number of PlwD is expected to rise to 139 million by 2050 [3]. In Germany, approximately 1.8 million individuals were living with dementia in 2021 and that number is expected to reach 2 million people aged 65 years and older by 2033 [1].
The German AgeCoDe study represents over 75-year-olds living in their own homes. Results show prevalences of cognitive impairment (23%), depression (8%), physical limitations (8%), and living alone (51%) [4]. Thyrian et al. [5] described the prevalence of socioeconomic parameters (e.g., 50% of PlwD live alone) and various clinical variables (e.g., 15% of PlwD suffer from depression) for PlwD in an ambulant setting in Germany (DelpHi MV Study, n = 516). Findings from the German IDemUck study (n = 235 community-living PlwD) demonstrate, among other things, that PlwD are predominantly married or in a partnership, had mild to moderate cognitive impairment, relatively high functional impairment, one-third receive antidementia medications, over half of the PlwD regularly consult a General Practitioner (GP), and that 58% of their caregivers would describe their quality of life as “good” [6]. The generalizability of these reported prevalences is unclear [7]. However, a comprehensive understanding of the sociodemographic and clinical characteristics of PlwD is vital to manage and improve their current situation [5]. We expanded our analyses to include more clinical and health-related variables (e.g., EQ-5D-5 L, body-mass-index, DEMMI, Timed-up-and-go, F-SozU, RUD, Zarit-Burden).
In many cases, PlwD have a complex and diverse need for healthcare and nursing because they often have several comorbidities, take various medications and need various types of support in their daily life. This complex situation causes unmet healthcare needs. The term “need” is based on the “ability to benefit” concept when a suitable intervention option is available that could address an unmet need [8]. Generally, unmet needs can be assessed by standardized instruments, like the Camberwell Assessment of Needs for the Elderly (CANE) [9], the John Hopkins Dementia Care Needs Assessment (JHDCNA) [10], or specifically developed Intervention Management Systems (IMS) [11]. Previous research has indicated that PlwD frequently experience various unmet healthcare needs, with their number ranging between 0.95 and 8.77 on average, depending on the respective questionnaire used [12–18].
Literature shows that unmet needs of PlwD are affected by a variety of factors [12–14, 17]. Eichler et al. [14] demonstrated that unmet needs were associated with worsening functional status. Black et al. [12] provided details about determinants, indicating that higher numbers of unmet needs among PlwD were significantly associated with lower income, less impairment in activities of daily living and more symptoms of depression. In addition, more unmet needs were significantly associated with lower quality of life [13]. The living situation among PlwD also determines unmet needs. Miranda-Castillo et al. [17] found that PlwD living in community networks with one to six members had significantly more unmet needs than individuals residing in communities with more than seven members. Individuals living alone show higher numbers of unmet needs than PlwD living in a partnership [17].
There is a need to study relationships, associations, and interactions between different variables in PlwD [5]. It is also necessary to conduct a comprehensive needs assessment to develop tailored interventions that address individual needs [14]. To our knowledge, the effects of clinical and sociodemographic parameters on unmet needs have yet to be considered separately to a large extent for women and men. A growing scientific literature documents that sex and gender have a differential impact on the risk, clinical presentation, and progression of dementia, and sex should, therefore, be considered as a factor in studies [19–21].
For example, it was found that neuropsychiatric abnormalities differed between the sexes [20]. A Canadian study also found that women received more supportive care but had higher unmet needs for home care than men [21]. As a result, these gender differences should be considered when developing programs, assessing the needs of care recipients and providing services [21], as these differences can impact health policy [20].
Therefore, this paper aims to describe the sociodemographic and clinical parameters of a baseline sample of community-dwelling PlwD, demonstrate the prevalence and types of unmet needs and identify associations between PlwD characteristics and needs stratified by sex.
METHODS
Study design
InDePendent (Interprofessional Dementia Care: Redistribution of tasks between physicians and qualified nurses in primary care) is a multi-centre, cluster-randomized, controlled trial with an intervention and a waiting control group to examine the efficacy of dementia-specific case and care management. The study protocol is published elsewhere [22]. Study participants were recruited in the primary care setting by GPs and medical specialists, e.g., neurologists and psychiatrists, who are members of one of five physician networks in three federal states in Germany (Mecklenburg-Western Pomerania, Brandenburg, and Hesse). Practitioners were informed about their randomization group after consenting to participate in the study, and they also informed their patients about the course of treatment and thus their study group upon inclusion in the study. Due to the nature of the intervention in this study, it is not possible to blind the study staff (nurses or practitioners) or the participants. The inclusion criteria for PlwD were: community-dwelling, formally diagnosed for dementia or positively screened for dementia (DemTect Score≤8 [23]), and provision of written informed consent. If the person could not provide written consent and had a legal guardian, then the guardian was asked to sign the consent form on his or her behalf. If a caregiver was available, he or she was also asked to provide written informed consent. The participating GPs received an allowance for each PlwD included in the study. The recruitment started in January 2021 and ended in December 2022.
The intervention is based on a collaborative dementia care model previously implemented and evaluated in the DelpHi-MV study [24], adapted for implementation in existing physician networks. Advanced care roles and substitution of medical activities enhanced the InDePendent intervention. This means that dementia-specifically qualified nurses, so-called Dementia Care Managers (DCM), collect all medical, pharmaceutical, psychosocial, social, and care needs using a self-developed computerized IMS at the patient’s home, and take over some of the tasks of the GPs with the aim of meeting or addressing all unmet needs within an intervention period of six months. The InDePendent study (funded by the German Innovationsfonds, ref. no.: 01NVF18034) aims to evaluate whether DCMs and the redistribution of tasks between nurses and physicians could significantly reduce the number of unmet needs of PlwD compared to routine care after six months.
The ethics committees of the University Medical Center Greifswald, the State Medical Council Brandenburg and the State Medical Council of Hesse approved the implementation of the InDePendent study (registration number: BB 144/20; AS 81(bB)/2020; 2020-2081-zvBO).
Study population
From n = 149 participating GPs and specialist practices, n = 471 PlwD and additionally, n = 188 informal caregivers provided their informed consent and participated in the study. Before baseline, n = 54 patients dropped out (11.5%), for example due to lack of interest, moving away or death. Finally, n = 417 PlwD started the baseline assessment (Fig. 1).
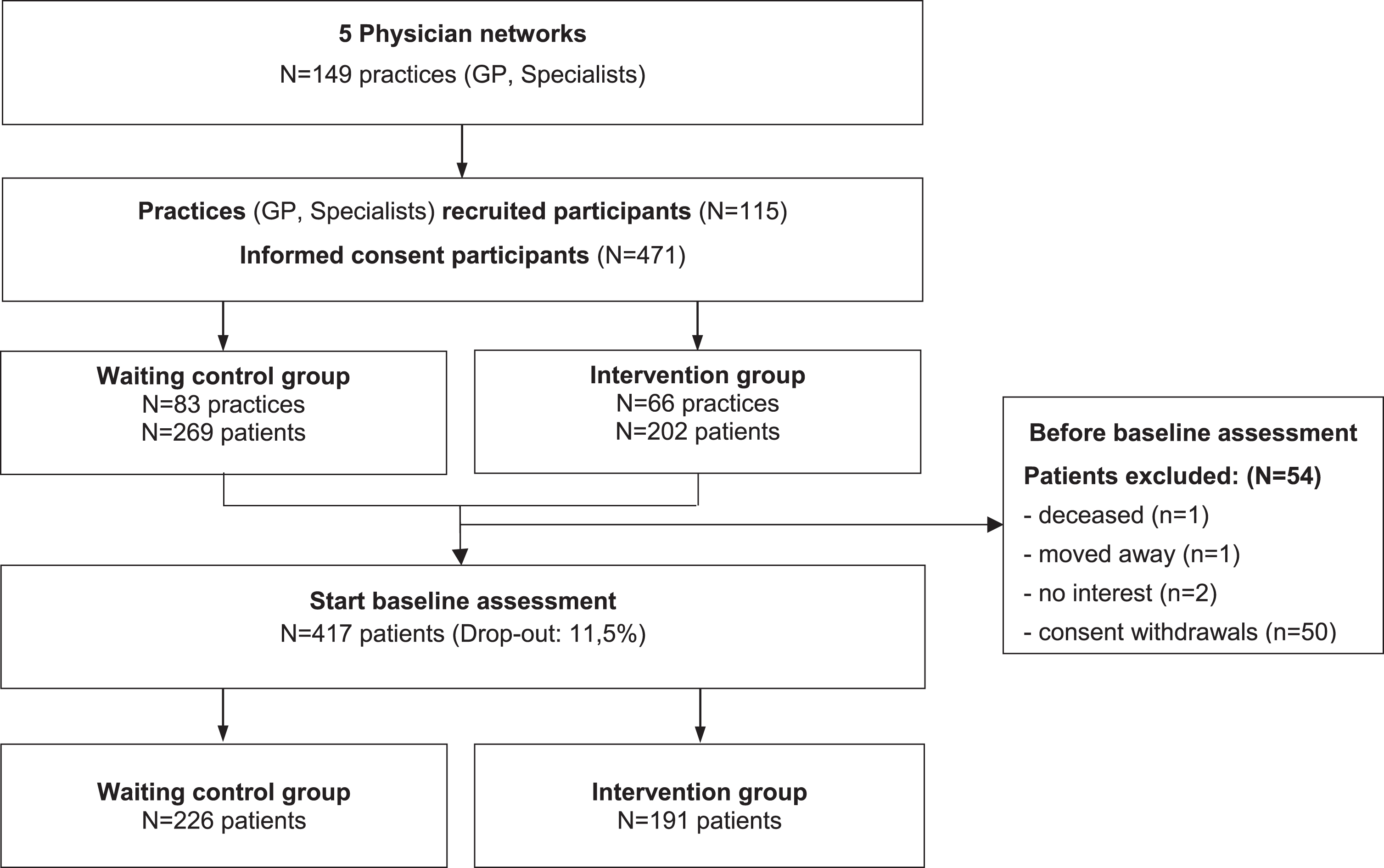
CONSORT Diagram InDePendent study Baseline.
Differences between those who dropped out and those who started the baseline interview were tested using a logistic regression model controlled for age, sex, study group, and physician network membership.
Selection bias was found concerning the study group and physician network membership, as there was a highly significant difference between those who dropped out and those who started the baseline interview. The detailed analysis can be found in Supplementary Tables 1 and 2.
Data assessments
Upon enrolment in the study, all participants (PlwD and their caregivers) received a comprehensive computerized baseline assessment conducted by the DCMs in their homes. All data were collected as part of a personal face-to-face interview, in which the DCM read the questions separately to the PlwD and caregiver, if available [22]. The duration of the interviews varied depending on the condition of the interviewee and whether there was a caregiver who could also be interviewed. On average, the baseline interview could be conducted in 2.2 visits within about one month (mean = 27.8 days, SD = 50.9), and for example, CANE questionnaire lasted approximately 17.4 minutes (SD = 14.3). All instruments recorded the participant’s current condition unless stated otherwise below.
Sociodemographic factors
Sex, age, marital status (single, married, divorced, separated, widowed), self-assessed financial situation (good/not good), presence of children (yes/no), school education (primary education/ lower secondary education/ higher secondary education), living situation (alone/ not alone), and caregiver availability (yes/no) were assessed.
Clinical factors
Quality of life
Health-related quality of life was measured by the EQ-5D-5 L (self-rating instrument), covering five dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression) with five response options that range from 1 = “no problems” to 5 = “extreme problems” [25]. A completely healthy patient would, therefore, have a number combination of 11111. Based on this 5-digit number, a health index can be calculated using a special algorithm (the German value set by Ludwig et al. [26]), anchored between 0 (worst) and 1 (full) [27]. EQ-5D index values are derived from the general population using preference weights that reflect the severity of the corresponding health condition [28]. Such index values can then be used for country-specific economic evaluations of health measures and enable the calculation of quality-adjusted life years [27].
Functional status
Functional status was measured by the Bayer Activities of Daily Living Scale (B-ADL) (answered by caregiver), which scored 1 to 10, with 1 representing the best and 10 the worst functional status [29, 30]. To measure mobility status, the De Morton Mobility Index (DEMMI) was used, which covers the PlwD perspective and ranges from 0 to 100 points, with 100 points representing the best mobility [31]. Mobility was also assessed by administering the Timed “Up and Go” (TUG) test, wherein PlwD perform the task themselves. The TUG test measures the time to stand up from a chair, walk three meters, turn around, and sit down again. Less than 10 seconds represent “unrestricted mobility”, 10 to<20 seconds a “mobility impairment without everyday relevance”, 20 to<30 seconds a “restricted mobility with everyday relevance”, and more than 30 seconds a “pronounced restriction of mobility” [32, 33].
Depression
The Geriatric Depression Scale (GDS) (answered by PlwD) was used to detect depressive symptoms [34]. The score values are: 0–5 points, representing “no depressive symptoms”, 6–10 points = “indication for mild depression”, 11–15 points = “indication for severe depression” [35].
Cognition
Global cognitive performance was assessed by asking the PlwD using the Mini-Mental-Status-Test (MMST) [36], with scores categorized as 30 “no cognitive impairment”, 29–20 “mild cognitive impairment”, 19–10 “moderate cognitive impairment “ and ≤9 “severe cognitive impairment” [37].
Comorbidity and polypharmacy
All ICD-10 diagnoses listed in the treating practitioner’s file and all drugs taken (including over-the-counter medications) according to the medication plan were assessed by the DCM. Based on that data, we calculated the number of diagnoses and medicines taken and identified potentially inappropriate medications, according to the Priscus List [38] 1.0 1
Additional measures of health
We also looked for presence of a long-term care grade. A care grade (“Pflegegrad”) is a German classification for the level of care needed by an individual. It determines the amount of care and support a person receives due to his or her health condition or disabilities. The care grade ranges from 1 to 5, with one indicating some problems and five extreme problems. In Germany, the Medical Service of the Health Insurance Fund (MDK) decides on the classification into a care grade. This assessment is based on an appraisal of individual care needs by specially trained MDK assessors. We also assessed the Body-Mass-Index (BMI) of PlwD based on measurements of body length and weight.
Utilization of care services and informal care
The utilization of care services was measured using the Questionnaire for Health-related Resources in Older People (FIMA) by asking the PlwD [39]. Informal care provision by caregivers was recorded using the Resource Utilisation in Dementia (RUD) instrument, covering caregiver support (from the caregiver’s perspective) in hours per month for i) activities of daily living (ADL) (e.g., personal hygiene, eating, dressing), ii) instrumental ADL (e.g., shopping, meal preparation, housekeeping) and iii) supervision (such as preventing dangerous events) [40].
The following FIMA items have a recall period of three months: Utilization of GP, neurologist/psychiatrist, ambulatory care, physiotherapy, occupational therapy, speech therapy, ambulant nursing service, relatives and the following one a recall period of twelve months: semi-stationary care facility, day clinic, stationary treatment. In the case of RUD, the last 30 days were surveyed.
Social support
The F-SozU (reported by PlwD) is a questionnaire on social support, covering emotional support, practical support, social integration, and social stress with scores ranging from 1 (strongly agree) to 5 (not agree), where higher scores indicate higher social support [41].
The Zarit Burden questionnaire measures the subjective burden of PlwD’s caregivers, ranging from zero to 88 points, with higher scores representing a higher level of subjective caregiver burden [42].
Unmet needs
Unmet needs of PlwD were assessed using the German version of the Camberwell Assessment of Needs for the Elderly (CANE), which evaluates the met and unmet needs from the patients’ and the caregivers’ (proxy) perspectives. The CANE questionnaire includes 25 daily life domains (plus two caregiver needs items) to assess older people’s physical, psychological, social and environmental needs in various domains like household, nutrition, food, activities [9]. The CANE encompasses three inquiries for each designated domain: i) Does a need exist within this domain? ii) Is the need met or unmet? iii) Whom does the individual wish to engage as the person or service provider to address the unmet need? The result of the CANE is a total number of unmet needs of PlwD (minimum 0, maximum 27) [43]. For the regression, a joint CANE variable was created from the perspective of the PlwD and the caregiver (n = 414). To collect the CANE, either the PlwD or, if available, the caregiver was interviewed. In the rare cases (n = 10) where both answered the CANE, the caregiver version was chosen because PlwD typically report significantly fewer (unmet) needs than their caregivers, which could be due to a lack of awareness of difficulties, lack of knowledge about the existence of services, barriers to accessing services and unsatisfactory service provision [18, 44].
Since it is difficult to correctly record unmet needs within the complex home care situations for PlwD, a self-developed, algorithm-based, computerized needs assessment and intervention management system (IMS) was used in addition to the CANE, as it has a larger number of variables from various questionnaires for detecting unmet needs [11, 22]. The conceptualization of the IMS is published elsewhere [11], was tested in the DelpHi-study [11, 45] and further developed for use in care practice the InDePendent study. The results show that the IMS improves the systematic identification of unmet needs and the subsequent recommendation of measures to address these needs [11]. The IMS functions as a rule-based expert decision support system, utilizing a variety of validated questionnaires, tests, and customized queries (e.g., surveys on the housing situation, use of care aids) to align responses from the PlwD’s perspective to the computerized knowledge base. Unfulfilled needs are automatically identified through a standardized survey, employing algorithm-based trigger conditions preset by the system. Confirmation of these needs is carried out automatically by the system and validated by a DCM or additionally pinpointed by them. For each questionnaire, specific trigger conditions have been meticulously developed and defined, signifying distinct unmet needs. These unmet needs are categorized into the following types: a) medical care needs, b) medication care needs, c) nursing care needs, d) psychosocial care needs, and e) social–legal supply needs. In total, there are n = 115 predefined unmet needs.
Statistical analysis
Descriptive statistics were used to demonstrate the sample characteristics, number, and types of unmet needs. We used Fisher’s exact test and Welch’s t-test, depending on the specific variable being examined, to detect any statistically significant differences between the sexes. Due to the Bonferroni correction [46], the significance level was adjusted to<0.001. To identify associations between sociodemographic and clinical factors and unmet needs, we used multiple Poisson regression models with random effects for treating GPs, representing the clusters of PlwD. The number of unmet needs (from IMS and CANE, respectively) were used as dependent variables and sociodemographic and clinical variables as independent variables. All models were stratified by sex. Missing data on covariates were imputed using multiple imputations by chained different imputation sets were created for each variable (GDS, F-Sozu, MMST, BMI, B-ADL). Therefore, a total of 20 data sets were created. Statistical analyses were performed using StataSE 16 (TX, USA: StataCorp. © 2019) and SPSS Statistics 29 (Armonk, NY, USA: IBM Corp. © 2022).
RESULTS
Significant differences between the sexes were found in relation to age, family status, living alone, caregiver sex, and relationship between caregiver and PlwD at a significance level of p < 0.001.
Sociodemographics
The participating PlwD (n = 417) were on average 80.6 (SD = 6.9) years old and 55.9% of the participants were women. Most PlwD (52.0%) were married or widowed (39.3%), and 44.6% had a caregiver participating in the study. More than half of the participants had children (87.5%), most had less than ten years of school education, and 40% lived alone. The caregivers were, on average, 67.9 years old (SD = 12.4), and 66.3% were female. Detailed statistics of the PlwD and caregiver characteristics are shown in Table 1 and Supplementary Table 3.
Sociodemographic and clinical variables of PlwD, separated by sex
MMST, Mini-Mental-Status-Test, range 0–30, higher score indicates better cognitive functioning; B-ADL, Bayer Activities of Daily Living Scale, range 0–10, lower score indicates better performance; GDS, Geriatric Depression Scale, sum score 0–15, score≥5 indicates depression; F-SozU, range 0–5; higher score indicates better social support; ZARIT; range 0–88; higher scores indicates greater caregiver burden, EQ-5D-5 L; range 0-1; higher score indicates better health-related quality of life. RUD: examines 3 domains: ADL, activities of daily living (such as personal hygiene, eating, dressing), 2) instrumental ADL (such as shopping, meal preparation, housekeeping) and 3) supervision (such as preventing dangerous events), data in hours per month. p-values to test for significant differences between men and women.
Clinical characteristics
Half of the PlwD (50.1%) had an MMST score between 20 and 30, which indicates mild cognitive impairment. 39.3% had a moderate, and 10.6% severe cognitive impairment. The participants had, on average, 10.8 diagnoses (SD = 9.3). 66.5% of the PlwD were formally diagnosed with dementia (all others were positively screened for dementia without being formally diagnosed), 31.3% suffered from diabetes, 67.2% from hypertension, 18.7% from cerebrovascular disease and 20.2% from coronary heart disease. The PlwD took, on average, seven medications (SD = 3.6) regularly. At baseline, 31.3% of the participants received antidementia drugs, 19.4% antidepressants and 21.4% antipsychotics. According to the Priscus List, 12.1% of the PlwD received inappropriate medication. These administered medications include, for example, the antidepressant amitriptyline, the urological drug solifenacin or the antipsychotic diazepam.
The average EQ-5D-5 L index score was 0.74. Most PlwD have no mobility restriction relevant to everyday life (35.6%), closely followed by those with severely limited mobility (29.6%). According to the GDS score (3.6, SD = 3.0), most participants (73.0%) had no depression, 18% had mild depression, and 2.6% had severe depression.
Use of care services and informal care
In the three months before data assessment, 91.3% of the PlwD had consulted a GP and 31.8% a neurologist/psychologist. Almost a quarter of the participants visited a physiotherapist (22.4%), 11.0% received ergotherapy and 2.2% speech therapy. 37.8% of the PlwD received ambulant nursing service. Help from family members, friends, acquaintances or neighbours was received by 62.5% of the PlwD.
In the 30 days before data assessment, caregivers spent, on average, 60 hours per month (2 hours per day) supporting PlwD in their daily tasks, such as personal hygiene or eating. 74 hours (2.5 hours per day) were spent supporting PlwDs’ instrumental activities of daily living, such as shopping or housekeeping, and 83 hours (2.8 hours per day) supervising the PlwD.
PlwD perceived solid social support from their environment (mean F-Sozu = 3.9), and the caregivers had, on average, a relatively low subjective burden (mean Zarit Burden = 24.0).
Unmet needs
985 unmet needs among PlwD were detected using the CANE (sum of self-report by PlwD and proxy by caregivers). On average, 2.3 unmet needs (SD = 2.6) were assessed among n = 242 PlwD, and 2.5 unmet needs (SD = 2.8) among n = 184 caregivers. There are no significant differences between the sexes in terms of the number of unmet needs reported. The distribution of self- and proxy-assessed met and unmet needs set by CANE is shown in Figs. 2 and 3, respectively. If we look at the perspective PlwD and caregivers together and examine which three CANE areas result in the most unmet needs, then the areas “memory” and “daily activities” reveal the most unmet needs for both men and women—closely followed by the category “social contacts” for women and “social counselling/legal support” for men. 62,5% of PlwD had at least one unmet need. Referring to the total number of unmet and met needs across all domains calculated for the person level (mean = 7.7 reported by PlwD, mean = 10.7 reported by caregiver), unmet needs accounted for 27.2% from the PlwD perspective and 23.6% from the caregiver perspective of the total.
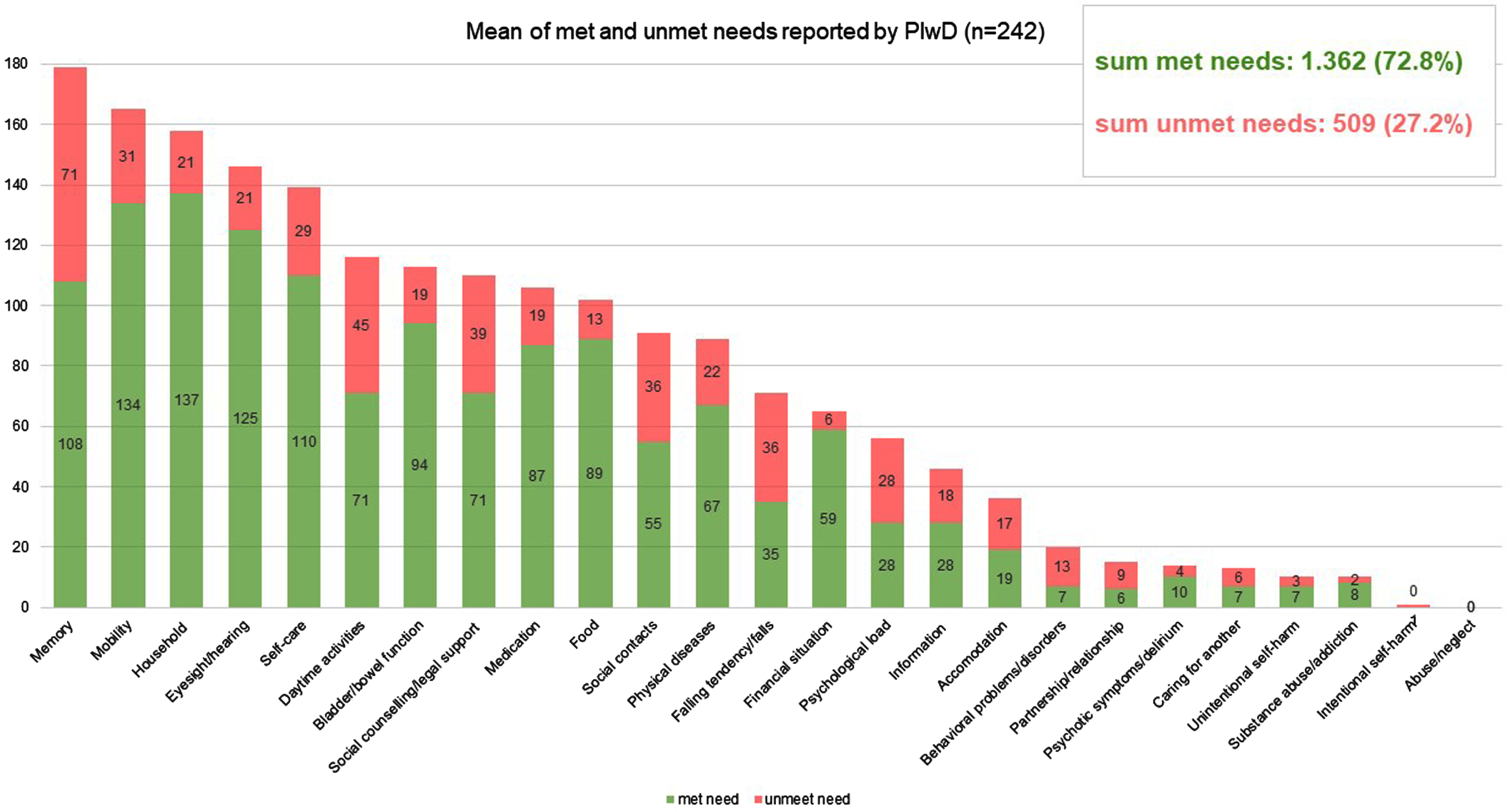
Mean number of met and unmet needs per PlwD reported by PlwD; CANE questionnaire.
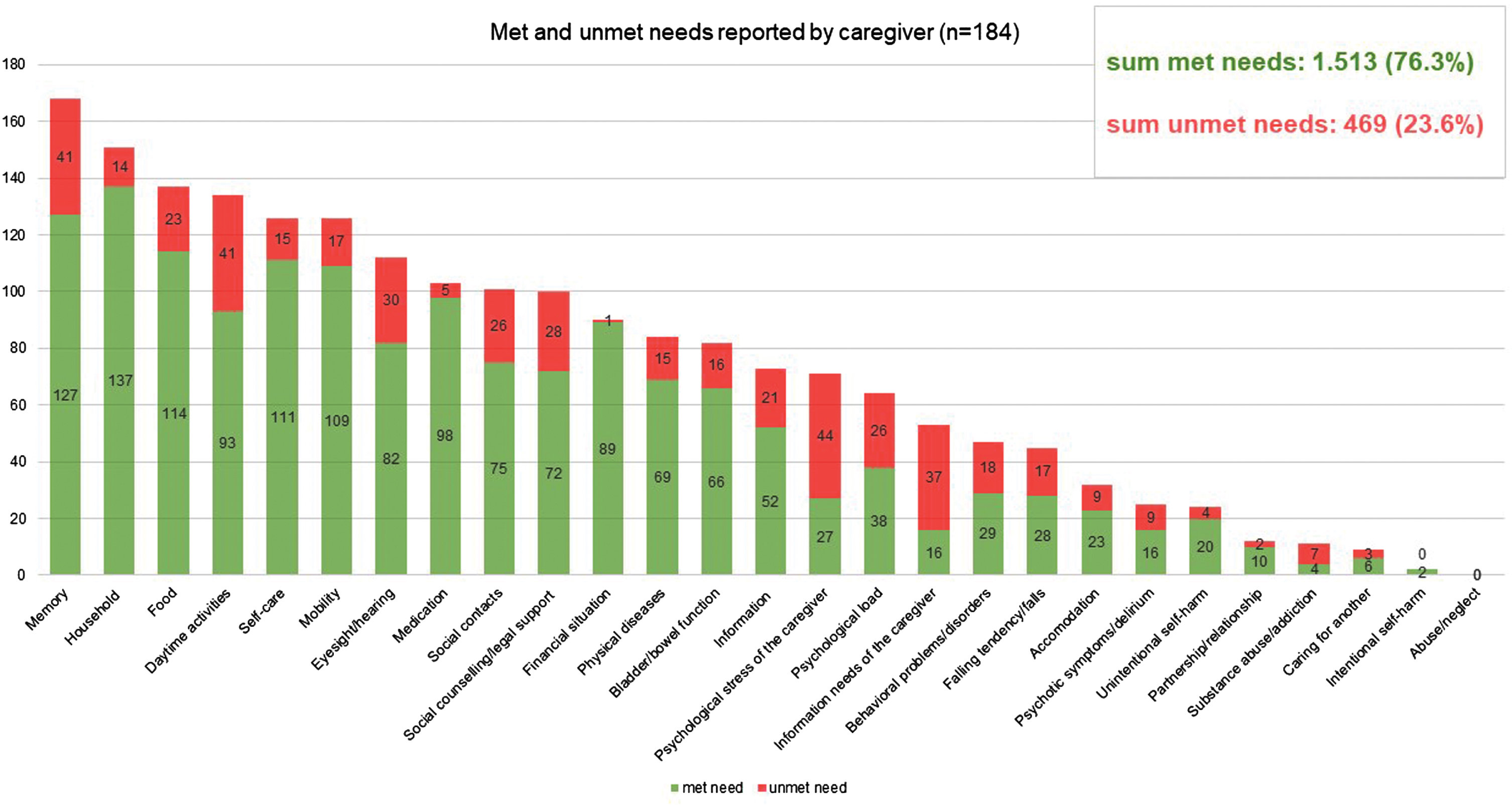
Mean number of met and unmet needs per PlwD reported by caregiver; CANE questionnaire.
The IMS revealed an average of 13.9 unmet needs (SD = 5.0) for PlwD (PlwD perspective).
Characteristics associated with unmet needs
The results of the multivariate regression models are demonstrated in Table 2. Most variables used had low missing values (maximum 4% missing values). Imputations were carried out for the following variables as they had many missing values: BMI (5%), F-SozU (14%), MMST (14%), GDS (18%), and B-ADL (39%).
Multiple regression models to identify determinants for unmet needs CANE and IMS, separately for men and women
MMST, Mini-Mental-Status-Test, range 0–30, higher score indicates better cognitive functioning; B-ADL, Bayer Activities of Daily Living Scale, range 0–10, lower score indicates better performance; GDS, Geriatric Depression Scale, sum score 0–15, score≥5 indicates depression; F-SozU, range 0–5; higher score indicates better social support; ZARIT; range 0–88; higher scores indicates greater caregiver burden, EQ-5D-5 L; range 0-1; higher score indicates better health-related quality of life. RUD, examines 3 domains: ADL, activities of daily living (such as personal hygiene, eating, dressing), 2) instrumental ADL (such as shopping, meal preparation, housekeeping) and 3) supervision (such as preventing dangerous events). p* < 0.05; p** < 0.01; p*** < 0.001 tested for each independent variable with the dependent variable (CANE or IMS), separately by sex. Poisson regression models with random effects for treating General Practitioners, representing the clusters of PlwD. β, regression coefficient; SE, standard error; Model1: n = 206, Pseudo R2 = 0.1703, p < 0.001; Model2: n = 163, Pseudo R2 = 0.0934, p < 0.001; Model3: n = 206, Pseudo R2 = 0.0740, p < 0.001; Model4: n = 165, Pseudo R2 = 0.1005, p < 0.001.
Unmet needs (CANE)
For both sexes, high social support (F-SozU), higher education, and having a care grade were associated with lower unmet needs in CANE. Similarly, a better cognitive status (MMST), a higher BMI, and increased functional limitation (B-ADL) were statistically significantly associated with higher unmet needs in both sexes.
In females living alone (β= 0.27, p < 0.05), the presence of depression (GDS, β= 0.08, p < 0.001) and visiting a neurologist within the last three months (β= 0.42, p < 0.001) were associated with higher unmet needs. In contrast, seeing a GP (β= –0.48, p < 0.005) emerged as a positive determinant among women.
In men, a better health-related quality of life (EQ-5D-5 L, β= –0.81, p < 0.005) and an increasing number of diagnoses (β= –0.04, p < 0.005) indicated fewer unmet needs, while a higher number of medications taken (β= 0.04, p < 0.05) was statistically significantly associated with an increased number of unmet needs.
Unmet needs (IMS)
Regarding the IMS, we also identified a better general health status (EQ-5D-5 L index) to be a positive determinant both in men (β= –0.41, p < 0.001) and women (β= –0.5, p < 0.001). Increased BMI is related to increased unmet needs for both women (β= 0.01, p < 0.01) and men (β= 0.01, p < 0.05).
In women, significant associations were found between the increasing number of diagnoses (β= 0.01, p < 0.01) and higher unmet needs; and a good financial situation (β= –0.11, p < 0.05) and lower unmet needs.
In males, there were associations between better social support (F-SozU, β= –0.11, p < 0.05) and higher education (β= –0.15, p < 0.005) and lower unmet needs.
DISCUSSION
This paper aimed to describe the InDePendent study sample of community-dwelling PlwD, their existing unmet needs and associations with clinical and sociodemographic parameters. The mean age was slightly over 80 years, and more than half of the participants were female, most had children, and were married or widowed. Most of the sample consisted of PlwD with no depression. Participants had an average of 10.8 diagnoses, and took an average of 6.7 medications. Using CANE, an average of 2.4 unmet needs (PlwD and caregiver perspective), and using the IMS (PlwD perspective), an average of 13.9 unmet needs were detected. Regardless of sex, a high BMI, low social support, a low education, not having a care grade, prevalent functional and cognitive impairment, and worse health were associated with more unmet needs. In women, depressive symptoms, increasing number of diagnoses, having visited a neurologist within the last three months, poor financial situation, and living alone were associated with higher unmet needs. In contrast, regular contact with a GP was associated with lower unmet needs. In men, however, unmet needs increased with more medications taken and decreased with more diagnoses.
Clinical characteristics
A large part of the sample consisted of PlwD with mild to moderate dementia (according to the MMST score), which is to be expected in primary care settings and is mainly in line with findings from Thyrian et al., who screened community-dwelling people aged over 70 years for dementia in GP practices [5]. Nevertheless, only two-thirds of study participants had a dementia diagnosis at baseline, potentially indicating an underestimation of dementia diagnoses and likely leading to a gap in healthcare for PlwD. On the other hand, this may also have been caused by the sensitivity and specificity of the MMST and the fact that people with mild cognitive impairment, in particular, may be less likely to be reliably detected by the test [47].
The results demonstrate that PlwD are often affected by multimorbidity and multiple medications, which is confirmed by the high utilization of healthcare services. Most PlwD had consulted a GP, almost one-third a neurologist/psychologist in the three months before the assessment, and nearly one-fifth had been hospitalized for inpatient treatment in the 12 months prior to the assessment, demonstrating a high burden of dementia disease on the medical system.
Unmet needs
Our findings confirm previous research [12–17, 48] and demonstrated a high disease load with a total number of 985 unmet needs in community-dwelling PlwD. PlwD (self-report, n = 242) had on average 2.3 unmet needs (CANE) and informal caregivers (n = 184) assessed on average 2.5 unmet needs (CANE) about their caregiver (in line with other study results [17, 18]). Nevertheless, the results differ from Khanassov et al. [16] and Kerpershoek et al. [13], who reported lower unmet needs among PlwD and Hancock et al. [49], who reported higher unmet needs. These variations in the results could be attributed to disparities in the characteristics of the samples used.
More than half of the participants (62.5%) showed at least one unmet need, which is a smaller proportion compared to what Black et al. [12] demonstrated in community-residing PlwD living in the US (99% had at least one unmet need). One possible explanation for this discrepancy could be related to the recruitment setting in our study through practices engaged in participating networks that likely have improved the communication among healthcare professionals. This could have resulted in more frequent and earlier recognition of unmet needs compared to an “average” GP practice.
In addition, we found unmet needs in almost every domain of the CANE (Figs. 2 and 3). This leads us to the conclusion that current primary care setting has potential to improve interdisciplinary care for PlwD. Eichler et al. [14] also found unmet needs (assessed with an earlier version of the IMS) in all predefined subcategories. Thus, PlwD and their caregivers are relevant target groups for individualized interventions.
Characteristics associated with unmet needs
The study demonstrated that unmet needs among PlwD and their caregivers are mainly predicted by predisposing, enabling and need factors.
Higher
Better
Better
Lower
Better
The
The relationship between an increased
The
The association between female PlwD who reported being in an excellent
Only men show a correlation between the
To our knowledge, this is the first study that provided determinants for unmet needs (according to CANE and IMS, respectively) stratified by patient sex in community-dwelling PlwD in Germany. In general, some determinants differ between patient sex, which leads to the recommendation that interventions in PlwD pay sufficient attention to patient sex to provide gender-sensible strategies in the future. In conclusion, our results provide evidence and quantify the diverse needs (medical, financial, and social) of PlwD living at home and emphasize the need for innovative individualized approaches adressing these needs. The outcomes of our study provide empirical support for challenges in the current healthcare provision for PlwD. Our findings also highlight the urgent need for PlwD and their caregivers to communicate with experts concerning the coordination of dementia care. Future research should focus more on differentiating the individual areas of unmet need to identify areas that would otherwise go unrecognized to develop innovative treatments and personalized interventions.
Limitations
The study sample was recruited within five physician and dementia networks, which are likely characterized by a higher communication standard among participating healthcare professionals compared to routine healthcare. Due to these more effective cooperative structures within the physician networks, advantages in terms of provision of dementia-specific medications and referrals to specialists [6], it is likely that the number of unmet needs identified may be lower compared to PlwD and their caregivers who are treated in separate primary care practices. Thus, the generalizability of the results may be somewhat limited. In addition, all assessments are based on self-reports of PlwD or their caregiver, which could lead to an over- or underestimation concerning specific unmet needs and, therefore, would also limit the external validity of the results.
The significant differences between the drop-outs and the PlwD who started the baseline interview in terms of the physician network cluster and the randomization group can be explained, on the one hand, by the fact that a larger proportion of PlwD who are randomized to the waiting control group and thus learn that they will receive the intervention six months later drop out of the study early. Second, the specific physician network clusters may have influenced the number of early drop-outs, as recruitment behaviour, structures within the network, physician-patient relationships, and motivation within network physicians might differ across these. Due to the nature of the intervention, it was unfeasible to implement blinding among participating physicians. Consequently, we cannot exclude that some participating physicians may have altered their recruitment behaviour upon becoming aware of their assigned group.
Whether met or unmet, care needs indicate the importance of individualized and targeted care services. This is more than just a one-time task. Both the PlwD and their caregiver need to be prospectively monitored, as due to the progressive course of dementia, any need that has been fulfilled may later transform into an unfulfilled need again.
AUTHOR CONTRIBUTIONS
Annelie Scharf (Formal analysis; Writing – original draft); Fabian Kleinke (Formal analysis; Writing – original draft); Bernhard Michalowsky (Conceptualization; Methodology; Writing – review & editing; co-principal investigator); Anika Rädke (Project administration; Writing – review & editing; study coordinator); Stefanie Pfitzner (data monitoring); Franka Mühlichen (Writing – review & editing); Maresa Buchholz (Writing – review & editing); Neeltje van den Berg (Conceptualization; Writing – review & editing; Evaluation); Wolfgang Hoffmann (Conceptualization; Supervision; Writing – review & editing; principal investigator).
Footnotes
ACKNOWLEDGMENTS
We would like to thank all participating patients, their caregivers, and the participating general practitioners and specialists for their most valued collaboration.
FUNDING
The study is funded by the Innovation Fund at the Federal Joint Committee (G-BA Grand No: 01NVF18034). The funders have had no influence on the conceptualization and conduct of the study and will not have any role in the data analysis and publication of the results.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Information about the data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
The Priscus list 1.0 was used before the updated Priscus list 2.0, which contains 133 additional drugs, was released (2023).
According to the “International Statistical Classification of Diseases and Related Health Problems” (ICD-10-Codes). Dementia (F01-F03), Diabetes (E10-E14), High blood pressure (I10-I15), Cerebrovascular diseases (I60-I69), Coronary heart diseases (I20-I25)