
Abstract
Background:
Obesity significantly increases Alzheimer’s disease (AD) and dementia risk. Understanding the link between a high body mass index (BMI) and these conditions is crucial for effective management and prevention.
Objective:
We aimed to estimate the burden of AD and other dementias attributed to high BMI from 1990 to 2019 based on sex, age, and socio-demographic indicators (SDI) at global, regional, and national levels.
Methods:
We collected data on deaths, disability-adjusted life years (DALYs), age-standardized mortality rates (ASMR), and age-standardized DALY rates (ASDR) from the 2019 Global Burden of Disease study for AD and dementia attributed to high BMI. We explored the correlation between SDI levels and ASDR.
Results:
In 2019, there were 198,476.2 deaths (95% UI: 32,695.4–593,366.4) and 3,159,912.4 DALYs (848,330.5–8,042,531) attributed to high BMI. Numbers of deaths, DALYs, ASMR, and ASDR increased since 1990. Females had higher deaths, ASMR, and ASDR than males. Mortality and DALYs rates increased with age. ASMR and ASDR increased across five SDI levels, with the highest rise in Low-middle SDI. High-income North America had the most deaths [30,993.9 (5,101.7–89,912.9)], while North Africa and the Middle East had the highest ASMR [4.61 (0.79–13.64)] and ASDR [72.56 (20.98–181.16)] in 2019.
Conclusions:
The burden of AD and other dementias attributed to high BMI increased since 1990 globally and is still heaviest in developed regions. Females accounted predominantly for the burden than males. Timely measures are needed to against high BMI.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) and other dementias are now significant and seriously endangering worldwide public health [1]. AD is primarily characterized by comprehensive dementia, including cognitive problems and memory deficits, behavior changes and mental disorder, interfering with the ability to perform daily activities among older adults [2]. Presently, the worldwide prevalence of dementia exceeds 55 million individuals, with a majority of over 60% residing in countries with low-to-middle income [3]. Annually, nearly 10 million fresh cases arise [4]. In 2016, dementia was responsible for 2.4 million deaths worldwide [5, 6]. There is a 10% incidence of dementia by age 85 [7] and an approximate 30% prevalence [8]. On a global scale, a 117% increase in dementia cases has been reported between the years 1990 to 2016. This growth can primarily be attributed to the phenomenon of population aging [9]. As per the statistics presented by the Global Burden of Disease (GBD) 2019 Dementia Forecasting Collaborators, the projected number of individuals with dementia is expected to rise to 83.2 million in 2030, 116.0 million in 2040, and 152.8 million in 2050, across the world [10]. Societies and families are facing serious economic and disease burdens as a result of this growing public health problem.
Global health challenges linked to high body mass index (BMI) continue to be a major concern. Studies have demonstrated that high BMI is an important risk factor for many metabolic [11] and cardiovascular [12] conditions, and these conditions have been associated with reduced survival. The longer the duration of obesity, the higher the risk of developing other chronic diseases [13] and higher mortality rate [14]. Research suggests that the annual burden of disease imposed by high BMI can be quantified as an estimated 216,000 deaths [15] and $113.9 billion in direct healthcare costs in the United States (US) alone [16]. It contributes significantly to the burden of diseases worldwide, such as diabetes, kidney diseases, cardiovascular disease, neoplasms [17], and AD [18, 19]. According to the Lancet Commission’s recent study, there are a number of risk factors associated with dementia, including obesity, diabetes, hypertension, physical inactivity, and low socialization frequency [20]. Recently, a meta-analysis showed that midlife underweight, obesity and late-life underweight conferred 1.39-, 1.31- and 1.64-fold excess risk for cognitive impairment and dementia [21], while late-life overweight and obesity conferred 21% and 25% reduced risk [22]. Obesity is associated with inflammation [23], oxidative stress [24], and mitochondrial dysfunction [25], which in turn affect neural development and lead to AD. In GBD 2019, BMI was added to the risk factors for AD and other dementia [26]. However, no comprehensive data is available to assess the global burden of AD and other dementias burden attributed to high BMI. Therefore, an updated report based on the latest data for AD and other dementias attributed to high BMI in terms of deaths and DALYs is needed.
It has been demonstrated that managing controllable risk factors for dementia can prevent or delay many dementia cases, despite the absence of effective measures to cure dementia. In order to develop prevention and intervention strategies, we provided detailed and updated information about AD and other dementias burden attributed to high BMI in global, regional, and national levels between 1990 and 2019. This study was based on the GBD database published by the Institute for Health Metrics and Evaluation to analyze the global burden of and its trends.
MATERIALS AND METHODS
Data sources
The GBD study is currently the sole research effort that assesses the burden of diseases caused by a wide range of modifiable risk factors across all countries and age groups worldwide, for both genders, and over an extended period [27]. The investigation adhered to the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) [28]. The number of deaths and disability-adjusted life years (DALYs), age-standardized DALYs rates (ASDR), and age-standardized mortality rates (ASMR) of AD and other dementias attributed to high BMI from 1990 to 2019. The specific data analyzed in the current study were obtained from the most recently updated online Global Health Data Exchange (GHDx) Query Tool (http://ghdx.healthdata.org/gbd-results-tool) on 10 February 2023. Information, including sex and age, was also acquired to estimate the burden of AD. The DALYs measure the combined impact of premature death and disability by adding the years of life lost to early death with years of life lived with disability. Essentially, one DALY equates to the loss of one year of healthy life [29].
Definitions
Dementia is a chronic and progressive neurological disorder characterized by memory impairment and other neurological dysfunctions. Diagnostic and Statistical Manual of Mental Disorders III, IV, or V, or International Classification of Diseases (ICD) case definitions were used as the reference. The relevant ICD-10 codes for dementia include F00, F01, F02, F03, G30, and G31, while the ICD-9 codes are 290, 291.2, 291.8, 294, and 331. Adults (age 20+) with a BMI of more than 25 kg/m2 were considered to have a high BMI [17]; this was determined using cutoff points from the International Obesity Task Force guidelines for children (age <20) [17, 30]. According to the socio-demographic indicators (SDI), countries and territories fall into five categories: high, high-middle, middle, low-middle, and low [31]. The SDI is a composite measure of a country’s development based on its geometric average of total fertility, per capita income, and mean years of education, ranging from 0 to 1, where the lowest level of development was 0 and the highest level was 1 [32]. The SDI values for all estimated locations in the GBD 2019 study, spanning from 1950 to 2019, were downloaded from this website: https://ghdx.healthdata.org/record/ihme-data/gbd-2019-socio-demographic-index-sdi-1950-2019.
Estimation methods
For GBD 2019, the fatal modelling process was redesigned to avoid the need for using estimates only from the highest dementia mortality locations. This was accomplished with an attributable risk model based on a systematic review of cohort studies and relative risk data, and end-stage disease proportions from linked hospital and death records. Relative risk models were employed using methods such as meta-regression, Bayesian, regularization, and trimming, and population attributable fractions (PAFs) were computed for each condition using the subsequent equation, with exposure being defined as the prevalence of the corresponding condition:
Finally, the attributable burden was computed by multiplying the PAF with the total burden [30].
Statistical analysis
Death, DALYs, and their ASMR and ASDR were the main indices used to evaluate the AD and other dementias burden attributed to high BMI. All estimates were reported with a 95% uncertainty interval (UI). To visualize the geographic variation regarding AD and other dementias burden attributed to high BMI in the number of deaths, ASMR, and ASDR in 2019, we generated maps of AD and other dementias burden attributed to high BMI. Percentage changes in AD and other dementias burden attributed to high BMI deaths number, ASMR and ASDR from 1990 to 2019 were defined as:
We assessed the relationship between the burden of AD and other dementias burden attributed to high BMI and SDI based on location and year. We used R statistical software (version 4.1.2) to analyze and visualize the data.
RESULTS
Global burden of Alzheimer’s disease and other dementias attributed to high body mass index
In 1990, there were 54,644.4 (95% UI: 8,275.9–170,846.5) deaths cases of AD and other dementias attributed to high BMI; the ASMR was 2.22 (0.33–7.13) per 100,000 population, contributing to 944,844.5 (232,042.7–247,1591.4) DALYs and the ASDR per 100,000 population was 32.37 (7.71–85.18). In 2019, there were 198,476.2 (32,695.4–593,366.4) AD-related deaths attributed to high BMI; the ASMR was 2.81 (0.46–8.42) per 100,000 population, contributing to 3,159,912.4 (848,330.5–8,042,531) DALYs and the ASDR per 100,000 population was 42.22 (11.24–107.37). In the year 2019, when compared to 1990, there was an increase of 263.2% in the number of deaths, 234.40% in the number of DALYs, 26.6% in ASMR, and 30.40% in ASDR related to dementia (Tables 1 and 2).
The death number and DALY number of AD and other dementias attributed to high BMI exhibited a rapidly upward trend in females and both sexes from 1990 to 2019. The ASMR and ASDR of AD and other dementias attributed to high BMI maintained a stable upward trend from 1990 to 2019 in both sexes, males, and females. The death number, DALY number, ASMR, and ASDR of AD and other dementias attributed to high BMI was higher in females than males (Fig. 1).
Regional and national burden of Alzheimer’s disease and other dementias attributed to high BMI
Among 21 GBD regions based on geography, Western Europe [41,430.2 (6,953.4–123,076.7)] had the highest number of deaths, followed by High-income North America [30,993.9 (5,101.7–89,912.9)], and East Asia [24,798 (3,410.6–81,858.1)], while Oceania [61.7 (8.7–194.7)] had the lowest in 2019. Likewise, North Africa and Middle East [4.61 (0.79–13.64)] and Central Europe [4.59 (0.77–13.7)] were the top 2 regions for the highest ASMR per 100,000 population in 2019, while South Asia had the lowest ASMR [1.26 (0.2–4.15)]. The percentage change in death number of AD and other dementias attributed to high BMI from 1990 to 2019, 21 regions have a different degree of increase. South Asia (902.5%), Tropical Latin America (590.9%), Southeast Asia (586.4%), East Asia (566.4%), and High-income Asia Pacific (548.9%) are the top 5 regions more than a five-fold increased regions, while the smallest increase in Central Asia (62.9%). Southeast Asia (152.3%) had the highest increased in percentage change of ASMR, while Oceania (12.7%) had the lowest (Table 1).
Death number and age-standardized mortality rates of Alzheimer’s disease and other dementias attributed to high body mass index by sex, SDI and GBD region in 1990 and 2019
SDI, socio-demographic indicators; GBD, Global Burden of Disease; No., Number; UI, uncertainty interval.
DALYs number and age-standardized DALYs rates of Alzheimer’s disease and other dementias attributed to high body mass index by sex, SDI and GBD region in 1990 and 2019
SDI, socio-demographic indicators; GBD, Global Burden of Disease; DALYs, disability-adjusted life years; No., Number; UI, uncertainty interval.
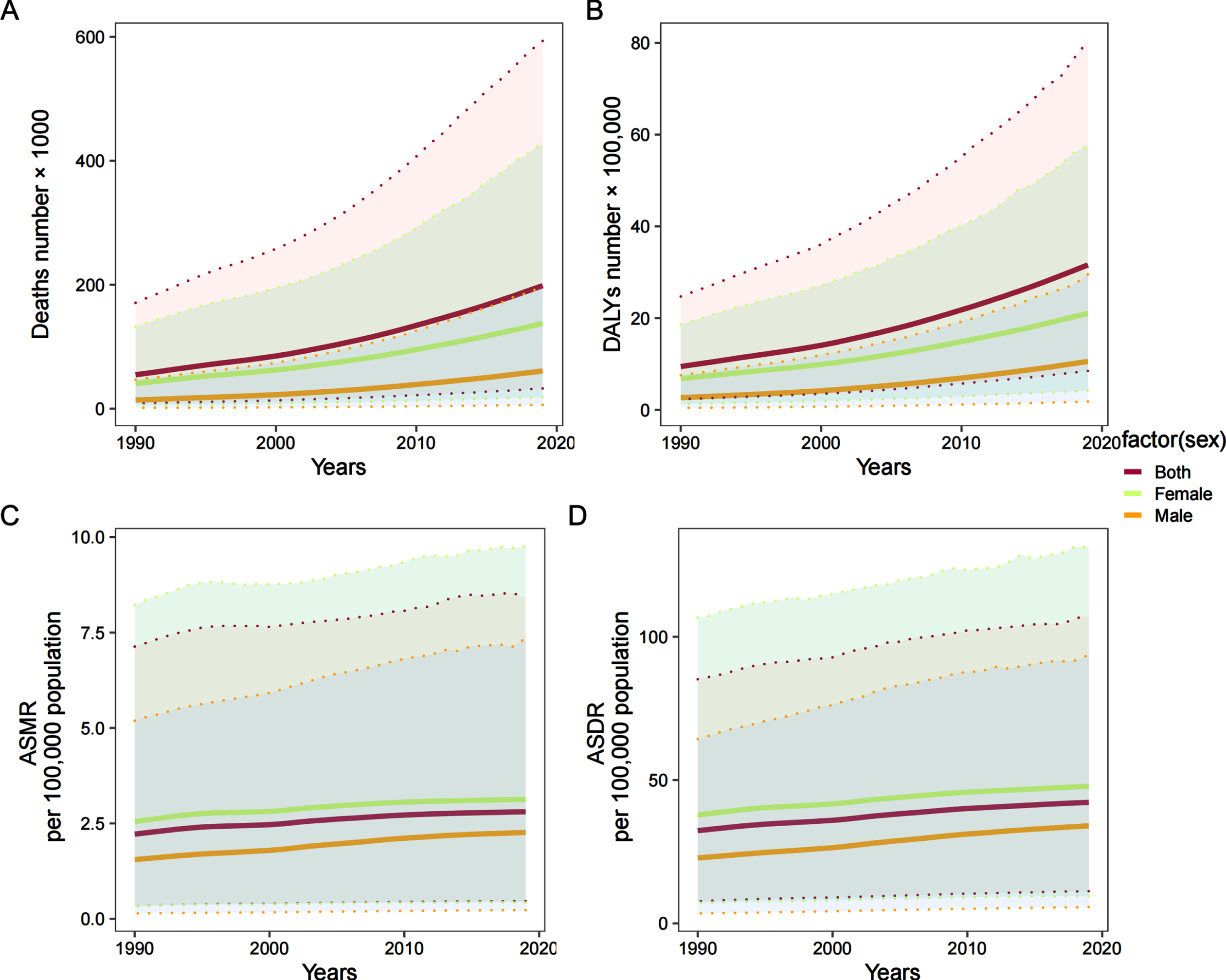
The deaths number (A), DALYs number (B), ASMR per 100,000 population (C), ASDR per 100,000 population (D) of Alzheimer’s disease and other dementias attributed to high body mass index by sex, 1990–2019. ASMR, age-standardized mortality rate; ASDR, age-standardized DALYs rate; DALYs, disability-adjusted life years.
Western Europe [570,870.2 (154, 392.2–1,412,400.2)], East Asia [493,694.5 (104,342.2–1,430,056.4)], and High-income North America [452,124.8 (132,223.5–1,078,920.9)] were the top 3 regions for the highest number of DALYs in 2019, while Oceania [1,264.3 (279.3–3,441.3)] and Central Sub-Saharan Africa [7,865.5 (1,767.2–22,219.5)] were the top 2 regions for lowest. North Africa and Middle East [72.56 (20.98–181.16)] and Central Europe [71.33 (20.38–180.28)] had the highest ASDR in 2019, while South Asia had the lowest ASDR [18.27 (4.12–51.32)]. The percentage change in DALYs of AD and other dementias attributed to high BMI between 1990 and 2019 differed across the 21 GBD regions, South Asia was experiencing the highest increased in number of DALYs (756.40%) and ASDR (161%), respectively. Central Asia (73.40%) had the lowest increased in percentage change of DALYs number, while Central Europe (26.70%) had the lowest increased in percentage change of ASDR (Table 2).
Among 204 countries and territories, US [27,980.2 (4,594–81,097.1)], China [23,787.1 (3,263.7–78,659.4)], Japan [10,297.2 (1,383.1–33,621.3)], and Russian [10,151.6 (1,693.6–30,966.5)] were the top 4 countries for the number of deaths of AD attributed to high BMI in 2019, and only in those four countries have the estimated deaths number exceeded 10,000. In contrast, there were 8 countries with fewer than one death (Micronesia, Kiribati, Palau, Marshall Islands, Tuvalu, Niue, Nauru, Tokelau) (Fig. 2A, Supplementary Material 1). The highest DALYs number were seen in China [477,209 (101,059.4–1,388,765.9)] and US [407,810.1 (120,053–965,583.3)], while the lowest were seen in Nauru [0.9 (0.2–2.6)] and Tokelau [0.6 (0.1–1.5)] (Fig. 2B, Supplementary Material 2). The highest ASMR were seen in Qatar [7.45 (1.16–23.76)] and Saudi Arabia [6.24 (1.07–18.22)] per 100,000 population in 2019, while there were 6 countries with fewer than one (Burundi, Central African Republic, Democratic People’s Republic of Korea, Bangladesh, Timor-Leste, Somalia) (Fig. 2C, Supplementary Material 3). The highest ASDR was observed in Qatar 112.23 [119.21 (29.3–285.75)] in 2019. By contrast, countries with the lowest ASDR were Timor-Leste [9.74 (1.37–32.87)] and Somalia [8.54 (0.88–31.54)] (Fig. 2D, Supplementary Material 4).
Age and sex patterns
In 2019, the global number of deaths, number of DALYs, ASMR, and ASDR of AD and other dementias attributed to high BMI in females in each age groups were higher than those in males. The number of deaths increased with age, peaking around 85–89 years in females and males, then began to decrease (Fig. 3A). Moreover, the number of DALYs increased with age, peaking at 80–84 years in females and males, then show a decrease trend. The number of age-specific DALYs peaked in 80–89-year-old females. Age-specific rates of deaths and DALYs shows an exponential growth, and the mortality and DALYs were highest in 95+ age group (Fig. 3B).
Association with the SDI
High SDI had the highest number of AD-related deaths attributed to high BMI [77,275.5 (13,021.9–229,166.4)] in 2019. High-middle SDI had the highest ASMR [3.32 (0.56–9.98)] in 2019. Low SDI had the lowest deaths number [3,973.1 (609–13,677)] and ASMR [0.8 (0.09–2.8)] in 2019. The percentage change in death number and rate of AD and other dementias attributed to high BMI between 1990 and 2019 were increased in five SDI, Low-middle SDI was seen the highest increase in deaths number (546.5%) and rate (96.7%) between 1990 and 2019, respectively. During the years 1990 to 2019, High SDI experienced the most modest increase in both the death count (190.1%) and the mortality rate (15.4%) (Table 1).
The highest number of DALYs was observed in High SDI [1,099,032.3 (302,022.7–2,723,907.8)], while the lowest was observed in low SDI [72,266.6 (15,340.1–201,923.2)] in 2019. High-middle SDI had the highest ASDR [51.13 (14.09–128.38)] in 2019. Similar to the case of death, the highest increase percentage change in DALYs number (486.1%) and rate (100.9%) were seen in Low-middle SDI. Conversely, High SDI showed the smallest rise in both the number of DALYs (158.3%) and the corresponding rate (17.9%) (Table 2).
We explored the relationship between SDI and the corresponding ASDR of AD and other dementias attributed to high BMI in 21 GBD regions from 1990 to 2019. A n-shape relationship was observed between the regional SDI and the corresponding ASDR. ASDR increases with SDI, but it decreases gradually when SDI is between 0.6 and 0.8. On the whole, the ASDR of the 21 regions showed an upward trend from 1990 to 2019. North Africa and Middle East, Tropical Latin America, Southern Sub-Saharan Africa, Central Latin America, Central Asia, Central Europe, Western Sub-Saharan Africa, and Oceania had higher than expected ASDR from 1990 to 2019. On the contrary, the ASDR of AD and other dementias attributed to high BMI was lower than expected for Andean Latin America, Caribbean, Southern Latin America, South Asia, East Asia, Southeast Asia, and High-income Asia Pacific. In the early years of the study period High-income North America, Australasia, Eastern Europe, Western Europe, and Eastern Sub-Saharan Africa had a lower burden of ASDR than expected, but their burden increased during the later years (Fig. 4).
DISCUSSION
AD is the most common type of dementia, a degenerative dementia. AD remains a major global health problem, with the burden of disease varying by regions and countries. This study represents the initial systematic analysis and report on the worldwide impact of high BMI on AD and other forms of dementia, spanning across global, regional, and national levels. In this study, we found that the number of deaths, number of DALYs, ASMR and ASDR of AD and other dementias attributed to high BMI increased from 1990 to 2019 globally. In 2019, there were 198,476.2 deaths and 3,159,912.4 DALYs of AD and other dementias attributed to high BMI, more than twice in 1990, highlighting a progressively greater burden of high BMI-related AD and other dementias. Besides, the ASMR increased by 26.6% and the ASDR by 30.4% between 1990 and 2019. The two main possible causes are an increase in obesity [33] and an ageing population with an increase in life expectancy [34–36]. At the regional level, Western Europe had the highest number of deaths, South Asia had the highest increased in percentage change of ASMR. North Africa and Middle East had the highest ASDR in 2019, while South Asia was experiencing the highest increased in percentage change of ASDR. At the national level, the US has the highest deaths number, the highest ASMR and ASDR were observed in Qatar. In addition, both the number and rate in deaths and DALYs were lower in males than in females, females have a greater disease burden than males. The mortality and DALYs rate increased with age, the mortality and DALYs were highest in 95+ age group. Furthermore, we found the relationship between regional SDI and corresponding ASDRs was a n-shape.
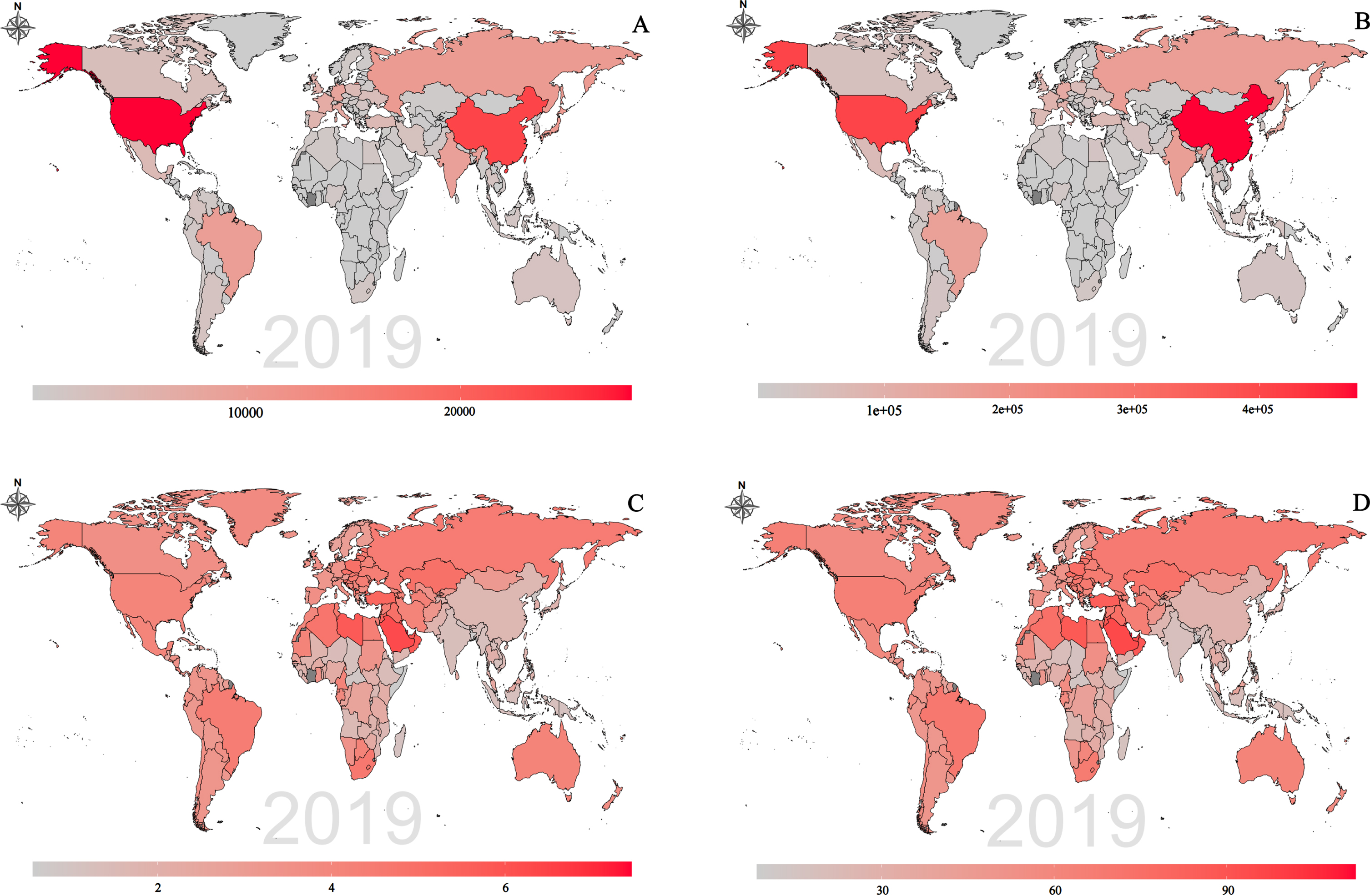
Global distribution of Alzheimer’s disease and other dementias attributed to high body mass index burden in terms of deaths number (A), DALYs number (B), ASMR (C) and ASDR (D) in 2019. ASMR, age-standardized mortality rate; ASDR, age-standardized DALYs rate; DALY, disability-adjusted life year.
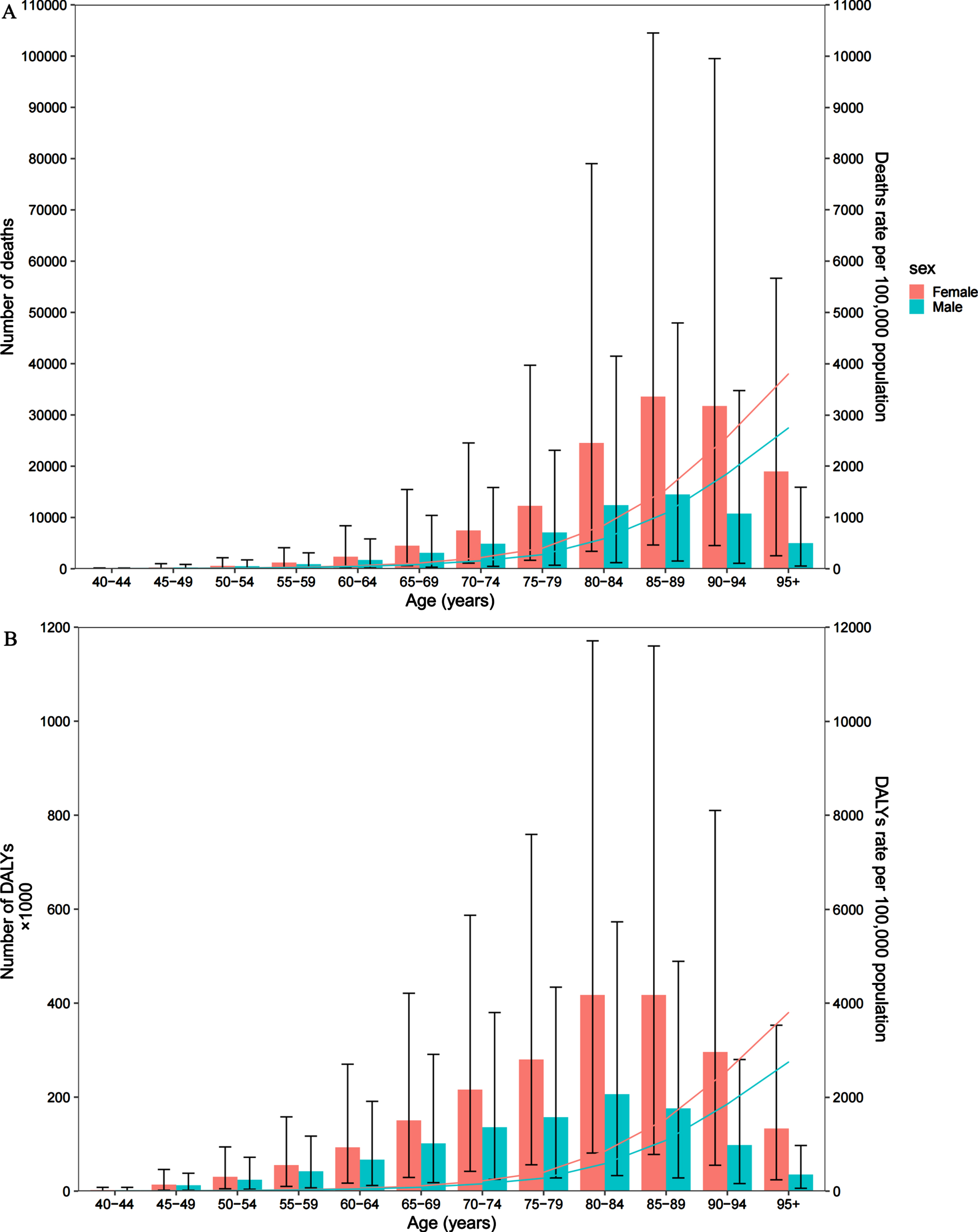
Global number of deaths and death rate (A) and global number of DALYs and DALY rate per 100,000 population (B) of Alzheimer’s disease and other dementias attributed to high body mass index by age and sex in 2019. DALY, disability-adjusted life years. The bar chart indicates the number, and the line indicates the rate.
Obesity stands among the foremost risk factors for premature mortality, with 4.7 million deaths globally in the year 2017 being attributed to this condition [33]. As per the World Health Organization (WHO), the number of obese individuals across the globe has exceeded 1 billion, comprising of 39 million children, 340 million adolescents and 650 million adults. This number is continually on the rise. WHO projects that by the year 2025, around 167 million individuals, including both children and adults who are overweight or obese, will experience a decline in their health status [37]. As outlined by WHO, for adults aged 20 years and above, BMI greater than 25 is considered overweight, while BMI greater than 30 is considered obesity [37]. In GBD 2019 study, individuals aged 20 and above with a BMI of less than 25 kg/m2 were classified as having a high BMI. Furthermore, BMI during middle age has been established as a modifiable risk factor for the development of dementia [20]. The association between high BMI in late life and the risk of developing dementia remains a topic of controversy, with some studies reporting such a link while others have not found any significant association [38–40]. However, a few studies have reported that high BMI in late life is indeed associated with an increased risk of developing dementia [41, 42]. On the other hand, some studies have indicated that late-life obesity is not significantly linked to the development of dementia [43, 44]. One potential explanation for the conflicting results regarding the association between late-life obesity and dementia risk is that the clinical diagnosis of dementia often comes after a lengthy preclinical and prodromal phase that can span several decades [41, 45]. However, dementia was the leading cause of death among diagnosed individuals. Dementia reduces lifespan, even after accounting for age, 25% of individuals with dementia passed away within a year after diagnosis, and approximately 62% within five years [46]. In this study, we found that the global number of deaths and DALYs of AD and other dementias attributed to high BMI show an age-related trend of rising first and then falling, however, the ASMR and ASDR were increased with age, our results supporting that high BMI in late life appears to increase AD risk.
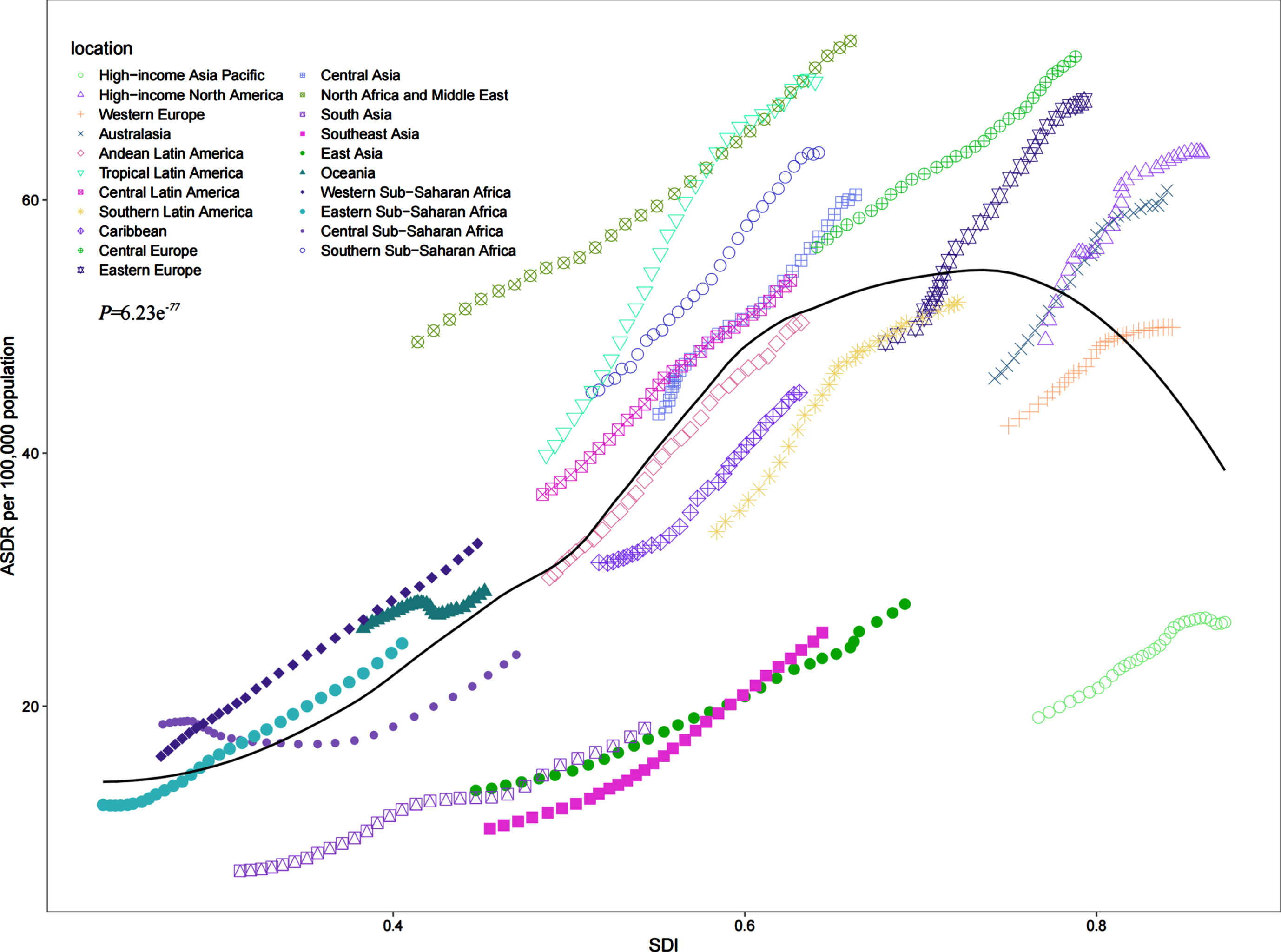
Age-standardized DALY rates (ASDR) of Alzheimer’s disease and other dementias attributed to high body mass index for 21 GBD regions by Socio-demographic Index, 1990–2019. Expected values based on Socio-demographic Index and disease rates in all locations are shown as the black line. p = 6.23e–77 < 0.01; DALY, disability-adjusted life-year; GBD, Global Burden of Diseases.
BMI and AD risk may be explained physiologically by the following mechanisms. Obesity can increase dementia risk through cerebrovascular disease [47], lowers the threshold for AD pathology, or directly affects amyloid accumulation [48, 49]. Studies have also revealed important roles of diabetes, APOE4 status, lipid profile smoking and traumatic brain injury (TBI) that associate with obesity in dementia risk. Diabetes, which is characterized by a longer duration, increases the incidence risk of prodromal AD [50]. Possible vascular risks and associated inflammation caused by low-density lipoprotein cholesterol aggravating amyloid protein in patients with mild cognitive impairment pathological changes [51]. Previous research has indicated that the APOE4 allele to be the strongest risk factor for sporadic AD and the impact of the APOE4 genotype on dementia or AD risk in nondemented participants was dependent on physical and lifestyle factors such as BMI, smoking, and physical activity [52]. Smoking associated with increased risk of development of dementia in older adults via increasing air particulate matter and vascular and toxic effects [53]. It also has synergistic effect with diabetes on dementia. TBI, mortality of which is predicted by high BMI [54], may also increase the risk of AD [55]. Metabolic dysfunction has been the common pathology in both TBI and AD [56]. The management of these potential risk factors may be beneficial to the early detection and prevention of dementia. Later in life, when underweight, macronutrients and micronutrients deficiencies may aggravate cognitive function since low energy intake causes low energy intake [57, 58]. For instance, the neuronal cell membrane is affected by essential fatty acids deficiency [59], and vitamin deficiencies may worsen oxidative stress [60]. Besides, research has shown that the prevalence rate of overweight and obesity on a global scale is significantly higher in older females when compared to their male counterparts [17, 61]. Public health strategies to screen for AD more actively in the overweight population in late life. Control weight at early stage of life and improve public nutritional status to prevent overweight in older adults may help reduce the burden of AD.
Furthermore, studies had suggested that the level and different life stages, high BMI contribute to different levels of risk of AD. As a metabolic risk factors, high BMI were more prevalent in females than in males [62]. In this study, we found that number of deaths and death rate, and number of DALYs and DALY rate of AD and other dementias attributed to high BMI were higher in females than in males among all age stages during this period. This finding suggests that the disease burden in females is higher than in males. The prevalence pattern differs between sexes may be caused by hormone levels, genetic susceptibility, or mental health [63]. Influenced by sex hormones, female’s brains are inherently more susceptible to AD [64]. Known to maintain neuronal homeostasis, estrogens protect neurons from damage and regulate bioenergetics in the nervous system [65–67]. Additionally, estrogens can inhibit amyloid-β (Aβ) deposition by regulating β-secretase (BACE1) or neprilysin [68]. AD is more likely to develop in females than males, and its incidence increases after menopause [69]. Sex and apolipoprotein E (APOE) allele polymorphisms may also work in concert with these [70]. APOE ɛ4 allele can inhibit mitochondrial dysfunction, modulates neurogenesis, and reduces levels of amyloid -protein. As a risk factor for AD, the expression of APOE ɛ4 allele are lower in females than males [71]. In comparison with males, females are twice as likely to develop structural and functional disorders of the nervous system, as well as psychological problems, such as depression [72]. These conditions all increase the risk of AD. In addition, females live longer than males, accounting for a substantial proportion of the aging population [73]. However, late-life BMI level and AD risk were complicated, further research is needed. In this regard, strengthening dementia prevention, treatment, and interventions targeting female patients is essential.
At the regional level, geographically, BMI-related AD and other dementias burdens exhibited significant heterogeneity. The prevalence of overweight and obesity is now increasing in low- and middle-income countries, particularly in urban areas [37]. In this study, Western Europe had the highest deaths and DALYs number, North Africa had the highest ASMR and ASDR. The percentage change in 21 regions have a different degree of increase from 1990 to 2019, South Asia was experiencing the highest increased in number of deaths, DALYs, and ASDR, South Asia had the highest increased in percentage change of ASMR. In 2019, North Africa and the Middle East had the highest ASDR attributable to overweight and obesity, while South Asia experienced the highest percentage increase in ASDR due to these risk factors. Besides, the deaths number, ASMR, and ASDR were increased in five SDI, although the ASMR and ASDR in High SDI were lowest increase among five SDI, High SDI still had the highest number of deaths in 2019. Therefore, it is widely thought that the effect of high BMI on AD will become more serious in the future. However, the percentage change of deaths number, ASMR, ASDR were increased in Low-middle SDI. Overall, the burden of overweight and obesity remains significant in developed regions, while it is increasing rapidly in less developed areas. When examining the relationship between the Social Development Index (SDI) and the corresponding ASDR of AD and other dementias attributed to high BMI, there is a positive correlation between the two. As the SDI increases, the corresponding ASDR also increases. The likely reason is the rise of urbanization, sedentary lifestyles, decrease in physical activity, increase in television and video games are factors that contribute to weight gain [74, 75]. Unrecognized factors may have a significant influence, such as people choose and consume junk foods due to inadequate pharmacological options and an increase in stress [76]. When the SDI falls within the range of 0.6 to 0.8, the ASDR evinces a gradual decrease as the SDI increases, which may be attributed to the country’s economic level. It is widely believed that more developed countries exhibit higher levels of medical sophistication. At the same time, the decline in ASDR may result from better dietary habits and improved socioeconomic conditions.
At the national level, we found that in 2019, the US had the largest deaths number of AD and other dementias burden attributed to high BMI, which was three-fold higher than Japan, which may be attributed to the fact that the US has a large obesity population in the world, the prevalence of overweight and obesity is 31.0% of those aged more than 60 years adults [77]. A previous study found high BMI to be one of the most significant risk factors for health in the US [78]. However, the highest ASMR and ASDR were observed in Qatar. There was a high prevalence of obesity among adults and children in the Arabian Gulf, which was considered a public health issue [79, 80]. Although the medical level of Qatar is considered to be of a high standard and is constantly improving. According to recent research conducted in Qatar, the comprehension of health care professionals about dementia and AD is moderate overall. Despite having a largely favorable attitude, their knowledge of fundamental disease pathophysiology and recent advances in research is inadequate [81]. To minimize obesity-related harm, government agencies and other healthcare organizations should implement new measures to reduce obesity, especially in developed countries. Meanwhile, proper prevention and education about high BMI should be given to the general population.
There were some limitations to our study. First, specific data on trends in mortality and DALYS from 1990 to 2019 were unavailable. Besides, in certain regions with low SDI and low-middle SDI, high-quality data was not available, and therefore, estimates were based on modeling techniques. This approach may introduce biases in the data analysis. Furthermore, several contributing factors, such as genetic influences, diabetes, and TBI, are interconnected with BMI. We did not further differentiate the impact of these factors on the outcomes. Finally, we did not assess the effect of different levels of high BMI on the risk of AD and otherdementias.
Conclusion
Our study found that the number of deaths, number of DALYs, ASMR, and ASDR were increased for AD and other dementias attributed to high BMI from 1990 to 2019, globally. Females accounted predominantly for the burden than males. The weight of the burden in developed regions remains significant, while that in less developed areas is rapidly increasing. The burden of AD imposed by high BMI is particularly dramatic, steps against high BMI may be effective in reducing the burden of AD and other dementias. Our results can be used as a reference for national and regional guidelines on AD and other dementias attributed to high BMI. The policy- and decision-makers of public health, as well as other relevant stakeholders, should prioritize this issue and design effective policies to address it.
Footnotes
ACKNOWLEDGMENTS
We are grateful for the work of the Global Burden of Disease study 2019 collaborators.
FUNDING
The work was supported by the National Natural Science Foundation of China (No.82074278), and the Special Foundation of Guangdong Educational Committee (No. 2021ZDZX2001).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.