
Abstract
Background:
No systematic review on delirium prevention within early, hospital-based rehabilitation on implementation of approaches specifically tailored for patients with cognitive impairment (PwCI), such as Alzheimer’s disease or vascular dementia, has been published despite the high relevance of specific medical care in this vulnerable population.
Objective:
To document design and effectiveness of delirium prevention programs by early rehabilitation during acute, hospital-based medical care and implementation of programs specifically tailored to PwCI.
Methods:
In a three-step approach, we first identified published systematic reviews of hospital-based, early rehabilitation interventions for older persons (>65 years) in relevant databases. In a second step, we screened each single trial of included reviews according to predefined inclusion criteria. In a third step, we analyzed studies with focus on delirium prevention.
Results:
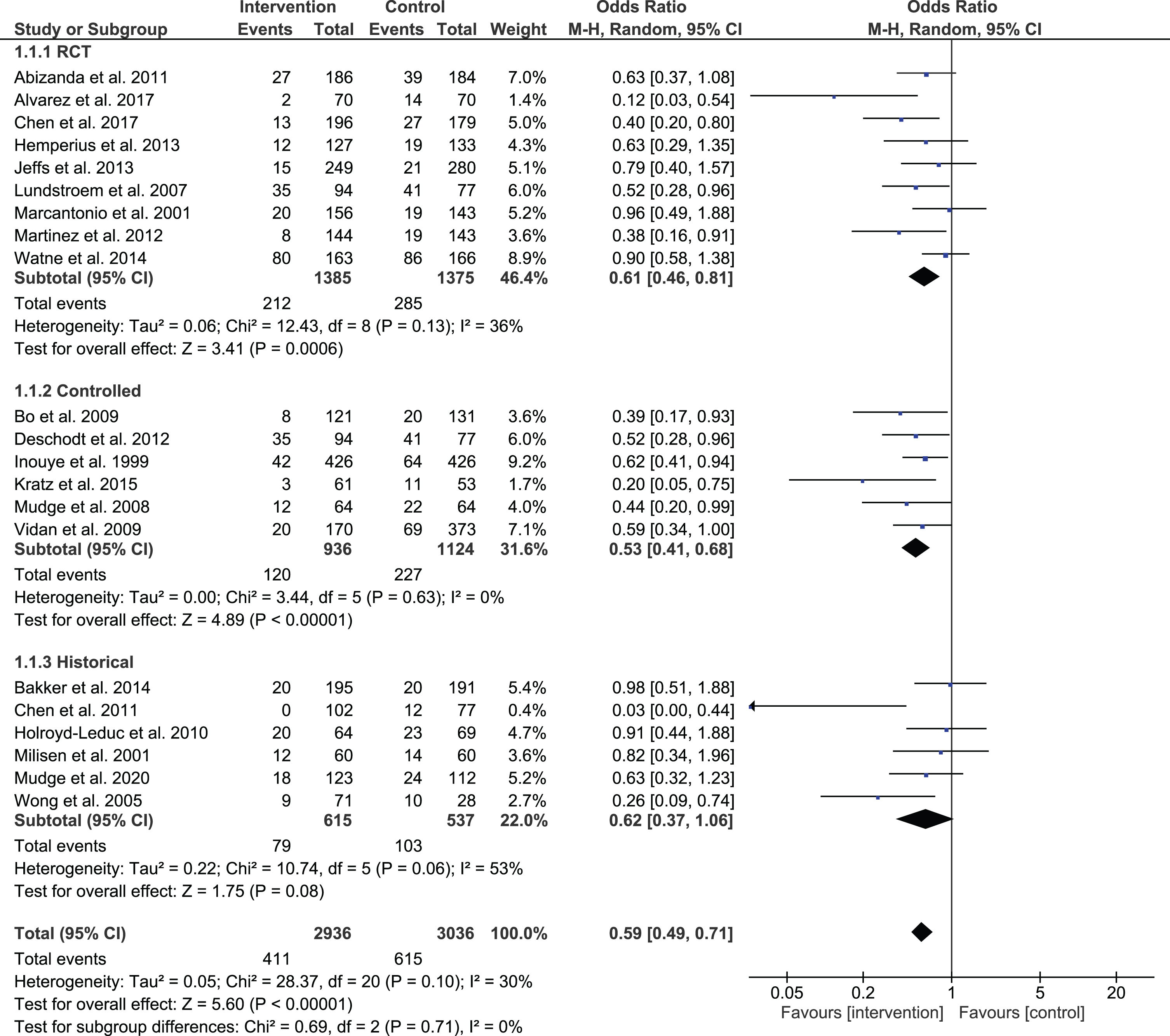
Among n = 25 studies identified, almost all intervention programs did not specifically target cognitive impairment (CI). Interventions were heterogeneous (modules: n = 2–19); almost all study samples were mixed/unspecified for cognitive status with more affected patients excluded. Only one study exclusively included delirium patients, and only one included CI patients. Results of random effect meta-analysis showed significant effects of generic programs to reduce delirium incidence during hospitalization by 41% (p < 0.001, odds ratio, 95% confidence interval: 0.59 [0.49, 0.71] with modest heterogeneity (I2: 30%).
Conclusions:
Study results document a lack of implementation for delirium prevention programs specifically tailored to PwCI by early, hospital-based rehabilitation. Specifying existing rehab concepts or augmenting them by CI-specific modules may help to develop, optimize, and implement innovative delirium prevention in PwCI in acute medical care.
Keywords
INTRODUCTION
Acute hospitalization in older persons (mean age > 65 years) is frequently associated with negative health outcomes. Acute medical illness causing admission, multiple chronic diseases, established frailty status, and factors associated with hospitalization itself lead to medical risks and adverse events such as incontinence, falls, malnutrition, and functional as well as cognitive decline during hospital stay [1–4]. Among older persons admitted to hospital, patients with cognitive impairment (PwCI) stand out as they represent a high risk group for multiple adverse outcomes even among other frail, older persons without cognitive impairment (CI) already representing a most vulnerable population. CI is frequent in hospitalized older persons with about 40% [5], or more than half of the inpatients aged over 85 years [6]. PwCI are more often admitted to hospital compared to patients without CI [7] and once hospitalized, they present with a high risk for in-hospital mortality, nursing home admission, long length of stay, falls, dehydration, reduced nutritional status, physical and cognitive decline, infections, and delirium [8].
Among adverse medical events, delirium— a state of acute confusion— ranks high as one of the most common complications for older inpatients, with about one-third of the general medical population over 70 years presenting with delirium at the beginning or during their hospital stay [9]. Depending on the setting, different occurrence rates have been described ranging from 8-50% in general or geriatric wards up to 82% incidence rates during intensive care [10–12]. The prevalence rates of delirium in PwCI, referred to as delirium superimposed on dementia (DSD), in hospital settings range from 12% [10, 13] to 41% [14]. Despite its frequent occurrence, delirium is often under-recognized [11], specifically in patients with advanced frailty [15]. The pathophysiology of delirium is not well understood; however, delirium is associated with significant cognitive and functional decline, psychological distress, and other negative outcomes including higher mortality, institutionalization rates, and costs [16–19], and seems to be more relevant for future cognitive decline than the hospitalization itself [20]. Additionally, CI and delirium mutually reinforce each other negatively [21, 22], while hospitalization itself (associated with change of location, etc.) triggers additional risks on the cognitive status [23–25]. Thus, the coexistence of CI and delirium further increases the risk for negative outcomes [26], such as increased mortality risk, risk of functional dependence, and institutionalization [27], and also complicates the situation during hospitalization due to relevant psycho-social effects and increased distress in affected persons, leading to higher burden for caregivers, and healthcare hospital staff [13, 29].
A number of systematic reviews have been published on prevention of delirium in older persons, indicating the feasibility and partly effectiveness of presented programs depending on setting, patient population, intervention, and assessment [30]. However, reviews focusing on persons with pre-diagnosed or previously existing CI are scarce, as these persons have frequently been excluded in clinical studies [31], and those reviews in persons with CI [32–34] did not specifically focus on delirium prevention as part of early rehabilitation during hospitalization, or did not identify appropriate studies [35]. It remains unclear whether the obvious need for programs specifically tailored for PwCI in this setting has been met by adequate implementation programs.
Within the framework of a systematic review on early rehabilitation interventions for PwCI (protocol registered at INPLASY; 202210006 [36]), which aims to assess the grade of implementation of CI-specific or CI-appropriate methods, we identified delirium prevention as a crucial domain with both delirium and dementia representing a status of impaired cognition with distinct, complex, and interconnected relationships and multiple effects on other health parameters and medical treatment/rehabilitation. Therefore, in addition to the overview review results, we focused on the aspect of delirium prevention specified for hospitalized PwCI in an in-depth analysis. The study objective of the present study was to document design and effectiveness of delirium prevention programs during early rehabilitation during acute, hospital-based medical care and implementation of programs specifically tailored to PwCI.
MATERIALS AND METHODS
The present scoping review is part of a larger data analysis covering early, hospital-based rehabilitation on a broader scale. In the present scoping review we targeted delirium prevention programs with focus on implementation for patients with chronic CI.
Two review authors worked independently to assess systematic reviews, respectively single studies, for eligibility and to extract data documented in standard data entry forms. In case of disagreement, a third researcher supported decision for final inclusion.
In a 3-step approach, the first step represents an umbrella review to identify relevant already published systematic reviews of hospital-based, early rehabilitation interventions for older persons. Relevant databases including Medline, CINAHL, PsycInfo, Web of Science, and Cochrane Library were searched from inception to September 2022. Search terms were adjusted for each database (for search terms, see Supplementary Material). Additional searches were performed for reference lists of existing systematic reviews and for studies conducted by experts in the field/trial authors to identify appropriate unidentified systematic reviews. Systematic reviews were considered for further analyses if they included controlled studies on hospital-based, early rehabilitation interventions, conducted during acute hospitalization in older persons with a mean age of > 65 years. Trials reporting on different or mixed settings without a clear focus on hospital-based early rehabilitation, or studies not published in English language were excluded.
In a second step, we screened each individual study of all included reviews according to predefined inclusion criteria similar to criteria mentioned above for identification of reviews: controlled study design, mean age of study population > 65 years reporting on an early rehabilitation during hospitalization, inclusion of functional assessment- and/or intervention modules. Studies performed in different or mixed settings, or without a focus on hospital-based, early rehabilitation, or data analysis not covering hospital stay, were excluded.
As the third step, for the present review only individual studies with a clear focus on delirium prevention using a multi-modular intervention but without an exclusive medical or pharmacological approach were included. The delirium studies identified by the search and reference lists of included articles were hierarchically evaluated for CI specific features including: 1) reference to CI/delirium in title or objective, 2) general sample description and selection with reference to cognitive status, 3) CI/delirium-specific cognitive assessment and other main outcome measures for primary and secondary outcomes, 4) analysis of comprehensive intervention programs or single program modules (individual parts of the program) and their match for persons with CI/delirium, 5) analysis of general effects of intervention and effects with respect to cognitive status/delirium including sub-analyses according to cognitive status representing relevant prerequisites respectively mandatory features for CI-specific programs, and effectiveness of programs with respect to delirium prevention/reduction. Random-effects meta-analysis was conducted to test for effects of interventions on delirium incidence using Review Manager (version 4.3, The Cochrane Collaboration) to calculate pooled Odds Ratio (ORs) and 95% confidence intervals (CIs). Pooled results were presented as forest plots. Subgroup analysis was performed based on the study design (randomized-controlled, non-randomized with simultaneous control, non-randomized with historical control) for studies reporting effect on delirium incidence during hospitalization. Heterogeneity was assessed using I2 statistics, with values considered low for I2 < 25%, modest for 25–50%, and large for > 50% [37]. For a sensitivity analysis of effect of CI in the mixed or unspecified samples, we classified included studies for prevalence of CI in low versus moderate status according to established cut offs for means of applied screening tests (Mini-Mental State Examination (MMSE > 24 scores), Short Portable Mental Status Questionnaire (PMSQ > 4 scores)) or a 20% prevalence of CI, in case no results of cognitive screening were presented.
RESULTS
Literature search
Among the 322 articles identified in the basic search in published systematic reviews, we finally selected 25 studies for the analysis on delirium prevention (see Fig. 1). The classification as a delirium prevention study (n = 17) partly contrasted with competing main outcomes in mixed domain studies including also functional or other interventions (n = 8). Almost all (n = 21) included articles mentioned delirium/CI in their study title and/or objective and all included studies had delirium as a major study outcome justifying the classification as delirium studies. All studies included assessment of functional status and most studies (n = 23) described functional training/early rehabilitation as program modules of intervention, while two provided unspecific information in this respect. Details of the description of studies are provided in Table 1. For detailed results, a comprehensive summary for individual studies is given in Supplementary Table 1.
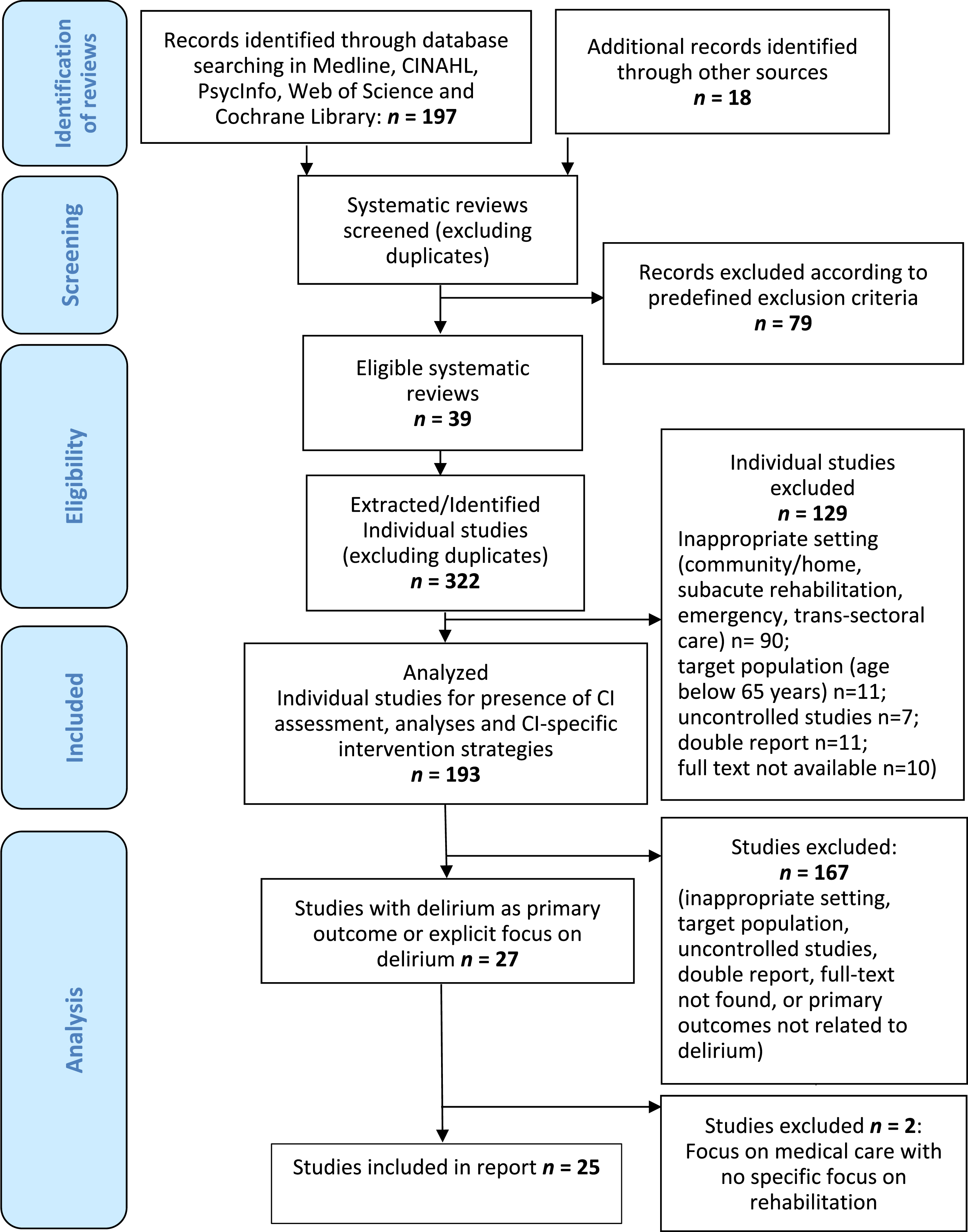
Flowchart of the literature search / Inclusion of articles.
Basic information and description of included studies
1during hospitalization; ADL, Activities of daily living; AMT, Abbreviated Mental Test; BADL, Basic activities of daily living; CG, control group; CGA, comprehensive geriatric assessment; CI, Cognitive impairment; excl., excluded; HELP, Hospital Elder Life Program; IG, Intervention group; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; PwCI, people with cognitive impairment; PwD, people with dementia; RCT, randomized controlled trial; SPMSQ, Short Portable Mental Status Questionnaire; vs., versus.
Settings/study design
Studies were conducted in different settings including general medical-, geriatric/oncologic/orthopedic or surgery hospitals or comparisons were made between such settings and associated differences in specialized treatment with a focus on hospital-based, acute medical care. Ten studies were designed as randomized or cluster randomized controlled trials, nine as non-randomized, controlled trials with a simultaneous control group, and six as controlled trials with a pre-post design comparing acute interventions with historical controls of the same setting.
General sample description
All study samples included multi-morbid, older patients (mean age 79.1 years, range: 69.5-84.7 years) representing mostly mixed populations with respect to admission diagnosis, while in some studies, specific populations such as surgery/orthopedic/oncologic patients were included, related to the primary hospital setting and objective of hospital treatment.
Inclusion of PwCI
There was large heterogeneity in prevalence at admission for CI, which was only reported in 15 studies (27.3%; range: 0–100.0%). Partly, only mean values for cognitive assessment were presented, not allowing for classification of patients with and without CI. CI or dementia diagnoses were partly merely mentioned in tables or text and the related assessment was not described. For those studies reporting no baseline CI prevalence (n = 10), but mean values for cognitive screening, higher MMSE scores (n = 8; mean score 25.5) and moderate SPMSQ scores, (n = 2, mean score 4.1 scores) indicated low to zero prevalence or low level of CI in these studies. Two studies did not report cognitive status at all. Six studies excluded patients with severe CI (unspecified), one study excluded patients “with disorientation in time and locus”, and one study included patients with MMSE scores > 24 indicating patients with intact cognitive status. Only one study exclusively focused on patients with CI/dementia.
Inclusion of patients with delirium
Delirium incidence during hospitalization was reported in 22 studies (21.7%; range 7.6–45.2%). Six studies excluded patients with preexisting delirium, one study with severe delirium. Only nine studies reported baseline delirium prevalence (mean 26.6%, range 23.9–33.2%) representing a subsample of studies with higher risk for delirium (also associated by higher incident delirium). Only one study exclusively included patients with preexisting delirium.
Delirium assessment
Various delirium-related outcomes were assessed such as delirium severity-, duration-, number of episodes, number of days with delirium, cumulative proportion of sustained improvements in delirium symptoms, recurrence, prevalence of acute pre-existing delirium, history of delirium, or ongoing delirium pre/post hospitalization with cumulative delirium incidence as used in all but four studies. Delirium status was based on established screening instruments such as: Confusion Assessment Method (CAM), Delirium Rating Scale (DRS), Delirium Symptom Interview (DSI), Memorial Delirium Assessment Scale (MDAS) (severity), Delirium Observation Scale (DOS), Organic Brain Syndrome Scale (OBS), Delirium Index (DI) based on CAM, NEECHAM Confusion Scale, with the CAM as the most often used outcome for other delirium outcomes including duration, frequency, and severity of delirium during intervention. Except for one study, different types of delirium (hyperactive/hypoactive/mixed) were not documented [38]. Screening results were partly backed up by an expert diagnosis according to established diagnostic guidelines such as Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM IV). Delirium was assessed in all included studies as a main outcome criterion, while frequency of delirium assessment varied from daily assessment to two pre-post measures repeated at specified intervals, or was not specified for frequency of assessments.
Assessment of cognitive status
Cognitive status was documented in 22 studies at baseline, but only in n = 8 studies as an outcome measure for the intervention. Assessment of CI was performed by different assessment methods and included: MMSE, 12-item MMSE, SPMSQ, Functional Independence Measure (FIM, sub-score cognitive items), Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE), Clock Drawing Test, Modified Blessed Dementia Rating Scale (MBDRS), Blessed Dementia Rating Scale (BDRS), Digit Span Test, Consortium to Establish a Registry for Alzheimer’s disease battery (CERAD), MINI-Cog, AD8 informant review, Informant Questionnaire on cognitive Decline in the elderly (IQ-Code), Abbreviated Mental Test (AMT), with the MMSE as the most often used measure. Partly, classification of CI was specified as “dementia” indicating a formal dementia diagnosis rather than a screening result for CI, in a few cases backed up by expert rating or based on established guidelines. In some studies, dementia was merely reported in descriptive tables or documented from patient charts without further description. Cognitive status was partially used for descriptive or predictive purpose in result documentation. Applied cognitive assessments represented established and validated methods, although alternative assessments for more advanced stages of cognitive impairment/delirium were not specifically addressed. Specific training for CI, especially delirium assessment, were partly mentioned but with restricted information on the training and experience of assessors. Only one study gave a comprehensive description of parallel assessment of CI and delirium with daily evaluations during the interventions and specified proceedings to differentiate between transient (delirium) and chronic CI [38].
Descriptive and other outcome assessment
A comprehensive basic assessment was partly specified as a separate module/part of the study proceedings (in geriatric settings stated as Comprehensive Geriatric Assessment, CGA), and was documented in n = 7 studies. In other studies (n = 16) such a comprehensive assessment has been provided as basics, in n = 2 studies with unclear description. Variables documented by such comprehensive assessments were used for sample descriptions or for lists of clinical or other study outcomes representing surrogate/secondary markers for effects of interventions. Specific approaches/training to assess persons with CI or the validity of (non-cognitive) assessments for persons with CI/delirium especially for severe forms was not or not stated in detail.
Intervention programs
All study interventions consisted of multimodal programs targeting delirium as a main study outcome also including a functional intervention module or functional outcomes. Intervention modules were extraordinary heterogeneous by number of modules (mean: n = 6.5; range 2–19) and domains including a wide variety of different interventions with some of the studies rather listing targets of interventions than specifying separate or well-described sub-interventions. The module description differed substantially with respect to comprehensiveness and clarity of interventions. Descriptions were partly mixed with objectives, assessments, and therapy option with no standardized phrasing for comparable content.
Seven studies focused on “risk factors” for delirium respectively general health status, with the HELP study by Inoyue et al. [52] representing an explicit model or reference for a number of subsequent studies, including intervention modules with focus on: cognitive impairment, sleep deprivation, immobility, visual impairment, hearing impairment, and dehydration [42, 53], or an abbreviated HELP version by three main modules: orienting communication/cognitive stimulation, oral/ nutritional assistance, early mobilization [41, 57]. Other studies used identical or similar/related modules (partly rephrased, modified or amended) such as: ADL training, cognitive stimulation/reality orientation, poly-sensory stimulation, environmental stimuli, positioning, stimulation of upper extremity motor function, graduated exercise or staff/lay person training, environmental changes, policy evaluation, motivation. Most other studies (n = 16) included modules of mixed intervention strategies. Modules addressing either specific medical risks/symptoms or adverse events during hospitalization were included in nine studies, including issues such as: prevention of medical complications, pneumonia, anemia, infection, embolism, bowel/bladder function, sleep/apnea, ulcers, pain, oxygen saturation, body temperature, medication use, partly further specified as medication review for psychoactive drugs, administration of atypical antipsychotics for hyperactive/psychotic symptoms, reduction of polypharmacy, adverse drug interaction, calcium/vitamin D provision, fluid/electrolyte balance, different specific laboratory-based measures, respiratory care with only few modules exclusively focusing on delirium or CI with cholinesterase inhibitors for sustained CI, screening for treatable causes of dementia, and treatment of psychiatric symptoms/agitated delirium.
About half of studies (n = 12) also had a focus on staff and lay persons, partly documented as fixed intervention modules or accompanying description related to training/knowledge transfer, change of attitude/awareness and inclusion in interventions/interaction to patients with modules on: Instruction of family members for geriatric syndromes and delirium prevention, interdisciplinary consultation and co-management with focus on delirium/cognition delivered by multidisciplinary work group, family participation, education of family members, avoidance of sensory deprivation, presence of familiar objects in the room, reorientation of patient provided by family members, extended visitation times, staff/family/patient education, partnership in care planning, education of multidisciplinary team including staff, patients, and caregivers to actively encourage mobility and functional independence, educational program to change approach of geriatric ward staff for patient care, proactive and intensive support by geriatrics team to improve patient-centered care to increase staff awareness and competency by ongoing education and introduction of trained volunteers for integration of care and well–being-directed activities, and programs on quality improvement methods. Very few modules explicitly reported specific, standardized communication and interaction strategies with CI/delirium patients as in Kratz et al. [53] with validation strategies according to Feil [62], while other studies [41, 47] included orienting communication as intervention modules. Only one intervention program presented with a socio-ecological, theory based model including: environmental and policy assessment; staff education; individualized family-centered, function-focused care (FAM-FFC) goals and mentoring and motivating nursing staff and patients [48], which was further adjusted to PwCI [49].
Nine studies included lay persons (family members (n = 6), trained volunteers/psychology students (n = 3)) in different levels of implementation. Other modules targeted organizational issues such environmental assessment/modification, advanced care planning, discharge planning or interdisciplinary interaction. One study did not report clear modules apart from general proceedings and could not be classified with respect to suggested intervention strategies [50].
Specifications for patients with CI/delirium
Surprisingly, only in two single studies, modules were consistently specified/tailored for persons with CI [49] or delirium [45], respectively. Few studies reported CI as a separate module [52], while in others intervention approaches not further specified for CI such as cognitive orientation or training [38–40, 55] were stated and very few single modules were highly specific by medical criteria for persons with CI/delirium (e.g., treatment of agitated delirium, cholinesterase inhibitors) [9, 61].
Operationalization of modules
For the majority of modules identified within multimodal interventions, no comprehensive operationalization was given as a prerequisite to quantify adherence and effectiveness of individual program modules. Modules were partly described for content, partly also for responsible staff. Only in two studies [52, 57] an operationalization with matching corresponding assessment clearly allocated to a module was provided and analyzed for effects. Operationalization of modules partly overlapped with study outcome measures/endpoints used in some studies to document effects of interventions for generalizing clinical/organizational or other effects [42, 55]. Modules on organization or staff/lay persons training/education were often not operationalized and often targeted knowledge transfer, less frequently attitudes towards or communication/ interaction with patients which are less easy to be quantified while specific other modules including medical parameters can assumed to have been operationalized following established medical guidelines for clinical routines.
Staff training
Staff training partly also including proxy or lay person programs was often not further specified or described in detail for a CI specific perspective. Sixteen programs were provided by professional staff, partly with specific training for study purpose but without a specifically documented comprehensive CI specific training, while six programs were delivered by professionals with different levels of training, and three programs were provided by volunteers with limited specific training while offering relevant potential strategies such as “change of attitude/awareness; interaction/ communication to patients, inclusion of familiar persons in interventions”. Most often a knowledge transfer for delirium /CI was reported as a specific training topic for professional staff and lay persons.
Usual care/control
The control group activity was defined by setting (e.g., geriatric versus orthopedic ward) or quality/quantity of standard routine care. However, descriptions were mostly very brief, not always clearly allowing to distinguish between intervention and usual care, with one study [40] presenting more comprehensive information on level of preexisting delirium prevention/care. As with intervention modules, the general level of staff training for such programs including knowledge on CI/delirium, specific training for communication, patient-staff interaction, treatment and assessment of PwCI/delirium was not specifically reported, limiting the benchmarking for newly implemented programs against usual care.
Effects of intervention
Results of the meta-analysis for the total of studies including studies that reported delirium incidence (n = 21 studies, n = 5,972 participants; 1,026 events/cases of incident delirium) indicated significant effects to reduce delirium incidence during hospitalization by 41% (p < 0.001, odds ratio (OR), 95% confidence interval: 0.59 (0.49, 0.71) with modest heterogeneity (I2: 30%). Results were confirmed for sub-analysis according to study design for randomized controlled trial studies for controlled trails with simultaneous interventions, and also for studies with historical pre-post controls, however, only with a trend for significance and larger heterogeneity. Overall, 13 studies out of 21 achieved a significant reduction of delirium incidence. Among the studies with a negative result for delirium incidence (n = 8), 3 studies achieved a positive result in another delirium related outcome such as delirium severity or duration of delirium. For delirium severity as the delirium parameter most frequently used apart from incidence, five out of nine studies reported significant effects. Single positive results could be achieved for duration and density of delirium, number of episodes, and number of patients discharged with delirium.
Among the four studies which did not assess delirium incidence, three studies achieved a significant reduction in delirium severity [45, 49], while for other delirium outcomes (number of days with delirium, proportion of sustained improvements in symptoms) no significant effect was documented. One study did not achieve a significant reduction in the documented delirium related outcome (number of delirium episodes) [51]. Adverse effects were in most studies not explicitly mentioned. The few studies which did, reported that no adverse events occurred [39, 51].
To test for impact of CI, we performed a sensitivity analysis according to predefined criteria irrespective of the study design for two categories of low versus moderate CI status. The definition of subgroups were further supported by data given in articles for delirium incidence during hospitalization, which was doubled in the subgroup with moderate CI (meta-analysis group lo CI: 11.5% versus moderate group: 24.6%) indicating distinct subgroups for analyses. Both subgroups presented with a significant reduction of delirium incidence during hospitalization with a low to modest heterogeneity (Low CI (n = 12, n = 3,005 participants, n = 346 events): p < 0.001; I2: 40%); moderate CI; n = 8; n = 2,834 participants; n = 637 events; p < 0.001; I2:7%). Effects were more pronounced in the group with low CI prevalence (Low CI: OR: 0.50 (0.36, 0.70) versus moderate CI: OR: 0.64 (0.52, 0.79)). Based on analysis of individual results in studies independent from meta-analysis, relative delirium incidence in general was higher in the subgroup with moderate CI (low CI: 11.3% versus moderate CI: 24.6%). As most studies included patients with no or low to moderate CI or delirium status, data on more affected patient groups could therefore not be included.
Effects of interventions on incidence delirium according to cognitive status.
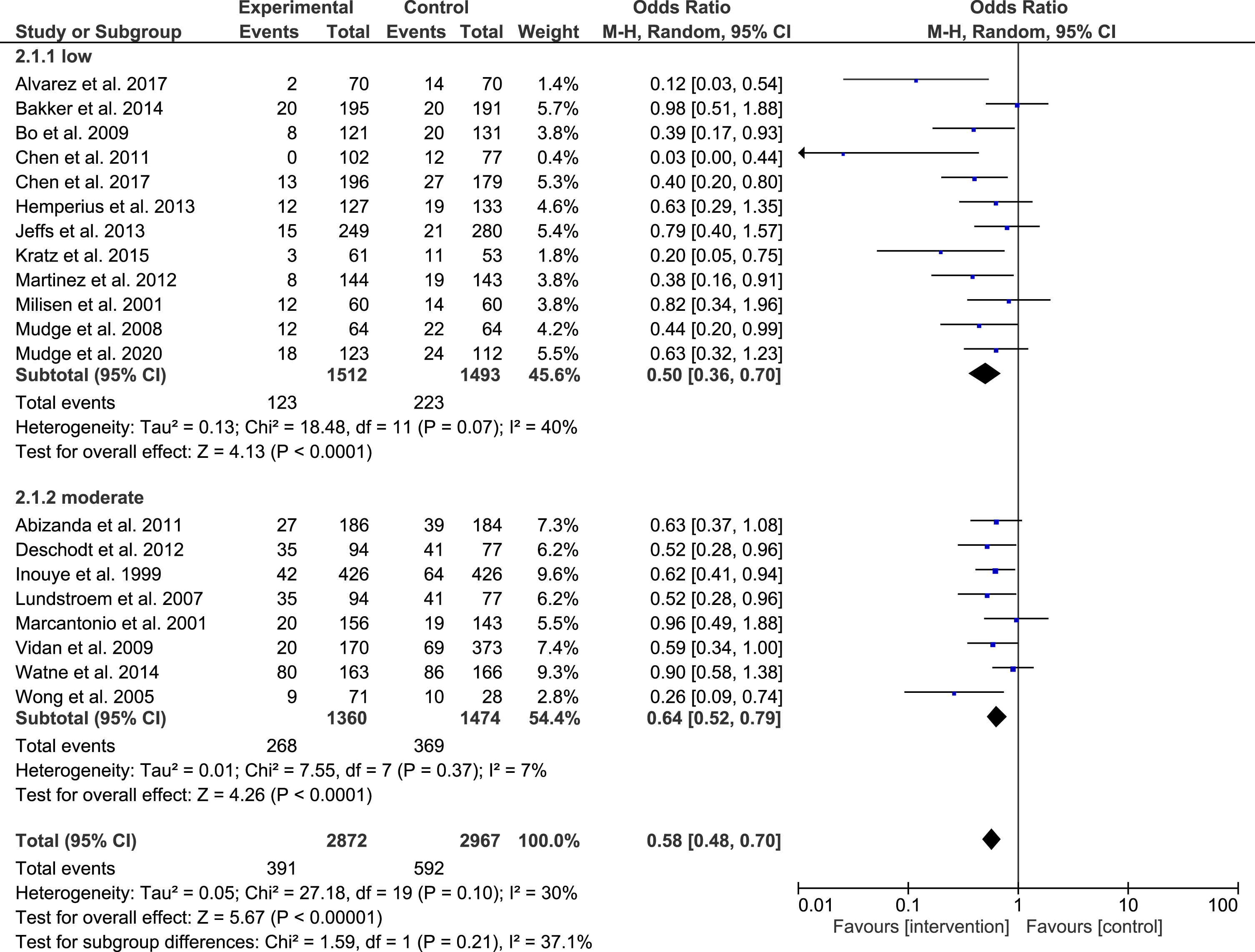
Effect of intervention according to cognitive status.
Sub-analyses for effectivity of modules
Effects of interventions were mostly given for the “package of modules” not further specified for effects of individual modules. Only in 13 studies at least basic information on adherence to/provision/implementation of program modules were reported. Operationalization and adequate assessment with a between group comparison for effects of intervention on individual program modules were only reported in two studies [52, 57], while in four studies effect of intervention on clinical, functional, cognitive, or organizational markers/indicators were analyzed for between group differences during intervention [42, 55]. However, these “markers” could not always be clearly attributed to intervention modules. Adherence/implementation rates differed largely depending on the generic versus specific nature of the module respectively setting, sample, and program with large differences even within single programs with provision of modules ranging from 0 to 100% (e.g., [40]). Adherence rates were partly not compared to routine/usual care. None of the studies used results of effects on individual modules to analyze their impact on the main study outcomes on delirium.
Sub-analyses according to cognitive status
Although most included studies were based on mixed or unspecified samples with respect to cognitive status or delirium, in only eight studies a sub-analysis according to cognitive status was performed, while 17 study authors did not. Design and objective for these sub-analyses were extraordinary heterogeneous and not always related to the study objective to evaluate effects of intervention programs on delirium or other main study outcomes. For sub-analyses, no separate sample calculations were mentioned.
Most often the association of CI on risk for delirium was analyzed and confirmed [9, 55]. For the two studies reporting on effects of CI on delirium prevention, heterogeneous results were documented. While one study found effects of delirium prevention with a lower prevalence of post-op delirium achieved also in PwCI [44], another studies reported no benefit of delirium intervention respectively a high delirium risk regardless of intervention in PwCI and loss of significant study results for delirium prevention when adjusted for cognitive status [9]. Two studies [52, 55] analyzed effects of their intervention according to delirium severity/risk indicating significant effects in moderate but not in high-risk group for incident delirium.
DISCUSSION
The present scoping review aimed to identify programs specific for PwCI to prevent or reduce delirium during early acute hospital-based rehabilitation. Within the framework of a large scoping review on implementation of CI-specific programs during early rehabilitation, we conducted an in-depth analysis of all studies with delirium as a primary/main outcome, study objective and/or related interventions. Early, hospital-based rehabilitation has primarily been introduced with the focus to stabilize respectively regain functional status. In the context of comprehensive medical care during hospitalization with the goal to restore general health status and prevent adverse events, early rehabilitation and prevention will include further health domains apart from functional status targeting also cognitive domains comprising persistent as well as transient CI. In this scoping review, we identified numerous studies targeting delirium prevention using multimodal intervention programs which represent the most efficient study type setting [63, 64] well fitting into the hospital-based, early rehabilitation setting.
However, despite the fact that all studies have an inherent focus on delirium, representing a transient form of CI, except for one study, all other studies did not report programs which were explicitly developed for PwCI or patients with delirium. Generic interventions were applicable and partly effective in mixed study populations including PwCI/delirium, and some of the studies were performed in samples with higher prevalence of CI/delirium, limited specifications for CI were documented, not targeting a large, most vulnerable subpopulation among older, multimorbid, in-hospital patients. In our understanding, the presence of CI will be associated with crucial consequences for study organization, sampling, assessment, interventional strategies, and data analysis of effects of delirium prevention/treatment interventions clearly calling for a modification and specification of programs with respect to the restricted abilities but also the remaining resources of PwCI. Most obvious was the lack of programs targeting patients with more advanced stages of CI, delirium, or co-existent DSD, that request even more specific methodology tailored for this vulnerable population.
Sample description and inclusion of patients with delirium and/or CI
Illustrated by the infrequent reporting of baseline rates for delirium, the on average low prevalence of pre-existing delirium/CI, and the exclusion of pre-existing delirium/CI in some studies, most interventions aimed at primary prevention of delirium, however, including mixed samples with respect to ongoing versus newly developed delirium. This patient selection led to an underrepresentation/exclusion of patients with pre-existing delirium/CI in identified articles, which has also been described in a recent reviews on delirium prevention for different contexts and settings [30, 31] and was most obvious for most affected patients at highest risk for adverse events and with limited ability to adhere to generic interventions not adjusted to this vulnerable sample.
Assessments
Applied cognitive and delirium assessments showed a large heterogeneity but represented basically established and validated methods with some methodological limitations for outcome reports. Assessment methods such as the CAM, as the most established for delirium documentation, critically depend on training of assessors, which was not sufficiently specified in most included studies. Validity of the CAM is severely reduced when assessed by non-trained persons [65, 66], especially so for more affected persons with impaired communication [67, 68]. In only very few of the identified articles different delirium severity staging strategies [52, 59] were documented. However, such a staging would also have a potential for the implementation of CI specific programs, as severity of delirium will have a relevant impact on the feasibility and effectiveness of interventions. However, in this review, no such graded interventions were identified using severity of delirium as a criterion for an individualized, tailored intervention. Only one study presented data on type of delirium. The lack of focus on different delirium types [69] implies a high risk of non-detection of hypoactive delirium, with potential exclusion of affected patients despite their high risk for worse outcomes [70], while difficulties with specific psychiatric symptoms in hyperactive delirium may request specific interventions which might both have relevant consequences for delirium programs [71].
Additionally, limitations of established CI screening methods as used in included articles such as MMSE to detect milder forms of CI, and both the MMSE and the Montreal Cognitive Assessment to detect and correctly rate severe forms of CI, have been discussed in the literature [72–74]. Use of such screening tools imply a relevant limitation in the context of inclusion of underrepresented groups such as severely affected patients or a clear stratification for persons with and without CI. Alternative assessments for more advanced stages of cognitive impairment were not specifically addressed in method descriptions of included studies, which is in line with the selective inclusion of non to mildly impaired patients in most studies. An ongoing, parallel assessment of delirium and cognitive status was not reported in most included studies, as the method of choice for differentiation between transient and chronic CI or DSD assessment during interventions [75, 76] including also assessments such as the IQCODE [77], which allows the documentation of history of CI before admission. Such methodological restrictions are relevant as the valid documentation of CI status represents a mandatory prerequisite for analysis of outcomes according to cognitive status and the development of CI specific interventions. Unfortunately a global consensus on assessment on DSD is lacking [78].
Apart from the CI/delirium specific assessments, in line with previous reviews in specific patient groups [79], comprehensive basic/geriatric assessment to recognize medical, social, neuropsychological, nutritional, and environmental conditions were reported in most studies, which is requested to detect individual needs to further individualize specific intervention modules. Results of comprehensive (geriatric) assessment represent the basis of medical modules as well as generic risk factors such as cognitive or functional status as part of most programs [79]. However, the suitability respectively validity of CGA or parts of the CGA in persons with more severe cognitive impairment remains unclear, as for example discussed for assessment of mobility [80, 81], depression [82], or pain [83, 84], or cognition as stated above. This may be less relevant for the majority of the included studies in non- to mildly impaired persons, but will be important for future studies in more affected populations.
For the evaluation of effects of intervention on the module level, a well-matched assessment strategy for single modules would also be mandatory (see also discussion of intervention programs). However, most studies did not specifically operationalize modules, or used outcomes not well matched for intervention (e.g., using the Barthel Index including non-motor items such as incontinence with low responsiveness to document effects of functional rehabilitation) (e.g., [41]). However, such a mismatching has a major negative impact on documentation of effects of early hospital based rehabilitation [85]. Overall, the assessments mainly followed a medical perspective and in only few studies, the staff -, proxy-, or patient perspective was documented (e.g., [49]), while such evaluations may help to develop and implement feasible, effective, and meaningful programs tailored for use in hospital settings including PwCI which specific assessment strategies [86, 87].
Intervention programs
All studies were multimodal programs, without an exclusive pharmacological focus, identified in previous systematic reviews as the most effective and studied type of intervention [30, 88]. Despite the absence of target-group specific adjustments, the majority of programs were applicable at least in less affected PwCI delirium targeting risks for delirium as well as general health status. Both aims go together as delirium prevention will also reduce adverse events during hospitalization such as falls, cognitive and functional decline as well as readmission, institutionalization, and health care costs independent from cognitive status [76]. However, contrasting our expectations, only one study reported a comprehensive CI specific programs which demonstrated a structured overarching approach clearly targeting delirium prevention in PwCI [49]. However, most programs report intervention modules in which modifications may be implemented with limited resources but with high potential to adjust programs for PwCI. Interventions could be classified in three major groups.
Medical interventions
Among typical modules identified in the review, medically defined intervention components were used in combination with other modules in the majority of studies. Such medical interventions target medical risk factors for delirium and also represent generic goals for medical care irrespective of cognitive status as part of an established clinical routine. These medically oriented interventions can be operationalized, implemented, and controlled following established medical guidelines as part of general medical care during hospitalization. Although most of medical modules will be applicable, even mandatory in PwCI, such medical interventions need a specific focus and knowledge for use in delirium treatment respectively prevention, or in PwCI, which were not, or only marginally reported in identified studies. By the perspective of innovative delirium biomarkers with potential use as diagnostic or interventional strategies, medical interventions [76] may further expand in the field of delirium treatment.
With the inclusion of PwCI/delirium patients and patients with more severe impairment often associated with advanced frailty level and higher risk for adverse events during and after hospitalization [17, 18], the complexity of medical care will further increase [89], calling for a specific training of medical staff. However, no such training modules or their implementation were reported confirming previous reports, that PwCI have often been neglected in previous medical delirium interventions [31]. As demonstrated in the single outstanding intervention including delirium patients only [45], all programs with a predominantly medical focus were successful to reduce in-hospital delirium [44, 61] even in patients with more severe CI [45] or higher prevalence of CI [9], indicating that this type of intervention may have a potential to be implemented in more affected patients. A specification of medical interventions for CI/ delirium may further improve effects especially so in clinical settings in which high standard medical care has not yet been implemented.
CI-specific strategies to include staff and family members
Medical or care staff in clinical routines or study implementation directly interact with patients and represent a major key to adherence and success in this vulnerable patient sample. Thus, staff training constitutes one of the domains with high potential for CI specification including targets such as knowledge transfer, change of staff attitude, communication/interaction, reassuring/motivating of patients. Appropriately, it was directly or indirectly addressed in most studies as well as highlighted in some programs as an individual program module [48, 61], or overall target of interventions [39, 59].
However, a specific focus on cognitive impairment was lacking in all but one study despite the obvious need for specific strategies for PwCI. In few studies, specific delirium experts have been included as proposed in the HELP study with specific training for the purpose to support successful program implementation [52, 57]. An overarching focus of staff training was the strengthening of soft skills of staff and proxies, such as specific communication strategies or attitudes, mostly with no specification for PwCI, but with high potential to be used and/or adapted for CI-specific programs as shown previously for targeted education to improve communication and attitudes towards dementia [90], or the implementation of specifically trained nurses to improve care [91]. Apart from Boltz et al. (2014, 2015) with a focus on family caregivers [48, 49], only one overarching module for interaction with PwCI (validation program by Feil [62]) was implemented in a single study [53] but was not further commented. However, effective strategies to facilitate communication with PwCI in hospital have been developed and introduced in other settings/programs [92, 93] to support healthcare professionals, which may be also be implemented in delirium prevention studies. Surprisingly, evaluation of staff satisfaction has, except for single studies with a focus on process analysis, mostly not been documented in included studies as discussed in one study for limitations [55], while a detailed proxy evaluation was supported in two other study with focus on staff and family members [48, 49], indicating that staff or proxy resources may not have been in the focus of previous research and clinical implementation of delirium interventions. The inclusion of proxies or family members as shown by Boltz et al. with a focus on family caregivers [48, 49] represents a potentially low-resource intervention strategy [38] with high potential for CI specific programs, allowing to reduce disorientation of patients with CI in the new hospital setting, and an intensive personal interaction to well-known family members in patients with low social contact density during hospitalization, and an implementation by lay persons, comprehensible for PwCI [94] thereby avoiding typical pitfalls in care transitions between informal and formal care [95] and relieve professionals in resource-limited settings [96].
In the present review, studies including family members achieved a significant delirium reduction demonstrating effectiveness of such a family centered approaches [38, 54] also including study samples more affected with CI [48, 49] indicating the effectiveness of such CI-specific approaches. The study by Boltz et al. (2015) earns a special focus as the only study reporting a program developed with exclusive focus on PwCI [49]. The study provided a comprehensive background and rationale for implementation of a CI-specific program and was based on a generic family caregiver program presenting with a strong focus on staff, family members as well as patients [48] grounded on a social–ecological model and a social–cognitive theory, which was further developed for PwCI. The study developed a number of main targets intervention modules highly specific and exemplary for delirium prevention in PwCI. However, even in this program concrete CI-specifications of the program allowing for replication have also been missing in the study description.
Core modules on delirium risk
In studies identified, generic core modules as selected in the most established program (HELP), targeting risk factors for delirium during hospitalization such as malnutrition, functional decline, cognitive impairment, were included, but were not specified for PwCI/Delirium respectively severity of CI. This lack is surprising as preliminary suggestions for CI-specification of (HELP-) modules have been published, urgently calling for adapted delirium prevention studies in PwD [76]. Even in modules targeting cognitive status including elements of cognitive orientation, cognitive stimulation or communication a modification to CI status was not reported in included articles. However, implementation of each of these core modules will have a very different context in CI/delirium patients as compared to patients with intact cognition, requesting CI-specification of interventions adjusted to different forms of impairment. On module level, successful intervention strategies have been developed and implemented in PwCI in hospital- or neighboring settings such as ward based geriatric rehabilitation, which could be used for adaption of existing interventions in early, hospital-based rehabilitation. Such interventions documented extraordinary results to improve functional performance [97], convincing evidence that even basic CI-specific clinical routines may allow improvement of overall cognitive status [98], or strategies to communicate and identify meaningful individualized rehab goals [87] in this vulnerable population receiving less therapy as compared to peers with intact cognition [99].
On the comprehensive intervention level, different treatment options for DSD prevention have been summarized [34], specific physical and occupational therapies in persons with DSD have been reviewed and analyzed [33], interventions in hospitalized persons without focus on CI [30], or in neighboring settings such as in long term care [100], or post-acute care [89] may be used to develop specific hospital-based early rehab delirium prevention interventions.
General effects of interventions
In the present review, results of the meta-analysis indicated significant effects to reduce delirium during hospitalization by generic interventions in study samples with on average low CI as well as for subtypes according to study design and cognitive status. Good news is both meta-analyses documented effectiveness of published programs confirming previous meta-analytic results for overall effects of delirium prevention studies [30, 88], with new aspects for effect of type of intervention and cognitive status by the present review. However, interventions were less effective in more affected PwCI, although this group included on average patients with only moderate stage CI as compared to the other subgroup with no or MCI. Results confirm the negative association/interaction between CI and delirium with an increasing CI level related to more frequent delirium incidence as also reported in single articles for effects of intervention [52, 101]. Results of the meta-analysis may thereby also document a reduced efficacy of untailored interventions with increasing impairment level indicating a potential lack as well as chance for future CI-specific programs. However, the analysis did not cover patients with advanced CI or severe stages of delirium which were excluded in studies allowing no general evaluation covering the whole range of CI.
Included studies did not differentiate between prevention of delirium versus reduction/treatment of ongoing delirium, although studies postulated respectively reported that preventive interventions are more effective than interventions once delirium is present [89, 102], with decreased effects according to increased delirium severity [52, 55] representing a potential link to the inferior effects of treatment in preexisting delirium. Unspecified programs including existing as well as newly developed delirium episodes as in most studies included in the present review did not allow to analyze specificity of effects with respect to prevention versus treatment (e.g., by documented cumulative delirium incidence as the main study outcome) also negatively affecting comparability of such mixed purpose studies.
Effect of intervention on individual modules
Effects of programs with respect to delirium prevention were presented in all studies for packages of interventions with only few studies [41, 57] providing an analysis of effects at module level as part of a multimodal intervention. As the study effects for comprehensive interventions were heterogeneous and cannot clearly be allocated to specific types of programs (e.g., mixed versus single domain studies, professional versus volunteer based interventions) nor to the number of modules, an in-depth analysis seems mandatory to clarify effectiveness of single modules. With the limitation that studies were not calculated for such exploratory (sub-) analyses with the risk of being under-sampled, analysis of individual modules may allow to improve operationalization, specification, and effects of modules and identify most effective program parts. Such analyses with a potential focus on responsiveness to interventions may have helped to further focus established programs [52] to reduce original more extended versions to abbreviated core versions [41, 57] with comparable effectiveness to reduce delirium incidence during hospitalization. While few studies presented effects of interventions on individual module level, none of the studies presented results for impact of modules on the main study objective to prevent delirium, thus not allowing to ascribe benefits of multicomponent interventions to individual elements [54]. The lack of such sub-analyses was accounted for by risk of under-sampling and inadequate study design [53, 60]. However, analyzing effects of single modules may represent a key to further optimize and specify programs in general and especially so for vulnerable subgroups such as PwCI also offering insights into mechanisms why interventions may work successfully. Unfortunately, due to the scarcity of sub-analyses for single modules and the restricted description of interventions, as well as the lack of modules specified for PwCI, the identification of most effective program modules for PwCI/delirium was limited in the present study.
Adherence/implementation
Effectiveness of interventions depends on key determinants of programs including duration, intensity, specificity, accessibility/implementation, and adherence to interventions [103]. While not very much detail information was given in studies on module level for duration, intensity, and specificity, some data was provided for implementation of and adherence to complete interventions. Only in twelve studies adherence/implementation of program modules were reported while continuous monitoring of participation and progress are mandatory to increase treatment fidelity (compare, as discussed in [41]) and efficacy [55]. Study results indicated a large heterogeneity for implementation respectively adherence which are not easy to adjust for treatment exposure (compare [104]) when analyzing interventions. Specific strategies to support adherence for participants in general or for PwCI or delirium were not addressed/reported, with one study having a (marginal) focus on motivation “to actively encourage mobility and functional independence” [54]. However, such strategies will be most requested especially in PwCI/delirium presenting with low adherence to study interventions [105, 106], and result in higher effectivity [103].
Sub-analysis according to cognitive status
Sub-analysis according to cognitive status represents a prerequisite to analyze the impact of cognitive impairment on effectiveness and feasibility and further development of CI-specific delirium programs as an alternate approach when the study design is not specified for CI. Surprisingly only one-third of the studies performed any sub-analysis despite the fact that all studies included mixed or unspecified samples with respect to cognitive status. Design and objective for these sub-analyses were extraordinary heterogeneous with no common target visible and not always related to the study objective to evaluate effects of intervention programs on delirium or other main study outcomes indicating a rather exploratory proceeding in most studies. For sub-analyses, no separate sample calculations were mentioned and therefore (sub)-analyses have been at risk for under-sampling, addressed as a limitation by authors [9].
Studies confirmed the narrow relationship between CI and delirium with a higher delirium incidence in PwCI in 4 studies [9, 55] as also confirmed by results of the meta-analysis for effects of intervention by the present study. Only two studies analyzed intervention effects according to severity of delirium [52, 101] reporting positive intervention effects in the moderate but not in high-risk group for incident delirium, indicating lower efficacy of such programs— unspecified for severity of delirium— in more affected persons. Surprisingly, no study performed a sub-analysis for effects of intervention for patients with preexisting delirium versus those patients which newly developed delirium, although a considerable number of studies included in the present review have included both forms of delirium while different effectiveness for treatment versus prevention of delirium has been reported in included studies with primary prevention as the most effective strategy [89, 102].
Sub-analyses of existing studies or comparative studies on issues discussed above are requested to provide solid evidence for effect of intervention. The lack of data analysis according to cognitive status also indicated that the subgroup of CI/delirium patients may not have been in the focus of interventions in early hospital-based rehabilitation so far, leaving considerable space to further optimization of programs for this field of research.
Risk of interventions
No adverse events were reported, which is in line with the expectations for the rather generic, low risk multimodal interventions targeting risk factors for delirium and general health status as included in this review. Thus, the lack of adverse events qualifies such interventions to be appropriate for good medical practice in hospital treatment in general and provides no justification for the frequent exclusion of PwCI/delirium in studies. However, further specification of interventions tailored for patients with CI and delirium may turn out to be superior to such generic approaches, increasing effects on delirium prevention with no additional risks of such future programs.
Strengths and limitations
According to the study objective a strength of the present review is to identify gaps in the literature to support the planning and commissioning of future research and clinical processes for delirium prevention using recently published, comprehensive, high class data sources preselected for the setting (acute hospital medical care) and intervention (early hospital-based rehabilitation) for clinically relevant research questions with direct implication for a most vulnerable patient population. The search strategy was mainly based on previously published scoping review articles reporting on state of the art in this field. As with other reviews, we cannot exclude that the search strategy may not have identified all published articles. However, by the most sensitive search of review articles by the umbrella approach and the inclusion of all single articles in these reviews, we are confident that most relevant publications in the field of hospital-based, early rehabilitation have been identified. No specific review for the study objective could be found by an extensive basic literature search.
We cannot exclude that intervention studies used programs or parts of interventions which were specific for PwCI, when specifications were not explicitly reported in articles or already part of clinical routines. However, we are confident that by the performed literature search we obtained a conclusive and most comprehensive picture of the state of the art with respect of implementation of CI specific programs in early hospital based rehab. Including indicators of a CI perspective allowed to identify also studies with incomplete CI-approaches, which would otherwise be hard to identify.
Conclusion
Study results document a lack of implementation for delirium prevention programs specifically tailored for older PwCI (mean age > 65 years) respectively patients with preexisting delirium in early, hospital-based rehabilitation. Study results call for the documentation of prevalence of CI/delirium at hospital admission, the sub-analysis and specification of the target study population according to cognitive status, as well as the distinction between prevention or reduction of ongoing delirium to design CI specific delirium programs in the future. Analysis of adherence and effectiveness of sub-programs (modules) may help to further optimize the development of programs, while programs tailored for CI status, respectively level of impairment, may substantially increase effects of intervention in the neglected group of patients with CI. A common data set as developed in other research fields such as fall prevention [107] may reduce heterogeneity of assessment and increase comparability of study results. Specification of existing rehab concepts for CI and amendment by specified CI modules/programs in related rehab settings may help to develop, implement, and further optimize delirium prevention in PwCI in acute medical care.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report. Compliance with guidelines on human experimentation as well as protocol approval by a local Institutional Review Board not required.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors declare no conflict of interest related to this work.
K. Hauer is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article and/or its supplementary material. Other data is available on request from the corresponding author.