
Abstract
Background:
In aging populations, more elderly patients are going to the intensive care unit (ICU) and surviving. However, the specific factors influencing the occurrence of post-intensive care syndrome in the elderly remain uncertain.
Objective:
To investigate the association between socioeconomic status (SES) and risk of developing dementia within two years following critical care.
Methods:
This study included participants from the Korean National Health Insurance Service Cohort Database who had not been diagnosed with dementia and had been hospitalized in the ICU from 2003 to 2019. Dementia was determined using specific diagnostic codes (G30, G31) and prescription of certain medications (rivastigmine, galantamine, memantine, or donepezil). SES was categorized into low (medical aid beneficiaries) and non-low (National Health Insurance) groups. Through a 1:3 propensity score matching based on sex, age, Charlson comorbidity index, and primary diagnosis, the study included 16,780 patients. We used Cox proportional hazard models to estimate adjusted hazard ratios (HR) of dementia.
Results:
Patients with low SES were higher risk of developing dementia within 2 years after receiving critical care than those who were in non-low SES (HR: 1.23, 95% CI: 1.04–1.46). Specifically, patients with low SES and those in the high-income group exhibited the highest incidence rates of developing dementia within two years after receiving critical care, with rates of 3.61 (95% CI: 3.13–4.17) for low SES and 2.58 (95% CI: 2.20–3.03) for high income, respectively.
Conclusions:
After discharge from critical care, compared to the non-low SES group, the low SES group was associated with an increased risk of developing dementia.
Keywords
INTRODUCTION
Post-intensive care syndrome (PICS) refers to the phenomenon that intensive care unit (ICU) survivors experience in the worsening of impairments in function, cognition, and mental health after critical illness [1–3]. Dementia occurs in approximately 4–62% of survivors after ICU discharge [4–7]. It reduces patient quality of life and results in tremendous societal healthcare costs and caregiving workforce needs [1, 9]. The number of patients who require critical care is increasing, and >80% of patients who receive ICU care survive [1, 10]. The number of patients who experience PICS such as dementia after discharge from ICU is expected to rise; therefore, we need to consider it as an important public healthissue.
PICS occurs more frequently in patients who are prescribed benzodiazepines, have worrying ICU memories, and have comorbid psychiatric illness [11]. In addition, old age, high disease severity, and delirium are risk factors for PICS [12, 13]. A meta-analysis showed that a prevalence of 25–44% for clinically important PTSD symptoms occurred at 1–6 months and 17–34% at 7–12 months after critical illness [11]. Declines in cognitive and physical function after critical care have been demonstrated as long as 6–8 years after hospital discharge [7, 15]. Despite the growing attention on determining the risk factors for PICS, few studies have examined equity in patient outcomes after critical care [16, 17].
Socioeconomic status (SES) is a strong influencing factor on individual health care utilization and health outcomes [18, 19]. In ICU survival, low SES has been associated with a 31% greater risk of 1-year mortality, and neighborhood disadvantage has been linked to an increase of 14% in disability burden [18, 19]. However, it is unknown whether patients with low economic status have a higher risk of developing dementia after being in ICU than patients who are not of low economic status.
Moreover, economic status has not been clearly reported as an risk factor of dementia onset, and there have been no consistent results regarding the relationship between economic status and dementia. Previous studies have frequently reported that lower SES is linked to a higher risk of dementia, later at the clinic, and with more advanced dementia [20–22]. However, other studies have reported that individuals with higher SES tend to receive referrals and diagnoses for medical conditions earlier than those with lower SES. This advantage can result in earlier access to treatment, which may delay symptomatic progression [23, 24].
Using nationally representative data for individuals with details of economic status and medical records, we aimed to evaluate whether socioeconomic status is associated with the risk of onset of dementia within 2 years of ICU hospitalization.
METHODS
This study used medical claims records from the Korean National Health Insurance (NHI) Service National Sample Cohort from 2003–2019. The National Health Insurance data (NHID), which included data on clinically determined International Classification of Disease, 10th revision (ICD-10) codes and socio-economic status, was a nationally representative random sample of approximately one million individuals from the Korean population [25]. All patients in the cohort were followed up unless they were excluded due to death or migration. As the NHID data are publicly available, anonymized, and de-identified, informed consent was waived by the Ethics Committee; the study was approved by the Institutional Review Board of Yonsei University’s Health System for academic research. It was conducted in accordance with the Declaration of Helsinki of 1975, as most recently amended.
Participants and design
We included participants who were admitted to a general or tertiary hospital for at least two or more days between 2003 and 2019. The exclusion criteria were as follows: 1) missing covariate values; 2) participants who had been diagnosed with dementia or had taken medication at least once for dementia before or during hospital admission; and 3) patients who were admitted to the ICU for only one day. This selection was made to minimize potential confounding factors on the outcome.
In South Korea, the National Health Insurance (NHI) program is a mandatory and comprehensive social insurance initiative that provides healthcare coverage to all citizens [26]. The government additionally administers a free medical assistance program, which offers healthcare benefits to economically disadvantaged families, including those who qualify through the National Basic Livelihood Security System [27]. Medical Assistance (MA) serves as an alternative for Koreans who cannot afford NHI premiums and closely resembles the Medicaid program in the United States. MA beneficiaries are not required to pay premiums and can access medical facilities either for free or at reduced medical expenses. Therefore, as in previous studies, we intend to use MA beneficiaries as proxy indicators for low SES groups [28, 29].
Low SES group comprised medical aid beneficiaries and non-low SES group was consisted of individuals in NHI. Because NHI premiums are determined based on income and property levels, our data provide that individuals of NHI premiums in the decile which can be used as a indirect indicator for income level for individuals of NHI. We investigate a subgroup analysis to assess the association between not only the type of insurance, but also the income level and the risk of dementia after critical care within 2-year. For this analysis, we divided the non-low SES group into four groups. The 1st to 2nd deciles were classified into the low-income group, the 3rd to 5th deciles were classified into the mid-low-income group, the 6th to 8th deciles were classified into the mid-high-income group, and the 9th to 10th deciles were classified into the high-income group.
The low SES group were then matched with the non-low SES group participants who were non-low SES group using propensity score matching. Propensity scores were calculated using sex, age, Charlson Comorbidity Index (CCI), primary discharge diagnosis from ICU admission and total days in the ICU. After measuring the propensity scores, 1:3 matching was performed using the OneToManyMTCH macro in SAS [30].
Outcome and variables
We defined dementia as an outcome variable in two ways. The first and second diagnoses were included in ICD-10 codes (G30 and G31). Second, in our data, all “F”-related ICD-10 codes are de-identified as vulnerable diseases, so only “F” can be identified. Therefore, we used a prescription of 1 or more medications for dementia (rivastigmine, galantamine, memantine, or donepezil) and the ICD-10 codes for (“F”) were defined as dementia [31, 32]. And to identify the risk of severe dementia, we evaluate a subgroup analysis of people who were prescribed memantine which used to treat dementia that was moderate to severe at the time of the first diagnosis [33, 34].
Independent variables included sociodemographic factors, socioeconomic status, health status, and treatment. Sociodemographic factors consisted of age (<39, 40–49, 50–59, 60–69, ≥70), sex (male or female), and region (metropolitan, city, or rural). Health status consisted of CCI (0–1, 2–3, 4–5 or ≥6). Medical utilization consisted of total days in the ICU divided into tertiles (2–3 days, 4–6 days, and 7 or more days), receiving at least one of three invasive treatments (mechanical ventilator care, renal replacement therapy, or central venous catheter) in the ICU (Yes or No), readmission to the ICU after hospital discharge (Yes or No), and primary discharge diagnosis from hospital (neurologic, oncologic, cardiovascular, respiratory, metabolic, etc.). And the types of hospitals providing ICU services were divided into three categories: tertiary hospitals, which offer advanced and specialized medical care; general hospitals, which have over 100 beds; and hospitals with more than 30 beds.
Statistical analysis
Chi-squared tests were used to determine significant differences in variables between participants who had dementia and those who did not. Statistical significance was set at p < 0.05. The propensity score was derived using logistic regression to calculate the probability of socioeconomic status according to sex, age, CCI, and primary discharge diagnosis. We calculated the incidence rate (IR) and incidence rate ratio (IRR) of dementia and the 95% CI with a generalized estimating equation using a Poisson distribution and expressed it as the incidence of dementia per 100,000 person-days. A Cox proportional hazards model was used to evaluate the association between socioeconomic status and incidence of dementia among participants who received critical care. For each participant, the index date was defined as the date of discharge from hospital, and the date of diagnosis of dementia or the date of prescription was defined as the final event date. We censored participants who died during follow-up or did not develop dementia. The results were reported as hazard ratios (HRs) and 95% confidence intervals (CIs) for the risk of dementia. Data were analyzed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
After applying the exclusion criteria, a total of 46,503 individuals remained. Subsequently, a 1:3 matching process was conducted, resulting in the selection of 4,195 individuals classified as the low SES group and 12,585 individuals classified as the non-low SES group (Fig. 1).
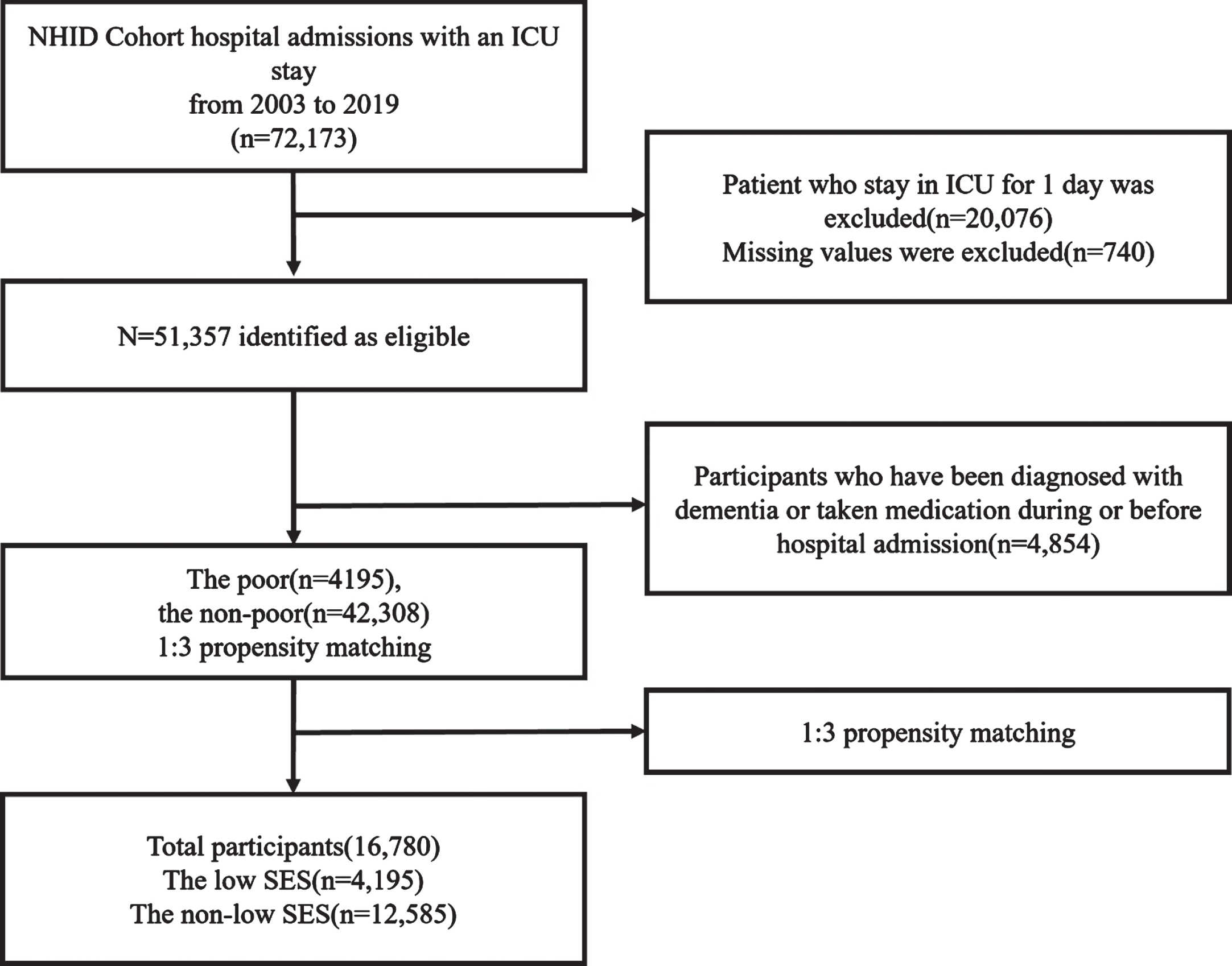
Flow chart of population selection.
Table 1 presents the general characteristics of the participants. Of the 16,780 participants included in our study, 621 (3.7%) developed dementia after being discharged from hospital. Among patients in low SES, 188 (4.5%) developed dementia. In addition, 433 (3.4%) patients who were in the non-low SES group developed dementia. There was a statistically significant difference in dementia development between the low SES and non-SES groups.
General characteristics of the baseline study population
Table 2 presents the findings of the IRR and Cox proportional hazard regression analysis for the association between socioeconomic status and the incidence of dementia within 2 years after ICU discharge. 188 of the patients with low SES developed dementia over 5,197,140 person-days (IR: 3.6 cases per 100,000 person-days). Patients with low SES were at higher risk of developing dementia within 2 years after receiving critical care than those who were in non-low SES group (HR: 1.23, 95% CI: 1.04–1.46). A longer stay in ICU was also a statistically significant factor affecting the risk of developing dementia; patients who stayed in ICU for >6 days were at higher risk than patients who were in ICU for 2–3 days (HR 1.43, CI 1.19–1.73). Also, patients with low SES did not exhibit a significantly higher risk of developing moderate to severe dementia within two years after receiving critical care, compared to those in the non-low SES group (HR: 1.01, 95% CI: 0.47–2.14, Supplementary Table 1).
Association between the socioeconomic status and the risk of dementia after critical care within 2 years
Kaplan–Meier survival curves showed that the risk of developing dementia among patients with low SES was higher than that in the non-low SES group (log-rank test, p < 0.001; Fig. 2).
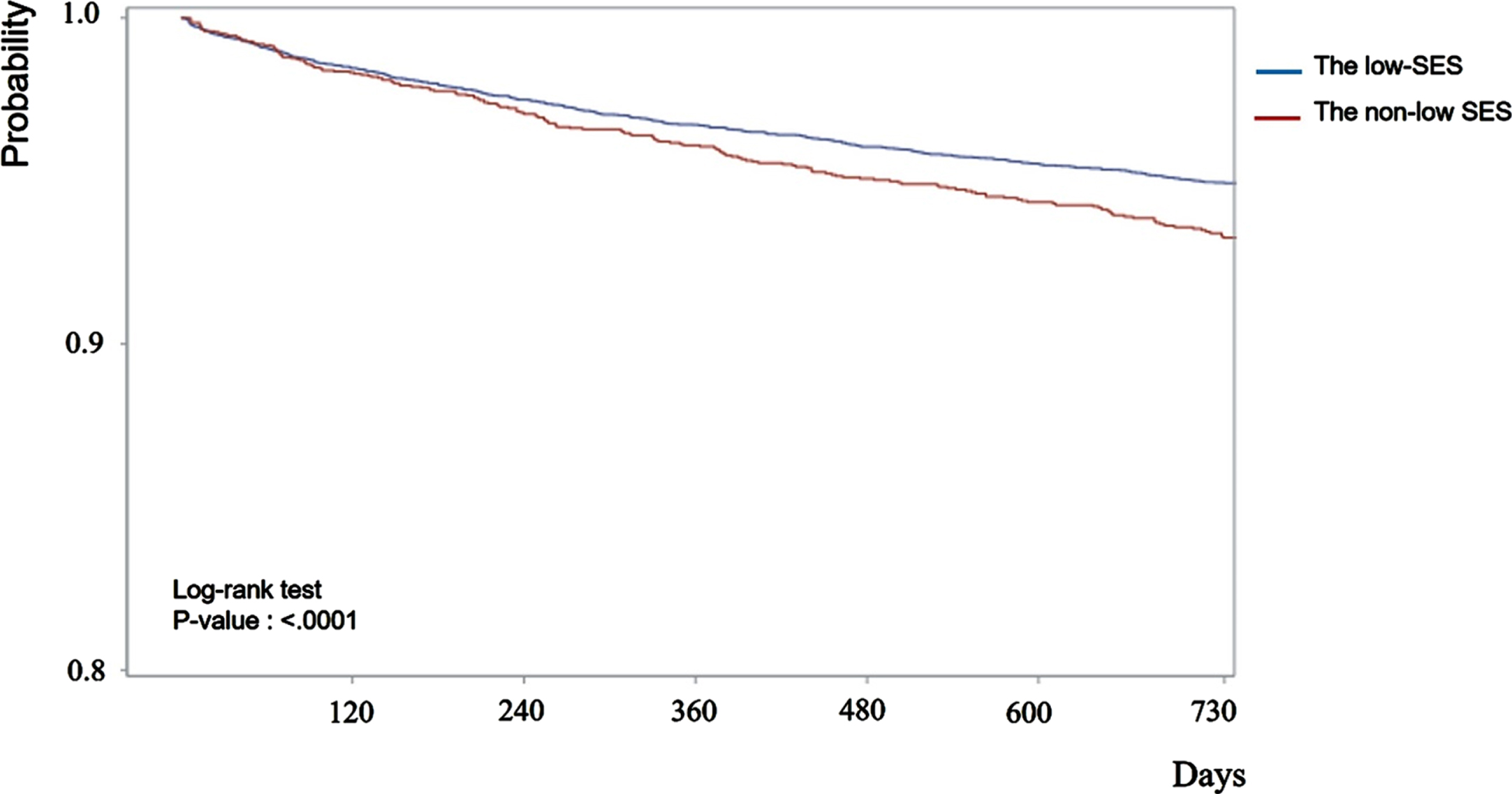
Kaplan-Meier survival curves for developing dementia after critical care within 2-year according to socioeconomic status of patients.
Figure 3 shows the incidence rate of dementia patients per 100,000 by subgroup to patients who were in low SES had the highest incidence rate of developing dementia (IR: 3.61, 95% CI: 3.13–4.17) and the high-income group also had high incidence rate of developing dementia (IR: 2.58, 95% CI: 2.20–3.03).
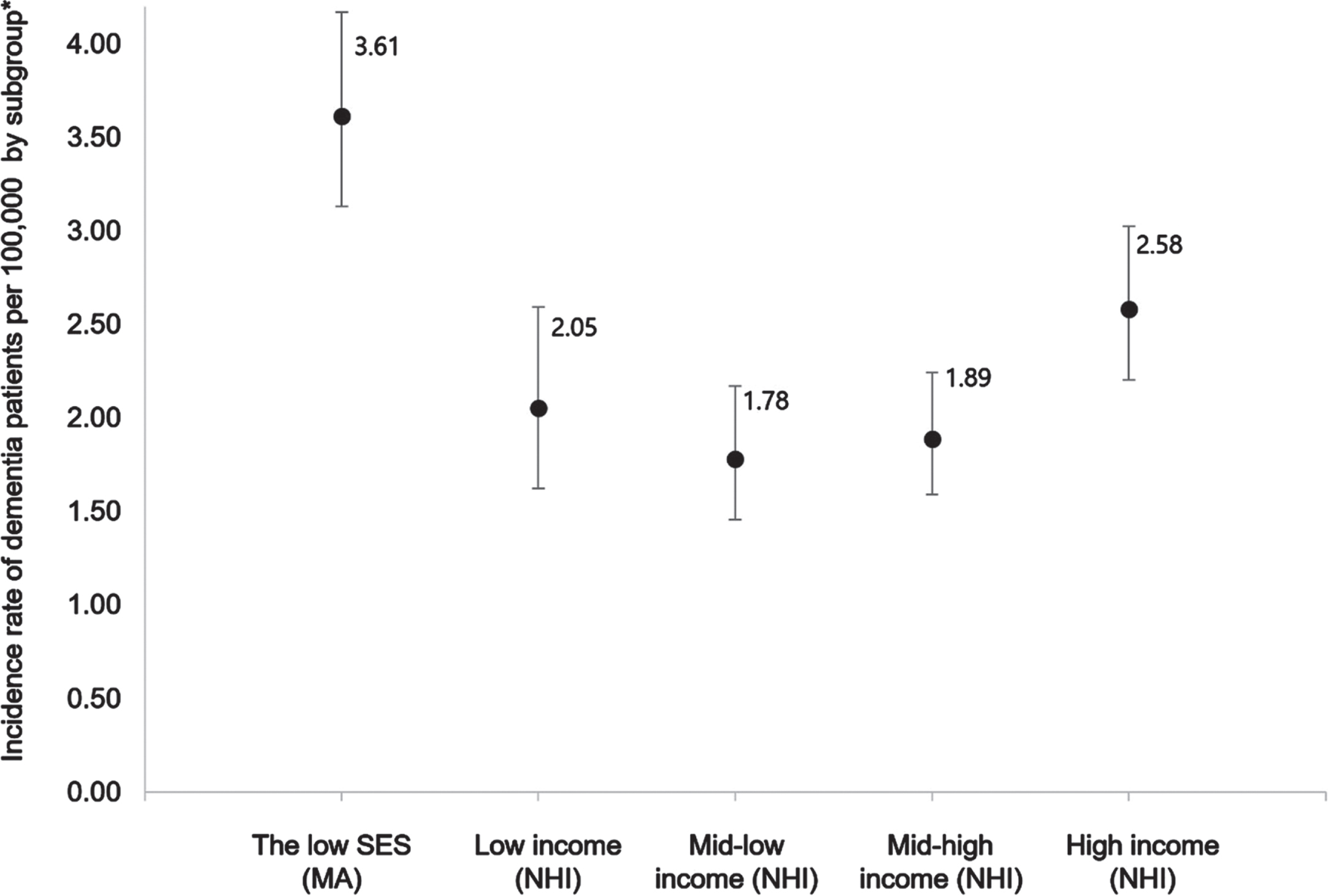
Incidence rate of dementia patients per 100,000 population stratified by income level.
Table 3 shows the results of the subgroup analysis assessing the impact of developing dementia within different periods after hospital discharge. Patients with low SES had a marginally significant higher risk of developing dementia within 18 months after being discharged from hospital (within 18 months, HR: 1.17, 95% CI: 0.97–1.41).
Association between the socioeconomic status and the risk of dementia by various periods
DISCUSSION
Our study investigated the effect of socioeconomic status on dementia development within 2 years after critical care, using national health insurance cohort data. Our results showed that the risk of developing dementia after critical care was higher for patient with low SES than for those who were not. Our finding that economic vulnerability might lead to impairment of cognitive function and dementia after ICU survival has meaningful implications for patients, families, and healthcare systems.
Lower SES is linked to higher ICU, in-hospital, 30-day, and long-term mortality [35, 36]. In addition, older adults receiving Medicaid and Medicare have a strong association with probable dementia in the United States [16]. Neighborhood socioeconomic disadvantage has a 9% higher risk of a higher disability burden after a critical illness following discharge from critical care compared with those in more advantaged areas [19]. Low SES reflects deprivation, which indicates a lack of resources or opportunities for healthcare utilization and poor access to health care. Additionally, those with low SES are more frequently exposed to adverse environments and have less knowledge of their health conditions. Our results suggest that a low SES may significantly contribute to the differential development of cognitive sequelae among survivors receiving critical care.
Our results showed an association between various income levels and risk of dementia development within 2 years of critical care. The association had an U-shape In a previous study, the rich tended to receive referrals and diagnoses for their medical conditions at an earlier stage than those with lower SES. As a result, the rich had the advantage of accessing earlier treatment, which potentially slowed down symptomatic progression [23]. In Korean national reports, both inpatient and outpatient centers were less medically utilized by patient with low SES s with dementia than rich patients with dementia [37].
For oncological and pulmonary diseases, ICU admission may have contributed to the observed socioeconomic differences in cognitive decline. These diseases are characterized by chronic conditions for which disease outcomes may be influenced by accessibility of healthcare and continuity of care, which are known to be worse for those with low SES [16, 39]. These results suggest that patients with certain diseases, especially those with low SES, should receive additional care or follow-up related to cognitive function and dementia after receiving critical care.
Many studies related to ICU syndrome have examined various sequelae, such as disability, weakness, physical impairment, and cognitive and psychosocial impairment. Discussions on when each sequela occurs after ICU discharge and for how long they persist are ongoing but there are no consistent results [1, 40–42]. Our results showed that the decline in cognitive function within one year of discharge from the ICU varies significantly according to SES status, and there is no difference in income status before six months. If patients receive long-term ICU treatment or have more comorbidities, the risk of dementia increases. In our study, our primary finding indicated the dementia risk associated with socioeconomic status during the post-ICU period. However, it is important to recognize that individuals with lower socioeconomic status can affect cognitive function irrespective of ICU admission. Establishing a definitive link between ICU admission and the onset of dementia is a complex issue. Nevertheless, in our research, we made efforts to address this concern by excluding individuals who had previously received dementia medication or a dementia diagnosis before their ICU admission.
This study has several limitations. First, we only considered dementia diagnosis in terms of ICD codes and drug prescriptions. Due to data limitations, we were unable to identify cases of mild and moderate cognitive impairment. However, a subgroup analysis was conducted to assess the impact of SES on the risk of severe dementia by using patients who were prescribed memantine, a medication typically used to treat moderate to severe dementia. Also, we excluded all patients with dementia at baseline. Second, since there was a data limitation regarding blinding-sensitive diseases such as delirium, we could not determine whether the patient experienced delirium during hospitalization. Further research is needed, because this may have affected our dependent variables. Third, the use of income status as a proxy for socioeconomic disadvantage in studies on health outcomes, including disability, is widespread. However, this approach does not distinguish between specific social and economic risk factors.
Conclusions
In summary, this study examined the association between socioeconomic status and the risk of developing dementia within 2 years of critical care. Our results showed that patients in socioeconomic status had a higher risk of developing dementia after critical care than those who were not. Our finding that economic vulnerability might lead to impairment of cognitive function and dementia after ICU survival has meaningful implications for patients, families, and healthcare systems.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the colleagues from the Department of Public Health, Graduate School of Yonsei University for advice on this manuscript.
FUNDING
This work was supported by the Technology innovation program (20024263, Development and validation of a digital phenotype based platform for the treatment and prevention of MCI using a multidisciplinary approach to decrease dementia risk) funded by the funded by the Ministry of Trade, Industry and Energy (MOTIE, Korea).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data that support the findings of this study are available from the National Health Insurance Sharing Service but restrictions apply to the availability of these data.