
Abstract
Background:
Nutrition has relevant role in the pathogenesis of dementia. However, in Latin American Countries (LAC), it is unknown which type of diet the subjects with dementia and cognitive dysfunction have.
Objective:
The main purpose of this study was to determine micro- and macronutrients and food frequency intake among the LAC population with mild cognitive impairment (MCI) and dementia.
Methods:
A systematic review using PubMed, Cochrane, Lilacs, and Scielo databases. Energy intake as well as micro- and macronutrients intake were analyzed using a random-effect model and presented in a forest plot.
Results:
Nine articles were included, an estimated energy intake of 1598.47 kcal (95% CI 1351.07–1845.88) was obtained. A daily consumption of 73.64 g/day (95% CI 64.07–83.2) of protein; 262.17 g/day (95% CI 214.51–309.93) of carbohydrates, and 57.91 g/day (95% CI 49.16–66.66) of fats were reported. A micronutrients daily intake consumption of 201.35μg/day of vitamin B9 (95% CI 125.32–277.38); 5.61μg/day of vitamin B12 (95% CI 2.53–8.70), and 139.67 mg/day of vitamin C (95% CI 59.33–220.02). Mineral intake of 637.32 mg/day of calcium (95% CI 288.54–986.11) and 9 mg/day of iron (95% CI 2.28–15.71) was obtained. A low intake of fruits and vegetables was found.
Conclusion:
Individuals with MCI and dementia from LAC have a nutritional deficiency characterized by a lower intake of fruits and vegetables, a high consumption of carbohydrates and protein, adequate fats intake and vitamins B12, vitamin C, and iron consumption, but a low intake of vitamin B9 and calcium.
INTRODUCTION
Elevated frequency of older adults population have led to an increase in the prevalence of some non-communicable diseases (NCDs) such as cancer, depression, and dementia, among many others [1]. Dementia is the term for memory loss, but this syndrome also includes a deterioration of the cognitive function that affects other abilities such as language, decision making, attention, communication, among others. The most common types of this condition are Alzheimer’s disease (AD), vascular dementia, Parkinson’s disease dementia (PDD), Lewy’s bodies dementia, and frontotemporal dementia [2]. Cognitive impairment is related to dementia and ranges from mild to severe forms. The worsening of cognitive impairment in any of its forms, leads to the diagnosis of dementia [3].
According to World Health Organization (WHO) data, 50 million people with dementia, with the majority of the remaining half, living in low- and middle-income countries including Latin American countries (LAC) [4]. Few data are available regarding cognitive impairment spectrum among LAC population [5]. A recent meta-analysis reported a 14.95% prevalence for all-types of cognitive impairment in LAC [6]. This prevalence is superior to frequencies reported in other countries with higher incomes [7].
Mild cognitive impairment (MCI) and dementia are important issues. However, LAC face many challenges including the lack of available epidemiologic data, clinical standardization, cultural barriers, and stigmatization [8]. Moreover, dementia is still an intractable disease, and no cure has yet been found. Because these are potentially modifiable, the current focus of science relies on the control of lifestyle-related risk factors such as an unhealthy diet, physical inactivity, and obesity. Systematic reviews indicate that the managing and improvement of these risk factors may aid in preventing or even slowing neurocognitive decline [3].
Diet and nutrition represent important factors in health. In the last few years, scientific reports have noted the relevant role of nutrition in the pathogenesis of dementia. In particular, the consumption of some nutrients or vitamins appears to be linked with cognitive impairment improvement in patients with dementia [9]. Therefore, a diet that emphasizes consumption of nuts, vegetables (leafy greens), other type of vegetables, berries, beans, whole grains, fish, poultry, olive oil, red wine, as well decreased in consumption of red meat, butter, stick margarine, pastries, sweets, fried or fast food and cheese may have a beneficial effect on the risk of developing dementia. In fact, these food recommendations are based on the Dietary Approaches to Stop Hypertension (DASH) intervention for Neurodegenerative Delay (MIND) diet [10]. Some current clinical trials are testing the effect of the MIND diet on cognitive function, with support from the National Institute on Aging and The Alzheimer’s Association in U.S. [11]; however, results have yet been reported [12].
Although the systematic review studies performed on the evaluation of dietary patterns, foods, and micro- and macronutrients among population with MCI and/or dementia had no country or language restriction [13], only one study from the LAC population was included [14]. Therefore, it is unknown what type of diet the subjects with dementia and cognitive dysfunction from LAC have. The Global Action Plan on the public health response to dementia 2017–2025 implemented by the WHO indicates that it is important to generate scientific evidence about dementia’ modifiable risk factors [4], then, it is necessary to identify micro- and macronutrients, and main foods that may contribute to these nutrition-cognition issues among the LAC population in order to develop potential strategies to prevent or slow cognitive deterioration.
As a result, the purpose of this systematic review was to determine the food frequency and micro- and macronutrients consumed by MCI and dementia from LAC population.
MATERIALS AND METHODS
Study design and search strategy
This systematic review was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [15] (Fig. 1) and registered in the International Prospective Register of Systematic Reviews (PROSPERO) under reference number CRD42023390588. Three independent researchers (ALGS, AGGD, and GCL) conducted the research on the relevant literature using the PubMed, Cochrane, Lilacs, and Scielo databases. According to the PEO strategy, this systematic review included population (P), exposure (E), outcome (O) [16] (Supplementary Table 1). The search was conducted from September to November 2022. The keywords used were “dementia” or “vascular dementia” or “Alzheimer” or “mild cognitive impairment” or “cognitive function” and “diet” or “food” or “dietary pattern” or “micronutrients” or “macronutrients” or “nutrients” and “Argentina” or “Chile” or “Mexico” or “Colombia” or “Cuba” or “Peru” or “Costa Rica” or “Honduras” or “Uruguay” or “Paraguay” or “Ecuador” or “Bolivia” or “Venezuela” or “Panama” or “Brazil” or “Dominican Republic” or “Puerto Rico” or “El Salvador” or “Guatemala” or “Nicaragua”. The search was adapted to the different databases, and the gray literature was performed on Google Scholar.
Selection of the studies and applied criteria for inclusion and exclusion
After removing the duplicates, the titles and abstracts were evaluated for eligibility according to the selection criteria by the three authors (AGGD, GCL, and VMZ). The remaining articles that were not eliminated were assessed in full text, and then the final inclusion and exclusion criteria were applied. The eligibility criteria for the studies were as follows: 1) cross sectional design studies; 2) studies performed on subjects with MCI, any type of dementia or a probable cognitive deficit; 3) descriptions of foods, food groups or micro- and macronutrients intakes; and 4) subjects from LAC. The exclusion criteria were: 1) protocols, theses, monographs, commentaries, or reviews; 2) studies analyzing enteral nutrition; 3) studies that included the “MCI” or “dementia” term, but no data nor diagnosis were presented; and 4) those studies that included the “food consumption” or “type of diet” terms, but no data were presented. No language publication restriction was applied for the search (Fig. 1).
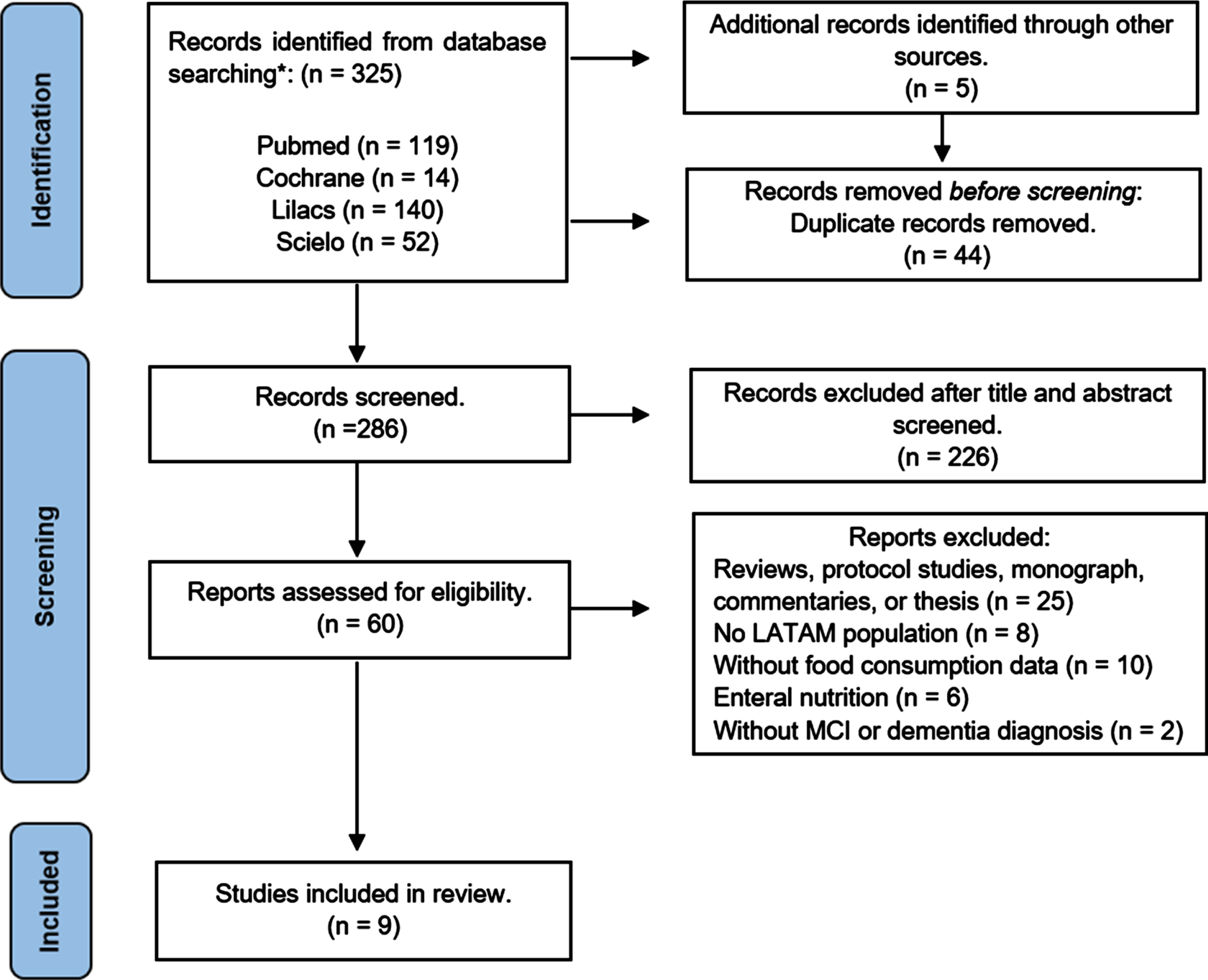
Flow chart of studies included.
Data extraction and quality assessment
Data extraction from the selected articles was performed independently by three investigators (AGGD, GCL and BPG) into a predefined database. Data regarding first author’s information, publication year, country, study design, sample, diagnoses, dietary assessment, and main findings was recorded. In the event of a discrepancy between AGGD and GCL, the final consensus was taken by another co-author (ALGS, AAN, BPG, and/or VMZ).
The quality of the included studies was apprised by three independent investigators (AGGD, GCL, and AAN) and assessed by the Joanna Briggs Institute’s (JBI) Critical Appraisal Checklist for Case Series, which includes 10 principles with yes/no/unclear questions [17] (Supplementary Table 2 and Supplementary Figure 1).
Statistics analysis
All statistical analyses were undertaken using the software RStudio version 1.0.153. Energy protein, carbohydrates, fats, vitamin B9, B12, C, calcium, and iron intakes that were reported in the selected cross-sectional studies were analyzed using a random-effects model and afterwards presented in a forest plot. Because not all the included studies had available data, only the studies that did reported were plotted and used for the analysis. Statistical heterogeneity was assessed using the I2 index. Finally, publication bias was assessed by visual inspection of funnel plots and with the Egger bias test [18].
RESULTS
Identified studies
A total of 325 articles were identified, and five additional articles were found in gray literature. Forty-four articles were removed due to duplications in the search. 226 records were excluded after being screened by title and abstract. Sixty full text articles were revised, and 51 were excluded for the following reasons: protocols, theses, monographs, commentaries, or reviews (n = 25), studies performed among subjects from non-LAC countries (n = 8), no description available of food consumption (n = 10), enteral nutrition-focused studies (n = 6), and no data or diagnosis of MCI and/or dementia (n = 2). Finally, 9 studies were selected for the present review (Fig. 1).
Description of the studies
The studies included were cross-sectional and their publication dates ranged from 2004 to 2019. Articles were published in English (n = 4), Spanish (n = 3), and Portuguese (n = 2) and were carried out in Brazil (n = 6), Colombia (n = 1), Mexico (n = 1), and Chile (n = 1), with Brazil the most represented country. The study population included subjects with diagnoses of AD (n = 6), PDD (n = 1), and MCI or probable deficit cognition (n = 3). The total number of participants ranged from 20 to 169 individuals with AD, PDD, and cognitive impairment in each study. Participant’s recruitment was performed at different health centers (n = 8) and a clinical trial (n = 1). A total of 672 subjects were analyzed in this review. Among all studies, the average age ranged from 66 to 84 years old. Food consumption information was registered through a 24-hour dietary recall (n = 4), food frequency questionnaires (n = 3), these both instruments at the same time (n = 1), and data from national health survey (n = 1) (Table 1).
Characteristics of the studies included in the systematic review
AD, Alzheimer’s disease; PD, Parkinson’s disease; PDD, Parkinson’s disease dementia; ASF, Animal source foods; ↑, High intake; ↓, Low intake; ⟶, Adequate intake; ↑↑ and ↓↓, statistically significant.
Energy intake
Four articles reported the total energy intake, which ranged from 1238.44 to 1826.3 kcal/day. Navarro-Meza et al. reported energy in kJ/day. Therefore, it was converted to kcal/day in order to be compared and plotted. The estimated total energy intake per day of the population with dementia or cognitive impairment from LAC was 1598.47 kcal (95% CI 1351.07–1845.88; I2 = 95%; p < 0.01). Agudelo-Ochoa et al. reported 1826.3±565 kcal among patients with AD in Colombia [19]. Machado et al. from Brazil reported that patients with AD in a mild state had a total consumption of 1645 kcal and subjects in a moderate state had a total consumption of 1482 kcal. However, this information was not included in the pooled analysis because data regarding the standard deviation was not available [20]. Another study from Brazil made by De Andrade Vieira et al. found that the total energy in AD patients was 1715.3±492.3 kcal [21]. Medeiros et al. also reported a total energy consumption of 1238.44 kcal among AD patients living in home health care centers [22]. Navarro-Meza et al. reported a 1622.13±206 kcal in subjects with AD and PDD in Mexico [23] (Fig. 2).
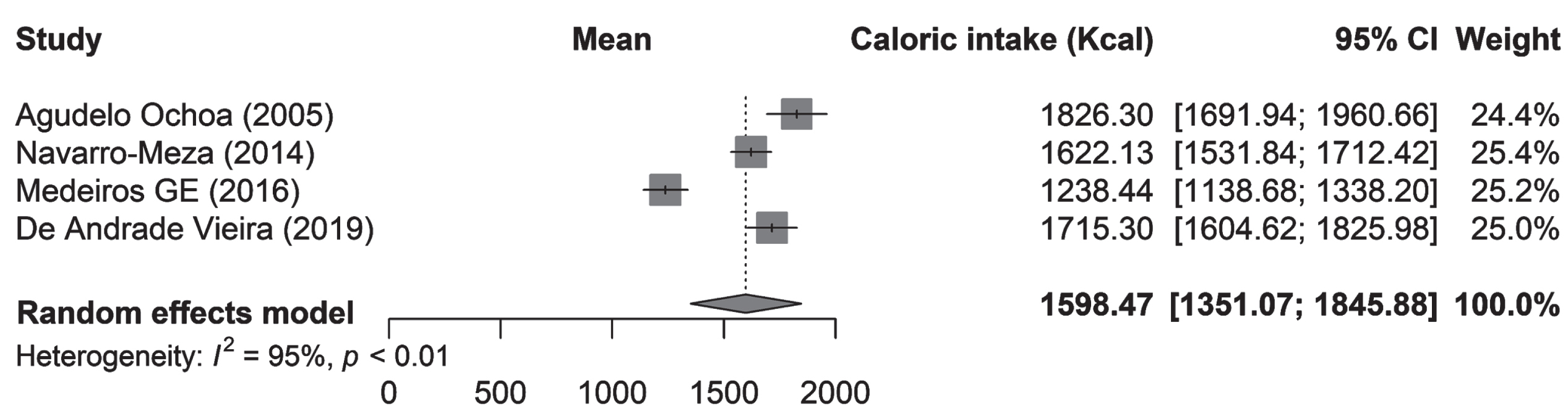
Total energy intake in subjects with MCI and dementia in LAC.
Macronutrients and micronutrients
Six manuscripts analyzed and described macronutrients and micronutrients contribution in diet. Agudelo Ochoa et al. reported that patients in a severe state of dementia showed an adequacy percentage of protein intake (%) according to the Dietary Recommendation Intake (DRI) [24]. However, patients in mild and moderate stages showed an excess in the adequacy percentage of protein. A low intake of micronutrients was reported, especially for magnesium, folates, vitamin B3, B6, and calcium consumption [19].
Machado et al. reported that macronutrients consumption in patients with mild stages of AD were distributed in 53.7% for carbohydrates, 17.5% for proteins and 28.8% for fats, while in patients in moderate AD stages, this proportion was distributed with a daily intake of 59.3% of carbohydrates, 16.1% protein, and 24.6% fats. A low intake of vitamin E was reported with an average 11 and 10 mg/dL intake for AD patients in the mild and moderate stages, respectively [20].
Navarro-Meza et al. compared patients with “AD and “PDD” versus “controls”, and the results showed that individuals with AD and PDD reported a greater protein consumption (82±8 versus 68±5; p = 0.293), but lower fat (70±13 versus 74±8; p1 = 0.688) and carbohydrate intakes compared with a control group (328±45 versus 357±28; p = 0.653). Additionally, vitamin C intake was lower in patients compared with control group (233±71 versus 3468±45; p = 0.016) [23]. Goes et al. found higher protein (74.4±378 g/day) and carbohydrate (211.9±93 g/day) intake in patients with AD compared to nutritional recommendations along with an insufficient intake of the vast majority of micronutrients analyzed [25]. Medeiros et al. reported an inadequate intake of protein (44.69 g/day) but an adequate intake of carbohydrates (133.11 g/day). Low intakes of vitamins E (5.28 mg/day), A (3.64μg/day), and B9 (35.71 mg/day), calcium (364.66 mg/day), zinc (5.13 mg/day), and selenium (14.33μg/day) were found in women and men with AD [22]. Finally, De Andrade Vieira et al. reported an adequacy percentage of macronutrients (carbohydrates (55.9%) and fats (52.4%)) but a higher protein (17.2%) consumption. In relation to micronutrients, vitamin C intake was acceptable but sodium did not reach the recommended dietary intakes [21] (Tables 1 and 2). No group achieved the recommend fiber intake.
Daily intake of energy, macro and micronutrients reported in subjects with MCI and dementia in LAC
MCI, mild cognitive impairment; LAC, Latin American Countries; akJ a kcal; b%; cnot unit of measure available; dRE (retinol); NA, not available; W, women; M, men; DRIs, Nutrient Recommendations: Dietary Reference Intakes (DRI) by the Food and Nutrition Board of the National Academies of Sciences Engineering, and Medicine.
Data on macro- and micronutrients were estimated and pooled. Results showed a total consumption of 73.64 g/day of protein (95% CI 64.07–83.21; I2: 91%; p < 0.01), 262.17 g/day of carbohydrates (95% CI 214.51–309.93; I2: 95%; p < 0.01), and 57.91 g/day of fats (95% CI 49.16–66.66; I2: 86%; p < 0.01) (Fig. 3). The following micronutrients were analyzed: vitamin B9 showing 201.35μg/day consumption (95% CI 125.32–277.38; I2: 98%; p < 0.01), vitamin B12 with 5.61μg/day (95% CI 2.53–8.70; I2: 52%; p = 0.12), and vitamin C with 139.67 mg/day (95% CI 59.33–220.02; I2: 96%; p < 0.01) (Fig. 4). Mineral consumption was reported by 637.32 mg/day of calcium (95% CI 288.54–986.11; I2: 98%; p < 0.01), and 9 mg/day iron intake (95% CI 2.28–15.71; I2: 95%; p < 0.01) (Fig. 5).
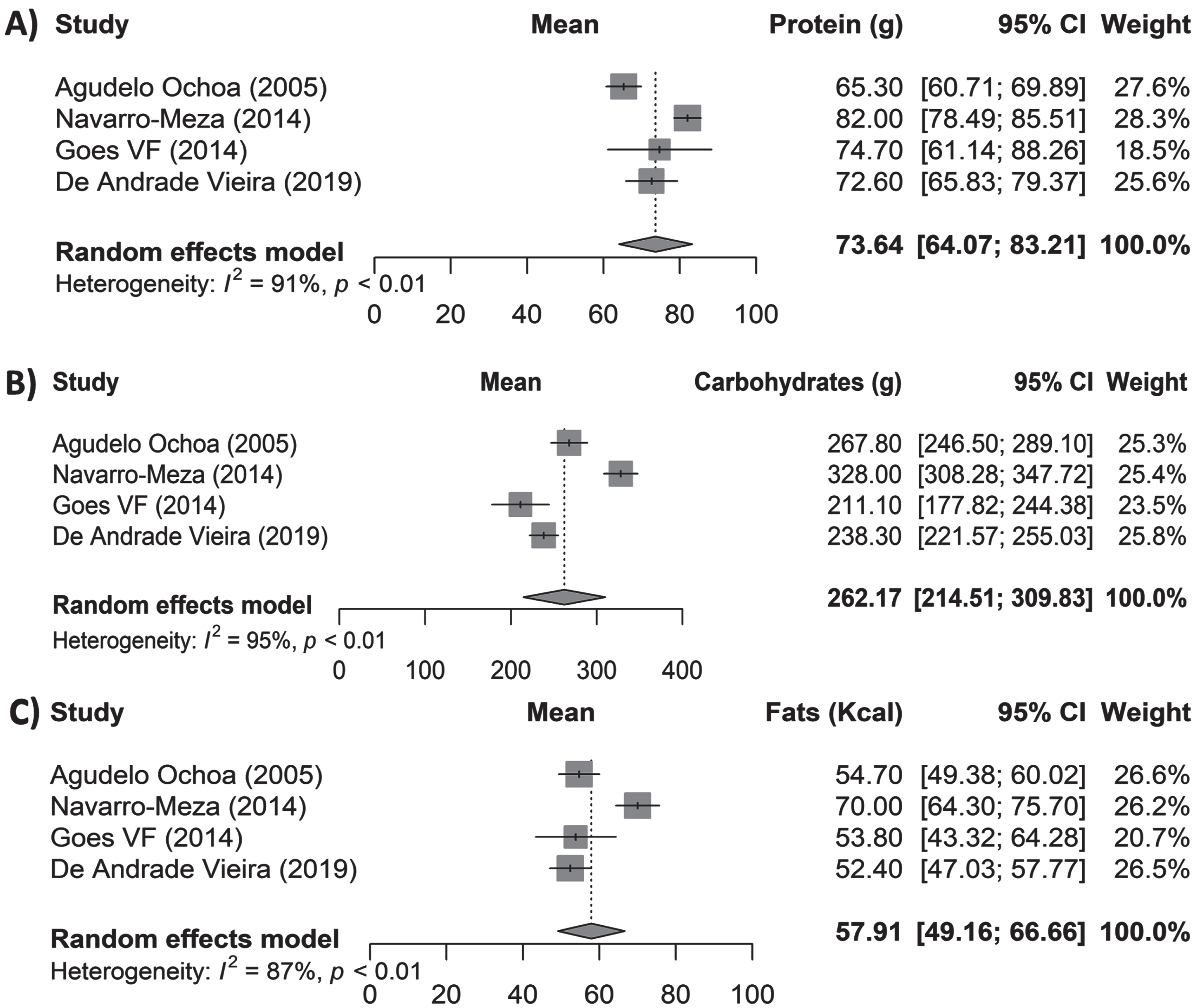
Daily intake of macronutrients in subjects with MCI and dementia in LAC.
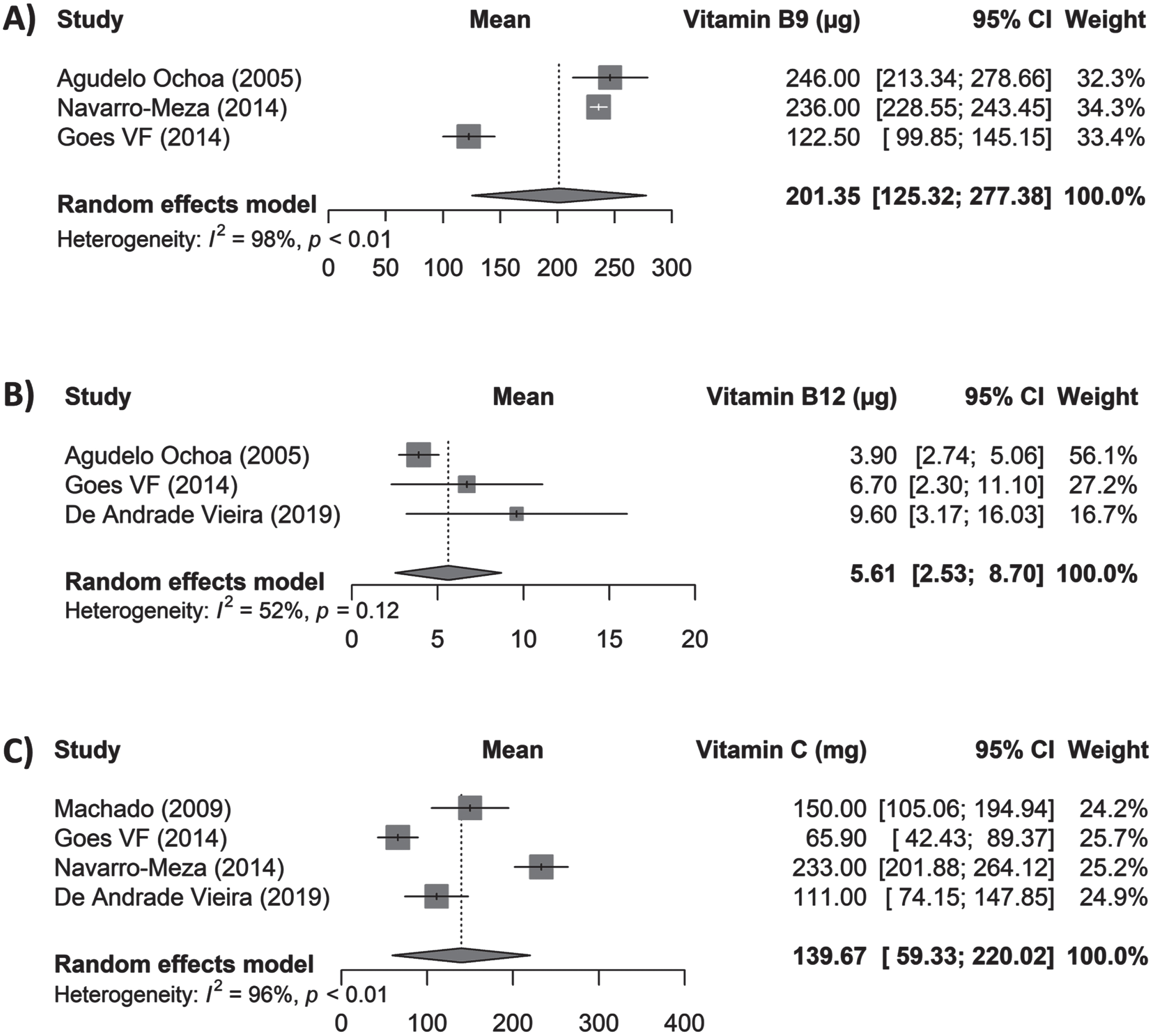
Daily intake of micronutrients in subjects with MCI and dementia in LAC.
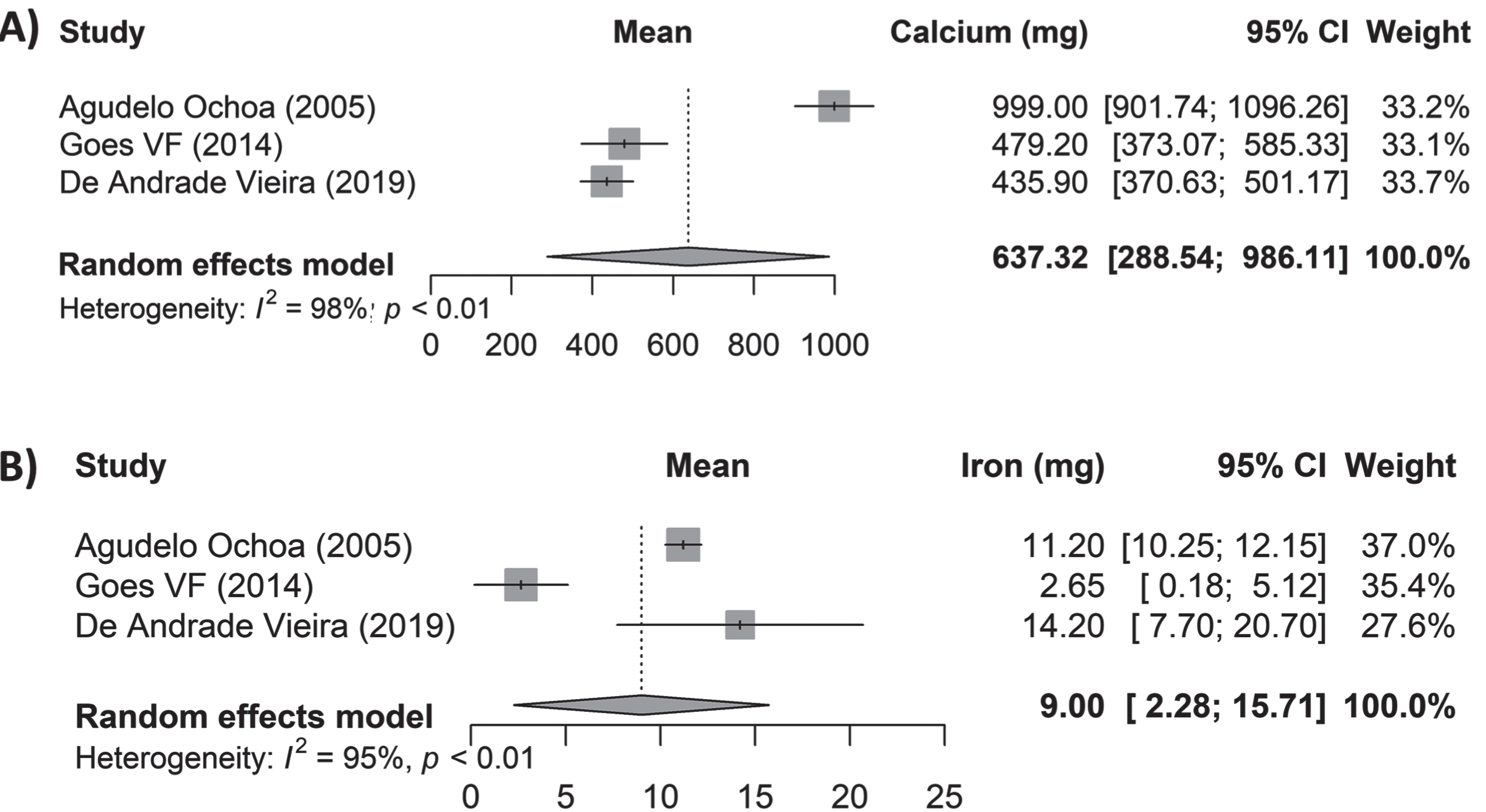
Daily intake of calcium and iron in subjects with MCI and dementia in LAC.
Food groups
Five studies described and distributed data on food consumption in groups. Machado et al. reported that the most consumed food group was grains, with 91% of patients with AD in the mild stage and 61% in the moderate stage consuming this food group daily. As for the group of protein foods, more than 50% of the patients consumed them daily, mainly red meats. Additionally, patients showed a low intake of fruits and vegetables [20]. Navarro-Meza et al. reported that patients with AD and PDD eat significantly less vegetables (156±4 versus 405±2; p < 0.001), fruits (156±4 versus 405±2; p = 0.037) oil and fats (4±4 versus 22±2; p = 0.002). However, they eat more cereal (438±44 versus 293±27; p = 0.017), high in fats-animal source foods (ASF) (14±3 versus 3±2; p = 0.024), whole milk (228±30 versus 40±19; p < 0.001), and alcohol (0.92±0.06 versus 0.089±0.040; p = 0.033), in comparison with a control group without neurodegenerative diseases [23].
Pastor-Valero et al. found out that individuals with cognitive impairment significantly eat less fruit and vegetables (p < 0.001) and fish (p < 0.001) compared to subjects without cognitive impairment [14]. According to França et al., participants who ate fewer vegetables (4 times per week) were 47.6% more likely to develop a cognitive deficit (OR: 0.524; 95% CI: 0.310–0.877; p = 0.045) [26]. Lastly, consuming < 5 servings /day of fruits and vegetables was positively associated with suspected cognitive impairment (OR: 2.02; 95% CI: 1.05–2.99; p = 0.048), as reported by Martinez et al. [27] (Table 1).
DISCUSSION
The main findings of this systematic review were that the mean energy consumption was similar to previous studies from populations with the same conditions [28, 29], but differences in the diet of LAC subjects with MCI and dementia were found, with this characterized in macronutrients by an increased intake of protein and carbohydrates and a possible adequate intake of fats, and in micronutrients by an increased intake of vitamin B12 and vitamin C but a decreased intake of vitamin D. Additionally, a low intake of fruits and vegetables was reported in this population. To the best of our knowledge, this is the first study that presents and summarizes data on food consumption, macro- and micronutrients in people with a cognitive deficit living in LAC.
To date, an optimal energy intake in individuals with dementia and MCI has not been established; however, recommendations by the National Institute of Health (NIH) mention that calorie intake can vary from 1500 to 2000 kcal in the elderly [30]. We found an average of 1598 kcal; this is similar to Mexican and Brazilian older adult population without cognitive dysfunction, that reported a calorie intake ranging from 1500 to 1600 kcal [31, 32]. The total energy described in the included studies in this systematic review ranged from 1238 to 1826 kcal. Medeiros et al. reported the lowest energy consumption among participants. This could be probably because the studied population was recruited from a home care program for older persons [22]. Nevertheless, some other studies from higher income countries have reported a total energy consumption greater than 2000 kcal among older people with a risk of dementia [33, 34].
Even though, studies that evaluate MCI and dementia patient’s nutrition tend to focus more on the report of micronutrients consumption, little literature on macronutrients can be found with inconsistent results, overall, studies conclude that moderate carbohydrate, fats, and protein consumption associates with a lower risk of dementia [33]. High and low percentages of macronutrients are related to adverse effects on MCI development [35]. The pooled average obtained in this study showed that the subjects with dementia and MCI have a diet composed of a high intake of protein and carbohydrates and a possible adequate intake of fat [36]. This is important because some studies have shown that eating protein is associated with lower chances of developing cognitive decline at an older age [37, 38]. On the other hand, a high consumption of carbohydrates, especially refined carbohydrates, compromises both physical and brain health [39, 40]. This was found in animal models and in subjects with AD carrying apolipoprotein E ɛ4 allele (APOE ɛ4) [41]. Fats consumption was found to be moderate in this systematic review; this acts as a protective factor against risk of dementia and cardiovascular health diseases [42]. However, it is important to note that not all types of fat may act as a protector. It has been reported that higher saturated fatty acids in dietary intakes are correlated with increased risks of AD and cognitive decline [43]. On the other hand, polyunsaturated fatty acids generate beneficial effects, as is the case with omega-3 fatty acids. This is because they are part of the neuronal structure and synapses. A study showed that consumption of polyunsaturated fatty acids (omega-3) generated a reduction in the rate of cognitive decline and better cognition in patients with MCI [44].
Among micronutrients, there was a high intake of vitamins B12 and C but a deficiency of vitamin B9 consumption. Various micronutrients have been shown to have beneficial effects, particularly attributed to their neuronal potential effect during neural stimulation and reduction of neurodegenerative processes [45]. In fact, it has been postulated that vitamin supplementation can be an adjuvant intervention for dementia patients [46]. The intake of vitamins and minerals in this study was obtained from the food consumption reports of the study population and not from supplements. A deficiency of Vitamin A (retinol) has been found among subjects with MCI and dementia [47]. It has been reported that vitamin A deficiency contributes to the pathogenesis of AD by stimulating the production of amyloid-β [48, 49]. Navarro-Meza et al. [23], Goes et al. [25], and De Andrade Vieira et al. [21] reported a lower consumption of vitamin A, when compared patients between controls or nutritional recommendations [30, 36]. However, we were not able to plot vitamin A because there is missing data regarding the units used for its measurement.
Vitamin B9 (folate) is another vitamin that plays an important role in Tau protein hyperphosphorylation, this process is related to neurodegenerative diseases [50, 51]. Besides, evidence shows that a daily intake of vitamin B9 (≥400μg/d) reduces risk of AD occurrence [52]. Pooled data from studies showed low intake of vitamin B9 in the study population; this deficiency intake was consistent among all the studies that reported data on this vitamin. In contrast, an adequate intake of vitamin B12 was found among included studies; deficiency of this vitamin linked to cognitive dysfunction [53]. This result can be due to the higher intake of protein that individuals with MCI and dementia from LAC have, according to our data. However, malabsorption of this vitamin has been noted in older adults [54]. Then if a final deficiency of vitamin B12 is found, a replacement therapy has been recommended in order to improve neurocognitive function [55]. Vitamin C (ascorbic acid) is an antioxidant vitamin that plays a defensing role against free radicals and prevents lipid peroxidation [56]. In our study, we found an adequate intake of this vitamin in the study population. However, it has been reported that, despite an adequate dietary intake of vitamin C, plasmatic levels of this vitamin might be reduced in this population [57]. Therefore, supplementation could protect against neurocognition deterioration [58].
Some minerals were evaluated, such as calcium and iron, which both have been found to be positively associated with cognitive function in older persons and to participate in the pathological process of dementia [59, 60]. Results from this study showed a low intake of calcium (637 mg/day) and an adequate intake of iron (9 mg/day). However, in other populations with MCI in Australia, a higher intake of iron was reported in 45 mg/day [61]. Iron dyshomeostasis, along with amyloid-β and tau pathologies, has been linked to AD [62]. It is critical to better understand the links between dementia and mineral intake, especially in the early stages of the disease when interventions are most likely to be effective. Scientific evidence has described a homeostasis dysregulation of calcium linked to brain aging and dementia physiopathology, known as “calcium hypotheses” [63]. In fact, results from The Shanghai Aging Study indicated that those older adults with lowest calcium intake (<339.1 mg/day) had the highest incidence rates of dementia [64].
The low consumption of vegetables and fruits was very consistent in the included studies. This is important because they are a great source of vitamins and minerals. Some studies have reported that lower consumptions of vegetables and fruits may be associated with cognitive impairment in older adults [65, 66], so this finding would support this acerbation. In addition, it has been found a reduce in amyloid-β aggregation in diets characterized by a high intake of plant foods and in compounds from specific plant-derived compounds [67, 68].
In addition, differences in the type of food consumption are found among countries; it has been reported that in European countries, there is a higher intake of meat, dairy, fats and oils, fruits, and sweets; meanwhile, in North America, eggs, vegetables, and roots and tubers are the most frequently consumed [69]. There are some similarities and differences in the LAC. In fact, the Latin American Study of Nutrition and Health showed dietary variations among countries, and this variation in the diet was also found among a range of ages. It was reported that adult population from Brazil showed high consumption of fish and seafood and processed meat in comparison to the population from Chile, which had a high consumption of processed meat and a low consumption of whole grains, nuts, and seeds [70]. Although Mexico was not included in this study, it is described that consumption of corn-based products, beans, and other legumes are fundamental foods in the diet of the Mexican population [71]. Despite these differences, it is important to note that there is a lack of studies on dietary variations among older adults from LAC.
Diet plays an important role at each stage of life. Some foods have been shown to have neuroprotective properties, especially some vitamins B [72], antioxidants (vitamins E and C) [73], and polyunsaturated fatty acids (PUFA) (omega-3 s) [74], which are the nutrients for which evidence has been reported in AD patients. In fact, among the studies evaluated in this systematic review, Navarro et al. noted that those individuals that were used as controls had higher consumption of vitamins such as C, A, E, and folic acid [23]. Together with other evidence, it can be suggested that the lack of these nutrients during life could lead to the development of AD.
Controlling nutrient imbalances in people living with MCI or dementia should be a priority for health professionals. This will help to prevent or control other diseases that are risk factors for the occurrence of cognitive dysfunction. When considering strategies, such as nutritional education, to improve the nutrition of people living with dementia in LAC, it is important to consider not only educational interventions for the principal carer and family members but also the staff working in nursing homes, hospitals, and private care homes.
We performed a systematic review of all relevant and available literature on the type of diet in subjects with dementia and cognitive impairment living in LAC for this study. Some limitations were that the studies focused only on AD, PDD, and different cognitive impairments. We did not find studies focused on other types of dementia, such as vascular dementia. This will be important to explore due to the high frequencies of obesity and overweight in LAC population. Another limitation was high heterogeneity, when each macro- and micronutrient was plotted in the forest plot, this could be due to a methodological difference among studies such as dietary assessments, population analyses, and differences in the reported units. We were not able to plot some data because of the lack of information in the measurement units used in the studies. Data on diet in older adults with MCI and dementia from LAC is limited; six of the nine included studies were performed in Brazil; additionally, the populations of Mexico, Colombia, and Chile were analyzed; however, no LAC population from central America was evaluated.
CONCLUSION
We found a nutritional deficiency that can affect the quality of life of subjects with MCI and dementia from LAC, characterized by a low intake of fruits and vegetables, an elevated intake of protein and carbohydrates, and a possible adequate intake of fats as well as in vitamin B12, C, and iron, but a low intake of vitamin B9 and calcium. These deficiencies can be easily corrected through nutritional education and an adequate detection and nutritional control by health professionals.
Footnotes
ACKNOWLEDGMENTS
We are grateful to Julio Vega for help us with the statistical analysis.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Data underlying this work are available upon reasonable request. Requests for data should be addressed to corresponding author.