
Abstract
Background:
The role of metabolic syndrome (MetS) on dementia is disputed.
Objective:
We conducted a Mendelian randomization to clarify whether the genetically predicted MetS and its components are casually associated with the risk of different dementia types.
Methods:
The genetic predictors of MetS and its five components (waist circumference, hypertension, fasting blood glucose, triglycerides, and high-density lipoprotein cholesterol [HDL-C]) come from comprehensive public genome-wide association studies (GWAS). Different dementia types are collected from the GWAS in the European population. Inverse variance weighting is utilized as the main method, complemented by several sensitivity approaches to verify the robustness of the results.
Results:
Genetically predicted MetS and its five components are not causally associated with the increasing risk of dementia (all p > 0.05). In addition, no significant association between MetS and its components and Alzheimer’s disease, vascular dementia, frontotemporal dementia, dementia with Lewy bodies, and dementia due to Parkinson’s disease (all p > 0.05), except the association between HDL-C and dementia with Lewy bodies. HDL-C may play a protective role in dementia with Lewy bodies (OR: 0.81, 95% CI: 0.72–0.92, p = 0.0010).
Conclusions:
From the perspective of genetic variants, our study provides novel evidence that MetS and its components are not associated with different dementia types.
Keywords
INTRODUCTION
Dementia is characterized by a chronic and progressive decline affecting cognitive function in aged adults [1]. Generally, the main types of dementia consist of Alzheimer’s disease (AD), vascular dementia, frontotemporal dementia, dementia with Lewy bodies, and dementia in Parkinson’s disease. It is estimated that there have 50 million patients around the world [2]. More seriously, the number of cases is dramatically increasing due to the increasing life expectancy and risk factors [3], which puts a heavy burden on individuals, families, health care, and society. Therefore, strategies for preventing and alleviating dementia are priorities in healthcare.
Metabolic syndrome (MetS) is a cluster of pathological conditions based on the World Health Organization’s (WHO) definition, including glucose abnormalities, hyperlipidemia, central obesity, and hypertension [4]. At present, the incidence of MetS is increasing rapidly, and approximately 25% adults have MetS [5]. Some studies have shown that MetS has a positive association with the risk of dementia [6, 7], while no association is observed, even the inverse relationship in other studies [8, 9]. In addition, obvious confounding factors such as the study design and retrospective features are inherent shortcomings in these observational studies, which may interfere with the understanding of these conclusions.
Mendelian randomization (MR), as a genetic approach, is a robust statistical analysis using genetic variants to make a causal inference, which can overcome the limitation of observational studies [10]. During gestation, single nucleotide polymorphism (SNP), a genomic variant at a single base position in the deoxyribonucleic acid (DNA), is assorted randomly in forming a zygote [11]. However, no study has been conducted to investigate the causal association of MetS and its five components on dementia. Therefore, we performed this MR analysis to illustrate their causal links.
METHODS
Study design
The overview of our MR study is shown in Fig. 1. In our study, we explored the causal relationship between MetS, waist circumference (WC), hypertension, fasting blood glucose (FBG), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and different dementia types, including AD, vascular dementia, frontotemporal dementia, dementia with Lewy bodies, and dementia due to Parkinson’s disease. No ethical approval is required due to the analysis of the public summary-level datasets.
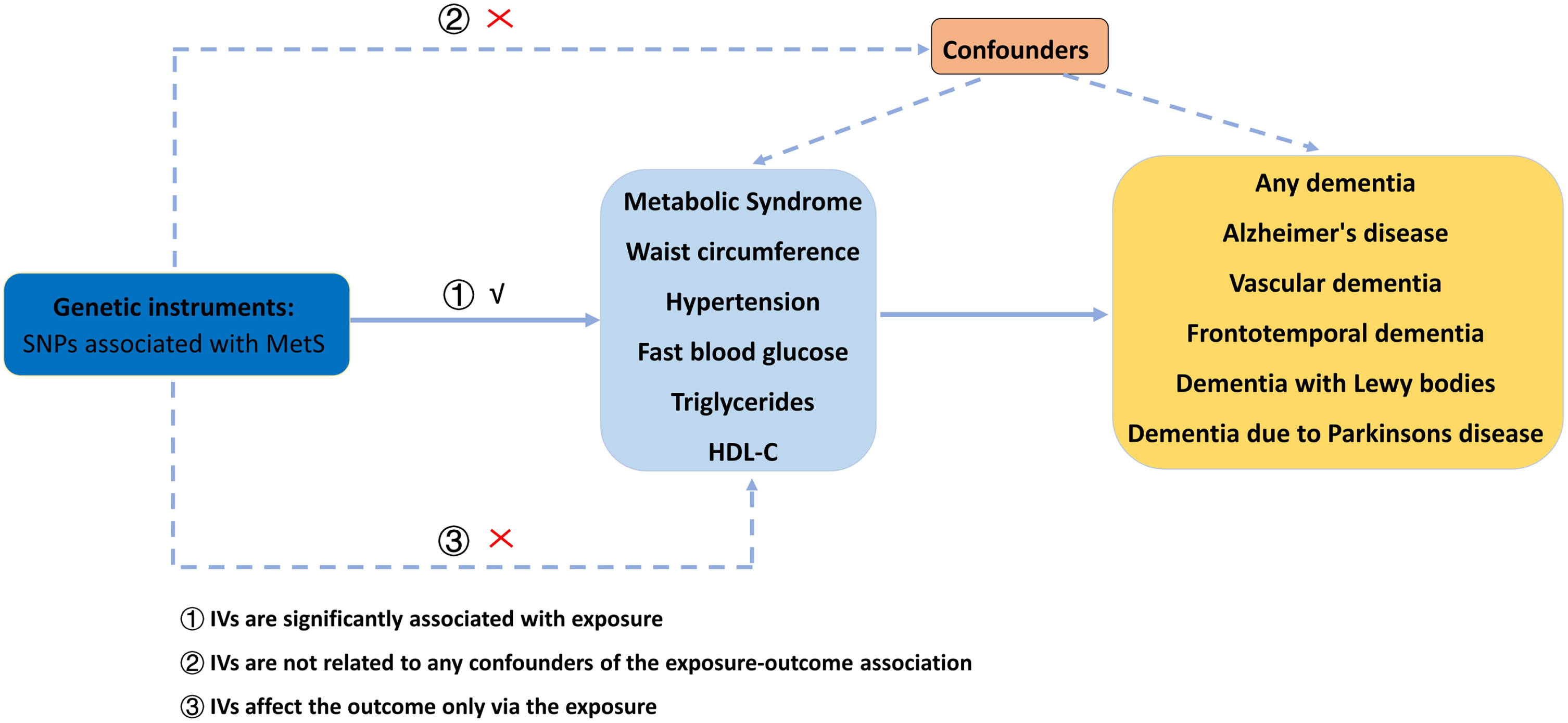
The flow chart of our MR analysis. MetS, metabolic syndrome; MR, Mendelian randomization; SNP, single nucleotide polymorphism; HDL-C, high-density lipoprotein cholesterol.
Date sources of exposures and outcomes
All exposure datasets are originated from public databases. MetS (N = 291,107 samples), WC (N = 462,166 samples), hypertension (N = 463,010 samples), TG (441,016 samples), and HDL-C (403,943 samples) are obtained from the UK biobank [12, 13]. Genetic predictors for FBG (281,416 participants) are available from the Meta-Analyses Glucose and Insulin-related traits Consortium (MAGIC) [14]. The detailed sources of these datasets utilized in our MR study are described in Table 1.
The R 2 and F-statistics for the genetic instruments in the MR analyses
MetS, metabolic syndrome; WC, waist circumference; FBG, fasting blood glucose; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol.
All outcome datasets are derived from European ancestry. The summary-level dataset for AD are taken from the MR study including 954 cases and 487,331 controls [15]. The dataset for vascular dementia is extracted from the FinnGen consortium, consisting of 212,389 samples (881 cases and 211,508 controls). As to frontotemporal dementia, its dataset includes 515 cases and 2,509 controls [16]. Summary statistics for dementia with Lewy bodies are collected from an independent GWAS multicenter study with 2,591 cases and 4,027 controls [17]. Dementia due to Parkinson’s disease consists of 212,389 samples (267 cases and 216,628 controls) from the FinnGen consortium. The detailed resources of our datasets are visualized in Table 1.
Genetic instrument selection
Genetic instruments are usually collected as those having statistically robust associations with the risk factor in a MR analysis [18]. The genetic instrument selection undertaken the following procedures. All the genetic instrumental variables (IVs) associated with MetS and its five components must meet a significance level at a genome-wide statistical threshold of p < 5×10–8. Then, the independent SNPs are identified using the linkage disequilibrium (LD) with the threshold of LD r 2 < 0.05 at a window size of 10,000 Kb [19, 20]. In addition, Mendelian Randomization Pleiotropy RESidual Sum and Outlier (MR-PRESSO) analysis is used to detect the potential outlier SNPs accounting for possible pleiotropy [21]. The SNPs will be removed when the outlier SNPs are detected. The qualified SNPs of MetS and its five components are displayed in Table 1.
Main statistical analyses
The inverse variance weighting (IVW) approach is deemed as the main method in our MR study because it can obtain a robust result by integrating the Wald ratio of each SNP into an overall weighted effect [22]. The Bonferroni-corrected p < 0.0013 (0.05/36) is regarded as the statistical significance. All analyses are performed using R packages including “TwoSampleMR”, “mr.raps”, and “cause”, in R software (version: 4.1.2, The R Foundation, Vienna, Austria).
Sensitivity analyses
We also chosen five methods to perform sensitivity analyses, including MR robust adjusted profile score (MR.RAPS), MR-PRESSO, weighted median, MR-Egger, and Maximum likelihood. When there were weak IVs that led to horizontal pleiotropy, the results of MR.RAPS could remain stable [23]. Significant outliers could be detected using MR-PRESSO and then removed for pleiotropy [21]. The weighted median approach could obtain consistent results even though 50% of SNPs were invalid [24]. The results of the comparison between the egger intercept term and zero were introduced in MR-Egger analysis, which represented the directional pleiotropy [25]. In the maximum likelihood analysis, a relatively low standard error existed, and it might be deviated by a small sample [26]. Furthermore, the egger intercept term in MR-Egger analysis and the p value in MR-PRESSO analysis were introduced into the regression model to test the directional pleiotropy. Cochran’s Q test was performed to identify possible heterogeneity. In addition, leave-one-out analysis was utilized to explain the robustness of the results when removing SNPs in turn.
RESULTS
The casual effects of genetically predicted MetS and its components on dementia
The results of this MR study are presented in Table 2. The demographic characteristics for dementia are displayed in Tables 3–5.
The causal effect of MetS and its components on different types of dementia
MetS, metabolic syndrome; WC, waist circumference; FBG, fasting blood glucose; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; IVW, inverse-variance weighted; RAPS, robust adjusted profile score; OR, odds ratio.
The demographic characteristics for any dementia, vascular dementia, dementia due to Parkinson’s disease
The demographic characteristics for frontotemporal dementia
The demographic characteristics for dementia with Lewy bodies
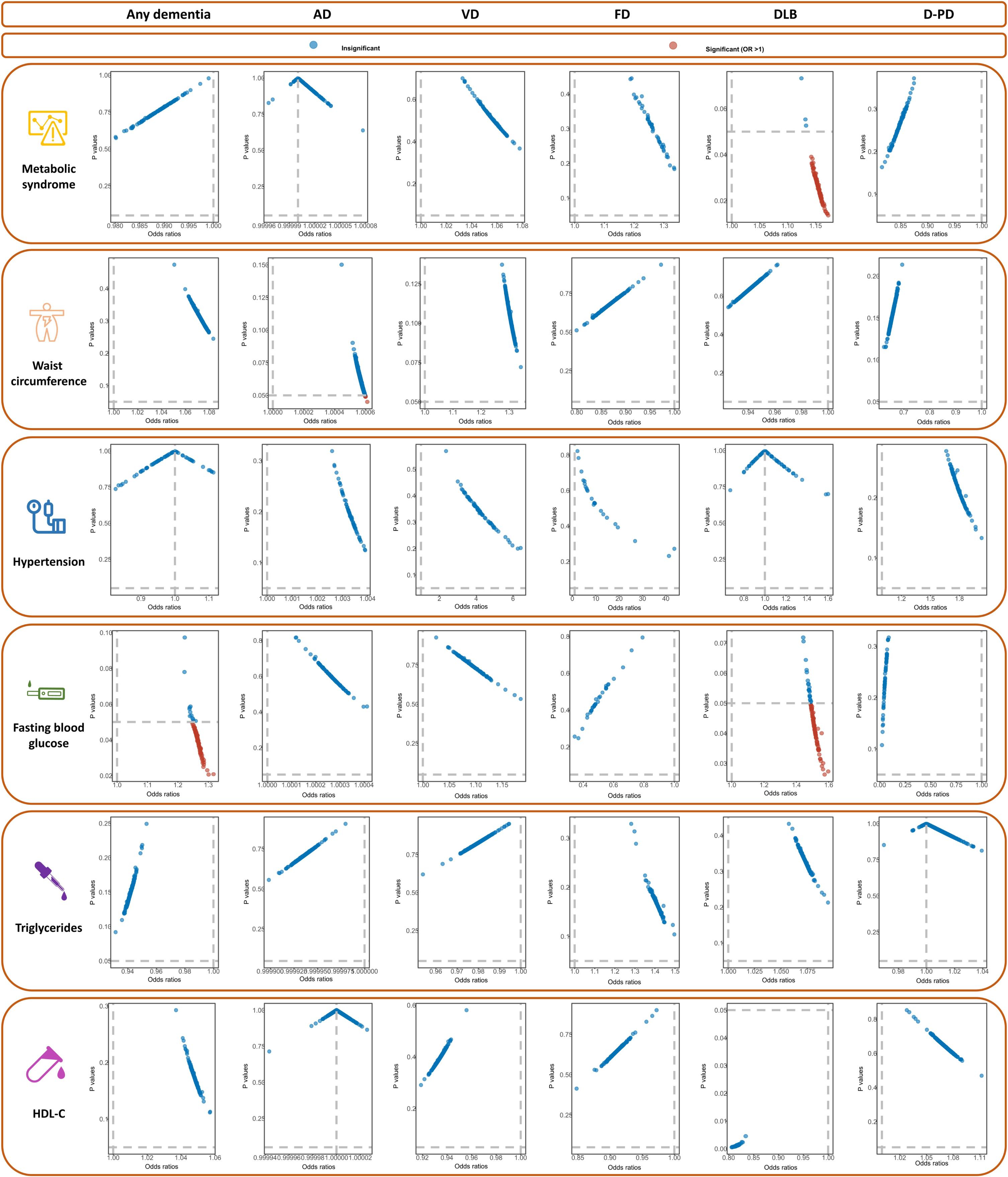
As to any dementia, it can be found that MetS, WC, hypertension, FBG, TG, and HDL-C are not causally associated with the risk of any dementia (all p > 0.0016, Table 2, Fig. 2). The results of Cochran’s Q analysis show a visible heterogeneity between TG and any dementia (Table 2), while a symmetry of MR results in the funnel plot (Fig. 3) is observed. In the MR-Egger and MR-PRESSO analyses, no pleiotropy is identified (MR-Egger: all p > 0.05; MR-PRESSO: all p > 0.05, Table 2). Additionally, no influential SNPs are detected in the leave-one-out analysis when excluding any one of the SNP in turn (Fig. 4). Figure 5 presents the results of the causal estimate of every SNP on any dementia.
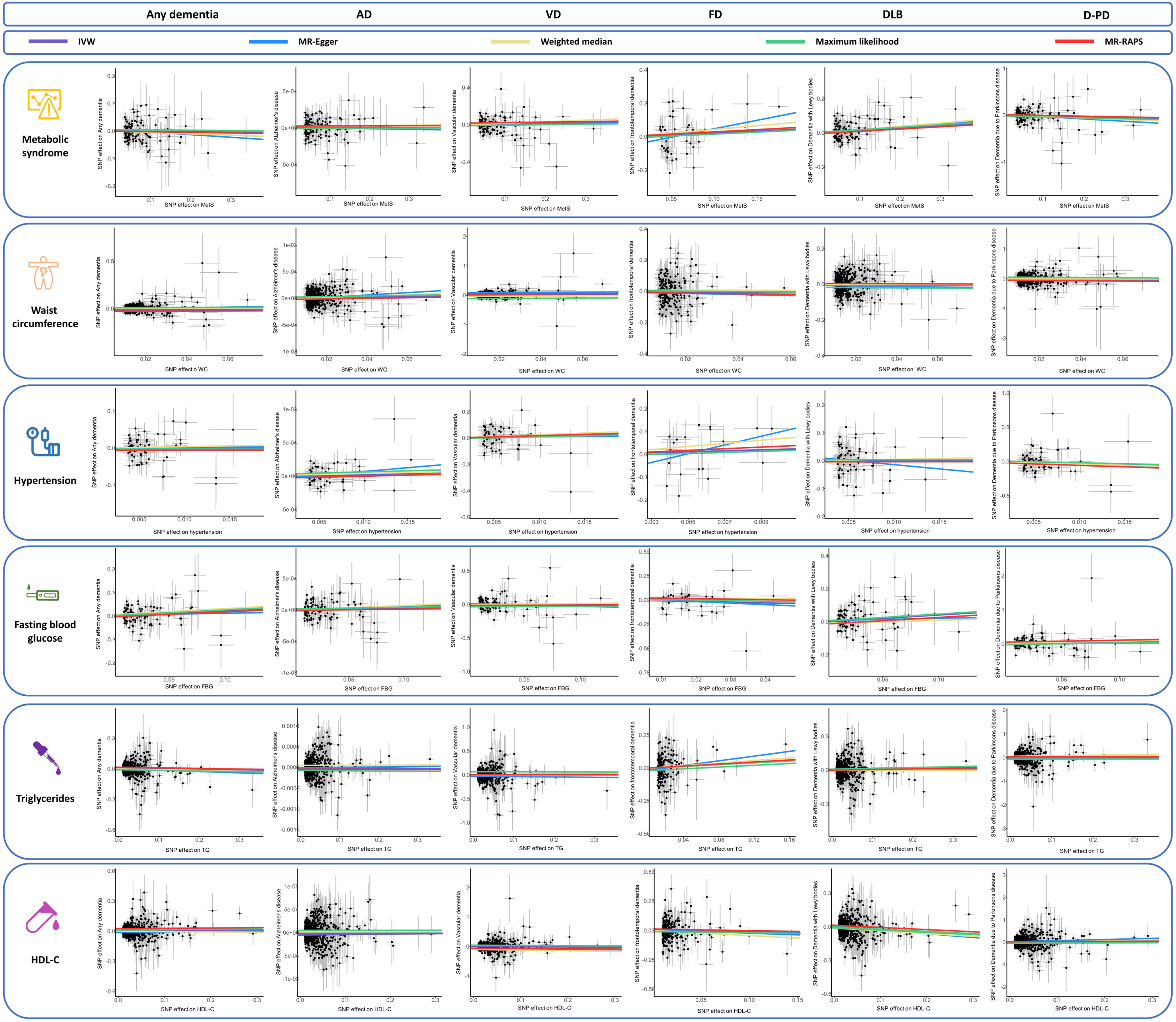
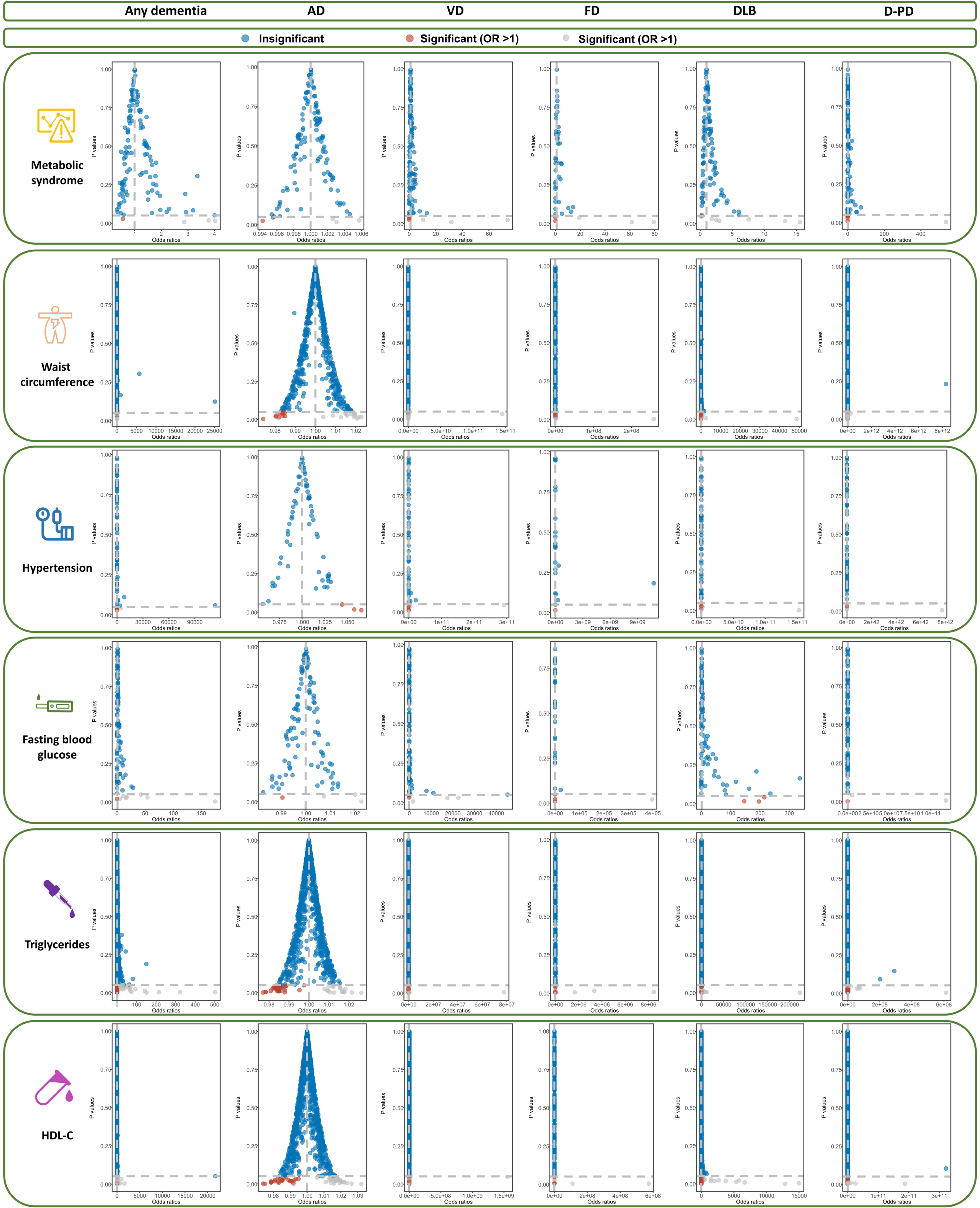
The scatter plots of the association between genetically predicted MetS and its components on dementia in the MR analysis. MetS, metabolic syndrome; WC, waist circumference; FBG, fasting blood glucose; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; AD, Alzheimer’s disease; VD, vascular dementia; FD, frontotemporal dementia; DLB, dementia with Lewy bodies; D-PD, dementia due to Parkinson’s disease.
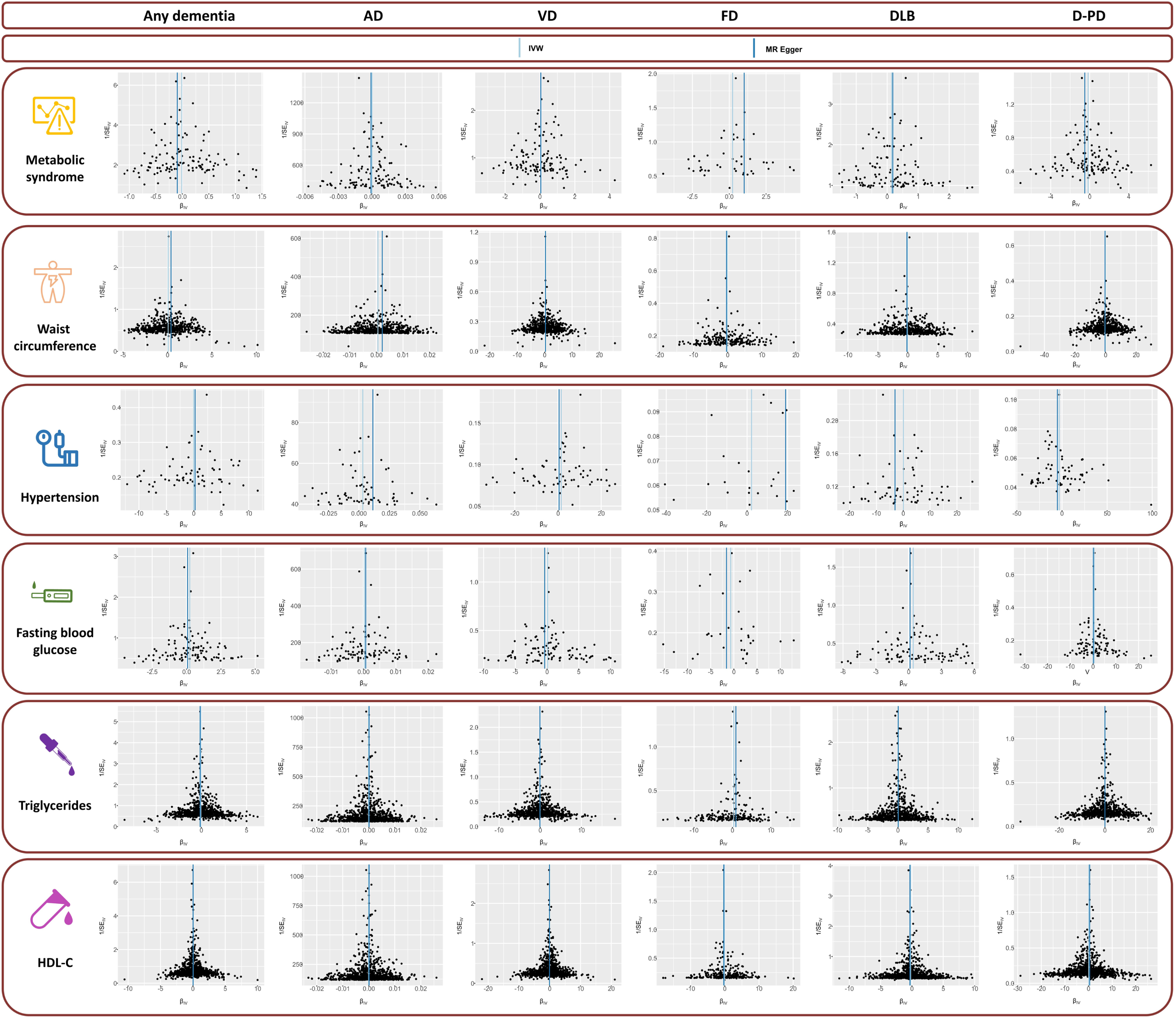
The funnel plots of the association between genetically predicted MetS and its components on dementia in the MR analysis. AD, Alzheimer’s disease; VD, vascular dementia; FD, frontotemporal dementia; DLB, dementia with Lewy bodies; HDL-C, high-density lipoprotein cholesterol; MR, Mendelian randomization; D-PD, dementia due to Parkinson’s disease.
The leave-one-out analysis of the association between genetically MetS and its components on dementia in the MR analysis. AD, Alzheimer’s disease; VD, vascular dementia; FD, frontotemporal dementia; DLB, dementia with Lewy bodies; HDL-C, high-density lipoprotein cholesterol; MR, Mendelian randomization; D-PD, dementia due to Parkinson’s disease.
The frost plots of the association between genetically MetS and its components on dementia in the MR analysis. AD, Alzheimer’s disease; VD, vascular dementia; FD, frontotemporal dementia; DLB, dementia with Lewy bodies; HDL-C, high-density lipoprotein cholesterol; MR, mendelian randomization; D-PD, dementia due to Parkinson’s disease.
For AD, the results of IVW method show that no causal relationship of MetS and its subtypes is identified (all p > 0.0016, Table 2, Fig. 2). No evidence of heterogeneity is detected in Cochran’s Q analysis (all p > 0.05, Table 2) and the funnel plot (Fig. 3). Furthermore, no signs of pleiotropy is found in MR-Egger and MR-PRESSO analyses (Table 2). The leave-one-out analyses indicate the robustness of our MR results (Fig. 4). The causal estimate of each IV on AD is shown in Fig. 5.
In MR analysis for vascular dementia, we do not observe significant causal association between MetS, its subtypes, and vascular dementia (all p > 0.0016, Table 2, Fig. 2). In sensitivity analysis, Cochran’s Q test does not find any heterogeneity (Fig. 3, Table 2). In addition, there is no evidence of pleiotropyin MR-Egger and MR-PRESSO analyses (Table 2). The causal estimates are not driven by single SNP in the leave-one-out analysis (Fig. 4, Table 2). The frost plot manifesting the casual estimate of every SNP on vascular dementia is shown in Fig. 5.
As to frontotemporal dementia, there is no causal association between MetS, WC, hypertension, FBG, TG, HDL-C, and frontotemporal dementia (all p > 0.0016, Table 2, Fig. 2). Although the results in Cochran’s Q test demonstrate a visible heterogeneity between MetS and frontotemporal dementia (Table 2), the funnel plot reveals a symmetry of MR results (Fig. 3). We do not find pleiotropy in MR-Egger and MR-PRESSO analyses (Table 2), and the results of leave-one-out analysis remain robust (Fig. 4, Table 2). The causal estimate of each IV on frontotemporal dementia is displayed in frost plot (Fig. 5).
HDL-C decreases the risk of dementia with Lewy bodies (odd ratios (OR) = 0.81, 95% confidential index (CI) = 0.72–0.92, p = 0.0010), while no causal relationship is observed between MetS, WC, hypertension, FBG, TG, and dementia with Lewy bodies (all p > 0.0016, Table 2, Fig. 2). The funnel plot is symmetrical despite a visible heterogeneity in Cochran’s Q analysis (Table 2, Fig. 3). MR-Egger method and MR-PRESSO do not find potential pleiotropy (Table 2). The results of the leave-one-out analysis are stable (Fig. 4). The causal estimate of each SNP on dementia with Lewy bodies is depicted in Fig. 5.
As shown in Table 2 and Fig. 2, MetS and its five components are not causally related to dementia due to Parkinson’s disease (all p > 0.05). In sensitivity analyses, although there has pleiotropy (MR-Egger: p-Egger intercept <0.05, Table 2), the relationship still does not exist after performing CAUSE analysis (p = 0.94). There is no evidence of heterogeneity according to the findings of Cochran’s Q test and the funnel plot (Fig. 3, Table 2). Additionally, the robustness of the MR estimates is verified by the leave-one-out analysis (Fig. 4). Figure 5 demonstrates the casual estimate of each SNP on dementia due to Parkinson’s disease.
The opinion about the relationship between MetS, its components and dementia in references
AD, Alzheimer’s disease; MetS, metabolic syndrome; WC, waist circumference; FBG, fasting blood glucose; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol.
DISCUSSION
In our MR analysis, we find that no significant causal association exists between MetS, its five components, and different dementia types, including any dementia, AD, vascular dementia, frontotemporal dementia, dementia with Lewy bodies, and dementia due to Parkinson’s disease, except for the relationship between HDL-C and dementia with Lewy bodies. HDL-C may play a protective role in dementia with Lewy bodies.
The previous results of the association between MetS, its components, and dementia is summarized in Table 6. The role of MetS on any dementia is not yet concluded. Some studies support the association between MetS and any dementia. For example, a cohort study including 1,519 participants conducted in Singapore finds that the MetS is associated with an increased risk of dementia [6]. The findings in the Whitehall II study also reveal that persistent MetS decline cognitive performance in late midlife [7]. In contrast, other studies do not support the association. In a cross-sectional and prospective study consisting of 2,476 men and women aged 65 years, researchers find that MetS is not associated with the increasing risk of dementia after 4.4 years of follow-up [8]. A recent meta-analysis including 18,313 participants ranging from January 1, 2000 to August 31, 2018 shows that no statistical significance pooled association emerges between MetS and dementia [27]. Some studies even support the protective role of MetS on dementia [9]. In our MR study, we do not identify the causal association between MetS and any dementia.
For the relationship between five components of MetS and any dementia, the association remains inconsistent. As to waist circumference, Abbatecola and his colleagues think that WC can predict the risk of cognitive decline during the 12-year follow-up in older patients with diabetes [28]. However, a study including 2,565 men and women does not find the association [29]. In our MR study, we do not support the causal association. The effect of hypertension on dementia remains unclear. Considering the numerous factors affecting hypertension, such as age and hypertension chronicity, the role of hypertension in dementia is complex [30]. For example, large epidemiological studies have demonstrated a consistent association between high midlife blood pressure and cognitive decline, while a similar association between late-life blood pressure and cognition decline is not consistent [31]. From the perspective of neuroimage, a recent study finds that hypertension may alter brain structure and function, which may result in disruption in cognitive function [32]. However, the causal association between hypertension and dementia does not exist in this study. FBG represents the abnormality of glucose level and is recognized as a well-known risk factor for dementia [33, 34], while we do not identify the causal association. In the association of TG, HDL-C, and dementia, the results also remain inclusive [35 –37]. Our MR analysis does not find a causal relationship.
Inconsistent conclusions are also obtained about the association between MetS, its components, and AD [27, 38]. A meta-analysis, including a total of 18,313 participants aged older than 40 years with mean MetS prevalence of 22.7% and followed on average for 9.41 years, found that no significant pooled association existed between MetS and AD [27]. However, contradictory results also been reported [39], and the inverse association also have been observed [40]. As for MetS components, the effects on AD remain inconsistent. For example, a meta-analysis including 16 cohort studies and 41,781 participants and 4,511 dementia cases, no beneficial impacts of obesity in older age on incident dementia is found [41]. However, a study including a total of 10,308 adults found the detrimental effects on AD incidence [42]. In our MR study, no causal association between MetS, its components and the risk of AD were identified.
The studies related to the role of MetS on vascular dementia support the detrimental effect of MetS and may increase the risk of vascular dementia [43, 44], although these studies are scarce. In the Italian Longitudinal Study on Ageing including a total of 2,097 participants (MetS subjects [n = 918], subjects without MetS [n = 1,179]), studies found that MetS elevated the risk of vascular dementia [44]. So far, potential associations between frontotemporal dementia, and head trauma [45], diabetes [46], and autoimmune conditions may exist [47]. However, the study about the causal association between MetS and frontotemporal dementia is limited [48]. The study related to the association between MetS and dementia with Lewy bodies [49] and dementia due to Parkinson’s disease is also scarce, and no association between MetS, its components and dementia due to Parkinson’s disease was identified [50]. In our MR study, we find no significant casual association between MetS, its components and vascular dementia, frontotemporal dementia, and dementia due to Parkinson’s disease. As for dementia with Lewy bodies, Dou and colleagues thought that reduced levels of HDL-C were associated with the development of dementia with Lewy bodies in a case-control study including 65 patients with Lewy body dementia and 110 older adult controls [51]. Several studies also supported the relationship [52, 53].
Many observational studies may be influenced by many confounding factors such as limited sample size or (and) retrospective study. The strength of our MR study overcomes the possible confounders and clarifies the causal association between MetS and different dementia types. Additionally, it is the first study to illustrate their association. However, this study has several limitations. Firstly, the cases of different dementia are relatively small. Second, there is an ethnic bias because the datasets are all of European ancestry, which may limit the generalization of the conclusion. Third, we do not make stratification based on some factors such as age and gender due to the unavailability of stratification datasets. Future studies are required to verify these association in other ancestries, larger studies, and proper stratification people.
Conclusion
In our MR study, MetS and its components do not increase the risk of different dementia types., while HDL-C may play a protective role in dementia with Lewy bodies.
Footnotes
ACKNOWLEDGMENTS
We give great appreciation to the participants and working staff for their excellent job to the study.
FUNDING
This study was supported by the 1 3 5 project for disciplines of Excellence-Clinical Research Incubation Project, West China Hospital, Sichuan University (2018HXFH010).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.