
Abstract
Background:
Periodontal disease (PeD) is a risk factor of Alzheimer’s disease and is associated with cognitive decline in older adults. However, the relationships between subitems of neuropsychological tests and PeD have not been fully clarified.
Objective:
To evaluate associations between PeD and subitems of neuropsychological tests.
Methods:
We performed a cross-sectional analysis of data of 183 participants (women: 50%, mean age: 79 years) from a clinical study. We enrolled patients who visited our memory clinic and assessed demographics, dementia-related risk factors, neuropsychological tests, brain magnetic resonance images, and a dental screening check. We evaluated the relationships between cognitive function and PeD using multivariable logistic regression analyses.
Results:
Participants with dementia were less likely to make periodical visits to the dentist, had fewer teeth, had less frequent tooth brushing habits, and were more likely to have PeD. Impaired cognitive function was significantly associated with an increasing degree of PeD. In multivariable logistic regression analyses, impaired visuospatial function and attention were associated with twice the risk of moderate or severe PeD compared with individuals with preserved visuospatial function and attention (odds ratio: 2.11, 95% confidence interval: 1.04–4.29, p = 0.037). Impaired word recall and recognition and following commands were associated with increased risk of PeD (odds ratio: 2.80, 95% confidence interval: 1.41–5.32, p = 0.003).
Conclusions:
Cognitive decline, such as impaired visuospatial function, attention, word recall and recognition, and inability to follow commands were independently and strongly associated with PeD. These items can be assessed easily on a daily basis.
INTRODUCTION
Dementia is a major public health issue. Approximately 47 million people worldwide were living with dementia in 2015 [1]. The number of people with dementia globally is expected to increase approximately 1.5-fold by 2030 [1], and the financial cost of dementia has steadily increased in recent years [1, 2]. Japan is facing substantial age-related healthcare challenges. The percentage of the population in Japan aged 65 and over has risen to nearly 30% [3], and the number of patients with dementia is also increasing. Thus, a comprehensive strategy to reduce the impacts of dementia has been developed, with the aim of extending healthy life expectancy [4].
In recent years, there has been an increasing focus on the associations between periodontal disease (PeD) and cognitive decline [5–9]. PeD is an inflammatory disease that is affected by a variety of factors, including smoking, gender, stress, depressive mode, and education level [10, 11]. PeD increases the risk of life-threatening diseases, such as cerebrovascular diseases [12], as well as leading to tooth loss [13], and constitutes a potentially preventable and modifiable risk factor for cognitive impairment [8]. Additionally, PeD is associated with amyloid-β, which underlies the onset of dementia [14, 15]. Thus, the prevention and management of PeD in middle-aged and older adults may be important for reducing the risk of dementia.
Several clinical studies of the relationship between PeD and cognitive function have been conducted in a memory clinic setting, including a small interview-based study [16] and several case-control studies [17–19]. However, there is still a lack of knowledge regarding comprehensive assessment for both PeD and cognitive function, including various neuropsychological tests and brain magnetic resonance imaging (MRI).
We have conducted observational research to examine the relationship between gut microbiota and cognitive function. In our previous studies, gut microbiota were found to be associated with cognitive decline [20–22], risk factors [23, 24], cerebral small vessel disease [25, 26], and blood biomarkers [27, 28]. These findings suggest the existence of gut microbiome-brain cascades. However, PeD, as a microbial factor, has not yet been fully investigated. Examining PeD in the setting of a comprehensive memory clinic and identifying its links with various neuropsychological tests may clarify an unidentified pathway of the periodontal–brain axis. In addition, identification of specific subitems of neuropsychological tests which are closely related to PeD may be helpful for identifying older adults who have a high risk for PeD easily on a daily basis.
Thus, the present study aimed to evaluate the relationship between PeD, neuropsychological test performance, and cognitive biomarkers. We hypothesized that PeD would be independently associated with subitems of neuropsychological tests in our cohort data.
MATERIALS AND METHODS
Study design
This was a single-center observational study designed as a clinical survey to clarify the association between PeD, oral health, and cognitive function (Periodontal Disease Assessment Study: the Pearl study), conducted at the National Center for Geriatrics and Gerontology (NCGG) in Japan. The Pearl study was conducted as a collaboration between the NCGG and the Lion Foundation for Dental Health. The study complied with the Declaration of Helsinki and was approved by the institutional review boards of the NCGG (No. 1533) and the Lion Foundation for Dental Health (No. LDH202107). Informed consent was obtained from all patients and their families. This study was registered with the UMIN Clinical Trials Registry (UMIN000048126).
Participants
Between August 2021 and April 2022, we enrolled consecutive patients visiting the memory clinic at the NCGG who agreed to undergo medical assessment of cognitive function and a dental examination to assess PeD. Information about the Pearl study was provided via a leaflet at the memory clinic reception, and patients who wished to participate were informed about the study in detail. Patients were eligible for the study if they: 1) were able to undergo brain MRI; 2) provided written informed consent; 3) provided informed consent for the NCGG Biobank to store their clinical data and blood samples; and 4) were accompanied by family members who could assess the condition of the patient. We excluded patients if they: 1) were unable to undergo MRI examination, or if the MRI scan could not be evaluated because of movement; 2) had a history of a major psychological disorder, or currently exhibited serious or unstable alcohol or drug abuse; or 3) were judged by an investigator to be ineligible to participate as a study subject for any other reason.
Assessments
All participants underwent a comprehensive geriatric assessment [29] of the following features: 1) demographic characteristics; 2) risk factors; 3) activities of daily living (ADL); 4) global cognitive function; 5) neuropsychological tests; 6) behavioral and psychological symptoms; 7) depression status; 8) laboratory parameters, such as apolipoprotein E ɛ4; 9) ankle-brachial index and pulse wave velocity as indicators of arteriosclerosis [30] and the “impact” of pulse [31], respectively; 10) results of brain MRI; and 11) lifestyle factors, including living alone, physical exercise habits, daytime napping, and being a recipient of the Long-Term Care Insurance (LTCI) system [32]. Clinical data were partially provided by the NCGG Biobank, which collects clinical data for research.
Classification of cognitive function
Global cognitive function was assessed using the Mini-Mental State Examination (MMSE) [33] and Clinical Dementia Rating (CDR) scales [34]. We divided patients into two categories according to their MMSE scores and CDR scales: dementia and non-dementia. Dementia was defined as having either 1) CDR global score of ≥1 or (2) both an MMSE score of ≤23 and a CDR global score of ≥0.5 [35], because a CDR global score of 0.5 indicates very mild dementia [36]. Non-dementia was defined as having both an MMSE score of ≥24 and a CDR global score ≤0.5. Mild cognitive impairment was included in the non-dementia group in the present study. Our definitions of dementia and mild cognitive impairment were in accordance with the criteria of the National Institute of Aging-Alzheimer’s Association (NIA/AA) workgroups [37, 38]. We also conducted neuropsychological tests such as the Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-cog) [39], Frontal Assessment Battery (FAB) [40], Raven’s Coloured Progressive Matrices (RCPM) [41].
Brain imaging
Brain MRI scans were performed using a 3-Tesla MRI scanner (Magnetom Skyra, Siemens Healthineers AG, Munich, Germany). The MRI examination comprised standardized sequences used for analysis of the brain. T1-weighted, T2-weighted, fluid-attenuated inversion recovery imaging, T2*-weighted gradient echo imaging, and intracranial 3D time-of-flight MR angiography were conducted. The presence of cerebral small vessel disease and its components, such as silent lacunar infarcts, white matter hyperintensity, cerebral microbleeds, and enlarged periventricular space, was assessed. The voxel-based specific regional analysis system for Alzheimer’s disease (VSRAD) software (Eisai Co., Ltd., Tokyo, Japan) was used to quantify cortical and hippocampal atrophy as an indicator of Alzheimer’s disease.
Dental examination
The dental examination was conducted by one trained periodontist (Y.I.) and dental hygienists, independent of the clinical data collection. First, dental history was obtained from the participants and their family members. Second, the number of teeth, clinical attachment loss, and probing pocket depth were measured. Clinical attachment loss and probing pocket depth indicate the gingiva tissue destruction caused by PeD (Fig. 1) [42]. Participants were categorized into four groups (none, mild, moderate, and severe PeD) according to the CDC/AAP definitions (Supplementary Table 1) [43]. Six sites per tooth were examined with a CPUNC15 periodontal probe (Hu-Friedy Mfg. Co. LLC., Chicago, IL, USA) as previously reported [44].
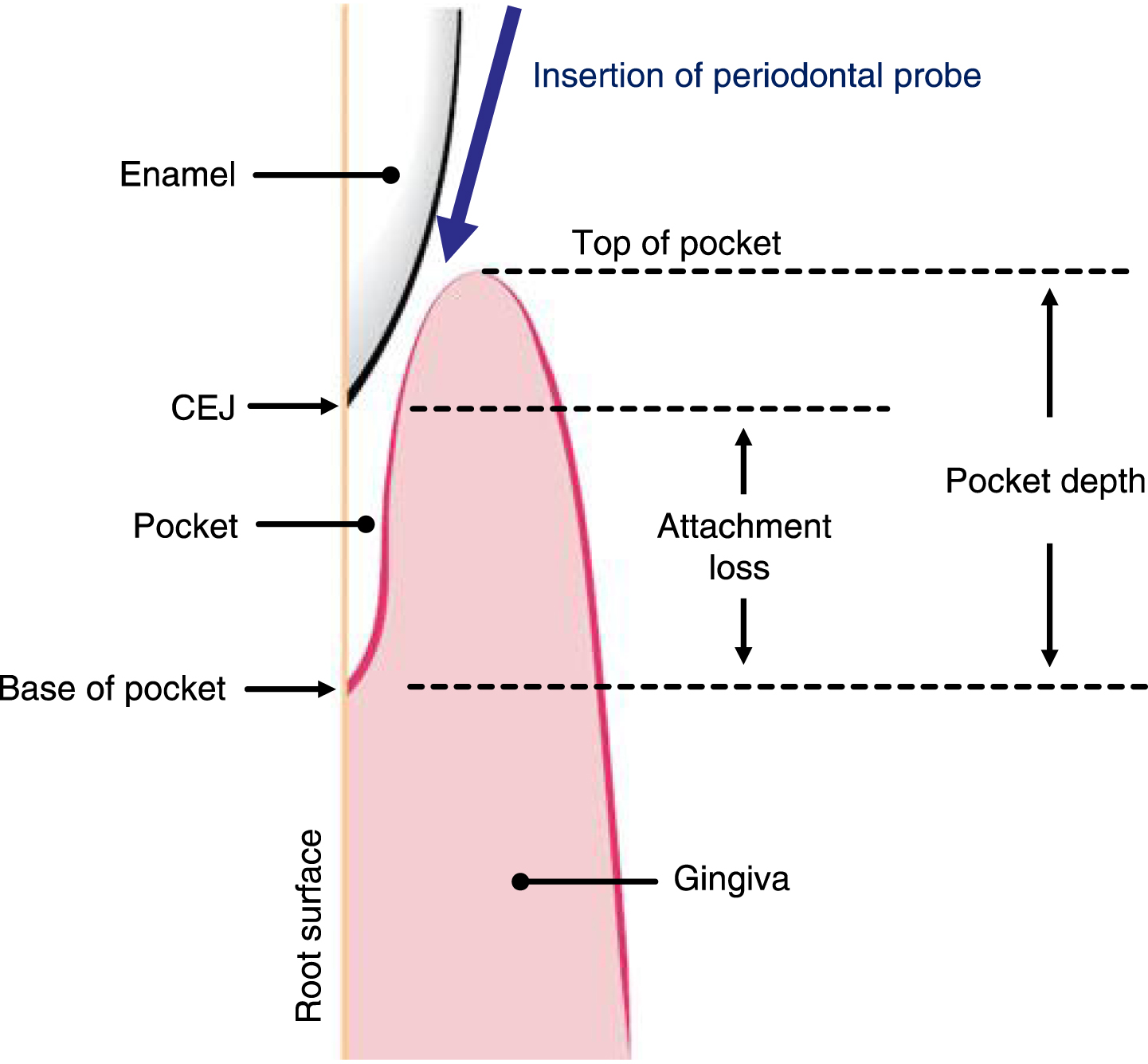
Diagram of clinical attachment loss and pocket depth in a patient with periodontal disease. This figure shows the schema of the clinical attachment loss and probing pocket depth, which indicate periodontal disease (PeD) [42]. The pocket is the space between the root surface and the gingiva. In PeD, the base of the pocket migrates apically, thereby creating a pocket. The base of the pocket is therefore apical to the cementoenamel junction (CEJ, the boundary between the enamel crown and the root), and attachment loss can be measured using a periodontal probe from the CEJ to the base of the pocket. Probing pocket depth is measured from the top of the pocket to the base of the pocket. Probing pocket depth is usually greater than attachment loss due to the inflammation-induced swelling of the gingiva. The direction of insertion of a periodontal probe is also indicated in this figure [42].
Statistical analysis
Continuous, ordinal, and categorical variables are expressed as means±standard deviations, medians and interquartile ranges, and frequencies and proportions (percentages), respectively. Data were compared using Student’s unpaired t-tests, Wilcoxon rank-sum tests, and χ2 tests, respectively. First, we compared clinical characteristics between men and women, participants with dementia and those without dementia. Second, we compared clinical characteristics and cognitive function between participants with moderate or severe PeD including edentate status, and those with mild PeD or no PeD. Third, we assessed the relationships between neuropsychological tests and the presence of PeD. MoCA-J items were categorized into six subgroups (visuospatial function, attention, language, executive function, memory, and orientation) according to a previous study [45]. We assessed the cutoff values of neuropsychological tests and area under the receiver operating characteristic curve (AUC) for the detection of severe or moderate PeD. Finally, multivariable logistic regression models were used to identify independent associations between the presence of moderate or severe PeD and neuropsychological tests. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. All comparisons were two-tailed, and p < 0.05 represented statistical significance. Data were analyzed using the JMP 17.1 software package (SAS Institute Inc., Cary, NC, USA).
RESULTS
Participant characteristics
We enrolled 201 participants in this study. Of these, 18 participants were excluded (13: participation revoked; 5: insufficient data). Ultimately, we analyzed 183 participants (women: 50%, mean age: 79 years, dementia: n = 93). Women were less likely than men to have a current and/or past smoking habit (women versus men; 8.8% versus 65.2%, p < 0.001), to consume alcohol (9.9% versus 34.8%, p < 0.001), to have a hearing impairment (46.1% versus 68.5%, p = 0.003), to use a removable partial denture or dental implant (44.0% versus 59.8%, p = 0.039), to take naps, and were more likely to live alone (16.7% versus 3.4%, p = 0.004), and to brush their teeth daily (Supplementary Tables 2 and 3). However, there were no significant differences between women and men in age, global cognitive function, risk factors such as hypertension and diabetes mellitus, and the degree of PeD.
Dementia versus non-dementia
Compared with participants without dementia, participants with dementia were more likely to be apolipoprotein E ɛ4 carriers (dementia versus non-dementia; 40% versus 24%, p = 0.028), to have impaired cognitive function, to have a history of falls in a year (39% versus 25%, p = 0.040), and to exhibit white matter hyperintensity (58% versus 36%, p = 0.003), as well as having higher VSRAD scores (median score: 1.81 versus 0.97, p < 0.001), walking more slowly (gait speed; 0.93 versus 1.06 m/s, p < 0.001), and taking naps more frequently (Table 1, Supplementary Table 4). Furthermore, participants with dementia were less likely than those without dementia to make periodical visits to the dentist (67.7% versus 84.4%, p = 0.010), had a smaller number of remaining teeth (median number; 21 versus 23, p = 0.036), and had less frequent teeth-brushing habits (Table 2, Supplementary Table 5).
Comparisons of background information between participants with and without all-cause dementia
Data are presented as medians, interquartile ranges or number of patients (%). The Wilcoxon rank-sum test and χ2 test were used. ADAS-cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; APOE, apolipoprotein E; CDR-SOB, Clinical Dementia Rating-Sum of Boxes; CMB, cerebral microbleed; DBDS, Dementia Behavior Disturbance Scale; EPVS, enlarged periventricular space; FAB, Frontal Assessment Battery; GDS, Geriatric Depression Scale; IADL, instrumental activities of daily living; LTCI, Long-Term Care Insurance; MMSE, Mini-Mental State Examination; MNA-SF, Mini-Nutritional Assessment-Short Form; MoCA-J, Montreal Cognitive Assessment-Japanese version; MRI, magnetic resonance imaging; RCPM, Raven’s Coloured Progressive Matrices; SLI, silent lacunar infarct; VSRAD, voxel-based specific regional analysis system for Alzheimer’s disease; WMH, white matter hyperintensity.
Comparisons of periodontal information between participants with and those without all-cause dementia
Data are presented as medians, interquartile ranges or number of patients (%). The Wilcoxon rank-sum test and χ2 test were used. *Periodontal disease was defined according to the classification proposed by the workgroup from the Centers for Disease Control and Prevention in partnership with the American Academy of Periodontology (CDC/AAP criteria). †Fifteen participants had no data for attachment level and probing depth because they had no teeth as a result of severe periodontal disease. ‡Any use of removable partial denture or dental implant.
No PeD and mild PeD versus moderate and severe PeD
Compared with participants with no PeD and mild PeD, participants with moderate and severe PeD were more likely to have impaired cognitive function, apathy (median vitality index; 9 versus 10, p = 0.037), and had higher scores on the ankle-brachial index (median value; 1.13 versus 1.10, p = 0.003). However, there were no significant differences between these two groups in age, sex, and risk factors (Table 3, Supplementary Table 6). Furthermore, participants with moderate and severe PeD were less likely than those with no PeD and mild PeD to make periodical visits to the dentist (moderate and severe PeD versus no PeD and mild PeD; 69.4% versus 86.1%, p = 0.013), had a lower number of remaining teeth (median; 21 versus 24, p = 0.009), and had less frequent teeth-brushing habits (Table 3, Supplementary Table 7). Participants with moderate and severe PeD were more likely to live alone, to rarely engage in physical exercise, and to receive LTCI, and more frequently took daytime naps, although these differences were not significant.
Comparisons of background information of participants with periodontal disease (PeD; moderate and severe versus none and mild)
Data are presented as medians, interquartile ranges, or number of patients (%). The Wilcoxon rank-sum test and χ2 test were used. ADAS-cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; CDR-SOB, Clinical Dementia Rating-Sum of Boxes; EPVS, enlarged periventricular space; FAB, Frontal Assessment Battery; LTCI, Long-Term Care Insurance; MMSE, Mini-Mental State Examination; MoCA-J, Montreal Cognitive Assessment-Japanese version; MRI, magnetic resonance imaging; RCPM, Raven’s Coloured Progressive Matrices.
Cognitive function and PeD
Cognitive function impairment, as indicated by MMSE, MoCA-J, ADAS-cog, FAB, and RCPM scores, was significantly associated with increasing severity of PeD (Fig. 2). The significant cutoff values of these neuropsychological tests for the presence of moderate and severe PeD detection were as follows: MMSE: 24, MoCA-J: 18, ADAS-cog: 16, FAB: 14, RCPM: 23, respectively (Table 4, Supplementary Figure 1). The AUC of the MMSE was the lowest among the neuropsychological tests. Two MoCA-J items (impaired visuospatial function and attention) and three ADAS-cog items (impaired word recall task, following commands task, and word recognition task), which were extracted on the basis of significant results in the univariate logistic regression analyses, showed the highest OR (OR 1.21; by two MoCA-J items) and the highest AUC (AUC 0.653; by three ADAS-cog items) among the neuropsychological function tests (Supplementary Figure 2, Supplementary Table 8).
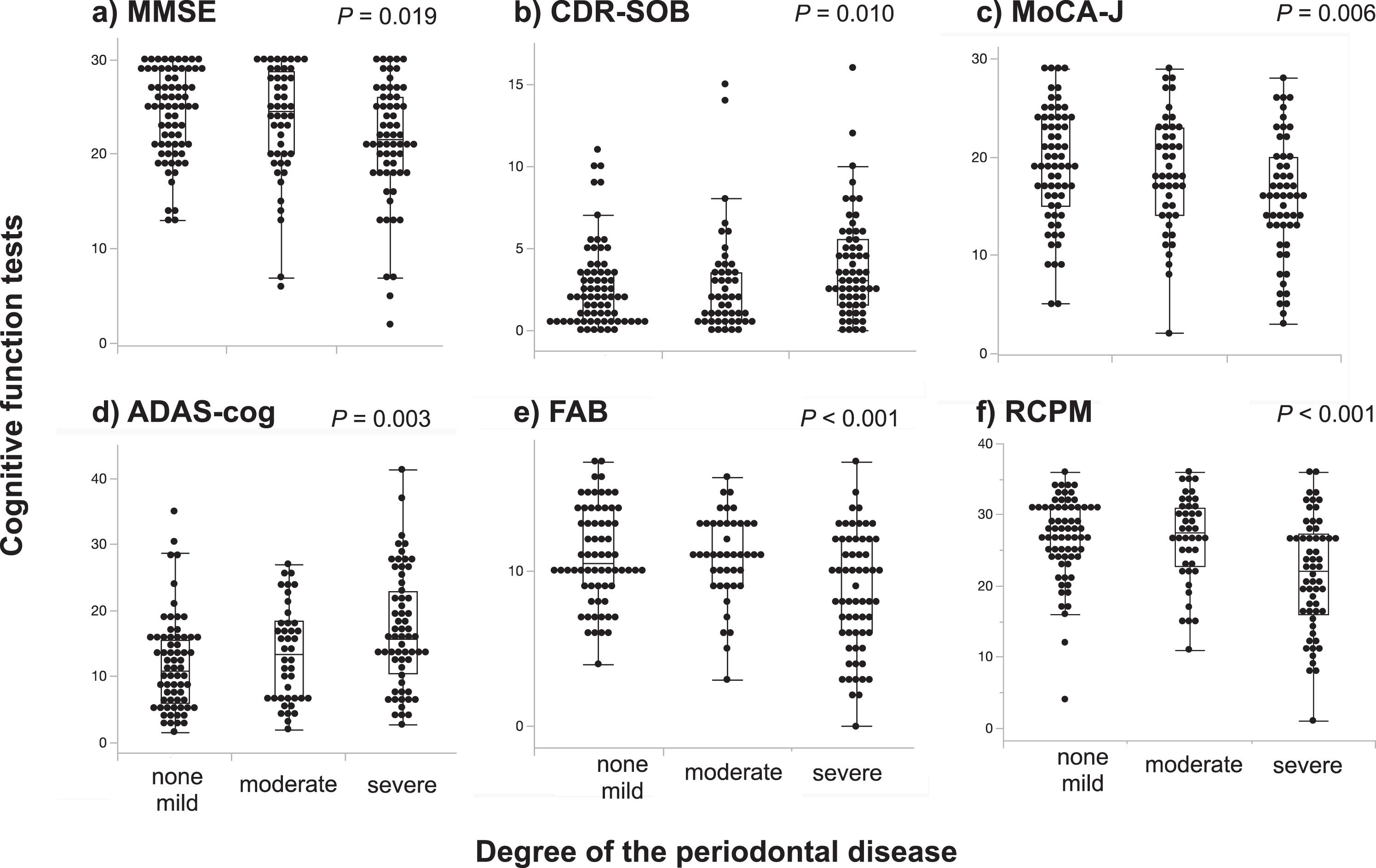
Associations between cognitive function tests and the degree of periodontal disease divided by three groups. The results of cognitive function tests indicated by MMSE (a), CDR-SOB (b), MoCA-J (c), ADAS-cog (d), FAB (e), and RCPM (f) are plotted relative to the degree of periodontal disease stratified into three groups based on the following classifications: none or mild, moderate, and severe periodontal disease. Degree of cognitive impairment increase with increasing degrees of periodontal disease (Kruskal–Wallis test). ADAS-cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; CDR-SOB, Clinical Dementia Rating-sum of boxes; FAB, Frontal Assessment Battery; MMSE, Mini-Mental State Examination; MoCA-J, Montreal Cognitive Assessment-Japanese version; RCPM, Raven’s Coloured Progressive Matrices.
The cutoff values of neurological tests for the presence of mild or severe periodontal disease detection
*Odds ratio indicates cognitive function impairment per one point of increase or decrease in performance on each neuropsychological test. †Two MoCA-J items and three ADAS-cog items were extracted according to the assessment of the individual items of MoCA-J and ADAS-cog showing the presence of moderate or severe periodontal disease, as shown in Table S3. ADAS-cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; AUC, Area under the receiver operating characteristic curve; FAB, Frontal Assessment Battery; MMSE, Mini-Mental State Examination; MoCA-J, Montreal Cognitive Assessment-Japanese version; OR, odds ratio; RCPM, Raven’s Coloured Progressive Matrices.
Multivariable analyses
Multivariable logistic regression analyses revealed significant associations between moderate and severe PeD, and the results of neuropsychological tests (MMSE, MoCA-J, ADAS-cog, RCPM, and FAB) (Supplementary Table 9). In addition, two MoCA-J items (lower than the cutoff score for the detection of moderate or severe PeD) were associated with twice the risk of the presence of moderate or severe PeD (OR: 2.11, 95% CI: 1.04–4.29, p = 0.037) compared with the MMSE (by 1 point decrease; OR: 1.06, 95% CI: 1.00–1.13, p = 0.051). Likewise, three ADAS-cog items were associated with approximately three times the risk (OR: 2.80, 95% CI: 1.41–5.32, p = 0.003), as calculated in the stepwise multivariable logistic regression analyses after adjusting for other confounding covariables (Table 5, Supplementary Table 10).
Multivariable logistic regression analyses for the presence of moderate or severe periodontal disease
The dependent variable was the presence of moderate or severe periodontal disease. Model: backward stepwise multivariable logistic regression analysis adjusted for age, sex, risk factors (hypertension, dyslipidemia, diabetes mellitus, a history of stroke, chronic kidney disease, smoking, alcohol consumption, and apolipoprotein E ɛ4), years of education, components of cerebral small vessel disease (silent lacunar infarcts, white matter hyperintensity, cerebral microbleeds, and enlarged perivascular spaces), and VSRAD score. ADAS-cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; CI, confidence interval; EPVS, enlarged perivascular spaces; MMSE, Mini-Mental State Examination; MoCA-J, Montreal Cognitive Assessment-Japanese version; OR, odds ratio.
DISCUSSION
The main finding of the present study was that performance on a range of neuropsychological tests (MMSE, MoCA-J, ADAS-cog, FAB, and RCPM) was independently associated with the presence of moderate or severe PeD. Among the tests, the MMSE had the lowest AUC. Additionally, impaired visuospatial function and attention extracted from the MoCA-J were associated with twice the risk of the presence of moderate or severe PeD compared with the MMSE after adjustment of covariables. Likewise, impaired word recall and recognition, and following commands task performance extracted from ADAS-cog, were associated with approximately three times the risk of PeD. These findings may indicate close relationships between cognitive impairment and the presence of PeD.
Few previous studies have conducted comprehensive testing with a range of scales, such as assessment of ADL, various neuropsychological tests, brain MRI, and oral function testing. In addition, none of the previous reports comprehensively assessed the importance of accurately measuring cognitive impairment when considering its relationship with PeD. Previous studies reported an association between dementia and PeD using various neuropsychological tests, such as MMSE, CDR, and ADAS-cog [17–19, 47]. Importantly, the present results revealed the novel finding that two MoCA-J items and three ADAS-cog items were superior for detecting the presence of moderate or severe PeD compared with the MMSE. The MMSE is widely used as a standard cognitive screening test. A previous study reported that 14 of 22 clinical studies of PeD used the MMSE alone [9]. Our findings identified specific neuropsychological items that were closely associated with PeD. Furthermore, these items can be assessed easily on a daily basis without measuring MMSE.
Teeth-brushing is an important factor for preventing PeD [8]. In older adults with dementia, maintaining oral healthcare is difficult because of decreased ADL ability. Specifically, impaired visuospatial function and attention can lead to an inability to brush teeth. Preparing a toothbrush and toothpaste, and correctly performing teeth-brushing requires visuospatial function and attention, which correspond to two MoCA-J items. Furthermore, impaired word recall and recognition, and impaired performance in the following commands task may interfere with tooth brushing and the inability to implement teeth-brushing recommendations from family members or caregivers. In contrast, the ratio of the orientation area to the whole area is high in the MMSE compared with that of MoCA-J (score of orientation per total score; MMSE: 10/30, MoCA-J: 6/30). This high ratio in the MMSE may have led to the lowest AUC for detecting the presence of PeD.
Social factors may be also associated with PeD [8, 19]. Older adults with dementia were less likely to visit dentists, had less frequent teeth-brushing habits, and more frequently took daytime naps in the present study. Daytime napping increases the risk of PeD because salivation decreases during sleep [8]. Additionally, salivation decreases in older adults with dementia [8]. Thus, these factors increase the risk of PeD. Furthermore, older adults with moderate or severe PeD were more likely to live alone, to rarely engage in physical exercise, to receive LTCI, and to more frequently take daytime naps in the present study. These factors are suggestive of impaired ADL and social frailty. Living alone with cognitive decline leads to a greater need for daily living support to continue living in the community and passive attitudes about their dental care [48] may be associated with difficulty visiting dentists. Dental visits are important because they can prevent oral and physical frailty [49], in addition to preventing PeD. Poor oral health status has negative biological, behavioral, and social impacts on daily activities and quality of life among older adults [50]. Furthermore, oral health interventions by oral healthcare coaches may be effective for improving oral health in care-dependent older adults [51]. Therefore, social healthcare support for oral function may contribute to the prevention of worsening PeD in older adults with dementia.
The present study yielded several important findings. First, there were significant differences between women and men regarding habits of smoking, alcohol consumption, and brushing teeth. Additionally, the extent of PeD was less severe in women compared with men. However, women with PeD had an increased risk of cognitive decline compared with men [52]. These findings suggest gender differences in the risk of PeD [47]. Second, in the current study, probing depth was not significantly different between the dementia and non-dementia groups. This finding is in accord with a previous study [7].
The present study had several strengths. First, the results revealed novel relationships between neuropsychological test performance and PeD. To reduce the burden of PeD and prevent PeD in older adults, detection of potential risk and the development of countermeasures for PeD may contribute to healthcare in older adults with dementia. Second, we identified neuropsychological assessment items for detecting moderate or severe PeD that were more sensitive compared with the MMSE. In daily life and clinical settings, assessing these items will be helpful for screening PeD in older adults by checking teeth-brushing ability. Finally, whereas most previous studies of PeD used the MMSE alone [9], we conducted a detailed assessment of ADL, brain MRI, and lifestyle in addition to neuropsychological tests. Concomitant assessment of these factors and cognitive function may shed light on the association between PeD and dementia.
The present study involved several limitations. We were unable to clarify the causal relationship between PeD and cognitive function because of the study’s cross-sectional design. Additionally, selection bias may have affected the results because our sample was a single hospital-based cohort and sample size was not calculated. Because of the small number of participants, we handled individuals with moderate PeD, severe PeD, and edentulism as an aggravation group, because edentulism status is known to be associated with a high risk of mortality, as well as moderate or severe PeD [53]. Additionally, we did not assess the details of each dementia subtype. We plan to examine this issue further in future research. We did not assess oral microbiota such as Porphyromonas gingivalis in the present study, which are recent clinical problems regarding Alzheimer’s disease [55]. Concomitant assessment of oral and fecal microbiota [56] was not performed in the present study. However, because we stored the oral samples from the Pearl study, we plan to address this issue in the near future.
Overall, although this was a cross-sectional study, the results provided evidence for the existence of relationships between PeD and cognitive function, and identified some neuropsychological items that were strongly associated with the presence of PeD. Specifically, visuospatial function, attention, word recall and recognition, and performance in the following commands task were associated with teeth-brushing and the presence of PeD. Social factors may also be associated with more severe PeD. Assessment of the relationships between PeD and dementia focusing on PeD bacillus should be conducted in future studies to determine the underlying mechanisms.
Conclusions
Cognitive decline such as visuospatial function, attention, word recall and recognition, and following commands task performance were strongly associated with the presence of PeD. These items can be assessed easily on a daily basis without measuring MMSE. Social factors may also be important to prevent worsening PeD.
Footnotes
ACKNOWLEDGMENTS
We thank Yukie Ohsaki, Hana Saito, Mieko Suzuki (NCGG) and Shiho Yunoue, Misaki Mugiyama, Kazumi Hosokubo, Minami Ido, Kaori Nohara, and Momo Shinmei at the Lion Foundation for Dental Health for their technical and secretarial assistance. We also thank the BioBank and NCGG for quality control of the clinical samples and data. Finally, we thank Benjamin Knight, MSc., from Edanz (![]() ) for editing a draft of this manuscript.
) for editing a draft of this manuscript.
FUNDING
This study was supported by JSPS KAKENHI (Grant Numbers: JP20K07861, JP20H03904, JP22K10011, JP23H03122), grants from the Research Funding of Longevity Sciences from the NCGG (19-24, 21-6, 22-23), the Lion Foundation for Dental Health, the Danone Institute of Japan Foundation, and the Honjo International Scholarship Foundation.
CONFLICT OF INTEREST
Dr. Saji received JSPS KAKENHI Grant Number JP20K07861, the Danone Institute of Japan Foundation, and the Honjo International Scholarship Foundation. Dr. Ishihara received JSPS KAKENHI Grant Number JP22K10011. Dr. Matsushita received JSPS KAKENHI Grant Numbers JP20H03904 and JP23H03122, and research grants from the Lion Foundation for Dental Health. Drs. Saji, Takeda, Sakurai, and Matsushita received research grants from the Research Funding of Longevity Sciences from the National Center for Geriatrics and Gerontology (19-24, 21-6, 22-23). Drs. Murotani and Uchiyama report no conflicts of interest related to this study. Dr. Saji is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.