
Abstract
Background:
There is increasing recognition of cognitive and pathological heterogeneity in early-stage Alzheimer’s disease and other dementias. Data-driven approaches have demonstrated cognitive heterogeneity in those with mild cognitive impairment (MCI), but few studies have examined this heterogeneity and its association with progression to MCI/dementia in cognitively unimpaired (CU) older adults.
Objective:
We identified cluster-derived subgroups of CU participants based on comprehensive neuropsychological data and compared baseline characteristics and rates of progression to MCI/dementia or a Dementia Rating Scale (DRS) of ≤129 across subgroups.
Methods:
Hierarchical cluster analysis was conducted on individual baseline neuropsychological test scores from 365 CU participants in the UCSD Shiley-Marcos Alzheimer’s Disease Research Center longitudinal cohort. Cox regressions examined the risk of progression to consensus diagnosis of MCI or dementia, or to DRS score ≤129, by cluster group.
Results:
Cluster analysis identified 5 groups: All-Average (n = 139), Low-Visuospatial (n = 46), Low-Executive (n = 51), Low-Memory/Language (n = 83), and Low-All Domains (n = 46). Subgroups had unique demographic and clinical characteristics. Rates of progression to MCI/dementia or to DRS ≤129 were faster for all subgroups (Low-All Domains progressed the fastest > Low Memory/Language≥Low-Visuospatial and Low-Executive) relative to the All-Average subgroup.
Conclusion:
Faster progression in the Low-Visuospatial, Low-Executive, and Low-Memory/Language groups compared to the All-Average group suggests that there are multiple pathways and/or unique subtle cognitive decline profiles that ultimately lead to a diagnosis of MCI/dementia. Use of comprehensive neuropsychological test batteries that assess several domains may be a key first step toward an individualized approach to early detection and fewer missed opportunities for early intervention.
INTRODUCTION
Although Alzheimer’s disease (AD) research has moved toward earlier detection [1], our understanding of cognitive heterogeneity within the pre-mild cognitive impairment (MCI) phase or early stages of the AD continuum remains underdeveloped. Statistical data-driven approaches such as cluster analysis or latent profile analysis applied to neuropsychological test data have identified multiple mild cognitive impairment (MCI) subtypes [2–8] beyond the traditional amnestic/nonamnestic distinction [9, 10]. In various studies, amnestic (i.e., predominant memory impairment) [2, 5–8], dysnomic (i.e., predominant language impairment) [2, 7], dysexecutive (i.e., predominant attention/executive functioning impairment, often with concurrent memory difficulties) [2, 7], and mixed/multidomain MCI subtypes [3, 8] have emerged. These empirically-derived MCI subtypes can have unique associations with cerebrospinal fluid and neuroimaging biomarkers, as well as different trajectories of functional decline and risk of dementia [2, 12]. Overall, data-driven methods outperform conventional methods of diagnosis in capturing individuals with MCI who have positive (i.e., abnormal) AD biomarkers, progress to dementia, or have AD pathology at autopsy [3].
Few studies have specifically examined the heterogeneity of cognitive performance within cognitively unimpaired (CU) individuals to determine if there are specific cognitive phenotypes that have increased risk of developing MCI and dementia. Studies that have examined combined CU and MCI participants in analyses have typically only classified CU participants into high- and low- average cognition groups [3, 13] or into a single “subtle cognitive impairment” group [7]. An exception is a recent study that used a statistical approach to classify CU participants into cognitive phenotypic groups and then examined the association of these subtypes with modifiable vascular, physical activity, and diet factors [14]. This approach identified high-average and average groups, as well as Low-Memory and Low-Executive groups [14]. However, this study did not examine longitudinal outcomes and, to our knowledge, no studies focusing only on CU participants have longitudinally examined the impact of cognitive phenotypes on rates of progression to MCI/dementia. Therefore, the aim of our study was to identify cluster-derived groups of CU participants based on comprehensive neuropsychological test data and to compare their baseline characteristics and rates of progression to MCI/dementia.
METHODS
Participants
Participants included 365 CU individuals (i.e., without a consensus diagnosis of MCI, “impaired not MCI,” or dementia), aged 50+, who were enrolled in the longitudinal study at the University of California San Diego (UCSD) Shiley-Marcos Alzheimer’s Disease Research Center (ADRC). Inclusion criteria included stable health status, English- or Spanish-speaking, available study partner, and no history of major stroke/neurologic condition, severe psychiatric illness, substance abuse, or learning disability. Participants diagnosed with “impaired, not MCI”, MCI, or dementia at baseline were excluded from the current study. Participants completed the neuropsychological testing in their preferred language of English or Spanish. The protocol was reviewed and approved by the UCSD institutional review board. Written informed consent to participate in the study was obtained from all participants or a designated caregiver.
Neuropsychological measures
Individual neuropsychological measures from participants’ baseline visit representing the domains of memory (California Verbal Learning Test (CVLT) or CVLT-II Learning Trials 1–5; CVLT or CVLT-II Long Delay Free Recall; Wechsler Memory Scale-Revised [WMS-R] Logical Memory Delay), language (Boston Naming Test [BNT] or Multilingual Naming Test [MINT]; Category Fluency [animals, fruits, vegetables]; Letter Fluency [F, A, S];), processing speed and executive functioning (Trail Making Test Parts A and B; modified Wisconsin Card Sorting Test [WCST] categories completed), and visuospatial functioning (Block Design; Clock Drawing Test [CDT] command) were included in the cluster analysis. Consistent with our previous work, prior to analyses, each raw test score was converted to a demographically-adjusted (age, sex/gender, education) z-score [3]. Z-scores were determined based on the difference between the observed score and expected score divided by the standard error of measurement. Regression coefficients to determine the expected score were derived from a subset of the larger UCSD Shiley-Marcos ADRC sample who were considered to be robust CU participants. These robust CU participants (n = 355) had at least 1 year of follow-up data (mean follow up = 6.6 [SD = 5.6] years) and were considered CU via consensus diagnosis for the duration of their participants in the ADRC study. The robust CU participants were demographically well-matched to the participants in the current study (mean age = 71.6 years [SD = 8.5]; mean education = 14.9 years [SD = 3.7]; 59.4% female; 92.1% White).
Outcome measures
As part of the research protocol, participants completed annual clinical, neurologic, and neuropsychological evaluations [15, 16]. Clinical status (CU, MCI, or dementia) was determined at each visit based on a multidisciplinary (2 neurologists and a neuropsychologist) consensus diagnosis [3]. In addition to longitudinal clinical diagnosis, an outcome of Dementia Rating Scale (DRS) score ≤129 [17] was also examined given that a consensus diagnosis of MCI or dementia may be more heavily weighted for memory impairment and may not be as sensitive to capturing progression of nonamnestic profiles.
Analyses
A hierarchical cluster analysis was conducted on individual neuropsychological z-scores at baseline for all CU participants. Next, a discriminate function analysis was conducted to test whether the individual neuropsychological measures could predict cluster-group membership. Analysis of variance and χ2 tests compared cluster-derived groups on baseline demographic and clinical characteristics including: age, sex/gender (male or female), educational level, race, and ethnicity (Hispanic or non-Hispanic); Mini-Mental State Exam (MMSE) and DRS for general cognition; presence of a subjective memory complaint (yes or no); Apolipoprotein E (APOE) ɛ4 carrier status (carrier or noncarrier), history of diabetes (yes or no) and hypertension (yes or no); Functional Activities Questionnaire (FAQ) [18] and Clinical Dementia Rating – Sum of Boxes (CDR-SB) [19] to measure everyday functioning; and the specific neuropsychological test z-scores.
Cox regression adjusting for age, education, sex/gender, and ethnicity (Hispanic or non-Hispanic) determined the risk of progression to (a) consensus diagnosis of MCI or dementia, or (b) a DRS score ≤129 within an average of 6.25 years (range 1–20 years) by cluster group. Kaplan-Meier curves were used to depict the rate of progression to MCI/dementia or DRS score ≤129 over time. Follow-up time was restricted to 20 years or less given the low number of participants with data after 20 years (n = 8). Participants who did not progress to MCI/dementia or DRS score ≤129 during their follow-up period were censored at their last visit.
RESULTS
The following sample characteristics were observed across all participants: mean age = 71.93 (SD = 7.51) years; mean education = 15.44 (SD = 3.15) years; 55.9% female; 93.4% White; and 15.6% Hispanic/Latino/a/x/e. Cluster analysis resulted in 5 cognitive groups: 1)
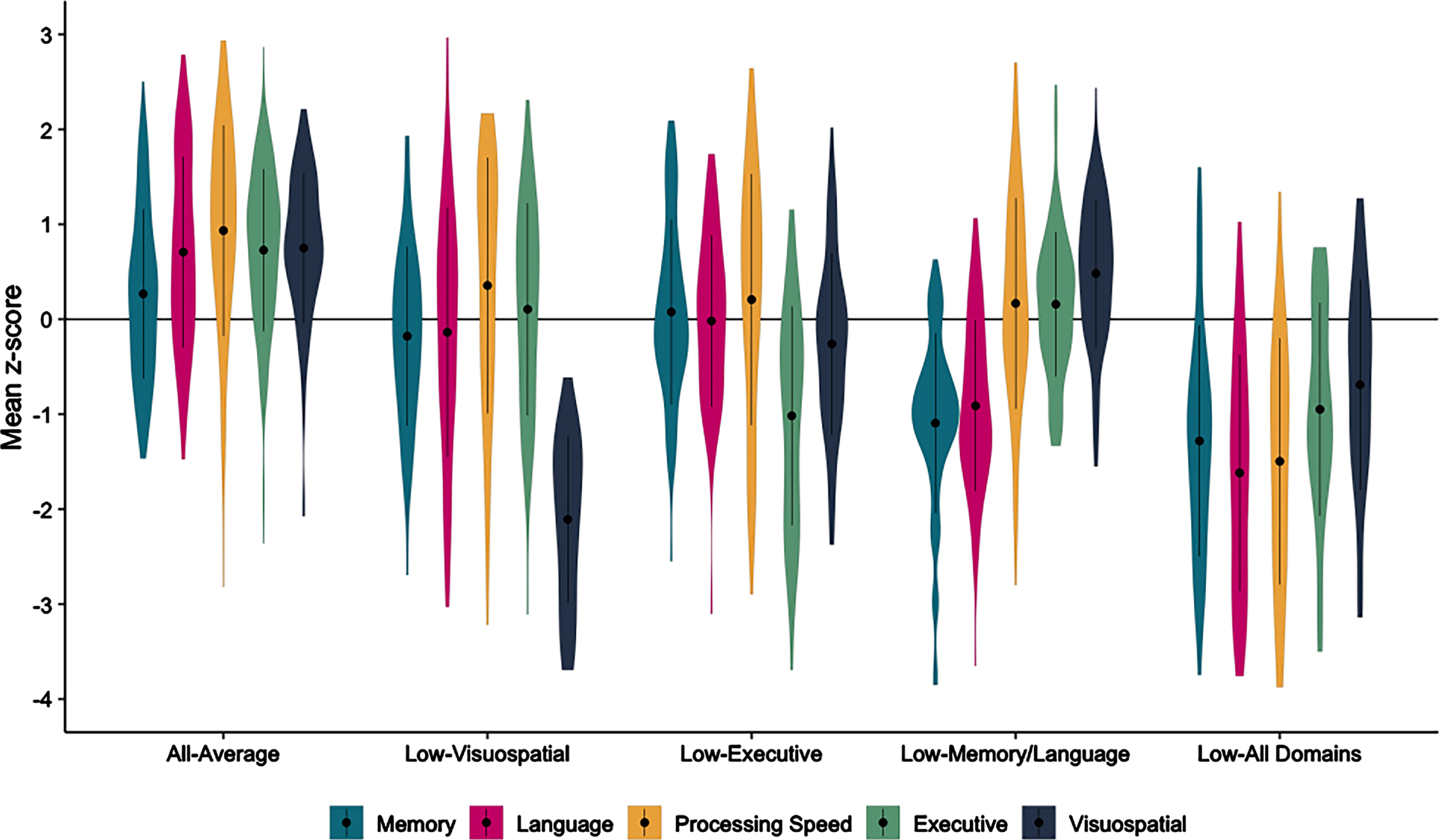
Baseline neuropsychological scores across the cluster-derived groups of cognitively unimpaired participants. Mean neuropsychological domain scores, rather than individual scores, are used for the figure only: Memory (CVLT Learning and Delay, Logical Memory Delay), Language (BNT/MINT, Category Fluency, Letter Fluency), Processing Speed (Trails A), Executive Functioning (Trails B, WCST Categories), Visuospatial (Block Design, CDT Command).
Table 1 shows the demographic, clinical characteristics, and specific mean neuropsychological test scores by cluster-derived group. Briefly, groups did not significantly differ on age, proportion of participants tested in Spanish, or diabetes status. The All-Average group had the highest proportion of APOE ɛ4 carriers yet performed the best on the MMSE and DRS at baseline. The Low-Visuospatial group had the fewest years of education and were more likely to be female and Hispanic/Latino/a/x/e. The Low-Executive group had the most difficulty in everyday functioning. The Low-Memory/Language group had the greatest proportion of participants with a subjective memory complaint and had a slightly longer duration of follow-up. The Low-All Domains group was more likely to be non-White (2.2% Black/African American, 6.5% Asian, 6.5% other race) and have a history of hypertension.
Baseline demographic, clinical, neuropsychological, and biomarker characteristics of the cluster-derived groups
Data are summarized as mean (standard deviation), unless otherwise indicated. APOE, apolipoprotein E; MMSE, Mini-Mental State Exam; DRS, Dementia Rating Scale; FAQ, Functional Activities Questionnaire; CDR-SB, Clinical Dementia Rating –Sum of Boxes; CVLT, California Verbal Learning Test; LM, Logical Memory; BNT, Boston Naming Test; MINT, Multilingual Naming Test; CDT, Clock Drawing Test. Superscript indicate differences (p < 0.05) between cluster-group pairwise comparisons. asignificantly different than All-Average; bsignificantly different than Low-Visuospatial; csignificantly different than Low-Executive; dsignificantly different than Low-Memory/Language; esignificantly different than Low-All Domains.
Across the sample, 85 participants progressed from CU to a diagnosis of MCI or dementia over an average of 6.89 years (SD = 4.83). Cox regressions, adjusting for age, education, sex, and ethnicity showed that relative to the All-Average group, the Low-Visuospatial (hazard ratio [HR] 2.39, 95% CI [1.03, 5.56], p = 0.044), Low-Memory/Language (HR 4.37, 95% CI [2.24, 8.51], p < 0.001), and Low-All Domains (HR 7.21, 95% CI [3.59, 14.48], p < 0.001) groups had greater risk of progressing to MCI/dementia. The Low-Executive group was also twice as likely to progress to MCI/dementia compared to the All-Average group, but did not statistically differ (HR 2.03, 95% CI [0.88, 4.70], p = 0.096). Examining all group comparisons, relative to the All-Low Domains group, the Low-Visuospatial (HR 0.33, 95% CI [0.15, 0.71], p = 0.005) and Low-Executive (HR 0.28, 95% CI [0.13, 0.61], p = 0.001) groups were less likely to progress to MCI/dementia, and while the Low-Memory/Language group was also less likely to progress, it did not statistically differ (HR 0.61, 95% CI [0.34, 1.06], p = 0.080). The Low-Executive and Low-Memory/Language groups did not differ from the Low-Visuospatial group, and the Low-Memory/Language group was more likely to progress relative to the Low-Executive group (HR 2.15, 95% CI [1.03, 4.48], p = 0.043).
Across the sample, 73 participants progressed to a DRS score of ≤129 over an average of 5.54 years (SD = 4.47). The pattern was similar to progression to MCI or dementia, with the Low-Memory/Language (HR 3.70, 95% CI [1.80, 7.56], p < 0.001) and Low-All Domains (HR 5.79, 95% CI [2.74, 12.27], p < 0.001) groups at greater risk of progression to a DRS ≤129 than the All-Average group, along with the Low-Executive group (HR 2.82, 95% CI [1.26, 6.29], p = 0.012). The Low-Visuospatial group was also twice as likely to progress to DRS ≤129 compared to the All-Average group, but did not statistically differ (HR 2.02, 95% CI [0.80, 5.06], p = 0.135). Examining all group comparisons, relative to the All-Low Domains group, the Low-Visuospatial (HR 0.35, 95% CI [0.15, 0.82], p = 0.016) was less likely to progress to a DRS ≤129. The Low-Executive (HR 0.49, 95% CI [0.23, 1.02], p = 0.057) and Low-Memory/Language (HR 0.64, 95% CI [0.34, 1.21], p = 0.166) groups were also less likely to progress relative to the All-Low Domains group but did not statistically differ. The Low-Visuospatial, Low-Executive, and Low-Memory/Language groups did not differ from each other on risk of progression to a DRS ≤129. Figure 2 shows the Kaplan Meier curves for rates of progression to MCI/dementia diagnosis and DRS ≤129.
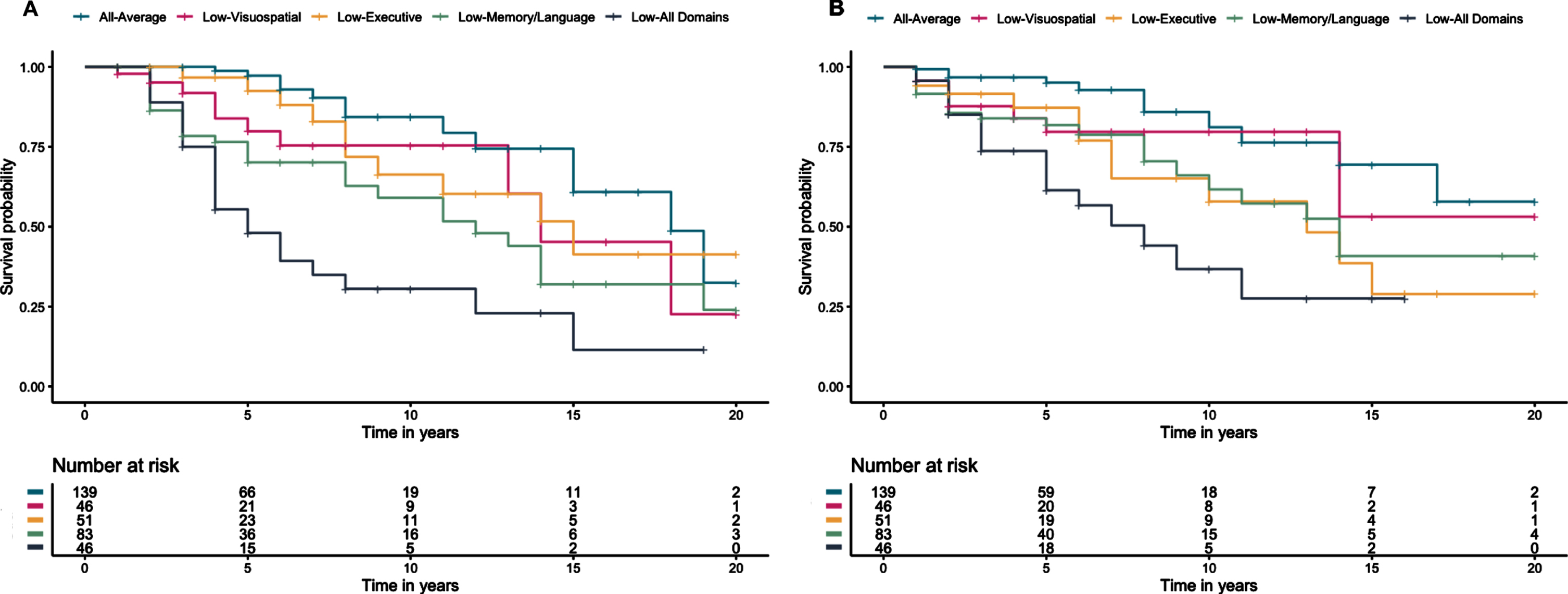
Kaplan Meier curves for time to (A) progression to consensus MCI/dementia diagnosis and (B) progression to a Dementia Rating Scale score ≤129 since baseline visit.
DISCUSSION
In this study we identified five cluster-derived groups within participants classified as cognitively unimpaired (i.e., without a consensus diagnosis of MCI/dementia). While several of the cluster groups were consistent with those observed in other studies (All-Average, Low-Executive, Low-Memory/Language) [14], Low-Visuospatial and Low-All Domains groups also emerged. The All-Average group was the largest cluster group, as expected for a CU sample, followed by the Low-Memory/Language group, a profile consistent with an early “typical” AD presentation. Across the groups, the Low-All Domains group progressed to MCI/dementia the fastest, and the All-Average group progressed the slowest; the Low-Visuospatial, Low-Executive, and Low-Memory/Language groups progressed at intermediate and similar rates, though the adjusted HRs for the Low-Memory/Language group was higher than both the Low-Visuospatial group and Low-Executive groups and statistically differed from the Low-Executive group for the progression to MCI/dementia outcome. These rates of progression reflect the possibility that there are multiple pathways or initial cognitive symptoms that ultimately lead to greater risk of a diagnosis of MCI/dementia. The pattern of results was similar when a DRS ≤129 threshold was used to assess progression to cognitive impairment, possibly because total DRS score was considered when making the consensus diagnosis. However, on this outcome, the Low-Visuospatial, Low-Executive, and Low-Memory/Language groups did not statistically differ. This suggests that the DRS may be more sensitive to capturing nonamnestic profiles relative to the consensus diagnosis.
Unlike previous studies that sought to derive cognitive subtypes in CU-only participants, our study included visuospatial measures and our results demonstrate the potential value of including these measures in a cognitive test battery when trying to determine whether someone is at increased risk for cognitive decline or progression to MCI/dementia. The Low-Visuospatial group we identified may be consistent with findings from recent work examining the heterogeneity of tau distribution in AD, which identified a group of individuals with a slow-progressing, posterior pattern of tau deposition, likely with predominant visuospatial impairment [20]. Although they had a greater proportion of female and Hispanic/Latino/a/x/e participants than the other groups, importantly, the Low-Visuospatial group was not substantially younger than the Low-Memory/Language group (or any other group), suggesting that it is likely not solely capturing individuals with posterior cortical atrophy which tends to have a younger onset than typical AD [21]. Similarly, the Low-Executive group did not differ from other groups in regard to age and did not progress as quickly as may occur in dysexecutive AD or frontotemporal dementia [22, 23]. However, even within these clusters, there is likely significant heterogeneity of pathologies and future work will need to replicate these clusters and explore underlying AD and non-AD biomarker profiles.
Despite being considered cognitively unimpaired, a cluster group with relatively widespread cognitive weaknesses emerged. This Low-All Domains group performed well on the MMSE and DRS and did not evince particularly high proportions of subjective memory complaints or everyday functioning difficulties (despite greater rates of vascular disease) and this may have contributed to their being classified as CU instead of MCI or dementia by consensus at their initial visit. Additionally, the regression weights used for the z-scores were derived from a robustly normal group, which may have resulted in these z-scores being especially sensitive to subtle weaknesses compared to a standard score based on published norms that generally have a less strict criteria for inclusion into the normative sample. The Low-Memory/Language group had the highest proportion of individuals with a subjective memory complaint, consistent with findings that self-reported memory concerns may emerge in the preclinical phase of AD [24] and be associated with cognitive decline, particularly in an ADRC sample [25]. The Low-Executive group had the worst everyday functioning, though their mean scores on the FAQ and CDR-SB still reflect minimal functional difficulty. This slightly worse functioning, however, is consistent with studies showing that executive function is more strongly associated with real-world instrumental activities of daily living than other cognitive domains [26].
Our study has several strengths including the use of a comprehensive neuropsychological test battery, thorough consensus diagnostic/classification procedures, and the opportunity to examine up to 20 years of longitudinal data on some individuals. One consistent challenge in determining the earliest cognitive changes associated with future declines is the potential for circularity of the predictor (e.g., lower cognitive scores) and the outcome (e.g., MCI/dementia). In the current study, we aimed to work around aspects of this circularity by including two outcome variables (consensus MCI/dementia and DRS score) and, importantly, examining the longitudinal rates of progression. Few previous studies have sought to identify and understand very early subtle cognitive decline profiles specifically within CU participants, despite the field’s growing focus on earlier, preclinical stages of AD [27]. We chose to examine only CU participants and this may have allowed more empirically-derived groups to emerge compared to studies that have combined CU and MCI participants and found only one or two CU phenotypes [3, 28]. This is only an initial study, and more work is needed to replicate these findings in larger, more diverse, and community-based cohorts. Additionally, future projects should examine biomarker and neuropathological data to better understand the underlying etiologies of decline across the cognitive phenotypes. While an ‘amnestic’ presentation has historically been thought to be linked with AD pathology and other non-amnestic presentations thought to represent non-AD phenotypes [10], the current results suggest there are many cognitive phenotypes that predict progression, likely regardless of the underlying (and likely multiple) pathologic underpinnings.
Our results add to a growing literature documenting heterogeneity in the earliest cognitive and pathological presentations associated with AD and related disorders [29, 30]. Despite unique cognitive profiles, participants with subtle memory/language, executive, and visuospatial weaknesses all declined at faster rates than the All-Average group. These results have important implications for early identification of individuals at risk for MCI/dementia. Given that the same classification approach may not be optimal for everyone, determining profiles of subtle cognitive difficulties in CU individuals and implementing neuropsychological test batteries that assess each domain may be a key step towards an individualized approach to early detection with the goal of decreasing missed opportunities for early intervention.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the U.S. Department of Veterans Affairs Clinical Sciences Research and Development Service (Career Development Award-2 1IK2CX001865 to K.R.T.; and Merit Award 1I01CX001842 to K.J.B), the NIH (P30 AG062429 to K.R.T, D.P.S, and M.W.B.; R03 AG070435 to K.R.T.; R01 AG049810 to M.W.B.; R01 AG063782 to K.J.B.), and the Arizona Alzheimer’s Consortium and Arizona DHS (CTR057001 to E.C.E.).
D.P.S. serves as a paid consultant for Biogen, Inc. and Takeda Pharmaceuticals. M.W.B. is a consulting editor for the Journal of the International Neuropsychological Society, a Senior Editor for Journal of Alzheimer’s Disease, and receives royalties from Oxford University Press.