
Abstract
Background:
The association between uric acid (UA) and cognitive function still remains controversial. Moreover, the role of inflammation in the above association is also unclear.
Objective:
We aimed to determine the association between UA and cognitive function among non-hyperuricemia adults, and in particular, whether the association was shaped by different inflammation levels.
Methods:
From the China Health and Retirement Longitudinal Study (CHARLS), 7,272 participants aged 45 and above were enrolled in 2011. Cognitive function measurement included orientation and attention, episodic memory, and visuospatial ability. Fasting blood samples were collected to measure levels of UA and high-sensitivity C-reactive protein (hs-CRP). Generalized estimating equation models were used to evaluate the effect of UA on cognitive function in all participants and those at different levels of hs-CRP (hs-CRP <3 mg/L or ≥3 mg/L).
Results:
Among non-hyperuricemia adults (mean age: 58.08, 49.59% males) for a median of 7 years follow-up, participants with higher levels of UA had better cognitive function score compared to those with lower UA levels (β: 0.09, 95% confidence interval [CI]: 0.01–0.17, p = 0.023). And this association was significant under low-grade inflammation levels condition (β:0.10, 95% CI: 0.10–0.19, p = 0.024), but not in high-grade inflammation levels condition. Further, the cognitive function benefit of elevated UA existed only in people with persistent low-grade inflammation levels at a longitudinal perspective (β: 0.14, 95% CI: 0.01–0.27, p = 0.039).
Conclusions:
Elevated UA levels were associated with better cognitive function in non-hyperuricemia population, especially for those at low inflammation levels.
INTRODUCTION
Cognitive impairment, encompassing everything from mild cognitive impairment (MCI) at one end of the spectrum to dementia at the other end, is a disorder characterized by slowly progressing cognitive decline [1]. A recent survey showed that the overall dementia and MCI prevalence were estimated to be 13% and 15.5% in people aged 60 years or older in China [2]. The prevalence of Alzheimer’s disease (AD) and dementia escalated exponentially with increasing age and doubled at 5-year intervals [3, 4]. This condition exerted considerable health, social, and economic costs on individuals, families, and societies [5]. Studies have demonstrated the association between cognitive impairment and mortality [6, 7]. A cohort study of 11,732 Chinese older adults reported that participants with rapid cognitive decline had a 75% higher risk of death and faster cognitive decline was associated with higher mortality [8]. Studies reported that metabolic disorders such as hyperlipidemia and hyperglycemia were associated with worse cognitive function [2, 9]. Identifying modifiable metabolic risk factors would have benefits in preventing cognitive impairment.
Uric acid (UA) is a primary natural antioxidant, which could exert neuroprotective effects through its antioxidant properties [10]. Epidemiological evidence suggested that serum UA was related to cognitive function, but the conclusions seemed to be controversial [11–16]. It was reported that high levels of serum UA were positively associated with cognitive function, especially in people with normal levels of UA [11–13]. However, contrasting findings had merged in other studies [14–16]. It is still unclear why UA has a heterogeneous effect on cognitive function. Besides this, according to previous studies, it is well established that inflammation contributed to the progression of cognitive impairment, while UA and inflammation were closely related [2, 17]. Diverse effects of UA on depression and mortality were observed at different levels of inflammation [18, 19], which supported that the function of UA varied in different inflammation levels. Nevertheless, few studies explored the association between UA and cognitive function taking the effect of inflammation into account. Interest will be aroused to explore whether the association between UA and cognitive function was shaped by inflammation levels.
Therefore, the present study aimed to explore the effect of UA on cognitive function among non-hyperuricemia adults, and in particular, whether this relationship was affected by different levels of inflammation.
METHODS
Study population
The present study was based on the China Health and Retirement Longitudinal Study (CHARLS), which was described in detail elsewhere [20]. In brief, CHARLS was a nationally representative longitudinal survey of the Chinese population from 2011 to 2015, using a multi-stage random sampling method to investigate individuals from 28 provinces in China. Demographic characteristics, health behavior, physical function and disease history were obtained from questionnaire among 17,705 participants in 2011. The inclusion criteria were: 1) age ≥45 years old; and 2) providing serum UA measurement; and 3) providing cognitive function assessment results. The exclusion criteria were: 1) with hyperuricemia; and 2) without follow-up. Participants younger than 45 years old (n = 474), or without baseline information (n = 5,073), or without UA measurement (n = 3,708), or with hyperuricemia (UA ≥420μmol/L (7.05 mg/L) for older adults, n = 244), or loss to follow up (n = 934) were excluded. Eventually, as shown in Fig. 1, 7,272 participants were included. The CHARLS was approved by the Institutional Review Board of Peking University (IRB00001052-11015). All participants signed an informed consent before participating in the survey.
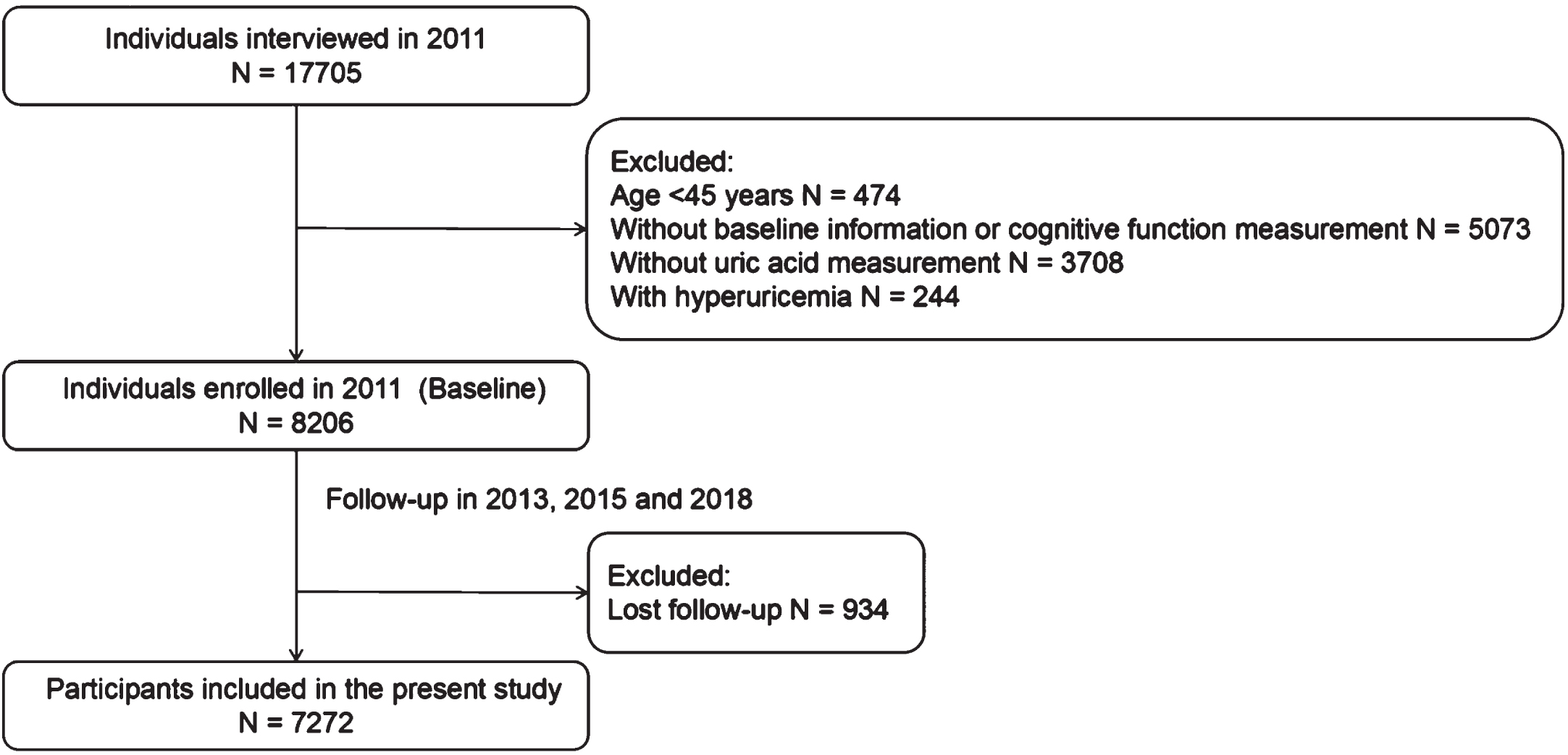
Flow chart of the study.
Measurement
Cognitive function. Cognitive function was assessed by face-to-face interviews. Cognitive function assessment included three dimensions: orientation and attention, episodic memory, and visuospatial ability [21]. Telephone Interview of Cognitive Status (TICS) was used to measure orientation and attention. The TICS includes 9 mental-state questions, including completing the task of subtracting 7 from 100 consecutively (up to 5 times), and awareness of the date of the visit (day, month, year) and day of the week. TICS score ranged from 0 to 9, and 1 point for each correct answer. Episodic memory was assessed by immediate and delayed word record. Participants remembered as many words as possible from a list of 10 words given by the interviewer immediately (immediate remember of words) and after 5 min (delayed remember). Episodic memory score ranged from 0 to 20 and 1 point for each correct answer. Figure drawing test was used to assess visuospatial ability. Participants was showed a photo and was required to draw a similar picture. Visuospatial ability score ranged from 0 to 1 and 1 point for those who could copy same picture. Total cognitive score ranged from 0 to 30 and higher score mean better cognitive function.
Blood biomarkers. Fasting blood was collected from each participant and detected at local Centers for Disease Control and Youanmen Center for Clinical Laboratory of Capital Medical University. UA Plus was used to detect UA. Immunoturbidimetric assay was used to detect hs-CRP. According to the upper limit of normal value (3 mg/L) [20], high inflammation risk group and low inflammation risk group were discriminated. Rate-blanked and compensated Jaffe creatinine was used to detect creatinine and Particle-enhanced turbidimetric assay was used to detect Cystatin C.
Covariate. Age (year), gender (male/female), current smoker (yes/no), alcohol consumption (never/>1 time per month/<1 time per month), education level (primary school and below/junior high school/high school and above), marital status (separated or divorced/married but temporarily separated/married and cohabiting), residence (urban/rural) were obtained by trained interviewers using standard questionnaires. Height and weight were measured while wearing light clothing and no shoes to calculate body mass index (BMI). Physical activity was defined if participants have 30 min moderate activity at least fifth times per week or 20 min vigorous activity at least third times per week [22]. Hypertension was defined if participants had hypertension history, or already received anti-hypertensive treatment, or the mean systolic blood pressure ≥140 mmHg or the mean average diastolic blood pressure ≥90 mmHg. Diabetes mellitus was defined if participants had a history of diabetes mellitus, or already received treatment for diabetes mellitus, or fasting blood glucose ≥7.0 mmol/L and/or glycated hemoglobin A1c ≥7.0 mmol/L as defined by American Diabetes Association criteria [23]. Stroke was defined by medical diagnosis. Renal function was estimated by the estimated glomerular filtration rate (eGFR) calculated using the CKD Epidemiology Collaboration (CKD-EPI) equation [24]. CKD was diagnosed based on an eGFR of < 60 mL·min–1·1.73 m–2.
Data analysis
The analysis of the study was carried out in four steps. First, continuous variables were presented as mean (standard deviation) or median (interquartile range), and categorical variables were presented as frequency (percentage). Second, since cognitive scores were repeated measurement data, generalized estimating equation (GEE) model was used to detect the association between UA levels and cognitive function. And the relationship between UA levels and cognitive function was further explored according to the levels of different inflammatory markers (hs-CRP <3 mg/L or ≥3 mg/L). Third, considering that inflammation levels were time-variant, based on the levels of inflammatory markers measured in 2011 and 2015, the population was divided into those with persistently low levels of inflammation and those with randomly elevated inflammation (in 2011 or in 2015). The relationship between average UA (in 2011 and 2015) and cognitive function at different dynamic inflammation status (persistent low level/random high level) was also analyzed based on GEE model. Subgroup analysis was employed to examine the effect of UA on cognitive function in the various subgroups, including age (< /≥65 years), sex (male/female), CKD (no/yes), hypertension (no/yes) and diabetes (no/yes). Finally, a series of sensitivity analyzes were used to further support our conclusions. Including: 1) Using the UA levels in 2011 to replace average UA levels in 2011 and 2015; 2) Using different inflammation indicators, such as white blood cells (WBC) to replace hs-CRP; 3) Using different threshold values of hs-CRP level (hs-CRP <5 mg/L or ≥5 mg/L); 4) Using different diagnostic criteria of hyperuricemia as ≥420μmol/L (7.05 mg/L) in men and postmenopausal women, and ≥360μmol/L (6.05 mg/L) in non-menopausal women.
Baseline characteristics of the study population
BMI, body mass index; WBC, white blood cell; hs-CRP, hypersensitive-C reactive protein; Cys C, Cystatin C; UA, uric acid. *p < 0.05.
The missing data in the study population were < 2%, and the method of the last observation carried forwards or the means and medians were used to interpolate the missing data. Stata 15.0 and R (version 4.2.2) were used for data analysis.
RESULTS
Baseline characteristics
The baseline information about 7,272 participants is shown in Table 1. The mean (standard deviation) age was 58.08 (8.53) years old and 49.59% of which were men. The mean (standard deviation) of UA and median (interquartile range) of hs-CRP were 4.38±1.7 mg/dL and 1.01 (0.54–2.07) mg/L, respectively. Adults with high levels of hs-CRP were more likely to be older, men, less physical activity, more BMI, and urban resident. Alcohol consumption and smoking behavior, hypertension, diabetes mellitus and stroke were more prevalent among adults of high levels of hs-CRP.
Association between UA and cognitive function
Table 2 presents the association of UA with cognitive function. After a median of 7 years follow-up, in univariate analysis, participants with 1 mg/dL increase in UA had 0.13 (95% CI: 0.04–0.21) increase in cognitive score (p = 0.003). After multivariable adjustment for age, sex, BMI, education, marriage status, smoking, alcohol consumption, physical activity, hypertension, diabetes mellitus and stroke, for every 1 mg/dL increase in UA, the cognitive score increased by 0.09 (95% CI: 0.01–0.17, p = 0.023). Similar results were found when dividing UA into quartiles. In the full-adjusted model, compared with those in the lowest quartile (Q1), patients in the highest quartile (Q4) of UA had 0.26 (95% CI: 0.02–0.49, p for trend = 0.022) increased cognitive score.
β-coefficients for the associations between UA and cognitive function
UA, uric acid. Model 1: unadjusted; Model 2: adjusted for age, sex, and BMI; Model 3: adjusted for age, sex, BMI, education, marriage status, smoking, alcohol consumption, physical activity; Model 4: adjusted for age, sex, BMI, education, marriage status, smoking, alcohol consumption, physical activity, hypertension, diabetes mellitus and stroke. *p < 0.05.
Association between UA and cognitive function at different levels of inflammation
In order to examine whether the inflammation status shapes the association between UA and cognitive function, the participants were further divided into low inflammation level group (hs-CRP <3 mg/L) and high inflammation level group (hs-CRP ≥3 mg/L) according to baseline hs-CRP levels. We found that adults with low baseline inflammation levels had higher cognitive scores than those with high baseline inflammation levels at each follow-up (Fig. 2a). As shown in Table 3, the protective effect of UA on cognitive function was found in low levels of inflammation group, not in high levels of inflammation group. After full adjustment for the factors included in model 4, for every 1 mg/dL increase in UA, cognitive score increased by 0.10 (95% CI: 0.10–0.19, p = 0.024). The results of subgroup analysis also supported our findings (Supplementary Figure 1).
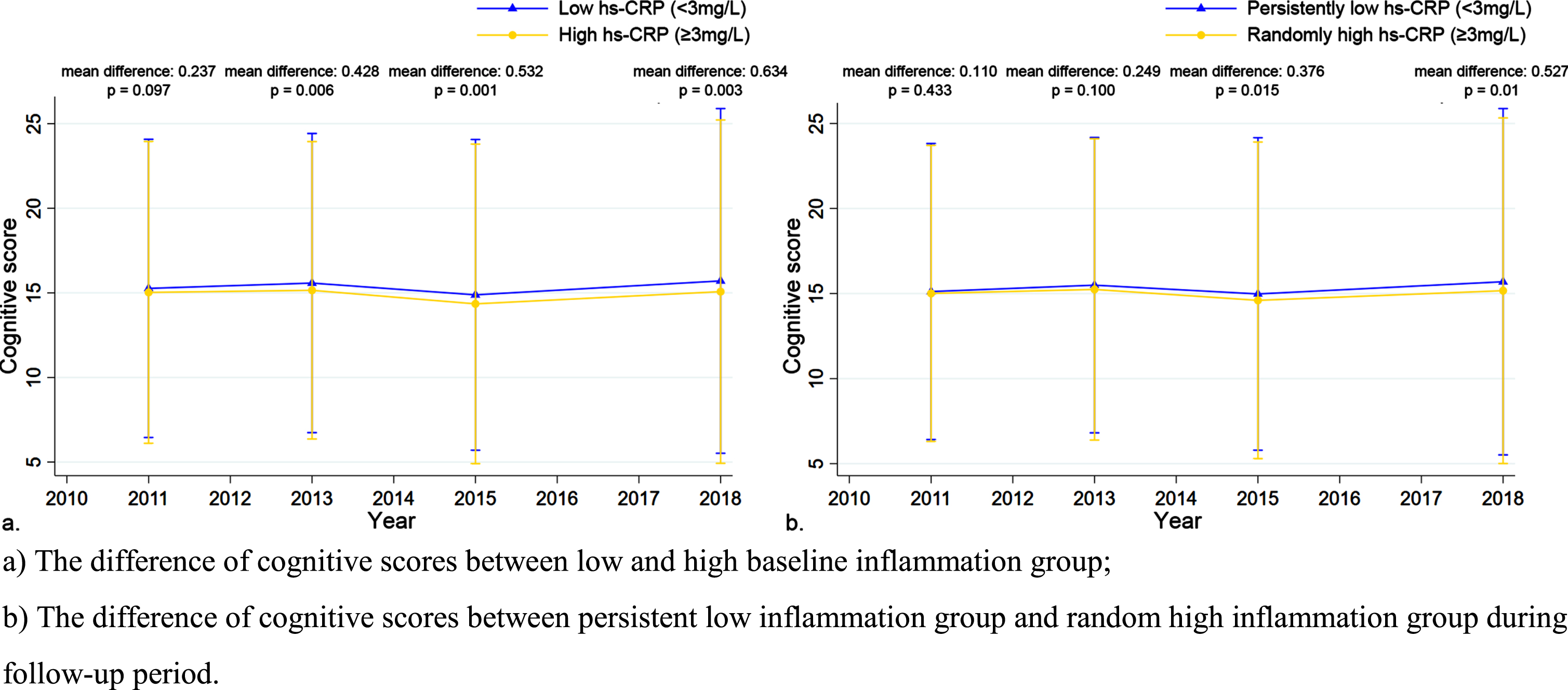
The difference of cognitive scores of different groups at each follow-up.
Additionally, we also evaluated the effect of UA on cognitive function in those with persistent low levels of inflammation and with random high levels of inflammation. Compared to those with random high levels of inflammation, adults with persistent low inflammation levels had higher cognitive scores (Fig. 2b). As shown in Table 4, cognitive function was benefit from increased average UA levels (β: 0.14, 95% CI: 0.01–0.27, p = 0.039 in model 4) in those with persistent low levels of hs-CRP, while there was no significant association among those with random high levels of hs-CRP.
β-coefficients for the associations between UA and cognitive function in different baseline inflammatory state
UA, uric acid; hs-CRP, hypersensitive-C reactive protein. Model 1: unadjusted; Model 2: adjusted for age, sex, and BMI; Model 3: adjusted for age, sex, BMI, education, marriage status, smoking, alcohol consumption, physical activity; Model 4: adjusted for age, sex, BMI, education, marriage status, smoking, alcohol consumption, physical activity, hypertension, diabetes mellitus, and stroke. *p < 0.05.
β-coefficients for the associations between average UA and cognitive function in different inflammatory status during the follow-up period
UA, uric acid; hs-CRP, hypersensitive-C reactive protein. Model 1: unadjusted; Model 2: adjusted for age, sex, and BMI; Model 3: adjusted for age, sex, BMI, education, marriage status, smoking, alcohol consumption, physical activity; Model 4: adjusted for age, sex, BMI, education, marriage status, smoking, alcohol consumption, physical activity, hypertension, diabetes mellitus, and stroke. *p < 0.05.
Sensitivity analysis
To verify the protective effect of UA on cognitive function at low levels of inflammation, we adjusted the hs-CRP threshold to 5 mg/L (Supplementary Table 1), substituted the WBC level as the inflammation marker (Supplementary Table 2), replaced the baseline UA levels with the average of the UA values from 2011 to 2015 (Supplementary Table 3) and adopted different diagnostic criteria of hyperuricemia (Supplementary Tables 4–6). Interestingly, the results were consistently observed with our main findings.
DISCUSSION
The present study revealed that the positive relationship between UA and cognitive function among the non-hyperuricemia people, and inflammation status shaped the association. Among the people with low inflammation levels, those with higher UA levels had better cognitive function while this association between UA and cognitive function disappeared in people with high inflammation levels. Furthermore, the cognitive function benefit of elevated UA was only observed with persistently low levels of inflammation at longitudinal perspective.
In recent decades, despite a large number of epidemiological studies have reported that serum UA was related with cognitive function, the conclusions still remained inconsistent [25–29]. Previously studies have demonstrated a protective role of UA against the progression of cognitive impairment [25, 26]. One study observed that the composite z-score, representing holistic cognitive capacity, was improved by 0.29 (95% CI: 0.06–0.52) in the highest UA quartile group (392.6–701.9μmol/L) compared with the lowest UA quartile group (178.4–279.5μmol/L) (p < 0.05) [27]. Similarly, a prospective cohort study of 7,828 non-hyperuricemia participants reported that participants with high-normal UA levels were associated with better cognitive performance [28]. In contrast, one study reported that people with hyperuricemia had predominantly evident worsen cognitive function compared with normouricemic persons [29]. Besides, another study demonstrated that higher UA baseline levels were associated with faster cognitive decline over-time in a visual memory/visuo-construction ability test [30]. One possible explanation for the controversial results in previous studies was that the inclusion of participants with hyperuricemia might influence the association between UA and cognitive function. Moreover, cardiovascular metabolic disorder caused by hyperuricemia might increase the long-term risk of cognitive decline [31, 32]. To address this problem, our study was performed among non-hyperuricemia participants and found that higher UA level was associated with better cognitive function after 4 years of follow up. In addition, we included a large sample size in China and more covariates including physical activity, hypertension, diabetes mellitus and stroke history to enriched further understanding of the effect of UA on cognitive function.
The effect of UA on the progression of diseases at different inflammation levels came into focus currently [18, 33]. One study showed that inflammation influenced the association between UA and the progression of depression. In participants without low-grade inflammation, higher UA levels were associated with deteriorated depressive symptom [18]. Another report demonstrated that increased hs-CRP may amplify the effect of increased UA on albuminuria in type 2 diabetic patients [33]. Besides, Wang et al. found that low grade system inflammation induced by obesity might attenuate the significant association between lower serum UA levels and higher risk of MCI in non-obese patients [34]. Taken together, these studies exhibited different effect of inflammation on the association between UA and diseases. Therefore, we explored the effect of UA levels on cognitive function at different inflammation levels among non-hyperuricemia. Interestingly, we found that higher UA level was significantly associated with better cognitive function at low inflammation level (hs-CRP <3 mg/L). Furthermore, elevated UA also resulted in cognitive function only at persistently low inflammation levels. As far as we know, our study firstly explored the influence of different levels of inflammation on the relationship between UA and cognitive function, indicating the need of special attention to non-hyperuricemia individuals with high inflammation levels.
The evidence regarding the mechanism of UA on cognitive function is still unclear. UA possesses both antioxidant and pro-oxidant properties, while the reason behind the functional transition is complicated. Study has indicated that central nervous system is one of the major sites where UA plays a role of antioxidant [35]. The potential cause of the neuroprotective action may be that UA is an efficient scavenger for reactive oxygen species which could suppress oxyradical accumulation, stabilize calcium homeostasis, and preserve mitochondrial function [36]. Furthermore, UA could also scavenge peroxynitrite, nitric oxide, and hydroxyl radicals, thereby preventing protein nitration and lipid peroxidation and enhancing longevity and endurance and protecting the brain [37]. However, UA can also be pro-oxidative under certain conditions, such as when other antioxidants are at low level during active inflammatory response [38, 39]. Besides, high inflammation status itself may also impaired the effect of UA on oxidative balance, which is conducive to promoting oxidation. Specifically, a study reported that patients with both high UA level and high hs-CRP had significantly higher mortality rate than those with hs-CRP only [19]. In addition, as observed in present study, people with high levels of inflammation were accompanied by higher prevalence of cardiovascular risk factors (overweight, smoking, diabetes, and hypertension), which could suppress the protective effect of UA on cognitive function [40]. Overall, our study provided evidence that inflammation level shaped the role of UA in cognitive function. However, more research is needed to confirm and explore the findings.
Limitation
There were still some limitations in the present study. First, due to the observational research design, we cannot exclude the effect of residual confounders on the results. Nevertheless, we adjusted for a wide range of covariates for the studied association and the results were still significant. Second, this study was conducted among the middle-aged and older adults. Therefore, whether the conclusions applied to other age groups needs to be further explored. Third, dietary intake was not investigated in this study due to lack of relevant data in the CHARLS, although plasma UA levels are a biomarker reflecting nutrition intake, particularly the consumption of purine-rich foods. Nevertheless, our study also provides some insight into the importance of adequate purine intake for maintaining cognitive health.
Conclusion
In sum, the present findings supported the notion that significant association between higher UA levels was associated with better cognitive function in non-hyperuricemia people with low inflammation levels. This suggests that the inflammation level should also be taken into account when considering the impact of UA on the cognitive function. Keeping a high level of UA within normal range as well as low inflammation levels is effective to maintain cognitive health, especially for the middle-aged and the elderly.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This study was supported by the National Key Research and Development Program of China (No. 2016YFC1301202), the Science and Technology Program of Tibet Grant (No. XZ202201ZY0051 G), Guangzhou Municipal Science and Technology Project (Basic and Applied Basic Research), China (NO. 202201010892), Guangdong Provincial Clinical Research Center for Cardiovascular disease (No. 2020B1111170011), and the Medical Scientific Research Foundation of Guangdong Province, China (No. A2021025).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.