
Abstract
Background:
Alzheimer’s disease (AD) is the most common type of dementia, causing progressive decline of memory, thinking, and behavior, impairing daily functioning. Early AD (eAD) includes mild cognitive impairment (MCI) due to AD and mild AD dementia.
Objective:
The aim of this study was to investigate symptomatic treatment prevalence and treatment patterns in eAD.
Methods:
Embase, MEDLINE, and EBM Reviews were searched in November 2021 for observational studies reporting symptomatic treatment patterns in eAD. The range of patients receiving treatment was collated. Risk of bias was assessed using the Joanna Briggs Institute (JBI) prevalence tool. Two independent reviewers screened the records, one performed data extraction and quality assessment while a second checked.
Results:
Twenty-one studies (prospective and retrospective cohorts, cross-sectional studies, and a survey) were included. Population size ranged from 23 to 2,028. Worldwide, 18 to 35% of patients diagnosed with MCI due to AD received any AChE inhibitor (three studies; n = 631), 7 to 8% memantine (two studies; n = 229), and 9% combination therapy (one study; n = 402). Patients receiving no treatment ranged from 41 to 54% (two studies; n = 733). Worldwide, in mild AD dementia patients, 13 to 89% received any AChE inhibitor (six studies; n = 3,715), 1 to 21% memantine (five studies, n = 3,527), and 0.4 to 39% combination therapy (four studies, n = 3,018). Patients receiving no treatment ranged from 9 to 26% (five studies, n = 4,073).
Conclusion:
Limitations in reporting led to unclear risk of bias. The results reveal a pattern of use of symptomatic treatment in eAD beyond approved labels and highlights the opportunity for new consensus guidelines to inform clinical practice.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) and other dementias are a major and increasing global health challenge, with an estimated 50 million people currently living with dementia [1]. AD is the most common cause of age-related dementia, accounting for an estimated two thirds of cases [2].
AD is characterized by cognitive deficits resulting in progressive decline in memory, reasoning, thinking, and behavioral symptoms that impair a person’s ability to function in daily life [2]. AD progresses along a continuum with three phases: preclinical disease, mild cognitive impairment (MCI), and clinically apparent dementia (mild, moderate, and severe AD dementia) [3]. Early clinical stages of AD, hereafter referred to as early AD (eAD), are defined as MCI due to AD (also referred to as prodromal AD) and mild AD dementia. The early indicators are decline in mental capabilities in the absence of impaired performance on objective cognitive testing. MCI describes the earliest symptomatic stage of cognitive impairment in which at least one cognitive domain is impaired to at least a mild extent whilst functional capacities are relatively preserved [4]. By contrast, dementia is defined as cognitive impairment of sufficient magnitude to impair independence and affect daily life. Symptoms evolve over time and the pace at which symptoms advance from mild to moderate to severe dementia differs between individuals. Short periods of memory loss characterize the early clinical stage of the disease with interference in some everyday activities as dementia progresses to a mild stage [2].
A meta-analysis featured in a 2018 North American practice guideline update reported that MCI due to AD affects 6.7% of 60–64-year-olds and 25.2% of 80–84-year-olds [5]. A study to characterize severity of AD amongst a primarily Caucasian population in the Framingham Heart study found 50.5% of people with AD had mild AD dementia [6].
Currently, no cure exists for AD, and until the recent approval of aducanumab in the US [7], no treatments existed to slow its progression. However, therapeutic interventions exist to temporarily slow symptoms and improve cognitive function. A summary of the current guidelines for the treatment of AD in the US, Canada, and Europe is presented in Supplementary Table 1. There are currently no recommendations for pharmacological management of MCI due to AD. For dementia due to AD, two classes of symptomatic treatments have existing approvals in Europe and the US, the acetylcholinesterase (AChE) inhibitors - donepezil, galantamine and rivastigmine, and the N-methyl-D-aspartate (NMDA) antagonist, memantine [7–9]. AChE inhibitors are considered as first line treatment for mild-moderate AD dementia, acting to increase acetylcholine and improve memory [9]. As AD dementia progresses to the moderate-severe stage, memantine is recommended as an add-on therapy.
Recent results from surveys on the clinical management of MCI due to AD and mild AD dementia suggest the use of symptomatic treatment in both patient populations [10, 11]; however, neither report actual patient data. Similarly, recent data from clinical trials in eAD report baseline use of AChE inhibitors and memantine which is not necessarily in line with current regulatory EU and US approvals or clinical guidelines [12–14]. Therefore, our review aims to describe the current real-world use of AD symptomatic treatments in patients with MCI due to AD and mild AD dementia, with an emphasis on understanding the extent of AD symptomatic treatment use beyond approved labels.
METHODS
The systematic review was pre-registered, and the protocol can be accessed at https://www.crd.york.ac.uk/prospero/ (ID: CRD42022296104). Reporting aligns to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline [15] and the checklists can be found in Supplementary Tables 2 and 3.
Search, study selection, and data extraction
Searches were conducted in Embase, MEDLINE, and EBM Reviews via Ovid on November 30, 2021, to identify studies reporting on symptomatic treatment prevalence and treatment patterns in the earlier clinical stages of AD dementia. Symptomatic treatments included were AChE inhibitors such as donepezil, galantamine, and rivastigmine and the NMDA antagonist, memantine. Searches were restricted to 2009 onwards to capture the most recent evidence from the last decade and reflect current practice. This was informed by a pragmatic review that found the earliest included study was from 2009 [16]. Searches were not restricted by language. A search filter was used to identify observational studies and real-world data studies and as such would also identify systematic reviews of observational studies and real word data studies. The full search strategies are presented in Supplementary Tables 4 to 6. Reference lists of included studies and relevant systematic reviews were searched to identify additional studies. The main Embase strategy was independently peer reviewed by a second analyst, based on the Peer Review of Electronic Search Strategies (PRESS) [17].
Two reviewers independently performed title and abstract screening, followed by full paper screening using the inclusion and exclusion criteria presented in Supplementary Table 7. To summarize, full publications of observational studies (prospective/retrospective observational studies, registries, medical record reviews, and surveys) were included if they reported pharmacological symptomatic treatment patterns of patients in the early clinical stages of AD. Studies that reported reasons for treatment outside guidelines were also included. Data extraction was performed by one reviewer, and all data were checked by a second reviewer. Any disagreements were resolved by consensus or discussion with a third reviewer.
Risk of bias assessment
Study quality assessment was performed by one reviewer and checked by a second reviewer using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Prevalence Studies [18]. Any disagreements were resolved by consensus or discussion with a third reviewer. The JBI Critical Checklist for prevalence data addresses important issues of internal and external validity to consider when assessing validity of prevalence (or frequency) of treatment use regardless of study design [19].
Data analysis
A formal narrative synthesis was planned based on the reporting guideline for Synthesis Without Meta-analysis (SWiM) in systematic reviews [20]. All included studies were summarized by country and grouped according to disease stage (MCI due to AD or mild AD dementia). A summary of study design, patient characteristics, treatment pattern, and risk of bias was presented. To capture treatment patterns, the range of treatment use was reported for ‘any AChE inhibitor monotherapy’ (donepezil, rivastigmine, or galantamine), memantine monotherapy, AChE inhibitor plus memantine combinations, other combined therapies, or no symptomatic treatment. To indicate the certainty of the evidence, the findings of the synthesis were reported alongside the risk of bias, number of studies, and the study size (or range). To summarize the best quality data, studies at high risk of bias were extracted (Supplementary Table 9 (Risk of bias assessment) and 10 (Study results)) but not considered further in the data ranges for analysis and synthesis. Studies that reported on drug dose only in populations receiving symptomatic treatment were reported separately as they were not directly comparable to treatment pattern data.
Patient and public involvement
This study did not have any direct patient or public involvement.
RESULTS
Following database searching, 1,463 records were retrieved: 369 duplicates removed and 1,094 screened at title and abstract. A total of 159 records were sought for full paper screening and of these, 21 met the criteria for inclusion in the review (Fig. 1). The 138 records excluded at full paper screening are listed together with the reason for exclusion in Supplementary Table 8. A summary of the characteristics of the included studies is presented in Table 1. Prospective and retrospective cohorts, cross-sectional studies, and a survey were all represented; however, most studies were prospective and focused on European populations. Nearly all the studies (86%) reported on mild AD dementia, four (19%) reported on MCI due to AD [21–24], and two reported on early AD (a mixed population of MCI due to AD and mild AD dementia) [25, 26]. AChE inhibitor monotherapies were the most frequently reported treatment (91% of studies) followed by AChE inhibitors and memantine (33%), memantine monotherapy (33%), or no treatment (33%). Population size ranged from 23 [27] to 2,028 [28] (IQR = 514.5). Patient characteristics were not widely reported. Where reported, mean age was broadly consistent across studies (70.8 [26] to 79.3 years [29]) whereas the proportions of gender were variable (4.4% [27] to 64.4% males [21]). Mean severity (MMSE) ranged from 22.6 [30] to 27.0 [21] with most studies reporting mean MMSE in the middle of the range for mild AD dementia (mean 23.2 [21, 31–35]). No studies reported on the reasons for discordance between guidelines and clinical practice.
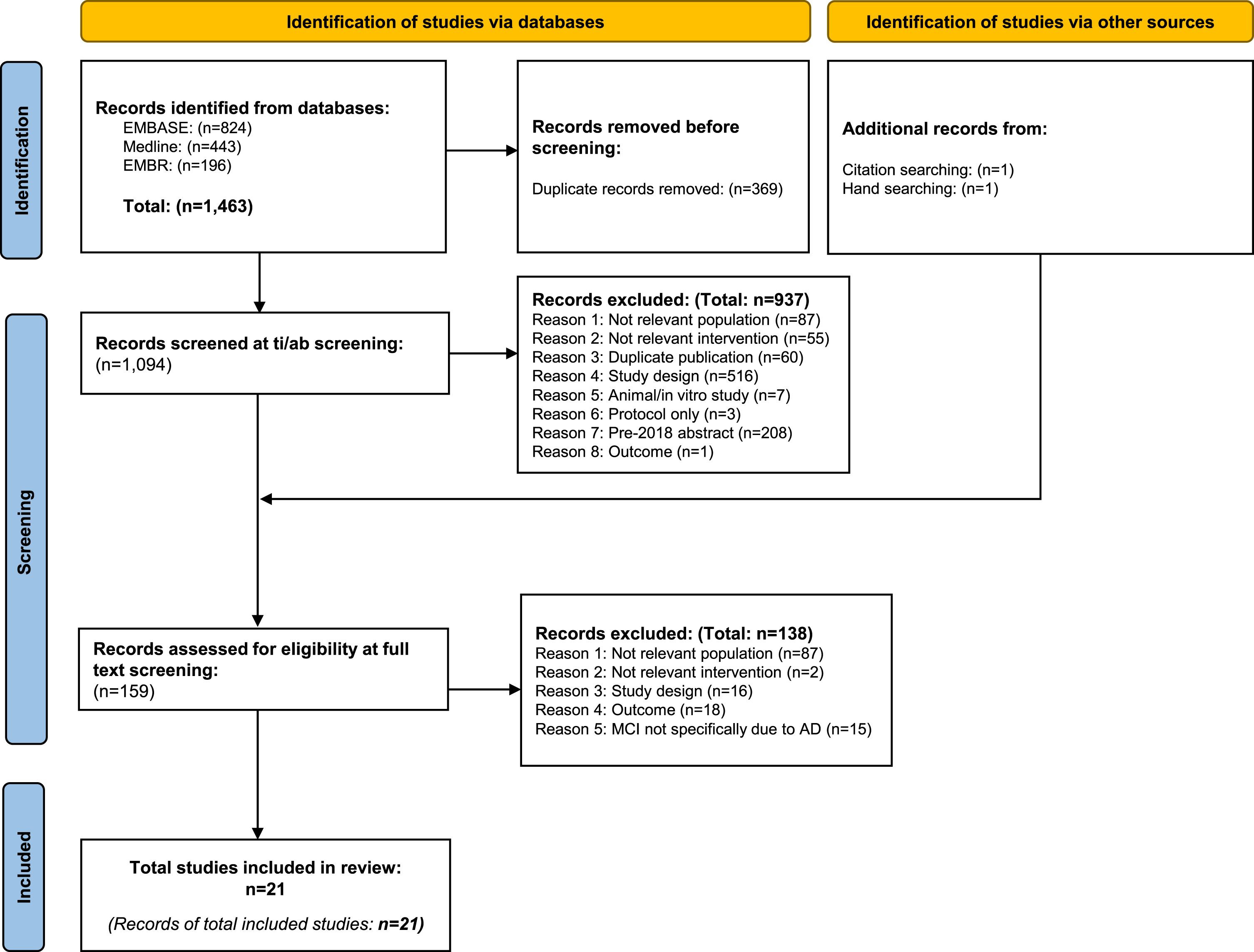
PRISMA diagram documenting the flow of studies during systematic review process.
Overall six studies were identified with low risk of bias [21, 36], eight were judged to have one or more ratings at high risk [25, 37–39], and seven were unclear [22, 41] (summarized in Supplementary Tables 9 and 10). High risk of bias was associated with a low sample size (<100) [30, 39] or having a population that may not represent the intended population (96% of study participants were female) [27]. Studies reporting the proportion of patients receiving different doses of a specific AChE inhibitor are recorded in Supplementary Table 11.
Summary of study characteristics
AChEi, acetylcholinesterase inhibitor; ADC, Alzheimer’s Disease Centers; AD, Alzheimer’s disease; ADNI, Alzheimer’s Disease Neuroimaging Initiative; APOE, apolipoprotein E; CDR, Clinical Dementia Rating; CS, cognitive stimulation; HRG, health region of Girona; IQR, interquartile range; MCI, mild cognitive impairment; MMSE, Mini-Mental State Exam; N, number; NACC, National Alzheimer’s Coordinating Center; NR, not recorded; PCHS, Public Health Catalan Healthcare Service; ReDeGi, Registry of Dementias of Girona; RUD, resource utilization in dementia; SATS, the Swedish Alzheimer treatment study; SD, standard deviation; UDS, uniform data set; UK, United Kingdom; USA, United States of America. *In Supplementary Table 1.
There were multiple sources of bias in the constituent studies. Some studies were limited due to their retrospective nature [25–28, 38] and many studies used medical records [26, 34] or databases as their source of data [21, 36]. Retrospective studies of medical records or databases are prone to bias as they are designed to assess pre-existing data which may be subject to recall bias or misclassification bias and data on confounding factors may be missing. The information on diagnosis was often established by the recruiting physician [24, 36] or from medical records [27, 40] or databases [23, 28]. Diagnostic criteria were reported but with no additional methodological details [21, 41]. A validated tool (Resource Utilization in Dementia (RUD)) was used to determine treatment records in four studies, [29, 36] while others used questionnaires or interviews with patients and/or carers [22–24, 41] or databases [21, 28]. The use of a validated tool is considered a more robust method as the tool has been tested for reliability and is considered fit for purpose. The study population is likely to be representative of real-world practice as community dwelling patients were recruited in seven studies [25, 35–37] and the majority of studies were multicenter [21–24, 41].
Table 2 summarizes prevalence data for symptomatic treatment patterns in MCI due to AD from four studies across six countries with low or unclear risk of bias. In Germany and North America, 18% [22] to 35% [21] of patients received any AChE inhibitors (including individual AChE inhibitors (three studies; n = 631 [21, 42]), 7% [23] to 8% [22] received memantine (two studies; n = 229), and 9% [21] received combination treatment (one study; n = 402). Of the population receiving symptomatic treatment, 9% to 87% had AChE inhibitors, 10% had memantine, and 4% had combined treatment (one study; n = 331) [24]. Patients receiving no treatment ranged from 41 [24] to 54% [21] (two studies; n = 733).
Summary of symptomatic treatment patterns in MCI due to AD by country
AChEi, acetylcholinesterase inhibitor; AD, Alzheimer’s disease; MCI, mild cognitive impairment; NR, not recorded; UK, United Kingdom; USA, United States of America. *Any or an individual AChEi. **Likely to report mixed population of monotherapy and combination therapy. • low risk of bias; •• unclear risk of bias.
Table 3 summarizes the prevalence data for symptomatic treatment patterns in mild AD dementia from ten studies across ten different countries with low or unclear risk of bias. In mild AD dementia patients from Europe or North America, 13 [22] to 89% [41] (IQR = 32.8) received any AChE inhibitor (46% [21] to 89% [41] received multiple AChE inhibitors) (6 studies; n = 3,715 [21, 41]), 1 [29] to 21% [22] (IQR = 15.6) received memantine (5 studies, n = 3,527 [21, 41]), and 0.4 [24] to 39% [21] (IQR = 29.8) received a combination of both (four studies, n = 3018 [21, 41]). There was insufficient data to demonstrate any differences by region. Of the population receiving symptomatic treatment, 10% [36] to 88% [24] received AChE inhibitors, 7% [24] to 10% [36] received memantine, and 3% [24] to 12% [36] received combined therapy (two studies; n = 1271). Patients not treated ranged from 9% [21] to 26% [28] (IQR = 10.4) (five studies, n = 4073 [21, 36]).
Summary of symptomatic treatment patterns in mild AD dementia by country
AChEi, acetylcholinesterase inhibitor; AD, Alzheimer’s disease; MCI, mild cognitive impairment; NR, not recorded; UK, United Kingdom; USA, United States of America. Denominator is the population with mild AD. *Any or an individual AChEi. **Likely to report mixed population of monotherapy and combination therapy. • low risk of bias; •• unclear risk of bias.
Table 4 summarizes symptomatic treatment patterns in early AD, a mixed population of MCI due to AD and mild AD dementia). Of patients treated for early AD, 15% to 80% received any AChE inhibitor while 70% received no symptomatic treatment (one French study; n = 195) [26].
Summary of symptomatic treatment patterns in early AD by country
AChEi, acetylcholinesterase inhibitor; eAD, early Alzheimer’s disease; MCI, mild cognitive impairment; NR, not recorded; UK, United Kingdom; USA, United States of America. Denominator is the population with early AD. *Any or an individual AchEi. • low risk of bias.
DISCUSSION
Summary of findings
Twenty-one studies were included in this review of symptomatic treatment patterns in the early clinical stages of AD. Findings confirm that patients being treated primarily with AChE inhibitors and to a lesser extent memantine and combination therapy. A proportion of patients remain untreated. Studies that reported on drug dose only in populations receiving symptomatic treatment were reported separately as they were not directly comparable to treatment pattern data.
Worldwide, 18 to 35% of patients diagnosed with MCI due to AD received any AChE inhibitor (three studies; n = 631 [21, 42]), 7 to 8% memantine (two studies; n = 229 [22, 23]), and 9% combination therapy (one study; n = 402 [21]). Patients receiving no treatment ranged from 41 to 54% (two studies; n = 733 [21, 24]). Worldwide, in mild AD dementia patients, 13 to 89% received any AChE inhibitor (six studies; n = 3,715 [21, 41]), 1 to 21% memantine (five studies, n = 3,527), and 0.4 to 39% combination therapy (four studies, n = 3018, [21, 41]). Patients receiving no treatment ranged from 9 to 26% (five studies, n = 4073 [21, 36]).
Treatment patterns for MCI due to AD were broadly similar in Europe and North America. AChE inhibitor use in Europe was 31% [22] and North America ranged from 19 to 35% [21, 23]. Use of memantine was lower in Europe (8%) [22] and North America (7%) [23]. Use of combination therapy was 9% in North America [21] and not reported in Europe [22]. Patients receiving no symptomatic treatment ranged from 41% (Internationally) to 54% (North America).
For mild AD dementia, use of AChE inhibitor was higher in Europe (up to 89% [41]) than in North America (46%) [21]. Use of memantine was low in Europe ranging from 7% [41] to 21% [22] and not clearly reported in North America. Combination therapy was low across Europe (0.4% [41] to 8% [28] but higher in North America (39%) [21]. The proportion of patients not treated was low in North America (9%) [21] and slightly higher in Europe (16% [32] to 26% [28]), and internationally (19%) [24].
The observed variations between regions may be explained by differences in the reimbursement status of the symptomatic treatments as well as differences in access to treatment (e.g., availability of generic medicines) and healthcare funding mechanisms (public and/or private).
Comparison to other reviews
To our knowledge, this is the first systematic review to investigate treatment patterns in MCI due to AD and mild AD dementia without geographical restrictions. A similar review was published in 2018 and focused on Japanese data but found no studies that reported on treatment or prescribing patterns in the management of cognitive function among patients with AD dementia in Japan [43]. Our study supports this view, and we included only one study, published in 2020, presenting Japanese data combined with France, Germany, UK, and US [24]. In a European survey of clinicians, a small proportion of the respondents routinely prescribed AChE inhibitor (21%) and memantine (13%) to patients with MCI due to AD [11]. In a Delphi survey of German clinical experts, the consensus reached was that most mild AD dementia patients were likely to receive AChE inhibitor, followed by memantine and 53% of patients are expected to receive no symptomatic treatment [10]. Our review is broadly in line with these surveys; however, we reported lower rates for ‘no treatment use’ in Europe (14% [36] to 26% [28]); no data was identified for ‘no treatment use’ in Germany. This disparity may be due to differences in the methodology and data reported, i.e., these surveys report the proportion of physicians prescribing treatments [11] or the clinical expert opinion of what patients are likely to receive, rather than actual proportion of patients receiving treatment or no treatment [10].
Implications
The review highlights that MCI due to AD patients are receiving treatment with AChE inhibitor, memantine, or combination therapy not reflected in the current guidelines and approvals [7–9]. Similarly, mild AD dementia patients are being treated with AChE inhibitors, memantine, or combination of AChE inhibitor with memantine where only AChE inhibitor is recommended and memantine is approved for moderate and severe AD treatments only [7–9]) In addition, up to 26% of mild AD dementia patients received no treatment [28], which is discordant with current guidelines [44–54]. Recent clinical trials report similar findings, where baseline data reported patients were receiving symptomatic treatment [12–14]. The current review aimed to capture reasons for non-compliance with guidelines; however, no reasons were explicitly reported, which could indicate limited evidence to support the recommendation and use of treatment options. The lack of approved treatments for MCI due to AD as well as limited evidence are likely to be the main reasons for no treatment in this population. Although there are approved treatments for mild AD dementia, potential reasons for no treatment may include lack of treatment availability, affordability issues, or patient refusal. Broadly, in psychiatry and more specifically in the treatment of dementia, prescribing patterns outside the approved drug labels are not uncommon and is mainly due to limitations of the evidence. Although some divergence was expected between guidelines and clinical practice due to their interpretation, the guidelines appear completely discordant with practice rather than just not ideally aligned. The differences between current guidelines and clinical practice, together with the recent approval of aducanumab in the US and the ongoing late-stage development of other disease modifying treatments presents a new opportunity for a consensus review of current guidelines [55].
Limitations
Our searches were restricted to 2009 onwards to reflect current practice, but it is important to acknowledge that there may be missing evidence. Furthermore, our supplementary searches were limited to reference checking and conference proceedings.
Data on the included patient characteristics, study methodology, or treatment dosage details were not widely reported by the included studies and therefore did not allow a closer interrogation of the data. Limited information was reported on missing data or timing of diagnosis and prescription such that changes in diagnosis or treatment may not be adequately captured. Such findings are common in real-world data, and a recent report [56] found that a third of all real-world evidence studies had limited reporting reflecting the challenges of meta-research of observational data. The GERAS [29, 32] and GERAS II [31, 36] databases featured quite heavily in our review focusing on different countries or timeframes. It is likely there is some overlap in the patients in these studies. The variance in the denominator population description highlights the challenge of heterogeneity: ‘mild AD dementia’, ‘mild AD dementia receiving treatment’, or ‘mild AD dementia receiving AChE inhibitors’; this variation limits comparisons across studies and countries/regions. A proportion of studies had low sample size (<100) but overall, the majority were in large studies with no overall concerns for risk of bias.
In our review, we found limited numbers of publications on MCI due to AD. Very few used the term prodromal AD [11, 24]. Although treatment patterns are reported, this is likely to be an under-representation of the population as MCI due to AD is inadequately identified in affected patients [57].
No reasons for the use of symptomatic AD treatments outside of their approved labels were identified. Future research should be designed to understand why clinicians are prescribing treatments outside of the current guidelines to patients with MCI due to AD and mild AD dementia.
Conclusions
Our systematic review demonstrates that while as per approved treatment labels and treatment guidelines, the use of symptomatic treatment is not recommended in MCI due to AD and only limited treatment is recommended in mild AD dementia, there is widespread real-world clinical use. These findings confirm the unmet medical need in early AD and together with the emergence of disease modifying treatments presents an opportunity to revise AD clinical treatment guidelines to accurately reflect current practice.