
Abstract
Background:
Cognitive decline is a major reason for dependence and resource use in long-term care.
Objective:
We explored whether social activities may prevent cognitive decline of older residents of long-term care facilities.
Methods:
In a routine care cohort, 3,603 residents of long-term care facilities were assessed on average 4.4 times using the interRAI-Long-Term-Care-Facilities instrument which includes frequency of participation in social activities of long standing interest over the last 30 days and the Cognitive Performance Scale. Linear mixed models repeated measures analyses were performed corrected for age, sex, physical activity, Activities of Daily Living, mood, and health indicators.
Results:
Social activity was associated with cognitive preservation over time. This association was stronger in those with no or mild cognitive impairment at baseline, relative to those with moderate to severe impairment. Participation in specific social activities such as conversing and helping others showed a similar positive association. The relation between social activity and cognitive impairment appeared to be bi-directional.
Conclusions:
The protective effects of social activity offer a window of opportunity to preserve cognitive functioning in long-term care residents.
Keywords
INTRODUCTION
Many factors have been associated with cognitive decline throughout the ageing process. The Lancet Commission for Dementia Prevention, Intervention and Care, estimated that 12 potentially modifiable risk factors—lower education, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, alcohol intake, poor sleep, air pollution, and low social participation—may account for 40% of worldwide dementia risk [1]. A recent review and a meta-analysis supported conclusions of an association between social relationships and cognitive function respectively incident dementia [2, 3]. The role and impact of social participation in cognitive decline, however, is not understood very well [2].
Cognitive decline in long term care residents is common. Webber et al. reported 24.6% cognitive decline over a year in long term care residents in Ontario, Canada, defined as 1 point decline on the Cognitive Performance Scale [4]. How do social participation of residents and their cognition relate? Gerritsen et al. reported an average score of 3.27 on the Revised Index of Social Engagement (RISE) in Dutch nursing home residents. Residents with relative intact cognition had a higher average of 4.01 indicating more social engagement [5]. Yoon et al. reported a moderately strong association of 0.58 between social engagement and time involved in social activities in South Korean nursing home residents [6]. There appears to be little literature on participation in (specific) social activities in nursing homes.
Observational cohort studies suggest that a social activity in late life might delay incidence of dementia in community dwelling older persons [3, 8]. Considering the challenges of randomized trials in this area, quasi-experimental research may be informative. COVID-19-related social isolation measures, introduced to contain the disease, resulted in a reduction in social participation, which affected some, such as those living alone, more than others. The evidence on how this affected dementia risk may become evident in future years. However, some studies have found that social restrictions may have affected cognitive function. A review of the effect of COVID-19-related isolation on the cognition of people with dementia found that 60% of 15 studies reported a detrimental effect on cognition [9]. Angevaare et al. compared changes in cognitive functioning of care home residents pre and post COVID-19 lockdown. They did not find clinically relevant negative effects [10]. Possibly, staff mitigated the negative effects.
The causal pathway of the association has not yet been determined. The presence of cognitive impairment could decrease one’s interest in and ability to participate in activities involving social and cognitive skills. Therefore, the association may reflect the effect of cognitive impairment on social and cognitive activities rather than the effect of social activities on risk of cognitive decline. Nevertheless, the SUPERBRAIN trial among older persons without dementia reported improved neuropsychological status at 24 weeks of follow-up of participants in the multi-domain intervention including social activities through multiple group meetings weekly and additional scheduled monthly social activities [11]. Despite this promising finding it remains unclear to what extend it can be attributed to the social elements of this multi-domain intervention.
Finally, most research on this relationship has been carried out in community dwelling older persons without cognitive impairments at baseline. Little is known of whether possible protective effects extend to older persons in residential care facilities, many of whom suffer from cognitive impairments. Social activity may potentially be a target for intervention. Also it is not clear what type of social activity would be beneficial.
The main objective of this study was to explore whether participation in social activities has an effect oncognitive functioning in long term care residents with and without cognitive impairment. Secondly, we explored the effects of specific social activities (e.g., conversing, reminiscing about life, helping others, visits by family members) were on cognitive functioning.
METHODS
This study used data of the Dutch and Flemish interRAI routine care cohort of residents in long-term care facilities [12], in which the interRAI Long Term Care Facilities comprehensive instrument was used to collect data and inform care decisions.
Data use followed the EU General Data Protection Regulation. Ethical clearance was provided by the Amsterdam University Medical Centres –location VU University under no 2021–0358. After de-identification, data were transferred to the interRAI database at the Amsterdam University Medical Centres –location VU University. Up until 2014, an opt-out procedure was applied in compliance with the EU General Data Protection Regulation. Older people were informed in general terms that their data could be used for research purposes by their practice nurses and through their practices’ newsletters, websites, and posters, and they had the possibility to object. As off 2014, most facilities adopted an opt-in informed consent policy.
We reported according to the STROBE guidelines for cohort studies (Supplementary Material).
Setting and residents
The facilities constituted a mix of residential care housing and nursing homes. The first offer mainly unskilled support in daily living and medical support from external physicians, the latter having skilled in-home (para)medical teams. Any home that used the interRAI observation instrument between 2006 and 2014 was included. The residents’ characteristics did not differ from the Dutch national average regarding age, gender, and need of daily support. The Dutch and Flemish interRAI database consists of residents in Long Term Care Facilities who undergo regular assessments, on average every six months, to determine their functioning and well being on domains pertaining to physical and psychosocial health.
We included all older residents 65 years or older with at least two assessments. We excluded residents with (i) missing data on the Cognitive Performance Scale (CPS) and on the social activity measures at baseline, (ii) residents with a maximum CPS score at baseline of 6, indicating very severely impaired cognition, as further decline could not be measured.
In addition, from the eligible residents we used all routine care assessments at intake and follow up being at least 30 days apart from each other to allow enough time for a potential change in cognitive functioning to develop. Discharge assessments without clinical information and assessments done because of acute change of functioning were omitted from the analyses.
Measurement
The interRAI-LTCF instrument was developed by the interRAI network (http://www.interrai.org), as a comprehensive assessment instrument for care professionals in long term care facilities. The basis is a minimal data set of approximately 250 items covering a person’s demographics, physical and cognitive functioning, psychosocial and emotional well-being, living environment, service use, and medical diagnoses and conditions. The instrument integrates information from direct observation, medical records, and communication with the person under assessment and their informal care network. Care professionals use assessment software that generates a dashboard with (i) a patient profile, (ii) 14 validated scales for monitoring the status and triggers, and (iii) 26 Collaborative Action Points to guide care planning (CAPs) [13]. CAPs alert the assessor to specific problems that can be addressed in care planning either to maintain or to improve functioning. The scales support monitoring of functional dependence, cognition, mood, pain, aggressive behavior, social engagement, pressure ulcer risk, risk on unplanned hospitalizations, and health instability.
Most interRAI items have, by default, three days look back period. The items of the LTCF instrument demonstrated a high interrater reliability in multiple studies and in different countries [14–16].
Main variables
Cognitive functioning was measured using the CPS [17]. The CPS is based on the following items: 1) Cognitive skills for daily decision-making; 2) Short-term memory; 3) Making oneself understood; 4) Eating performance. The scores range from 0 (no impairment) to 6 (very severe impairment). The CPS was validated against the Mini-Mental State Examination[18] and can capture cognitive decline over the course of several assessments. Details of the CPS decision tree can be found at https://interrai.org/applications/status-and-outcome-scales/.
The main independent variable was the amount of participation in social activities in the facility. This was defined as the person engaged in social activities that have been of long-standing interest to him or her. The activities may be quite varied and should be counted as long as they involve interaction with at least one other person. Examples include attending meetings of informal clubs, playing bingo or card games, attending religious services or informal discussion groups. It was assessed by asking the person, direct care staff, and family, if available. Possible responses to this item were 0: never, 1: more than 30 days ago, 2 : 8 to 30 days ago, 3 : 4 to 7 days ago, 4: in the last 3 days and 8: not assessable. Non assessable measurements were considered asmissing.
To improve the frequency distribution, five original answering categories were re-organized to create three categories: 0: no activity in the past thirty days; 1:between four and thirty days; and 2: last three days.
Supplementary to the global measure of social activity used in the main statistical model, we explored the association with participation in specific activities. We utilized activities that were unequivocally social in nature: conversing, reminiscing about life, helping others, and going on trips or going shopping. The responses to these activities were analyzed dichotomously: participation in any activity in the last three days- yes/no.
In addition, we measured physical activity, ADL performance with the interRAI Long Form scale, pain with a 4-level scale, mood with the Depression Rating Scale (DRS), and Deafness and Blindness Severity Index (DbSI) [19–22].
Statistical analysis
Descriptive statistics were used to describe the sample characteristics on sociodemographic-, functional- and clinical status. The dependent variable was the CPS scale.
Initially, a three-level linear mixed model analysis was applied to assess the longitudinal relationship between participation in social activities and cognitive functioning, i.e., assessments were clustered within residents and residents were clustered within residential facilities. Adding the level of residential facility did not improve the model fit, effectively reducing the model from three to two levels. All models only included random intercepts. We used a random intercept at the level of the resident as we have repeated measurements with correlated observations within persons. All variables in the model were fixed.
Missing at follow up was handled by the linear mixed models. An important feature of the linear mixed model technique is that it allows for missing measurements as well as varying time intervals between the measurements, which suits the routine-care data structure. Slope estimates can be calculated if at least one follow up measurement is present. On average 4.4 assessments per resident werepresent.
Besides a crude analysis, we also performed an adjusted analysis adding variables that were considered potentially important in the relation between social activities and cognitive performance (i.e., age, gender, marital status, history of mental illness, loneliness, diagnosis of Alzheimer’s or other dementia, physical activity, ADL capacity (interRAI Long Form scale), the DbSI, a 4-level pain scale, and the DRS [19–22]. Additionally, the same analyses were performed for participation in the specific social activities.
Because the regression coefficient from a linear mixed model analysis reflects both the within- and between subject effects, we also performed crude and adjusted hybrid model analyses. In a hybrid model, separate regression coefficients are estimated for the within- and between subject effects. The within subject effects are of particular interest as these reflect the potential impact of social activity on cognitive functioning. In addition, all models were also stratified based on the baseline measurement of cognitive impairment, resulting in two groups:1) intact cognition or mild impairment (CPS 0–2), and 2) moderate to severe impairment (CPS 3–5). Finally, we performed sensitivity analyses to further explore the direction of the relationship. We ran cross lagged models: one estimating the effect of social activity on cognition measured at the next assessment, and one vice versa, estimating the effect of cognition on social activity measured at the next assessment (data not shown).
In the regression analyses, the values of the CPS scale were inverted to aid interpretation; a higher value indicates a more intact cognition. Standardized effect sizes were calculated mimicking Cohen’s D by dividing the regression coefficient of a particular model by the standard deviation at baseline of the dependent variable (CPS scale) of the population subset included in that model.
For all analyses, a significance level of p < 0.05 was used and all analyses were performed using STATA version 14.
RESULTS
After applying exclusion criteria 3,603 residents from 42 homes, and 18529 assessments were eligible for the analysis. The average number of assessments per resident was 4.4 (SD: 3.45) and the average number of days between assessments was 142 (SD: 80.19). Figure 1 shows the flowchart of participants and measurements after applying each in- or exclusion criterion. Baseline demographics and clinical status are described in Table 1. The average decline on CPS score between two assessments was 0.049 points. (p < 0.001) The average decline was larger in men (0.057) than in women (0.047). (p < 0.001) The standard deviation of the CPS scores was 1.643 in the entire sample, 1.248 in the baseline cognitively preserved group, and 1.099 in the baseline cognitively impaired group.
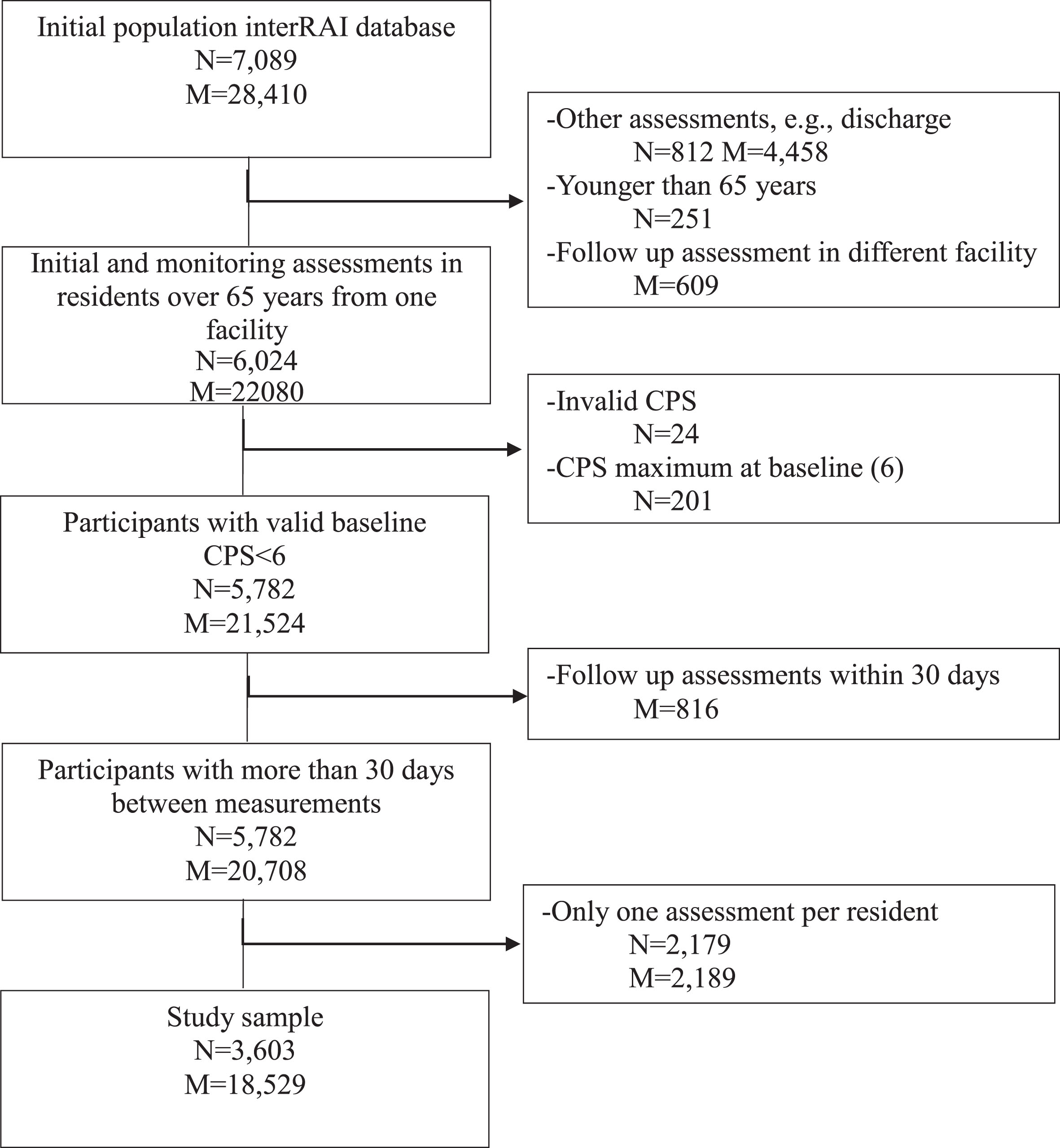
Flowchart on number of participants (N) and number of measurements (M).
Baseline characteristics of study population N = 3603
Linear mixed model (social participation and cognitive functioning)
More frequent participation in social activities was associated with preserved cognitive functioning over time, in the entire sample (Table 2). The positive value of the beta signifies better cognition for the group of residents which frequently participate in social activities, compared to the reference group which did not engage in any social activity.
Hybrid model: within and between persons effects of social participation
In both the within and between persons effects models, positive effects were found for the group that had participated in a social activity in the past three days as well as for the group with social participation in the last 4–30 days, compared to the reference group with no activity (Table 2). In general, between persons effects were stronger than within persons effects, although confidence intervalsoverlapped.
Association between participation in social activity in the last 30 days and cognition
Reference group comprises persons without social activity in the last 30 days, *Significance level: p < 0.05. CPS, Cognitive Performance Scale (0–6), CPS values were inverted to aid interpretation. Thus, positive values indicate a better cognitive functioning. †Adjusted for age, gender, marital status, history of mental illness, loneliness, diagnosis of Alzheimer’s or other dementia, physical activity, ADL capacity (interRAI Long Form scale), the Deafness and Blindness Severity Index, a 4-level pain scale, and the Depression Rating Scale.
Associations of specific social activities with cognitive functioning
For all but one of the social activities, participation was found to be significantly associated with preserved cognitive functioning (Table 3). The three models for which an overall effect was found, conversing, helping others, and going on trips/shopping, all showed within persons effects as well. From these, helping others demonstrated the strongest protective effect. In the between-persons models, all four social activities were significantly associated with preserved cognitive functioning.
Association between participation in specific social activities in the last three days and cognitive functioning. Within and betweenperson associations
Reference group comprises persons without participation in the social activity in the last 3 days. *Significance level: p < 0.05. CPS values were inverted to aid interpretation. Thus, positive values indicate better cognitive functioning. †Adjusted for age, gender, marital status, history of mental illness, loneliness, diagnosis of Alzheimer’s or other dementia, physical activity, ADL capacity (interRAI Long Form scale), the Deafness and Blindness Severity Index, a 4-level pain scale, and the Depression Rating Scale.
Stratification by baseline cognition with hybrid model
In the overall model, stratified on baseline cognitive impairment, both the cognitively intact and impaired groups showed a significant association of participation in social activity in the last three days and preserved cognitive functioning. The within persons model showed a protective effect of social activity only in the group with none or mild cognitive impairment at baseline. This association was not found in the participants with moderate to severe cognitive impairments at baseline. In the between persons model, the pattern was inverse, with the cognitively impaired group exhibiting an association between participation in social activity and preserved cognitive functioning which was not present in the cognitively intact group (Table 4).
Association between participation in social activity in the last 30 days and cognition, stratified for better (0–2) and worse (3–5) cognitive functioning at baseline
Reference group comprises persons without social activity in the last 30 days. *Significance level: p < 0.05. CPS values were inverted to aid interpretation. Thus, positive values indicate a higher level of cognition. †Adjusted for age, gender, marital status, history of mental illness, loneliness, diagnosis of Alzheimer’s or other dementia, physical activity, ADL capacity (interRAI Long Form scale), the Deafness and Blindness Severity Index, a 4-level pain scale, and the Depression Rating Scale.
Dose-response relationship
A dose-response relationship was seen in the association between frequency of participation in social activities and cognitive functioning. Standardized effect sizes of the different independent variable categories, as expressed by Cohen’s D, are shown in Fig. 2.
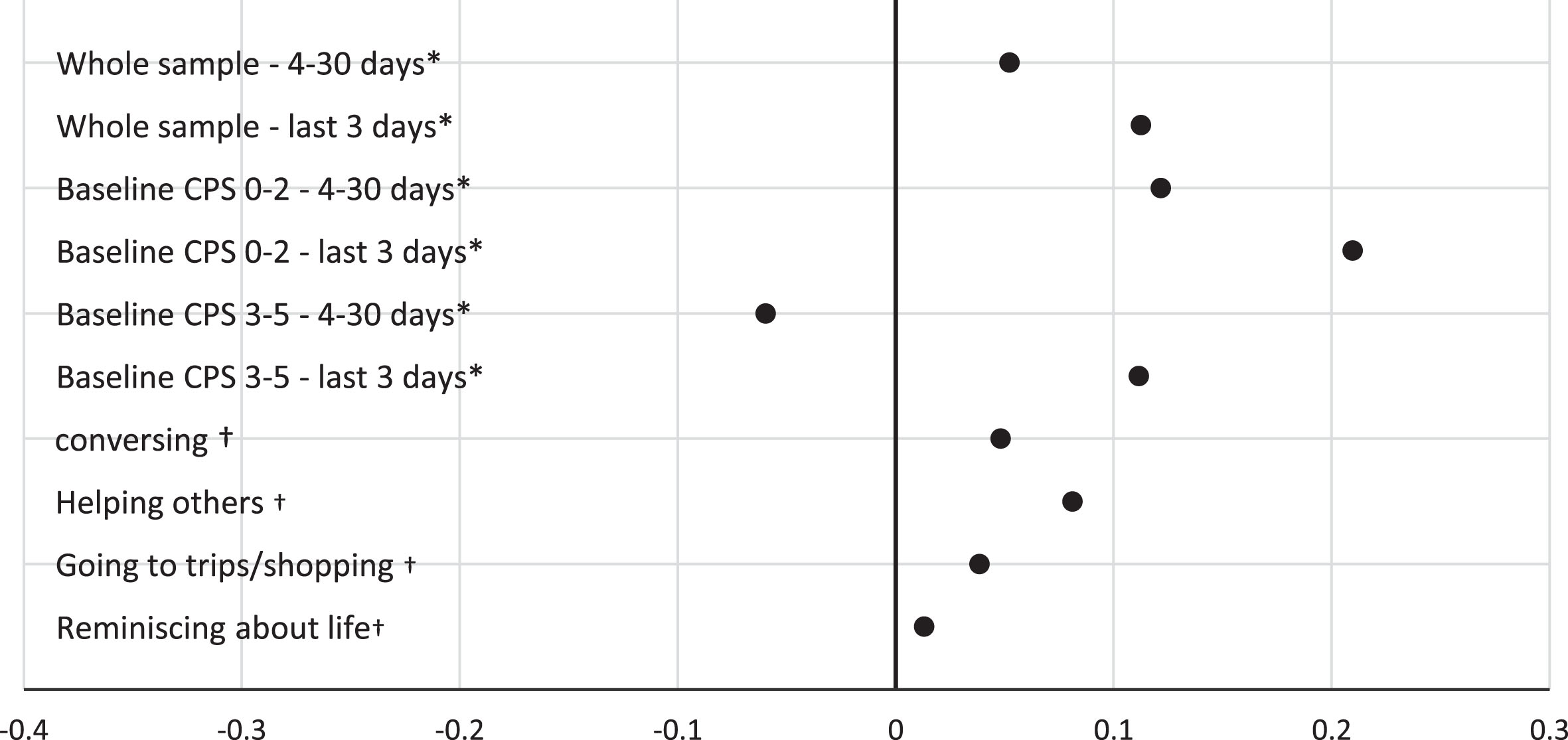
Forest plot of effect sizes (expressed as Cohen’s D) of the different frequencies and types of social activity, stratified for better (0–2) and worse (3–5) levels of cognitive functioning at baseline. *Reference group comprises persons without social activity in the last 30 days. †Reference group comprises persons without activity in the last 3 days. Estimates are based on within person models.
DISCUSSION
Short summary of main findings
We found a synchrony of change between social activities and global cognitive functioning of older residents of long-term care facilities which suggest the presence of a protective effect of social activities. Both social activity in general and specific social activities: conversing, reminiscing about life, helping others, and going on trips or going shopping had this positive relationship with cognitive functioning. This effect was particularly present in residents with no or only mild cognitive impairment at baseline. The effect size could be qualified as small but still relevant. The bi-directional nature of the relationship was confirmed in sensitivity analyses.
Strengths
This study had several strengths. We demonstrated a possible protective association between social activity and further cognitive deterioration, whereas previous studies examined associations between social activity and the incidence of cognitive impairment or dementia. Furthermore, the present study is unique due to the use of high-quality usual-care data on the under explored population of older residents of long-term care facilities many of whom already have cognitive impairment. Our routine care study was hardly affected by selection- and drop out bias, resulting in a high external validity. The cognitive assessment used in this study is a relevant measurement for a routine care population since it is highly correlated with likelihood of a person being dependent on help with ADL due to cognitive impairment [18]. Finally, the fact that an association was found using a relatively global measure of cognitive functioning such as the CPS adds to the confidence that the effect of social activity on cognitive decline is robust.
Limitations
One possible limitation is that some of the social activities might serve as a proxy measurement for physical activity. Although we controlled for the hours of physical activity there may have been an impact of specific physical activities that we did not capture.
Furthermore, since routine care data was used, the timing of the assessments was not as precise as in a rigorously run research cohort. Fortunately, the linear mixed model technique used in this study produces robust estimates while allowing intervals to vary between measurements.
Additionally, although we included several scales as indicators of functioning across different domains in this observational study, we cannot completely rule out confounding bias.
Lastly, we could not include interaction between residents and staff as a form of social activity in the analysis. We did control for ADL level, which is a main determinant of the amount of staff-resident interaction.
Participation in social activities and cognitive functioning
Our findings substantiate the interpretation by Fratiglioni et al. that an active lifestyle seems to have protective effects on cognitive functioning in older adults [7]. Whereas Fratiglioni et al. were not able to disentangle the effects of social, mental, and physical domains of activity, our findings suggest that social activity specifically has a positive association with global cognitive functioning in individuals [7]. This association was hardly affected by controlling for physical activity which suggests the effect of social activity is not a result of concurrent physicalactivity.
Kuiper et al. found a protective association between social engagement and the incidence of dementia in community-dwelling older persons. Our findings extend this protective association to residential settings populated with very frail older persons most of whom already suffer from some cognitive decline [23].
Social engagement varies among long term care residents and across countries [5, 24–26], being relatively low in Japan and South Korea and higher in the US, Denmark, and the Netherlands [6, 26]. In the South Korean longitudinal aging study, transitioning from engagement to non-engagement was associated with lower cognitive function among men only. Not being part of a senior center was associated with decreased cognitive function among both genders, while not being part of a religious group affected women only [27]. These findings have implications for policymakers as interventions targeting improved cognitive function may be more effective when gender-specific predictors are taken into consideration.
A recent review distinguished social activity, social networks, and social engagement and all three were positively associated with global cognitive function [2]. Additional associations with specific cognitive domains were found as well but these varied across these social indices [2].
The COVID-19 lockdowns greatly impacted social behaviors and reflect a natural experiment in a way. Mixed findings were reported ranging from increased incidence of dementia associated with social isolation [3] to no clinically relevant impact whatsoever [4, 10]. In these natural experiments it remains hard to control for the effects of possible measures by staff and family to mitigate the impact of the lockdowns. We would need more detail and integrate such local mitigation measures into impact analyses.
Larger association in cognitively intact or only mildly impaired residents
The results suggest that the relationship between participation in social activities and cognitive functioning differs based on the amount of cognitive impairment at the baseline measurement. In participants with no or mild cognitive impairments at baseline, higher participation in social activities seems to be associated with preserved cognitive functioning, whereas this effect was not found in participants with moderate to severely impaired cognition at baseline.
Practice and policy
The results provide evidence for a policy of facilitating social activities of long-standing interest, especially for the sizeable portion of residents with relatively intact cognitive performance. It may have consequences for the staff mix that needs to include sufficient professionals that can facilitate social activities. Any intervention that helps to preserve cognitive functioning, can positively impact both residents’ well being and their dependence on assistance in activities of daily living [22–25]. This may also impact the type and intensity of staff involvement and consequently the cost of long-term care resources for our society [28].
Future research
Future research may focus on further substantiating the potential protective effects of social activities in long term care facilities. The effect of specific social activities and possible interventions may be further explored. The effect sizes of the associations found in this study were relatively small, especially for within person effects. Therefore, it remains to be seen whether interventions that increase social activity will be powerful enough to protect cognitive decline in a meaningful way.
The conclusions of this study are of special importance regarding the COVID-19 pandemic during which residents of long-term care facilities were quarantined and physically and socially isolated. Although first reports range from limited impact [4, 10] to increased incidence of dementia [3], future studies may try to specify for whom forced physical and social isolation of residents of long-term care facilities may have impacted their functioning.
Conclusions
In this longitudinal cohort study, we found indications of protective effects of social activities on cognitive decline, especially in people with only mild cognitive impairment at baseline. Although the effects were small, it may provide a window of opportunity to test interventions to postpone cognitive decline that focus on increasing social activities. Controlled interventions should confirm protective impact of social activities on cognitive decline.
AUTHOR CONTRIBUTIONS
Hein van Hout (Conceptualization; Data curation; Project administration; Resources; Supervision; Writing – review & editing); Jack A Pieters (Conceptualization; Formal analysis; Writing – original draft; Writing – review & editing); Milou MJ Angevaare (Formal analysis; Methodology; Supervision; Writing – review & editing); Jos WR Twisk (Formal analysis; Methodology; Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors gratefully thank the Care organizations and software companies that provided the data.
FUNDING
This work was supported by Amsterdam UMC, Amsterdam, the Netherlands.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Viewing the data supporting the findings of this study are available on request from the corresponding author. The data remain on a secured server due to privacy and ethical restrictions.